Vital and Health StatisticsStatistics, in carrying out this study. Dr. Jennifer Madans, Sandra...
24
Series 1 No. 38 Plan and Operation of the NHANES II Mortality Study, 1992 June 1999 Vital and Health Statistics From the CENTERS FOR DISEASE CONTROL AND PREVENTION / National Center for Health Statistics U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention National Center for Health Statistics
Transcript of Vital and Health StatisticsStatistics, in carrying out this study. Dr. Jennifer Madans, Sandra...

Series 1No. 38
Plan and Operationof the NHANES II MortalityStudy, 1992
June 1999
Vital andHealth StatisticsFrom the CENTERS FOR DISEASE CONTROL AND PREVENTION / National Center for Health Statistics
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICESCenters for Disease Control and Prevention
National Center for Health Statistics

Copyright information
All material appearing in this report is in the public domain and may bereproduced or copied without permission; citation as to source, however, isappreciated.
Suggested Citation
Loria CM, Sempos CT, Vuong C. Plan and operation of the NHANES II MortalityStudy, 1992. National Center for Health Statistics. Vital HealthStat 1(38). 1999.
Library of Congress Cataloging-in-Publication Data
Plan and operation of the NHANES II Mortality Study, 1992.p. cm. — (Vital and health statistics. Series 1, Programs and collection
procedures ; no. 38) (DHHS publication ; no. (PHS) 99-1314).ISBN 0-8406-0556-01. Health surveys—United States. 2. Mortality—United States Statistics.
3. Vital statistics—United States. I. National Center for Health Statistics (U.S.)II. Series. III. Series: DHHS publication ; no. (PHS) 99-1314.
[DNLM: 1. National Health and Nutrition Examination Survey (U.S.)2. Mortality—United States. 3. Data Collection—methods—United States.4. Health Surveys—United States. W2 A N148va no. 38 1999]RA409.U44 no. 38362.1'07'23 s[614.4'273]—DC21DNLM/DLCfor Library of Congress 99-29384
CIP
For sale by the U.S. Government Printing OfficeSuperintendent of DocumentsMail Stop: SSOPWashington, DC 20402-9328Printed on acid-free paper.

Plan and Operation of theNHANES II Mortality Study,1992
Series 1:Programs and CollectionProceduresNo. 38
Hyattsville, MarylandJune 1999DHHS Publication No. (PHS) 99-1314
Vital andHealth Statistics
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICESCenters for Disease Control and PreventionNational Center for Health Statistics

National Center for Health Statistics
Edward J. Sondik, Ph.D.,Director
Jack R. Anderson,Deputy Director
Jack R. Anderson,Acting Associate Director forInternational Statistics
Lester R. Curtin, Ph.D.,Acting Associate Director forResearch and Methodology
Jennifer H. Madans, Ph.D.,Acting Associate Director forAnalysis, Epidemiology, and Health Promotion
P. Douglas Williams,Acting Associate Director for DataStandards, Program Development, and Extramural Programs
Edward L. Hunter,Associate Director for Planning, Budget,and Legislation
Jennifer H. Madans, Ph.D.,Acting Associate Director forVital and Health Statistics Systems
Douglas L. Zinn,Acting Associate Director forManagement
Charles J. Rothwell,Associate Director for DataProcessing and Services
Office of Analysis, Epidemiology, and Health Promotion
Jennifer H. Madans, Ph.D.,Acting Associate Director
Division of Epidemiology
Elsie Pamuk, Ph.D.,Acting Director
Elsie Pamuk, Ph.D.,Acting Chief, Population EpidemiologyBranch
Sandra T. Rothwell,Chief, Longitudinal Studies Branch

Preface
This first wave of the NHANES IIMortality Study was jointlyfunded by the National Center for
Health Statistics and the Food and DrugAdministration. The authors would liketo acknowledge the assistance ofDorothy Blodgett, Sandy (Chia-Ying)Chien, Mary Dudley, and Shirley Gray,Division of Health ExaminationStatistics, in carrying out this study. Dr.Jennifer Madans, Sandra Rothwell, andChristine Cox deserve thanks forproviding advice throughout the study.The contribution of Westat, Inc., thecontractor who assisted with datacollection, is also gratefullyacknowledged.
iii

Contents
Preface. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . iii
Background. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1The Second National Health and Nutrition Examination Survey (1976–80). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
NHANES II Mortality Study, 1992 Study Design. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2Mortality Ascertainment. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
National Death Index Search. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3Social Security Administration Death Master File Search. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3Combination of the National Death Index and Death Master File Searches for 1979–88. . . . . . . . . . . . . . . . . . . . . . . . . . . . 3Death Certificate Ordering and Review. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Final Mortality Status on the Public-Release File. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Causes of Death. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Assessment of the NHANES II Mortality Study, 1992. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Methods Used. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6Results. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6Discussion. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
NHANES II Mortality Study, 1992 Analytic Cohort. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
References. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Detailed Tables
1. Number of deaths according to years of follow-up and sources of mortality status information in the the NHANES IIMortality Study, 1992. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
2. Comparison of cumulative survival probabilities after 5 and 10 years for the U.S. population compared withthose for the NHANES II Mortality Study cohort according to race, sex, and age group. . . . . . . . . . . . . . . . . . . . . . . . . . . 9
3. Expected number of survivors and decedents based on U.S. vital statistics data compared with observed number ofdecedents from 1976–78 in the NHANES II Mortality Study according to sex and age for all races combined. . . . . . . . . 10
4. Expected number of survivors and decedents based on U.S. vital statistics data compared with observed number ofdecedents from 1976–78 in the NHANES II Mortality Study according to race, sex, and age for selected racegroups. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
5. Number of participants in the NHANES II Mortality Study by mortality status at end of follow-up in 1992 accordingto sex and age at baseline for all races combined. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
6. Number of participants in the NHANES II Mortality Study by mortality status at end of follow-up in 1992 accordingto race, sex, and age at baseline for selected race groups. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Figures
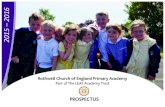
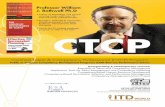
1. Tracing status of participants in the NHANES II Mortality Study, 1992 cohort. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32. An overview of the process used to assign mortality status to the NHANES II Mortality Study, 1992 participants. . . . . . 4
Appendixes
I. NHANES II baseline examination components for participants 30–75 years of age (1976–80). . . . . . . . . . . . . . . . . . . . . . . 14II. NHANES II baseline blood and urine assessments by specimen types for participants 30–75 years
of age (1976–80). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15III. NHANES II baseline pesticide residue and metabolite determinations for participants 30–75 years
of age (1976–80). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
v

ObjectivesThe NHANES II Mortality Study is a
prospective study of adult participantsexamined in the second National Healthand Nutrition Examination Survey(NHANES II) conducted between 1976and 1980. It was designed to investigatethe association between factorsmeasured at baseline and mortality. Themethods used in the study are describedand assessed in this report.
MethodsThe vital status of NHANES II
participants who were 30–75 years ofage at their examination was ascertainedafter 12–16 years. Vital status wasassessed by searching the NationalDeath Index and the Social SecurityAdministration Death Master File fordeaths occurring in the United States.Causes of death were obtained from theNational Center for Health StatisticsMultiple Cause of Death file or deathcertificates. To assess how well mortalitywas ascertained, the survival of thecohort after 5 and 10 years wascompared to that of the U.S. populationduring the same period.
ResultsAs of December 31, 1992,
23.2 percent of the 9,250 cohortmembers were found to be deceased.The remaining 76.8 percent that were notfound to be deceased may be assumedto be alive for analytic purposes.Cumulative survival probabilities for thecohort were generally higher thanprobabilities calculated from U.S. lifetable data. Although some differenceswere expected, these data suggest thatafter 10 years of follow-up using passivemethods, mortality may have been underascertained for the cohort. Discrepanciesbetween the survival patterns forNHANES II cohort and U.S. vital statisticswere larger for black than for whiteparticipants, indicating that ascertainmentof mortality was poorer among blackparticipants. Researchers using theNHANES II Mortality Study, 1992 datashould be aware of these study limitations.
Keywords: Epidemiologic methods cdata collection c health surveys ccohort studies c longitudinal study cfollow-up studies
Plan and Operation of theNHANES II Mortality Study,1992by Catherine M. Loria, Ph.D., Offıce of Analysis, Epidemiology, andHealth Promotion, National Center for Health Statistics, Centers forDisease Control and Prevention; Christopher T. Sempos, Ph.D., Offıceof Research on Minority Health, National Institutes of Health; andCuong Vuong, Division of Health Examination Statistics, NationalCenter for Health Statistics, Centers for Disease Control andPrevention
k
a
,II
n
ed
the
h
olytic
Background
The NHANES II Mortality Study isa prospective cohort study, whichpassively followed a subset
of participants in the Second NationalHealth and Nutrition Examination Survey(NHANES II). NHANES II, conductedbetween 1976–80, collected data from anational probability sample of the U.S.civilian, noninstitutionalized population6 months–74 years of age (1). Thesurvey included a standardized physicaexamination, laboratory tests, andquestionnaires that covered varioushealth-related topics. NHANES IIprovided a wealth of information on theprevalence of health conditions and risfactors. Nevertheless, the cross-sectionnature of the original survey limits itsusefulness for studying the effects ofclinical, environmental, and behavioralfactors on the development of specifichealth conditions.
The NHANES II Mortality Studywas designed to investigate theassociation between factors measuredbaseline and overall mortality or deathfrom specific causes. NHANES IIobtained information gathered fromphysical examinations, laboratory testsand interviews, whereas the NHANESMortality Study involved searchingnational data bases containinginformation about mortality and causes
l
al
t
of death. Mortality data from theNHANES II Mortality Study can belinked with the earlier baselineNHANES II data to examine therelationships between various factorsand specific causes of death.
Note that the design of theNHANES II Mortality Study differssubstantially from that of theNHANES I Epidemiologic FollowupStudy (NHEFS), a longitudinalfollow-up of an earlier NHANEScohort (2–5). NHEFS was an activefollow-up study in which participantswere recontacted and medical recordsand death certificates were obtained. Icontrast, the NHANES II MortalityStudy is entirely passive, that is,participants were not recontacted.Instead, mortality status was ascertainsolely by computerized matching tonational data bases and evaluation ofresulting matches. Furthermore, norecontact is planned in the future.Instead, matching to the National DeatIndex (NDI) and other national databases will continue periodically. Futurewaves will be released for public use asthey become available. One importantconsequence of the NHANES II MortalityStudy design is that persons not found tbe deceased are assumed alive for anapurposes. As a result the potential formisclassification of vital status exists.Researchers using data from theNHANES II Mortality Study should beaware of this study limitation.
Page 1

dn
ty,
n).
n
,of
icto
plnyg
ed
to
e
ns
d
o
s,
d
ded
rl
f
td
ly
od
,of
nd
f
Page 2 [ Series 1, No. 38
The Second NationalHealth and NutritionExamination Survey(1976–80)
An understanding of theNHANES II study design andprocedures is needed to use theNHANES II Mortality Study, 1992data effectively. A brief overview ofthe baseline study design and methois provided as follows and reported imore detail elsewhere (1).
NHANES II was designed to collecextensive demographic, medical histornutritional, clinical, and laboratory dataon a probability sample of the civilian,noninstitutionalized population betweethe ages of 6 months and 74 years (1The survey, conducted between1976–80, had a complex sample desigconsisting of a multistage, stratified,probability-based cluster sample ofhouseholds throughout the UnitedStates (1). The primary sampling unitswhich consisted of a county or groupcontiguous counties, were stratifiedaccording to demographic characteristand geographic region and grouped in64 superstrata. One primary samplingunit was selected from eachsuperstratum using a control selectionprocedure to produce a balanced samwith respect to variables such as regioState group, race-ethnicity, and povertlevel (1). Within each primary samplinunit, census enumeration districts,stratified by poverty level, were selectwith probability proportional to theirsize. Households within selectedenumeration districts were clustered insegments. One segment wassystematically selected within eachenumeration district. Approximately onperson was sampled from eachhousehold with oversampling of perso6 months–5 years of age and 60–74years of age.
A standardized set of questions anexamination procedures wasadministered by centrally trained staffand blood was drawn for variouslaboratory tests (1). At the initial visit tthe household, interviewers introducedthe survey, administered questionnaireand made appointments for theexamination. Interviewers also obtaine
s
s
e,
consent to retrieve additionalinformation from records includingthose from physicians, hospitals,schools, and State registry offices (1).Interviews and examinations wereconducted from Tuesdays throughSaturdays in mobile examinationcenters (MEC’s). Each MEC consisteof three trailers connected by enclospassageways and was divided intoseparate rooms for examinationcomponents, including a laboratory foprocessing blood and other biologicasamples. The examination andinterview lasted, on average, 2–3hours. Quality control proceduresincluded centralized training andperiodic retraining of field staff,routine calibration of instruments,replicate measures for a subset ofparticipants, and duplicate specimenprocessing for biochemicalmeasures (1).
NHANES II MortalityStudy, 1992 StudyDesign
The NHANES II Mortality Studycohort consists of adults whowere 30–75 years of age at
the time of their NHANES IIexamination. This cohort is a subset othe approximately 28,000 personsselected to participate in NHANES II.Some participants were interviewed bunot examined and only those examinewere followed for mortality status. Thebaseline included persons between theages of 6 months and 74 years but onadults were included in the follow-upcohort. Age at examination was used tidentify participants 30 years of age anover for selection into the NHANES IIMortality Study, 1992 cohort. Becauseseveral weeks could have elapsedbetween the interview and examinationsome participants who were 74 yearsage during their interview turned 75years of age between their interview aexamination. Therefore, the upper agelimit for the NHANES II MortalityStudy, 1992 cohort is 75 years. Atbaseline, 12,102 adults 30–74 years o
age agreed to be interviewed and 9,252(76 percent) completed a physicalexamination.
During this first wave of thestudy, mortality status was ascertainedfor the years 1976–92. Twoparticipants were unable to befollowed because of incompletepersonal identifying data and areconsidered lost to follow-up. Theremaining 9,250 cohort members weretraced in the NHANES II MortalityStudy, 1992 by searching national databases containing mortality and causeof death information. Length offollow-up ranges from 12 through 16years. Approximately 23 percent(n = 2,145) of the NHANES IIMortality Study, 1992 cohort werefound to be deceased as of December31, 1992 (figure 1).
Mortality AscertainmentMortality status was ascertained by
searching two computerized data basescontaining information on deathsoccurring in the United States. The NDI,compiled by the National Center forHealth Statistics (NCHS), contains astandard set of identifying data for eachdecedent provided by State vitalstatistics offices (6,7). Beginning withdeaths occurring in 1979, the NDIcontains deaths for all 50 States, theDistrict of Columbia, Puerto Rico, andthe Virgin Islands (6). The SocialSecurity Administration’s (SSA) DeathMaster File (DMF) contains informationon all U.S. decedents whosebeneficiaries received death benefitsfrom the SSA (8). The DMF pools datafrom a variety of SSA files, includingthe SSA Master Beneficiary Record thatcontains a record for each personentitled to receive retirement orsurvivor’s benefits and disabilityinsurance.
The results of each search wereevaluated separately and later combinedusing the following process (also,outlined infigure 2) to create theNHANES II Mortality Study, 1992public-release file.

e
stee
ia
s,
las
edhe
er
d
g
h
fe
esalst
of
t.
er
to
d
t.
h
Figure 1. Tracing status of participants in the NHANES II Mortality Study, 1992 cohort
Series 1, No. 38 [ Page 3
National Death Index Search
The NDI was searched for deathsoccurring between 1979–92. At the timthe NHANES II Mortality Study, 1992data were collected, 1992 was the lateyear for which cause of death data weravailable. Social Security numbers wernot collected during NHANES II;therefore, potential matches with theNDI were initially identified usingname, date of birth, and sex, accordingto the standard NDI matchingprocess (6). These NDI matching criterare liberal enough to ensure that truematches will not be missed, but alsothey generally yield many false matcheespecially for participants with commonnames.
In an attempt to eliminate falsepositive matches, all matches returnedby the NDI were manually reviewedusing the previously mentionedinformation and, additionally, observedrace, State of birth, State of residence,and marital status. Each potential NDImatch was tentatively classified byNHANES II Mortality Study, 1992 staffas ‘‘true,’’ ‘‘possible,’’ or ‘‘false.’’ Theonly exceptions to this manual reviewprocess were those matches thatmatched all fields exactly (i.e., name,date of birth, sex, observed race, Stateof birth, State of residence, and maritastatus); these matches were classifiedtrue without further review (54 percentof 1,973 true matches). For all otherNDI matches, a ‘‘true’’ classificationwas assigned if enough evidence existto assume that the death pertained to tNHANES II participant. A ‘‘possible’’was assigned if NHANES II MortalityStudy, 1992 staff were uncertain wheth
the death pertained to the NHANES IIparticipant based on the availableevidence from the NDI. This code wasused to identify cases for whom thedeath certificate identified by thepotential match should be ordered toallow for further evaluation. A ‘‘false’’was assigned if the available evidencefrom the NDI suggested that the deathdid not pertain to the NHANES IIparticipant. Overall, NHANES IIMortality Study, 1992 staff erred on theside of being conservative and assignea possible if they were uncertain ineither direction.
Social Security AdministrationDeath Master File Search
Because the NDI does not includedeaths occurring before 1979, the SSADMF was searched for deaths occurrinin 1976–78. Additionally, the DMF wasalso searched from 1979 through Marc31, 1988, to confirm the NDI matchresults for this period. Data extractedfrom the DMF after March 1988 werenot available at the time this study wasconducted.
As with the NDI, the initial criteriato identify potential matches to theDMF were based on name and date obirth and were liberal enough to ensurthat ‘‘true’’ matches would not bemissed. The quality of potential matchwas further evaluated using a numericscoring algorithm based on first and laname, date of birth, and State ofresidence. Matches with scores highenough to indicate at least partialmatching on name and date of birthwere then manually examined in an
attempt to eliminate ‘‘false’’ matches.Besides name and date of birth, theseevaluations used the last known Stateresidence compared with the Zip codewhere the lump sum payment was sen
Each DMF match was tentativelyclassified by NHANES II MortalityStudy, 1992 staff as true, possible, orfalse. A ‘‘true’’ classification wasassigned if enough evidence existed toassume that the death pertained to theNHANES II participant. A ‘‘possible’’was assigned if NHANES II MortalityStudy, 1992 staff were uncertain wheththe death pertained to the NHANES IIparticipant based on the availableevidence from DMF. The ‘‘possible’’code was used to identify cases forwhom the death certificate identified bythe potential match should be orderedallow for further evaluation. A ‘‘false’’was assigned if the available evidencefrom DMF suggested that the death didnot pertain to the NHANES IIparticipant. Overall, NHANES IIMortality Study, 1992 staff erred on theside of being conservative and assignea ‘‘possible’’ if they were uncertain ineither direction.
Combination of the NationalDeath Index and Death MasterFile Searches for 1979–88
When the NDI and DMF resultswere combined, differing outcomesexisted for some NHANES IIparticipants. For example, NCHS staffmay have assigned a ‘‘true’’ matchbased on NDI and a ‘‘possible’’ matchbased on DMF for the same participanIn some cases, NDI and DMF couldhave been referring to the same deathcertificate, but NHANES II MortalityStudy, 1992 staff could not be certainbecause DMF did not provide the deatcertificate number. The dates of deathwere used to identify cases where NDIand DMF were most likely referring tothe same death certificate.
Because very few cases existedwhere the NDI and DMF dates of deathdiffered, NHANES II Mortality Study,1992 staff were able to order the deathcertificates for both matches from Statevital statistics offices. If the certificateswere received, they were evaluated toresolve the discrepancy. Data on the

e,
n
Figure 2. An overview of the process used to assign mortality status to the NHANES IIMortality Study, 1992 participants
Page 4 [ Series 1, No. 38
death certificate, including address,spouse, State of birth, next of kin, racmarital status, and usual occupation,were checked against these datacollected during NHANES II. Based othis review, NHANES II MortalityStudy, 1992 staff decided which of thetwo matches, if any, pertained to theNHANES II participant.
More cases existed where the deathdates from NDI and DMF matchedexactly or were fairly close (e.g., theyear was the same but the monthdiffered, and it looked like atransposition error). In such cases, itwas assumed that NDI and DMF werereferring to the same death certificate.Before ordering death certificates,
NHANES II Mortality Study, 1992 staffassigned an outcome that gave moreweight to the NDI results because moreinformation was used in the matchingprocess for NDI (i.e., name, gender, dateof birth, race, State of birth, State ofresidence, and marital status) ascompared with DMF (i.e., name,gender, date of birth, and State ofresidence). However, the NDI-basedoutcome may have been changed inthese discrepant cases if theDMF-identified death certificate wasreviewed and it was determined thatthe DMF match pertained to theNHANES II participant.
Death Certificate Ordering andReview
Because of limited resources forthis study, NHANES II Mortality Study,1992 staff were unable to order deathcertificates from States and evaluate allof the true and possible matchesidentified from the NDI and DMF. Thematches were ranked and as many ofthe death certificates as resourcesallowed were ordered. Priority wasgiven to the following:
+ Matches for which NHANES IIMortality Study, 1992 staff could notobtain the cause of death frominternal NCHS files.
+ Cases with discrepant matches fromNDI and DMF in which the dates ofdeath differed.
+ ‘‘True’’ and ‘‘possible’’ matchesidentified solely through DMF(because NCHS had received solittle information from DMF todetermine whether the matchpertained to the NHANES IIparticipant). NHANES II MortalityStudy, 1992 staff ordered as manyNDI ‘‘true’’ and ‘‘possible’’matches as resources permitted,mainly from States that NCHS wasalready requesting deathcertificates identified by DMF,because this was the mostcost-effective approach. As aresult, death certificates wereordered for relatively few NDI‘‘true’’ and ‘‘possible’’ matches,because NHANES II MortalityStudy, 1992 staff felt more

dofge
,
d
toon
a
e
,d
r
s
Series 1, No. 38 [ Page 5
confident given that the NDImatches used more information inthe matching process.
Death certificates were ordered anreceived for approximately 27 percentthe 2,145 decedents. A small percentaof the death certificates ordered werenot received for one of the followingreasons:
+ DMF did not provide the State ofdeath and death certificate numberand the State vital statistics officecould not find the death certificatebased on name, gender, date ofdeath, and date of birth.
+ NDI provided the State of death andeath certificate number; but in asmall number of cases, the deathcertificate received did not appearbe the death certificate referencedthe NDI, possibly because oftypographic errors in the deathcertificate number.
NCHS was unable to evaluate allof the death certificates receivedbecause of staffing limitations. Fordeaths occurring during the periodcovered by DMF only (1976–78),death certificates were evaluated forsample of the DMF ‘‘true’’ matches toensure that criteria for classifyingDMF ‘‘true’’ matches were sensitive.For the same period, all deathcertificates were evaluated for DMF‘‘possible’’ matches because of theuncertainty about these matches thatwere based on so little information.Certificates for deaths occurringbetween 1979–88 for all ‘‘true’’ and‘‘possible’’ matches identified solelythrough DMF were evaluated in casethe death on the NDI was missed. Asample of death certificates for allNDI ‘‘true’’ and ‘‘possible’’ matcheswere evaluated to ensure that criteriafor classifying them were sensitive. Inall evaluations data on the deathcertificate were checked against thesdata collected during NHANES II,including address, spouse, State ofbirth, next of kin, race, marital statusand usual occupation. About one-thirof the 712 death certificates orderedand received were reviewed byNHANES II Mortality Study, 1992staff.
Final Mortality Status on thePublic-Release File
Decedents on the public-release fileconsist only of participants with a final‘‘true’’ match after combining the resultsof the NDI and DMF evaluations andreviewing selected death certificates. Foparticipants with a final ‘‘possible’’match, NHANES II Mortality Study,1992 staff concluded that the availableevidence was not convincing enough todetermine that the match pertained tothe NHANES II participant. Thus,NHANES II Mortality Study, 1992 staffassumed that the participants were stillalive. Matches with a ‘‘possible’’ codewill be stored on internal NCHS filesfor later investigation if the participantdoes not match to a national data baseafter a reasonable amount of time.Participants with a final ‘‘false’’ matchwere also assumed alive.
In all, 2,145 deaths were identifiedusing the process described earlier. Thenumbers of deaths by year of follow-upand sources of mortality data arepresented intable 1. Between 1976 and1978, 84 deaths were identified throughDMF, the only source of mortalityinformation available for this period.Between 1979 and 1988, 863 deathswere identified through NDI and DMF,363 deaths by NDI alone, and 88 deathby DMF alone. During the final period1989–92, 747 deaths were identifiedthrough the NDI, the only sourceavailable. A small percentage of thedeaths that occurred between 1979–88were identified through DMF(4.1 percent) and were not foundthrough NDI. In these cases,NHANES II Mortality Study, 1992 staffreviewed the death certificates andconfirmed the deaths.
Causes of DeathFor most deaths identified through
the NDI, causes of death were obtainedfrom the NCHS Multiple Cause ofDeath (MCD) file (9,10) by matching onthe death certificate number. Thesedeaths were coded by nosologists in theindividual State vital statistics offices orat NCHS according to theInternationalClassification of Diseases, NinthRevision(ICD–9). Death certificates
were ordered for all deaths identifiedonly through the DMF. The causes ofdeath for these participants were codedby nosologists at NCHS using the samecriteria as those used for the MCD file.Additionally, death certificates wereordered and causes of death coded for asmall percentage of NDI-identifieddeaths from States that did not have100 percent coverage on the MCD file.
Multiple causes of death areavailable for 98 percent (n = 2,104) ofdecedents, and, thus, are missing for 41decedents. Causes of death were missingif the death certificate could not befound in State vital statistics offices.Additionally, causes of death were notobtained for a few deaths that were laterdetermined to be missing from the MCDfile.
The date of death was abstractedfrom either the file returned by NDI orthe death certificate.
Assessment of theNHANES II MortalityStudy, 1992
The main advantage of usingpassive follow-up methods is thelow cost of tracing large,
dispersed cohorts. Nevertheless, reliancesolely on these methods to ascertainmortality introduces some uncertaintyand potential biases (11). Previousstudies have estimated the sensitivity ofmatching to the NDI at 87 to 97 percent.As in the NHANES II Mortality Study,1992, these studies used name and dateof birth as initial matching criteria withadditional information, such as gender,race, and marital status, to eliminatefalse matches (12–15). Estimates of thesensitivity of searching the SSA DMFare unavailable from previous studieswhen the Social Security number is notused in the matching process. In thisstudy the sensitivity of matching toDMF with the NHANES II MortalityStudy, 1992 study protocol was70 percent, using overlapping data forthe period 1979–88 from the DMF andNDI and using NDI as the ‘‘goldstandard.’’

e
x
d
S
e
t
o
s
f
hd
d
d
d
Page 6 [ Series 1, No. 38
Given the limitations of passivemethods, the survival of the NHANES IIMortality Study, 1992 cohort wascompared to that of the U.S. populationduring the same period to assess howwell mortality was ascertained in theNHANES II Mortality Study, 1992. Theoverall performance of the combinedresults from the NDI and DMF searcheswere evaluated by examining cumulativsurvival rates after 5 and 10 years.Additionally, the number of expecteddeaths were compared with observeddeaths for the period covered solely byDMF because matching to DMFappeared to be less sensitive thanmatching to NDI.
Methods UsedTo assess how well mortality was
ascertained in the NHANES II MortalityStudy, 1992, the survival of the cohortwas compared to that of the U.S.population during the same period.Cumulative survival probabilities after 5and 10 years were calculated for 24race-sex-age groups in the NHANES IIMortality Study, 1992 cohort using theKaplan-Meier product limit method (16).Sample weights were used to calculateestimates for the cohort but the complesample design of NHANES II was nottaken into account. Cumulative survivalprobabilities (nP0) for the U.S.population after 5 and 10 years werecalculated using mortality rates extractefrom U.S. life tables according toformula (1):
nP0 = ∏i = 0
n − 1
[1 − 1qa + i, 1978 +i ](1)
where
n = number of years of follow-up
1qx, y = probability that persons in agiven race-sex group alive atagex will die within 1 yearaccording to the U.S. life tablefor yeary
a = midpoint of the age interval atbaseline (1978)
The year 1978 was used as thebeginning of follow-up because it wasthe approximate midpoint of
NHANES II. Mortality rates forsuccessive years from life tables wereused to account for the decrease in U.death rates that occurred over thefollow-up period. Participants of racegroups other than white and black weromitted from this analysis because oftheir small numbers in the NHANES IIMortality Study, 1992 cohort.
To evaluate mortality ascertainmenfor the years covered solely by theDMF, the number of deaths expected toccur between 1976 and 1978 wereestimated and compared with theobserved number of deaths for thisperiod. Mortality rates for each race,sex, and age group from U.S. life tablewere used to calculate the expectednumber of survivors at the beginning o1979 (n1979) as:
n1979= [O1976(1 − qa, 19761/2)
(1 − qa + 1, 1977) (1 − qa + 2, 1978)]
+[O1977(1 − qa, 19771/2)
(1 − qa + 1, 1978)]
+[O1978(1 − qa, 19781/2)] (2)
where
Oy = number examined during yeary
1qx,y = probability that persons in agiven race-sex group alive atagex will die within 1 yearaccording to the U.S. life tablefor yeary
a = midpoint of the age interval atbaseline
The expected number of deaths in eacrace-age-sex group was then calculateas the difference between the totalnumber examined from 1976–79(N1976–78) and the expected number ofsurvivors during this period (n1979).
ResultsThe cumulative survival
probabilities for the U.S. population anthe NHANES II Mortality Study, 1992cohort are presented intable 2by race,sex, and age group. The survivalprobabilities for the cohort were largerthan for the U.S. population in each ofthe four race-sex groups. Differencesbetween probabilities for the cohort anthe U.S. population were most similar
.
among white males and females. In bothgroups the largest differences after fiveyears were observed in the oldest agegroup but after 10 years, groups withthe largest differences expanded toinclude 65–69-year-olds and60–64-year-old females. The largestdiscrepancies between the cohort andU.S. survival patterns were foundamong black men and women.Compared with white men and women,differences between survivalprobabilities after 5 years of follow-upwere consistently larger in all agegroups and much larger among blackmales 70–75 years of age. Differencesbetween survival probabilities by racewere generally larger after 10 yearscompared to 5 years of follow-up.
The expected and observed numberof deaths during 1976–78 are presentedin table 3by sex and age group for allrace groups combined and intable 4for24 selected race-sex-age groups.Overall, 84 deaths were observed, justover one-half of the expected deathsduring this period. Ratios of observed toexpected deaths were lowest amongparticipants 50–59 and 70–75 years ofage and highest among those 60–64 an65–69 years of age. Observed toexpected ratios were approximately thesame for males and females, althoughsome variation existed by age groupbetween the sexes, primarily in theyounger age groups. Ratios wereapproximately the same for white malesand white females but lower for blackparticipants. While the observed toexpected ratio for all age groupscombined was lowest among blackfemales, there were more age groupsamong black males in which none of theexpected deaths were found during thefirst 3 years of follow-up.
DiscussionCumulative survival probabilities
for the NHANES II Mortality Study,1992 cohort were generally higher thanexpected probabilities calculated fromU.S. life table data. Based on themagnitude of differences between them,mortality ascertainment was better forthe white participants and worse for theblack participants. Ascertainment after 5years was poorer among the white

ngr
ll
s
e
t
p,
t
t
s
e
k
)
eb
f
Series 1, No. 38 [ Page 7
participants 70–75 years of agecompared with other age groups,although it did not change substantiallyafter 10 years for the oldest age group.On the other hand, ascertainment amowhite females 60 years of age and ovewas poorer after 10 years comparedwith 5 years. Among black participantspoor ascertainment was not limited tospecific age groups. Althoughdifferences between 5- and 10-yearsurvival varied by age group among theblack participants, the differencessuggest that ascertainment was generapoorer after 10 years.
Some differences in mortalityascertainment were expected given theNHANES II sample design. NHANES IIwas a sample of noninstitutionalizedpersons, whereas expected probabilitiewere based on data for the entire U.S.population that included institutionalizedpersons with lower survival rates. Giventhis design the largest differences wereexpected among the oldest age groupand should have decreased over time.This expectation was consistent with thresults. Mortality ascertainment waspoorest among participants in the oldesage group during the first 3 years offollow-up. Larger discrepancies in5-year survival existed in this age grouand such differences did not increaseover time except among black females.However, it is unlikely that the sampledesign could explain all of thedifferences found between the cohortand U.S. survival patterns, even amongwhite men and women.
Incomplete national mortality datafor the first 3 years of follow-up couldhave contributed to under ascertainmenof mortality in the NHANES IIMortality Study, 1992. Because the firstwave of the study included years notcovered by NDI, NHANES II MortalityStudy, 1992 staff relied on the DMF forfinding deaths occurring for 1976–79. Inanother study comparing the totalnumber of deaths on the DMF to U.S.vital statistics data, the DMF contained89 percent of all deaths occurring in theUnited States between 1975–84 (8).Thus, at best, only 89 percent ofdeaths could be detected in theNHANES II Mortality Study duringthe first 3 years of follow-up. Thepercent of deaths actually detected
y
during the first 3 years of the studywas much less than this, especiallyamong black participants 70–75 yearsof age at baseline.
Limitations in personal identifyingdata for NHANES II participantsprobably also contributed to underascertainment. NHANES II was notdesigned as a longitudinal study, andbecause of this, important personalidentifiers, such as Social Securitynumber and father’s surname, were nocollected. Furthermore, personalidentifiers were not recorded with asmuch care as they would have been ifNHANES II staff had known thatidentifiers would be used to link tonational mortality data bases. Forexample, some participants only gavetheir first and middle initials instead ofcomplete names and this was acceptedwithout further probing. Thus, thequality of personal identifiers was not ahigh as it could have been if alongitudinal component had beenincluded in the NHANES II design.Problems with personal identifiers in thNHANES II Mortality Study wouldhave affected passive follow-upthroughout the entire follow-up period,and possibly contributed to largerdifferences in survival probabilitiesbetween 5 and 10 years among theblack participants and older women.
Under ascertainment of deathsduring the years covered solely by theDMF was greater among the black thanamong the white participants. Poorermortality ascertainment among the blacparticipants was consistent with largerdiscrepancies in 5-year survival for thisgroup and with previous studies (17,18using the DMF. Furthermore,discrepancies in 10-year survival werelarger among black than whiteparticipants, suggesting thatascertainment was problematic for theformer group throughout the entirefollow-up period. Previous studiesevaluating the effectiveness of NDI havsuggested that ascertainment may notas good for black decedents as it is forwhite decedents (12,19,20). In a studyof the survival of the NHEFS cohort,differences between observed andexpected survival after 5 and 8 years ofollow-up were larger for black than forwhite participants (21). Because
e
mortality was ascertained through activetracing methods in NHEFS (22), someof the differential ascertainment by racein the NHANES II Mortality Study,1992 may have been independent of thepassive methods used. Other factorsbesides under ascertainment may havecontributed to the larger differences insurvival among black participants. In theNHANES II Mortality Study, 1992,survival estimates for black participantsmay have been less stable than for whiteparticipants, given the smaller numberof black participants compared withwhite participants in the NHANES IIsample. Differences by race in thequality of denominator data used tocalculate the U.S. estimates may alsohave affected the comparisons.
In conclusion, the analysispresented here suggests that after 10years of follow-up using passivemethods, mortality may have been underascertained for the NHANES IIMortality Study, 1992 cohort. Becausethis analysis used expected data basedon the U.S. population, it probablyoverestimated the degree of underascertainment, but it is unclear by howmuch. Nonetheless, the analysis showsthat compared with white participants,ascertainment of mortality was pooreramong black participants.
NHANES II MortalityStudy, 1992 AnalyticCohort
A pproximately 23 percent(n = 2,145) of the NHANES IIMortality Study, 1992 cohort
(n = 9,250) was found to be deceased(table 5). The percentage of maledecedents (28.9 percent) was higher thanthe percentage of female decedents(18.1 percent) among all racescombined, a trend that was alsoobserved within each age group(table 5). This same pattern, higherpercentages of male decedents comparedwith female decedents, was alsoobserved among the white and blackparticipants (table 6).

r
n
f
e
1
1
1
1
1
1
1
2
2
2
Page 8 [ Series 1, No. 38
The remaining 77 percent(n = 7,105) that were not found to bedeceased as of December 31, 1992,(table 5) may be assumed to be alive foanalytic purposes. This assumption maypotentially result in the misclassificationof vital status for some cohort membersbecause of the passive methods used ithis study. That is, some true matchesmay have been inadvertently eliminatedand some false matches retained. It ismore likely that true matches wereeliminated rather than false matchesretained because NHANES II MortalityStudy, 1992 staff erred on the side ofbeing conservative in determiningmatches. True matches that wereeliminated would continue toaccumulate person-years of follow-up. Ithe rate of eliminating true matches isunrelated to the exposure of interest,eliminating true matches should notattenuate risk ratios but may reduce thestatistical power of studies using theNHANES II Mortality Study, 1992 data(11). More important, caution should beexercised when using the NHANES IIMortality Study, 1992 data to makecomparisons based on race because ofthe apparent differential ascertainment omortality by race. Researchers using thNHANES II Mortality Study, 1992 datashould be aware of these studylimitations and consider them whendrawing conclusions based on thesedata.
Finally, subjects 60–74 years of agewere oversampled in NHANES II and,thus, are overrepresented in theNHANES II Mortality Study, 1992cohort. Therefore, NCHS recommendsthat analysts use the baseline sampleweights and sample design variables toaccount for the complex sample designin analyses of the NHANES II MortalityStudy, 1992 data.
f
References
1. McDowell A, Engle A, Massey JT,Maurer K. Plan and operation of theSecond National Health and NutritionExamination Survey 1976–1980.National Center for Health Statistics.Vital and Health Stat 1(15). 1981.
2. Cohen BB, Barbano HE, Cox CS, et al.Plan and operation of the NHANES IEpidemiologic Followup Study1982–84. National Center for HealthStatistics. Vital and Health Stat 1(22).1987.
3. Finucane FF, Freid VM, Madans JH, etal. Plan and operation of the NHANESI Epidemiologic Followup Study, 1986.National Center for Health Statistics.Vital and Health Stat 1(25). 1990.
4. Cox CS, Rothwell ST, Madans JH, etal. Plan and operation of the NHANESI Epidemiologic Followup Study, 1987.National Center for Health Statistics,Vital and Health Stat 1(27). 1992.
5. Cox CS, Mussolino ME, Rothwell ST,et al. Plan and operation of theNHANES I Epidemiologic FollowupStudy, 1992. National Center for HealthStatistics, Vital and Health Stat 1(35).1997.
6. National Center for Health Statistics.National Death Index user’s manual.DHHS Pub. No. (PHS) 90–1148.Washington: Public Health Service.1991.
7. Patterson BH, Bilgrad R. Use of theNational Death Index in cancer studies.J Natl Cancer Inst 77(4):877–81. 1986.
8. Schnorr TM, Steenland K. Identifyingdeaths before 1979 using the SocialSecurity Administration Death MasterFile. Epidemiology 8(3):321–3. 1997.
9. Israel RA, Rosenberg HM, Curtin LR.Analytical potential for multiplecause-of-death data. Am J Epidemiol124(2):161–79. 1986.
10. National Center for Health Statistics.Multiple Causes of Death in theUnited States. Volume 32, number 10,supplement (2). (PHS) 84–1120. 1984.
11. Howe GR. Use of computerized recordlinkage in cohort studies. EpidemiolRev 20(1):112–21. 1998.
12. Boyle CA, Decoufle P. National sourcesof vital status information: Extent ofcoverage and possible selectivity inreporting. Am J Epidemiol 131:160–8.1990.
3. Stampfer MJ, Willett WC, Speizer FE,et al. Test of the National Death Index.Am J Epidemiol 119:837–9. 1984.
4. Wentworth DN, Neaton JD, RasmussenWL. An evaluation of the SocialSecurity Administration MasterBeneficiary Record File and theNational Death Index in theascertainment of vital status. Am JPublic Health 73:1270–4. 1983.
5. Williams BC, Demitrack LB, Fries BE.The accuracy of the National DeathIndex when personal identifiers otherthan Social Security number are used.Am J Public Health 82(8):1145–7.1992.
6. SAS Institute Inc. SAS Language andProcedures: Usage, Version 6. 1st ed.Cary, NC: SAS Institute, Inc., 1989.
7. Alvey W, Aziz F. Quality of mortalityreporting in SSA linked data: Somepreliminary descriptive results.Statistical Uses of AdministrativeRecords with Emphasis on Mortalityand Disability Research. Washington,D.C.: Social Security Administration.1979.
8. Reyes M, Stebbings JH, Voelz GL.Evaluation of social security follow-upof some southwestern populations. JOccup Med 24:198–202. 1982.
9. Curb JD, Ford CE, Pressel S, et al.Ascertainment of vital status throughthe National Death Index and theSocial Security Administration. Am JEpidemiol 121(5):754–66. 1985.
0. Acquavella JF, Donaleski D, HanisNM. An analysis of mortality follow-upthrough the National Death Index for acohort of refinery and petrochemicalworkers. Am J Ind Med 9(2):181–7.1986.
1. Madans JH, Cox CS, Kleinman JC, etal. 10 years after NHANES I: Mortalityexperience at initial followup, 1982–84.Public Health Rep 101(5):474–81.1986.
2. Madans JH, Kleinman JC, Cox CS, etal. 10 years after NHANES I: Reportof initial followup, 1982–84. PublicHealth Rep 101(5):465–73. 1986.

Table 1. Number of deaths according to years of follow-up and sources of mortality status information in the the NHANES II Mortality Study,1992
Year
Source of morality status
DMF1 NDI2 and DMF NDI Total
Numberof deaths Percent
Numberof deaths Percent
Numberof deaths Percent
Numberof deaths Percent
1976–78 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 84 3.9 . . . . . . . . . 84 3.91979–883 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 88 4.1 863 40.2 363 16.9 1,314 61.31989–92 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 747 34.8 747 34.8Total . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 172 8.0 863 40.2 1,110 51.7 2,145 100.0
. . . Category not applicable.1DMF is the Social Security Administration’s Death Master File.2NDI is National Death Index.3DMF was available through March 31, 1988. The remainder of 1988 was covered solely by the NDI.
NOTE: NHANES II is the Second National Health and Nutrition Examination Survey.
Table 2. Comparison of cumulative survival probabilities after 5 and 10 years for the U.S. population compared with those for theNHANES II Mortality Study cohort according to race, sex, and age group
Race, sex, and age group
5 years 10 years
United States
NHANES IIMortality Study
cohort1 United States
NHANES IIMortality Study
cohort1
White male30–39 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.990 0.996 0.977 0.98040–49 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.977 0.987 0.944 0.95450–59 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.940 0.957 0.858 0.89160–64 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.874 0.880 0.735 0.76365–69 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.824 0.835 0.624 0.66970–75 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.744 0.811 0.485 0.550
White female
30–39 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.995 0.994 0.988 0.98940–49 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.987 0.981 0.968 0.96850–59 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.969 0.989 0.923 0.93760–64 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.938 0.952 0.852 0.90265–69 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.908 0.935 0.780 0.84770–75 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.857 0.904 0.668 0.720
Black male
30–39 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.974 0.995 0.940 0.97740–49 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.948 1.000 0.883 0.98050–59 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.892 0.943 0.770 0.83660–64 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.827 0.887 0.654 0.83465–69 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.782 0.846 0.556 0.71170–75 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.715 0.872 0.451 0.595
Black female
30–39 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.989 1.000 0.973 0.98940–49 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.973 0.952 0.938 0.92450–59 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.942 1.000 0.865 0.96460–64 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.901 0.929 0.784 0.86665–69 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.869 0.942 0.706 0.85970–75 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.812 0.892 0.600 0.723
1Sample weights from the Second National Health and Nutrition Examination Survey were used.
NOTE: NHANES II is the Second National Health and Nutrition Examination Survey.
Series 1, No. 38 [ Page 9

Table 3. Expected number of survivors and decedents based on U.S. vital statistics data compared with observed number of decedentsfrom 1976–78 in the NHANES II Mortality Study according to sex and age for all races combined
Sex and age groupNumber
examined
Expectednumber ofsurvivors
Expectednumber ofdecedents
Observednumber ofdecedents
Ratio ofobserved to
expected
Male1
30–39 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 629 626 3 – –40–49 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 497 493 4 3 0.7550–59 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 511 501 10 2 0.2060–64 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 631 607 24 18 0.7565–69 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 495 468 27 19 0.7070–75 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 373 345 28 12 0.43Total . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3,136 3,040 96 54 0.56
Female1
30–39 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 697 696 1 2 2.0040–49 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 541 538 3 1 0.3350–59 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 591 585 6 3 0.5060–64 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 660 648 12 6 0.5065–69 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 585 570 15 11 0.7370–75 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 452 433 19 7 0.37Total . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3,526 3,470 56 30 0.54
Total1
30–39 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 1,326 1,322 4 2 0.5040–49 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 1,038 1,031 7 4 0.5750–59 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 1,102 1,086 16 5 0.3160–64 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 1,291 1,255 36 24 0.6765–69 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 1,080 1,038 42 30 0.7170–75 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 825 778 47 19 0.40Total . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6,662 6,510 152 84 0.55
– Quantity zero.1Includes races other than white and black.
NOTE: NHANES II is the Second National Health and Nutrition Examination Survey.
Page 10 [ Series 1, No. 38

Table 4. Expected number of survivors and decedents based on U.S. vital statistics data compared with observed number of decedentsfrom 1976–78 in the NHANES II Mortality Study according to race, sex, and age for selected race groups
Race, sex, and age groupNumber
examined
Expectednumber ofsurvivors
Expectednumber ofdecedents
Observednumber ofdecedents
Ratio ofobserved to
expected
White male
30–39 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 549 547 2 – –40–49 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 442 439 3 3 1.0050–59 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 455 447 8 2 0.2560–64 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 572 551 21 14 0.6765–69 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 428 406 22 15 0.6870–75 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 329 305 24 12 0.50Total . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2,775 2,695 80 46 0.58
White female
30–39 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 602 601 1 2 2.0040–49 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 457 455 2 – –50–59 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 503 499 4 3 0.7560–64 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 588 578 10 5 0.5065–69 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 517 504 13 10 0.7770–75 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 410 394 16 6 0.38Total . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3,077 3,031 46 26 0.57
Black male
30–39 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 62 61 1 – –40–49 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 39 38 1 – –50–59 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 47 45 2 – –60–64 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 52 49 3 4 1.3365–69 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 48 44 4 3 0.7570–75 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 37 33 4 – –Total . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 285 270 15 7 0.47
Black female
30–39 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 82 82 – – . . .40–49 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 72 71 1 1 1.0050–59 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 74 72 2 – –60–64 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 60 58 2 1 0.5065–69 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 55 53 2 1 0.5070–75 years . . . . . . . . . . . . . . . . . . . . . . . . . . . 38 35 3 1 0.33Total . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 381 371 10 4 0.40
– Quantity zero.
. . . Category not applicable.
NOTE: NHANES II is the Second National Health and Nutrition Examination Survey.
Series 1, No. 38 [ Page 11

Table 5. Number of participants in the NHANES II Mortality Study by mortality status at end of follow-up in 1992 according to sex and age atbaseline for all races combined
Sex and age group Total
Status at follow-up
Assumed alive1 Decedents
Number Percent Number Percent
Male2
30–39 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 871 832 95.5 39 4.540–49 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 691 629 91.0 62 9.050–59 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 700 565 80.7 135 19.360–64 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 877 548 62.5 329 37.565–69 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 697 339 48.6 358 51.470–75 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 513 178 34.7 335 65.3Total . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4,349 3,091 71.1 1,258 28.9
Female2
30–39 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 988 968 98.0 20 2.040–49 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 766 719 93.9 47 6.150–59 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 795 701 88.2 94 11.860–64 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 926 727 78.5 199 21.565–69 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 799 565 70.7 234 29.370–75 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 627 334 53.3 293 46.7Total . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4,901 4,014 81.9 887 18.1
Total2
30–39 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1,859 1,800 96.8 59 3.240–49 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1,457 1,348 92.5 109 7.550–59 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1,495 1,266 84.7 229 15.360–64 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1,803 1,275 70.7 528 29.365–69 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1,496 904 60.4 592 39.670–75 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1,140 512 44.9 628 55.1Total . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9,250 7,105 76.8 2,145 23.2
1Not found to be deceased, therefore, assumed alive.2Includes races other than white and black.
NOTE: NHANES II is the Second National Health and Nutrition Examination Survey.
Page 12 [ Series 1, No. 38

Table 6. Number of participants in the NHANES II Mortality Study by mortality status at end of follow-up in 1992 according to race, sex, andage at baseline for selected race groups
Race, sex, and age group Total
Status at follow-up
Assumed alive1 Decedents
Number Percent Number Percent
White male
30–39 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 750 719 95.9 31 4.140–49 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 610 560 91.8 50 8.250–59 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 611 500 81.8 111 18.260–64 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 791 490 62.0 301 38.065–69 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 605 285 47.1 320 52.970–75 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 448 152 33.9 296 66.1Total . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3,815 2,706 70.9 1,109 29.1
White female
30–39 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 860 843 98.0 17 2.040–49 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 654 618 94.5 36 5.550–59 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 677 595 87.9 82 12.160–64 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 828 653 78.9 175 21.165–69 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 696 491 70.6 205 29.470–75 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 559 296 53.0 263 47.0Total . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4,274 3,496 81.8 778 18.2
Black male
30–39 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 98 91 92.9 7 7.140–49 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63 52 82.5 11 17.550–59 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 79 56 70.9 23 29.160–64 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78 52 66.7 26 33.365–69 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 73 41 56.2 32 43.870–75 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58 23 39.7 35 60.3Total . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 449 315 70.2 134 29.8
Black female
30–39 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 111 108 97.3 3 2.740–49 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 98 88 89.8 10 10.250–59 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 103 92 89.3 11 10.760–64 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 85 66 77.6 19 22.465–69 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 88 61 69.3 27 30.770–75 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64 36 56.2 28 43.8Total . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 549 451 82.1 98 17.8
1Not found to be deceased, therefore, assumed alive.
NOTE: NHANES II is the Second National Health and Nutrition Examination Survey.
Series 1, No. 38 [ Page 13

Appendix I
NHANES II baseline examination components for participants 30–75 years of age(1976–80)
Examination components
Test group
Bile acids Glucose tolerance
Urine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X XBody measurements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X XPhysician examination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X XVenipuncture . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X XDietary interview . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X XAllergy test . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X XElectrocardiogram . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X XChest and neck x rays . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X XBack x ray
30–75 years for men . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X X50–75 years for women . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X X
Glucose tolerance test . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . XBile acids test: 35–75 years only . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X
NOTE: NHANES II is the Second National Health and Nutrition Examination Survey.
Page 14 [ Series 1, No. 38

Appendix II
NHANES II baseline blood and urine assessments by specimen types for participants30–75 years of age (1976–80)
Test group
Bile acids1 Glucose tolerance
Whole blood
Lead: Odd-numbered examinees . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X XCarboxyhemoglobin: Even-numbered examinees . . . . . . . . . . . . . . . . . . . . . . . . . . . X XProtoporphyrin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X XRed blood cell folate2 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X X
Serum
Ferritin2 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X XBile acids: 35–75 years only . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . XCholesterol . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X XTriglyceride . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . XHigh density lipoprotein . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . XPesticides: All examinees . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . XCreatinine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X XSyphilis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X XIron . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X XTotal iron binding capacity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X XFolate2 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X XVitamin B122 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X XCopper . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X XZinc . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X XAlbumin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X XGlucose tolerance 75 gram load at 0-, 1-, and 2-hour intervals . . . . . . . . . . . . . . . . . . XVitamin C . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X X
Urine
N-Multistix . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X XGonorrhea:
30–40 years for both sexes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X X30–40 years for men . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X
Microscopy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . XSpecific gravity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . XPesticides . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . X
1Bilirubin, SGOT, and alkaline phosphatase performed only on those samples with elevated bile acids.2Performed only on those samples with abnormal complete blood count, hemoglobin, hematocrit, or mean corpuscular volume.
NOTE: NHANES II is the Second National Health and Nutrition Examination Survey.
Series 1, No. 38 [ Page 15

Appendix III
NHANES II baseline pesticide residue and metabolite determinations for participants30–75 years of age (1976–80)
Serum Urine
Hexachlorobenzene alpha Monocarboxylic acidtrans Nonachlor Dicarboxylic acidDDT and Associated Analogs 3,5,6-Trichloro-2-pyridinolalpha-BHC Isopropoxyphenolgamma-BHC Carbofuranphenolbeta-BHC 3-Ketocarbofurandelta-BHC DicambaAldrin 2,4-DDieldrin PentachlorophenolEndrin para-NitrophenolHeptachlor alpha-NaphtholHeptachlor Epoxide DMTPOxychlordane DETPMirex DMDTP
DEDTPDMPDEP2,4,5-TSilvex2,4,5-Trichlorophenol
NOTE: NHANES II is the Second National Health and Nutrition Examination Survey.
Page 16 [ Series 1, No. 38

Vital and Health Statisticsseries descriptions
e
est
SERIES 1. Programs and Collection Procedures—These reports describethe data collection programs of the National Center for HealthStatistics. They include descriptions of the methods used tocollect and process the data, definitions, and other materialnecessary for understanding the data.
SERIES 2. Data Evaluation and Methods Research—These reports arestudies of new statistical methods and include analyticaltechniques, objective evaluations of reliability of collected data,and contributions to statistical theory. These studies also includeexperimental tests of new survey methods and comparisons ofU.S. methodology with those of other countries.
SERIES 3. Analytical and Epidemiological Studies—These reports presentanalytical or interpretive studies based on vital and healthstatistics. These reports carry the analyses further than theexpository types of reports in the other series.
SERIES 4. Documents and Committee Reports—These are final reports ofmajor committees concerned with vital and health statistics anddocuments such as recommended model vital registration lawsand revised birth and death certificates.
SERIES 5. International Vital and Health Statistics Reports—Thesereports are analytical or descriptive reports that compare U.S.vital and health statistics with those of other countries or presentother international data of relevance to the health statisticssystem of the United States.
SERIES 6. Cognition and Survey Measurement—These reports are fromthe National Laboratory for Collaborative Research in Cognitionand Survey Measurement. They use methods of cognitive sciencto design, evaluate, and test survey instruments.
SERIES 10. Data From the National Health Interview Survey—Thesereports contain statistics on illness; unintentional injuries;disability; use of hospital, medical, and other health services; anda wide range of special current health topics covering manyaspects of health behaviors, health status, and health careutilization. They are based on data collected in a continuingnational household interview survey.
SERIES 11. Data From the National Health Examination Survey, theNational Health and Nutrition Examination Surveys, and theHispanic Health and Nutrition Examination Survey—Datafrom direct examination, testing, and measurement onrepresentative samples of the civilian noninstitutionalizedpopulation provide the basis for (1) medically defined totalprevalence of specific diseases or conditions in the United Statesand the distributions of the population with respect to physical,physiological, and psychological characteristics, and (2) analysesof trends and relationships among various measurements andbetween survey periods.
SERIES 12. Data From the Institutionalized Population Surveys—Discontinued in 1975. Reports from these surveys are included inSeries 13.
SERIES 13. Data From the National Health Care Survey—These reportscontain statistics on health resources and the public’s use ofhealth care resources including ambulatory, hospital, andlong-term care services based on data collected directly fromhealth care providers and provider records.
SERIES 14. Data on Health Resources: Manpower and Facilities—Discontinued in 1990. Reports on the numbers, geographicdistribution, and characteristics of health resources are nowincluded in Series 13.
SERIES 15. Data From Special Surveys—These reports contain statistics onhealth and health-related topics collected in special surveys thatare not part of the continuing data systems of the NationalCenter for Health Statistics.
SERIES 16. Compilations of Advance Data From Vital and HealthStatistics—Advance Data Reports provide early release ofinformation from the National Center for Health Statistics’ healthand demographic surveys. They are compiled in the order inwhich they are published. Some of these releases may befollowed by detailed reports in Series 10–13.
SERIES 20. Data on Mortality —These reports contain statistics on mortalitythat are not included in regular, annual, or monthly reports.Special analyses by cause of death, age, other demographicvariables, and geographic and trend analyses are included.
SERIES 21. Data on Natality, Marriage, and Divorce—These reportscontain statistics on natality, marriage, and divorce that are notincluded in regular, annual, or monthly reports. Special analysesby health and demographic variables and geographic and trendanalyses are included.
SERIES 22. Data From the National Mortality and NatalitySurveys—Discontinued in 1975. Reports from these samplesurveys, based on vital records, are now published in Series 20or 21.
SERIES 23. Data From the National Survey of Family Growth—Thesereports contain statistics on factors that affect birth rates,including contraception, infertility, cohabitation, marriage,divorce, and remarriage; adoption; use of medical care for familyplanning and infertility; and related maternal and infant healthtopics. These statistics are based on national surveys of womenof childbearing age.
SERIES 24. Compilations of Data on Natality, Mortality, Marriage,Divorce, and Induced Terminations of Pregnancy—Theseinclude advance reports of births, deaths, marriages, and divorcbased on final data from the National Vital Statistics System thawere published as supplements to theMonthly Vital StatisticsReport(MVSR). These reports provide highlights and summariesof detailed data subsequently published inVital Statistics of theUnited States. Other supplements to the MVSR published hereprovide selected findings based on final data from the NationalVital Statistics System and may be followed by detailed reportsin Series 20 or 21.
For answers to questions about this report or for a list of reports published inthese series, contact:
Data Dissemination BranchNational Center for Health StatisticsCenters for Disease Control and Prevention6525 Belcrest Road, Room 1064Hyattsville, MD 20782-2003
(301) 436–8500E-mail: [email protected]:www.cdc.gov/nchswww/

DEPARTMENT OFHEALTH & HUMAN SERVICES
Centers for Disease Control and PreventionNational Center for Health Statistics6525 Belcrest RoadHyattsville, Maryland 20782-2003
OFFICIAL BUSINESSPENALTY FOR PRIVATE USE, $300
DHHS Publication No. (PHS) 99-1314, Series 1, No. 389-0345 (6/99)
STANDARD MAIL (A)POSTAGE & FEES PAID
CDC/NCHSPERMIT NO. G-284