
Visual outcome of patients with central eales disease
3
Reprints: Sandeep Saxena, MD, G-19 River Bank Colony, Lucknow, 226018 U.P., India. The authors are from the Retina Service, Department of Ophthalmology, King George’s Medical College, University of Lucknow, Lucknow (U.P.), India. Acknowledgment Supported by grants 8/47(32)96-EMR.1 and 13(7175-A)/97-Pool from the Council of Scientific and Industrial Research, New Delhi, India. ORIGINAL ARTICLE ANN OPHTHALMOL. 2001; 33(4):300–302 300 E ales disease is an idiopathic obliterative vasculopa- thy that primarily affects the peripheral retina in young adults. It is characterized by perivascular sheath- ing, peripheral nonperfusion, and neovascularization. 1 Visual loss results from recurrent vitreous hemorrhages and their sequelae. 2 The disease afflicts people world- wide, but for unknown reasons, it is more commonly found in patients from India. 3 Immune-mediated mech- anisms have been proposed in the etiopathogenesis of this condition. 4 It appears to be an immunologic reac- tion triggered by an exogenous exposure. 5 Central retinal vein occlusion (CRVO) in young adults is considered uncommon and is probably rare. 6 Central Eales disease, occurring between the ages of 20 and 40 years, is much less common than the peripher- al type and is usually unilateral. The optic disc is swollen; the veins are engorged and tortuous; and mul- tiple hemorrhages occur, spreading to the periphery. 7 We undertook a tertiary care center-based retro- spective study to evaluate the visual outcome of patients with central Eales disease. Patients & Methods A retrospective study was undertaken of patients with central Eales disease in our retina clinic, for whom there was accurate documentation of ophthalmic fea- tures. Eleven consecutive cases were included in this study. Central Eales disease was defined as optic disc edema with dilated retinal veins, tortuosity of the major retinal veins, and variable degree of retinal hemor- Sandeep Saxena, MD, & Dipak Kumar, MD Visual Outcome of Patients With Central Eales Disease A retrospective study was undertaken to evaluate visual outcome of 11 patients (13 eyes) with central Eales disease (median age, 22 years). All patients had raised erythrocyte sedimentation rates. Non- ischemic disease developed in 11 eyes, and 2 eyes had ischemic dis- ease. All patients were administered systemic corticosteroid therapy. One patient with ischemic disease also received panretinal photocoagulation. Final visual acuity of 6/6 was achieved in 7 eyes in the nonischemic group. ABSTRACT
-
Upload
sandeep-saxena -
Category
Documents
-
view
215 -
download
2
Transcript of Visual outcome of patients with central eales disease

Reprints:Sandeep Saxena, MD, G-19 River Bank Colony, Lucknow, 226018 U.P., India.
The authors are from the Retina Service, Department of Ophthalmology, King George’sMedical College, University of Lucknow, Lucknow (U.P.), India.
AcknowledgmentSupported by grants 8/47(32)96-EMR.1 and 13(7175-A)/97-Pool from the Council ofScientific and Industrial Research, New Delhi, India.
O R I G I N A L A R T I C L E
ANN OPHTHALMOL. 2001;33(4):300–302300
Eales disease is an idiopathic obliterative vasculopa-thy that primarily affects the peripheral retina in
young adults. It is characterized by perivascular sheath-ing, peripheral nonperfusion, and neovascularization.1
Visual loss results from recurrent vitreous hemorrhagesand their sequelae.2 The disease afflicts people world-wide, but for unknown reasons, it is more commonlyfound in patients from India.3 Immune-mediated mech-anisms have been proposed in the etiopathogenesis ofthis condition.4 It appears to be an immunologic reac-tion triggered by an exogenous exposure.5
Central retinal vein occlusion (CRVO) in youngadults is considered uncommon and is probably rare.6
Central Eales disease, occurring between the ages of 20and 40 years, is much less common than the peripher-al type and is usually unilateral. The optic disc isswollen; the veins are engorged and tortuous; and mul-tiple hemorrhages occur, spreading to the periphery.7
We undertook a tertiary care center-based retro-spective study to evaluate the visual outcome ofpatients with central Eales disease.
Patients & MethodsA retrospective study was undertaken of patients withcentral Eales disease in our retina clinic, for whomthere was accurate documentation of ophthalmic fea-tures. Eleven consecutive cases were included in thisstudy. Central Eales disease was defined as optic discedema with dilated retinal veins, tortuosity of the majorretinal veins, and variable degree of retinal hemor-
Sandeep Saxena, MD, & Dipak Kumar, MD
Visual Outcome of PatientsWith Central Eales Disease
A retrospective study was undertaken to evaluate visual outcome of
11 patients (13 eyes) with central Eales disease (median age, 22
years). All patients had raised erythrocyte sedimentation rates. Non-
ischemic disease developed in 11 eyes, and 2 eyes had ischemic dis-
ease. All patients were administered systemic corticosteroid
therapy. One patient with ischemic disease also received panretinal
photocoagulation. Final visual acuity of 6/6 was achieved in 7 eyes
in the nonischemic group.
A B S T R A C T

rhages, according to previously published criteria6 (Fig1). Systemic disease such as diabetes mellitus, sicklecell hemoglobinopathy, blood dyscrasias, sarcoidosis,collagen vacular disorders, and hypercholesterolemiawere ruled out with the use of a careful medical historyand appropriate laboratory tests. All patients hadundergone full ophthalmologic examination, whichincluded Snellen visual acuity, slit-lamp biomicroscopy,indirect ophthalmoscopy, and fluorescein angiography.
The eyes were categorized as having ischemic ornonischemic disease. The disease was classified asischemic if any of the following events occurred at anytime during the course of the disease: (1) relative affer-ent pupillary defect and decrease of visual acuity to lessthan 3/60; (2) severe degree of retinal ischemia on fluo-rescein angiograms, and (3) ocular neovascularization(formation of new iris and/or retinal vessels). Visualacuity was graded as follows: grade 1 (excellent), 6/6 orbetter; grade 2 (good), 6/9 to 6/12; grade 3 (fair), 6/18 to6/36; and grade 4 (poor), 6/60 or worse.8
All the patients were administered 60 mg of oralprednisolone for 1 week, followed by 40 mg of pred-nisolone for 3 weeks, with the dosage tapered there-after. A successful visual outcome was defined asmaintenance of visual acuity of 6/12 or better, orimprovement of visual acuity by 1 or more grades, bythe last clinic visit. Patients who did not fulfill thesecriteria were defined as having poor visual outcome.9,10
Cases with ischemic disease were also treated withpanretinal photocoagulation.
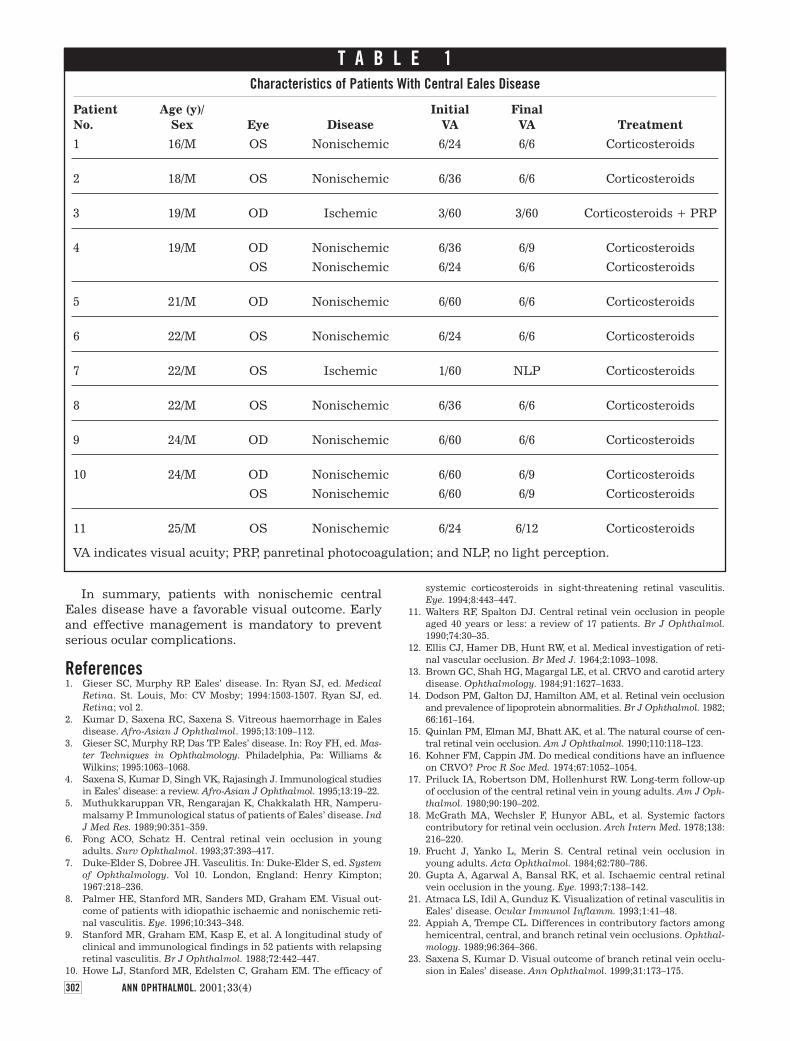
ResultsPatients with Eales disease included in this studywere aged between 16 and 25 years (median age, 22years), and all were male. Nine patients (81.8%) hadunilateral involvement, and 2 patients had bilateraldisease. Hence, 13 eyes were included in this study.The patients and their characteristics at presentationare described in Table 1.
All the patients had a raised erythrocyte sedimenta-tion rate (ESR) of more than 20 mm/h (Westergren). Themedian follow-up period was 13 months (range, 6 monthsto 19 months). Of the 13 eyes, 11 eyes had nonischemicdisease and 2 eyes had ischemic disease. One patient(patient 3) was treated with early prophylactic panretinalphotocoagulation. However, visual recovery was notachieved. Another patient (patient 7) did not return forfollow-up 1 month after initial presentation but thenreturned for examination after 14 months with phthisisbulbi and no light perception.
DiscussionCentral retinal vein occlusion in young adults has beenthought to be a different entity from CRVO in olderpatients and is probably a nonspecific change thatresults from a number of individual causes or a combi-nation of causes.6 Optic disc swelling in youngerpatients with CRVO is more common and moremarked than in elderly individuals. The reason forthis, in the absence of overt ischemia, is not clear but
may reflect the greater number of viable axons in ayounger eye, with more axoplasm therefore beingpassed along the optic nerve.11 Previous reports haveshown that 8% to 19.8% of CRVOs are found in patientsunder 40 years of age.12-18 The disease has been report-ed to be frequently mild and nonischemic,10 althoughoccurrence of ischemic CRVO is not unknown.19,20
Atmaca et al21 reported central Eales disease in 1.8%of 565 eyes in their study. Appiah and Trempe22 foundan association between ESR and CRVO. They hypoth-esized that the elevated ESR reflected changes inshear forces and viscosity of plasma that may have ledto hemodynamic changes at the lamina cribrosa andresulted in CRVO. Branch retinal vein occlusion inEales disease has been found to have a favorable visu-al outcome.23
The most notable finding in the present study wasthe young age (median, 22 years) at the time of pre-sentation. Erythrocyte sedimentation rates wereincreased in all patients. The typical fundus appear-ance was unilateral optic disc swelling with a moder-ate degree of retinal hemorrhages, but retinalischemia of any severity was uncommon. An initialdecrease in visual acuity resulted from associatedmacular edema. All the patients with nonischemiccentral Eales disease responded to systemic corticos-teroid therapy, and grades 1 and 2 visual acuity wereachieved in 7 and 4 eyes, respectively. The efficacy ofsystemic steroids in sight-threatening retinal vasculi-tis has been documented.10 Steroids may help inreducing inflammatory cell infiltrates around theoptic nerve and, therefore, improve blood flowthrough the CRVO. This, in turn, may reduce cystoidmacular edema and improve visual acuity.6 In ourstudy, eyes with ischemic disease also showed multi-ple cotton-wool spots at the time of presentation, andsevere retinal ischemia was evident on fluoresceinangiograms. Panretinal photocoagulation preventeddevelopment of neovascular glaucoma in 1 eye. Earlyprophylactic panretinal photocoagulation has beensuggested by Gupta et al.20 The patient who did notreturn for follow-up until 14 months after initial treat-ment showed a rapid downhill course.
ANN OPHTHALMOL. 2001;33(4) 301
Fig 1.—Fluorescein angiogram showing central Eales disease.
In summary, patients with nonischemic centralEales disease have a favorable visual outcome. Earlyand effective management is mandatory to preventserious ocular complications.
References1. Gieser SC, Murphy RP. Eales’ disease. In: Ryan SJ, ed. Medical
Retina. St. Louis, Mo: CV Mosby; 1994:1503-1507. Ryan SJ, ed.Retina; vol 2.
2. Kumar D, Saxena RC, Saxena S. Vitreous haemorrhage in Ealesdisease. Afro-Asian J Ophthalmol. 1995;13:109–112.
3. Gieser SC, Murphy RP, Das TP. Eales’ disease. In: Roy FH, ed. Mas-ter Techniques in Ophthalmology. Philadelphia, Pa: Williams &Wilkins; 1995:1063–1068.
4. Saxena S, Kumar D, Singh VK, Rajasingh J. Immunological studiesin Eales’ disease: a review. Afro-Asian J Ophthalmol. 1995;13:19–22.
5. Muthukkaruppan VR, Rengarajan K, Chakkalath HR, Namperu-malsamy P. Immunological status of patients of Eales’ disease. IndJ Med Res. 1989;90:351–359.
6. Fong ACO, Schatz H. Central retinal vein occlusion in youngadults. Surv Ophthalmol. 1993;37:393–417.
7. Duke-Elder S, Dobree JH. Vasculitis. In: Duke-Elder S, ed. Systemof Ophthalmology. Vol 10. London, England: Henry Kimpton;1967:218–236.
8. Palmer HE, Stanford MR, Sanders MD, Graham EM. Visual out-come of patients with idiopathic ischaemic and nonischemic reti-nal vasculitis. Eye. 1996;10:343–348.
9. Stanford MR, Graham EM, Kasp E, et al. A longitudinal study ofclinical and immunological findings in 52 patients with relapsingretinal vasculitis. Br J Ophthalmol. 1988;72:442–447.
10. Howe LJ, Stanford MR, Edelsten C, Graham EM. The efficacy of
systemic corticosteroids in sight-threatening retinal vasculitis.Eye. 1994;8:443–447.
11. Walters RF, Spalton DJ. Central retinal vein occlusion in peopleaged 40 years or less: a review of 17 patients. Br J Ophthalmol.1990;74:30–35.
12. Ellis CJ, Hamer DB, Hunt RW, et al. Medical investigation of reti-nal vascular occlusion. Br Med J. 1964;2:1093–1098.
13. Brown GC, Shah HG, Magargal LE, et al. CRVO and carotid arterydisease. Ophthalmology. 1984;91:1627–1633.
14. Dodson PM, Galton DJ, Hamilton AM, et al. Retinal vein occlusionand prevalence of lipoprotein abnormalities. Br J Ophthalmol. 1982;66:161–164.
15. Quinlan PM, Elman MJ, Bhatt AK, et al. The natural course of cen-tral retinal vein occlusion. Am J Ophthalmol. 1990;110:118–123.
16. Kohner FM, Cappin JM. Do medical conditions have an influenceon CRVO? Proc R Soc Med. 1974;67:1052–1054.
17. Priluck IA, Robertson DM, Hollenhurst RW. Long-term follow-upof occlusion of the central retinal vein in young adults. Am J Oph-thalmol. 1980;90:190–202.
18. McGrath MA, Wechsler F, Hunyor ABL, et al. Systemic factorscontributory for retinal vein occlusion. Arch Intern Med. 1978;138:216–220.
19. Frucht J, Yanko L, Merin S. Central retinal vein occlusion inyoung adults. Acta Ophthalmol. 1984;62:780–786.
20. Gupta A, Agarwal A, Bansal RK, et al. Ischaemic central retinalvein occlusion in the young. Eye. 1993;7:138–142.
21. Atmaca LS, Idil A, Gunduz K. Visualization of retinal vasculitis inEales’ disease. Ocular Immunol Inflamm. 1993;1:41–48.
22. Appiah A, Trempe CL. Differences in contributory factors amonghemicentral, central, and branch retinal vein occlusions. Ophthal-mology. 1989;96:364–366.
23. Saxena S, Kumar D. Visual outcome of branch retinal vein occlu-sion in Eales’ disease. Ann Ophthalmol. 1999;31:173–175.
ANN OPHTHALMOL. 2001;33(4)302
T A B L E 1Characteristics of Patients With Central Eales Disease
PatientNo.
1
2
3
4
5
6
7
8
9
10
11
VA indicates visual acuity; PRP, panretinal photocoagulation; and NLP, no light perception.
Age (y)/Sex
16/M
18/M
19/M
19/M
21/M
22/M
22/M
22/M
24/M
24/M
25/M
Eye
OS
OS
OD
OD
OS
OD
OS
OS
OS
OD
OD
OS
OS
Disease
Nonischemic
Nonischemic
Ischemic
Nonischemic
Nonischemic
Nonischemic
Nonischemic
Ischemic
Nonischemic
Nonischemic
Nonischemic
Nonischemic
Nonischemic
InitialVA
6/24
6/36
3/60
6/36
6/24
6/60
6/24
1/60
6/36
6/60
6/60
6/60
6/24
FinalVA
6/6
6/6
3/60
6/9
6/6
6/6
6/6
NLP
6/6
6/6
6/9
6/9
6/12
Treatment
Corticosteroids
Corticosteroids
Corticosteroids + PRP
Corticosteroids
Corticosteroids
Corticosteroids
Corticosteroids
Corticosteroids
Corticosteroids
Corticosteroids
Corticosteroids
Corticosteroids
Corticosteroids


















