Viscoelastic Response of the Thorax under Dynamic Belt Loading · Viscoelastic Response of the...
13
Viscoelastic Response of the Thorax under Dynamic Belt Loading R. S. Salzar, C. R. Bass, D. Lessley, J. R. Crandall, R. W. Kent, J. R. Bolton The University of Virginia, Center for Applied Biomechanics, 1011 Linden Ave., Charlottesville, VA 22902 USA ABSTRACT Three post-mortem human surrogates (PMHS) were mounted to a stationary apparatus that supported the spine and shoulders in a configuration comparable to that seen in a 48 km/h automobile sled test at the time of maximum chest deformation. A belt restraint was positioned across the anterior torso with attachments at D-ring and buckle locations based on the geometry of a mid-sized sedan. The belt was attached to a trolley driven by a hydraulic ram linked to a universal test machine. Ramp and hold experiments were conducted at rates of 0.5 m/s, 0.9 m/s, and 1.2 m/s and hold times of 60 seconds. Ramp-hold displacement waveforms of up to 20% of the chest depth were applied to the chest while the resulting belt loads and spinal reaction loads were recorded. These data were used to identify parameters in a 7-parameter thoracic structural model mathematically analogous to a viscoelastic material model. A final test with 40% deflection was performed at the completion of the loading sequence. Model fits to ramps of different magnitudes indicated that the assumption of temporal linearity was reasonable over the range of inputs in this study. In agreement with previous studies, the spatial (force-deflection) response was only slightly non-linear, indicating that a fully linear model would be reasonable up to the deflection levels used here. Pronounced variability in the instantaneous elastic behavior was observed, among the three test subjects; the relaxation behavior exhibited less variability. Keywords: cadavers, thorax, safety belts, models SEVENTY PERCENT OF BLUNT CHEST trauma occurs during motor vehicle crashes (Wang et al., 2000) and thoracic injury is the primary cause of death in 30% of traffic deaths (Mulligan et al., 1994). Further, serious thoracic injuries have societal consequences including lost wages and health costs. Thoracic deformation from anterior loading is generally accepted as the best predictor of chest injury in frontal crashes (Kroell et al., 1974, Kent et al., 2001). The National Highway Traffic Safety Administration (NHSTA) specifies a maximum allowable value of chest deformation as recorded by dummies in frontal crash tests (CFR 49, Part 571, Federal Motor Vehicle Safety Standard (FMVSS) 208). To control thoracic deformations from blunt trauma, it is important to understand the interaction of belt restraints with the thorax. However, owing to the complex interactions between the skin, sternum/ribs, interstitial tissues, and internal organs, deriving systemic response from component response is difficult. This difficulty is compounded by the limitations in the availability of well- characterized constitutive and geometric properties for use in detailed thoracic finite element (FE) models. One of the earliest thoracic characterization studies focused on thoracic hub loading from a 15 cm diameter circular impactor loading the mid-sternum of post-mortem human specimens (PMHS) (Lobdell et al., 1973, Kroell et al. 1974) – a loading condition intended to represent an unrestrained occupant impacting the steering wheel hub; this condition is not representative of today’s restraint system loading for belted occupants. Force-deflection corridors generated using this impact data apply only for the test conditions under which they were generated, which typically involve impacts at speeds much higher (4.3 m/s to 6.7 m/s) than those observed in the current restrained environment. Further, the resulting impact between the hub and the sternum of the cadaver generates sternal acceleration levels on the order of 1000 g, which results in response corridors that are dominated by the inertia of the sternum rather than by the elastic and viscous characteristics of the chest (Kent et al. 2004). An occupant subjected to restraint loading ideally does not experience mid-thorax impact. So, the peak acceleration of the sternum is much lower and the force-deflection characteristics of the thorax are determined by the elastic and viscous response of the thorax and the inertia of the anterior components, including sternum, rib structure, musculature and flesh. Models based on the inertially IRCOBI Conference – Bern (Switzerland) – September 2008 73
Transcript of Viscoelastic Response of the Thorax under Dynamic Belt Loading · Viscoelastic Response of the...

Viscoelastic Response of the Thorax under Dynamic Belt Loading
R. S. Salzar, C. R. Bass, D. Lessley, J. R. Crandall, R. W. Kent, J. R. Bolton The University of Virginia, Center for Applied Biomechanics, 1011 Linden Ave., Charlottesville,
VA 22902 USA ABSTRACT Three post-mortem human surrogates (PMHS) were mounted to a stationary apparatus that supported the spine and shoulders in a configuration comparable to that seen in a 48 km/h automobile sled test at the time of maximum chest deformation. A belt restraint was positioned across the anterior torso with attachments at D-ring and buckle locations based on the geometry of a mid-sized sedan. The belt was attached to a trolley driven by a hydraulic ram linked to a universal test machine. Ramp and hold experiments were conducted at rates of 0.5 m/s, 0.9 m/s, and 1.2 m/s and hold times of 60 seconds. Ramp-hold displacement waveforms of up to 20% of the chest depth were applied to the chest while the resulting belt loads and spinal reaction loads were recorded. These data were used to identify parameters in a 7-parameter thoracic structural model mathematically analogous to a viscoelastic material model. A final test with 40% deflection was performed at the completion of the loading sequence. Model fits to ramps of different magnitudes indicated that the assumption of temporal linearity was reasonable over the range of inputs in this study. In agreement with previous studies, the spatial (force-deflection) response was only slightly non-linear, indicating that a fully linear model would be reasonable up to the deflection levels used here. Pronounced variability in the instantaneous elastic behavior was observed, among the three test subjects; the relaxation behavior exhibited less variability. Keywords: cadavers, thorax, safety belts, models SEVENTY PERCENT OF BLUNT CHEST trauma occurs during motor vehicle crashes (Wang et al., 2000) and thoracic injury is the primary cause of death in 30% of traffic deaths (Mulligan et al., 1994). Further, serious thoracic injuries have societal consequences including lost wages and health costs. Thoracic deformation from anterior loading is generally accepted as the best predictor of chest injury in frontal crashes (Kroell et al., 1974, Kent et al., 2001). The National Highway Traffic Safety Administration (NHSTA) specifies a maximum allowable value of chest deformation as recorded by dummies in frontal crash tests (CFR 49, Part 571, Federal Motor Vehicle Safety Standard (FMVSS) 208). To control thoracic deformations from blunt trauma, it is important to understand the interaction of belt restraints with the thorax. However, owing to the complex interactions between the skin, sternum/ribs, interstitial tissues, and internal organs, deriving systemic response from component response is difficult. This difficulty is compounded by the limitations in the availability of well-characterized constitutive and geometric properties for use in detailed thoracic finite element (FE) models. One of the earliest thoracic characterization studies focused on thoracic hub loading from a 15 cm diameter circular impactor loading the mid-sternum of post-mortem human specimens (PMHS) (Lobdell et al., 1973, Kroell et al. 1974) – a loading condition intended to represent an unrestrained occupant impacting the steering wheel hub; this condition is not representative of today’s restraint system loading for belted occupants. Force-deflection corridors generated using this impact data apply only for the test conditions under which they were generated, which typically involve impacts at speeds much higher (4.3 m/s to 6.7 m/s) than those observed in the current restrained environment. Further, the resulting impact between the hub and the sternum of the cadaver generates sternal acceleration levels on the order of 1000 g, which results in response corridors that are dominated by the inertia of the sternum rather than by the elastic and viscous characteristics of the chest (Kent et al. 2004). An occupant subjected to restraint loading ideally does not experience mid-thorax impact. So, the peak acceleration of the sternum is much lower and the force-deflection characteristics of the thorax are determined by the elastic and viscous response of the thorax and the inertia of the anterior components, including sternum, rib structure, musculature and flesh. Models based on the inertially
IRCOBI Conference – Bern (Switzerland) – September 2008 73

dominated hub tests have, however, have been used to design restraint systems (e.g. Viano et al., 1987, Lau et al., 1987, Crandall et al., 2000, Shaw et al., 2007). To characterize the elastic and viscous properties of the thorax, which are the primary structural aspects exercised by modern restraints, Kent et al. (2003, 2004) used a battery of ramp-and-hold displacement tests on PMHS. The specimens were positioned supine on the platform of a testing frame, and subjected to ramp-and-hold displacements using a circular hub, a load distributing belt, and a diagonal restraint belt at rates representative of those observed in restrained cadaver sled tests. The thorax was subjected to displacements of varying magnitudes, which were then held while the force relaxation was measured (Kent et al. 2003). From these tests, response corridors were developed that were not dominated by inertia (2004). Further, structural constants (analogous to material constants) were determined that apportion the elastic and viscous characteristics of the thorax (2003). These studies were, however, subject to some important limitations. The posterior boundary condition was a flat plate with a head block and subsequent studies have identified sensitivity in the response for reasonable ranges of uncertainty in those interactions (Murakami et al. 2006). Furthermore, the range of sternal displacement rates tested ranged from quasistatic (Arbogast et al. 2006) up to approximately 1 m/s. The test fixture used in the current investigation mitigates some of the limitations of these earlier studies. This test fixture allows each subject’s spine to be rigidly positioned and mounted without constraining the costo-vertebral or costo-transverse joints. By prescribing the level of kyphosis to each subject, and combining restraint anchorages in a geometric arrangement similar to current mid-sized sedans, a more realistic distribution of force across the upper abdomen, center sternum, and clavicle is assumed. The current tests also included higher sternal displacement rates. METHODS SPECIMENS AND SPECIMEN PREPARATION: Three (3) PMHS consisting of thorax with head/neck, pelvis, and proximal humeri and femurs were tested (Table 1). All specimens were frozen post-mortem and thawed for use. The specimens were intubated to allow for lung inflation before testing. The target population was 50th percentile males with an upper age limit of 75 years. The cadaver specimens were screened for Hepatitis A, B, C and HIV and for pre-existing pathology that may influence the thoracic properties. Pre-test radiographs and CT scans were taken to verify that specimens with acute or healed rib fractures or other pre-existing thoracic trauma were excluded from this study. Test procedures were approved by the University of Virginia cadaver institutional review board.
Table 1. Specimen Description
Test ID Sex Age Weight
(kg) Stature
(cm) Chest Depth
(mm) 1 (412) M 62 68.5 175.3 224 2 (413) M 54 68.0 175.3 217 3 (419) M 31 90.0 193.0 244
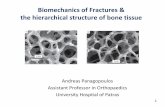
A table-top rig was employed in this test series similar to that used previously by Kent et al. (2004), but this study employed a different spinal boundary condition and a different torso orientation. For this series, alternating vertebral bodies of the test specimens were rigidly fixed using aluminum mounts that allowed free motion of the posterior costo-vertebral and costo-transverse joints. These mounts were attached to the test fixture through a series of threaded rods that allowed fine variations in the kyphosis or lordosis in the spine (Figure 1). The spinal curvature and the torso position were set to represent those at maximum forward excursion of the torso in a frontal impact sled test. This target yielded a torso pitch of 30° from vertical (in the sled, or horizontal on the test fixture) (Figure 1), with a normally kyphotic thorax spine curvature. Instrumentation: As shown in Table 2, the test specimens were instrumented with strain gages at several bony locations. These were used to identify any possible rib fractures during the test, and will be further used to validate finite element models. The loading table was instrumented with load cells under the spine and attached to the belt. A displacement sensor was used to determine belt actuator
74 IRCOBI Conference – Bern (Switzerland) – September 2008

motion. High-speed data was acquired through a TDAS G5 data acquisition system (DTS, Inc., Seal Beach, CA) at a sampling rate of 10 kHz with anti-aliasing hardware filters. Thoracic kinematic data was measured using a 16-camera Vicon MX™ 3-D motion capture system to track to motion of retro-reflective spherical targets mounted to the cadavers (Table 2) using a calibrated 3-D space lying within the cameras’ collective field of view. The calibration procedure, performed prior to the testing of each subject, established the position and orientation of cameras with respect to one another which was used to reconstruct the 3-D target locations from multiple 2-D camera images via a triangulation algorithm within the Vicon Nexus software package. Single and four-target clusters were secured to selected anatomical locations to facilitate the use of rigid body mechanics to determine the actual motion of the corresponding bone at each time step using a mathematical coordinate transformation (Lessley et al., 2008). Each cluster was tracked initially relative to a lab-fixed coordinate system; however relative motion between these local cluster coordinate systems (i.e. sternum and spine) was used to quantify deformation of the thorax. For this test, displacement data was sampled at 1000 Hz.
Table 2. Sensor Location and Type Sensor Location Vicon Marker Strain Gage
Right - - 1st rib Left - uniaxial Right 6-DOF uniaxial 4th rib Left 6-DOF uniaxial/uniaxial
on c-c junction Right 6-DOF uniaxial
Anterior Ribs
8th rib Left 6-DOF uniaxial Right 3-DOF uniaxial 4th rib Left 3-DOF uniaxial Right 3-DOF uniaxial
Lateral Ribs
8th rib Left 3-DOF uniaxial Right 6-DOF - 4th rib Left 6-DOF - Right 6-DOF uniaxial
Posterior Ribs
8th rib Left 6-DOF uniaxial
Sternum center 6-DOF rosette (inferior) distal 3-DOF - Unloaded (right)
proximal 3-DOF - distal 3-DOF
Clavicle
Loaded (left) proximal 3-DOF
rosette on posterior side
left 6-DOF - Acromion right 6-DOF - left 3-DOF - Humerus
right 3-DOF - Belt (Along CL) Multiple 3-DOF - Reference Frame Multiple 3-DOF - Reaction load cell Belt tension load cells (2) Head-block load cell String-potentiometer on belt actuator
IRCOBI Conference – Bern (Switzerland) – September 2008 75

30°30°
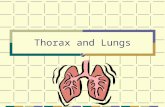
Figure 1. Spinal Fixation and Positioning Methodology TEST APPARATUS AND LOADING CONDITIONS: The PMHS were subjected to a series of diagonal belt loads designed to yield the force-deflection response sufficient to allow for the development of a quasilinear viscoelastic (QLV) structural model (Fung, 1993). A hydraulic master-slave cylinder arrangement with a material testing machine (Instron model 8874, Canton, Massachusetts) was used to generate chest deflection (Figure 2a) via cable-belt systems. All belts were constructed of ultra high molecular weight polyethylene (UHMWPE) fiber-reinforced sail cloth, which conforms to the chest similarly to a seatbelt, but did not elongate measurably during loading. This material was chosen rather than actual seatbelt webbing (which would stretch nominally 2%-4% in these tests) to isolate the thoracic response so that the measured force-deflection response would be a characteristic of the thorax rather than of the thorax in series with a deforming element. The use of this material will also presumably facilitate computational modeling of the test setup since the strain of the belt material in these tests is small. The diagonal belt anchor points were designed to reproduce the restraint anchors of the driver’s side of a typical late model 4-door sedan. The 5-cm-wide diagonal belt passed over the left shoulder and crossed the anterior thorax at an angle approximately 30° from the sagittal plane. The belt engaged the PMHS at the proximal third of the clavicle, crossed the midline approximately mid-sternum, and exited the body laterally at approximately the superior-inferior location of the 9th rib. The belt exited the left shoulder at an angle of approximately 60° from horizontal, representing the 30° forward pitch of the torso. Detailed positioning of the diagonal belt is shown in Figure 2b with individual test numbers in Table 3. Both the upper belt pre-tension and the lower belt pre-tension were set at approximately 8 N. Prior to the start of testing, each specimen’s lungs were inflated with 2.8 liters of air, and allowed to relax for 30 minutes. (a)
(b)
Figure 2 (a) Table-top Test Fixture Schematic; (b) Belt Placement Parameters Set and Recorded for Each Test: A - Upper Belt Edge to Top of Sternum, B - Lower Belt Edge to Bottom of Sternum, C - Subject Midline to Belt Centerline at the Level of Clavicle and Belt Intersection, D - Rib Number at Which Upper Belt Edge Crosses Lateral Aspect of Body.
A
B
C
D
76 IRCOBI Conference – Bern (Switzerland) – September 2008

To simulate the inertial loading of the arms onto the shoulder/clavicle complex, the distal humeri were loaded via cables. Each cable was preloaded to approximately 20N tension. Since the application of belt loading would generate an increase in the cable tension, which could possibly injure the shoulder complex, the cables were routed through a pulley and attached to a force-limiter (cf. Forman et al. 2005) that limited the force in each arm to 250 N. Each test specimen was subject to a battery of displacement-controlled tests designed to provide the information necessary for thoracic structural characterization. Two sternal deflection levels, measured as a percentage of chest depth as measured by CT, were used in the ramp-hold belt loadings to assess the temporal linearity of the viscoelastic model. Initially, a 10-cycle, 1-Hz sinusoid having the same deflection magnitude as the maximum ramp-hold test was applied to precondition the thorax. Next, the thorax of each PMHS was subjected to two ramp-hold displacement waveforms. The second ramp-hold on each PMHS was at a higher rate and a greater magnitude (Table 3). The third waveform was a sine wave at two frequencies, which was used to assess the model fit to the ramp-hold experiments. Finally, an injurious, or “failure”, ramp test was applied. Prior to the final test, palpation assessed the presence of rib fractures after each loading cycle. In the case that a fracture was identified, the test series was stopped for that specimen.
Table 3. Matrix of Test Conditions Belt Positioning Test
Number Waveform Speed Chest Compression
A (mm)
B (mm)
C (mm)
1.1 Precondition-sinusoid 1 Hz 15% of chest depth 11 122 54 1.2 Ramp and hold 0.5 m/s 10% of chest depth 12 107 50 1.3 Ramp and hold 1.0 m/s 15% of chest depth 15 103 56 1.4 Palpation indicated rib fracture – testing on specimen stopped 2.1 Precondition-sinusoid 1 Hz 15% of chest depth 39 48 70 2.2 Ramp and hold 0.5 m/s 10% of chest depth 56 28 75 2.3 Ramp and hold 1.0 m/s 15% of chest depth 46 40 70 2.4 Validation-sinusoid 1 Hz, 5 Hz 15% of chest depth 47 47 70 2.5 Step and hold-failure Belt Failure 2.6 Step and hold-failure Cable Failure 2.7 Step and hold-failure Belt Failure 2.8 Step and hold-failure 1.5 m/s 40% of chest depth 47 30 75 3.1 Precondition-sinusoid 1 Hz 20% of chest depth 6 ~0 85 3.2 3.3 Ramp and hold 0.5 m/s 15% of chest depth 65 ~0 86 3.4 Ramp and hold 1.0 m/s 20% of chest depth 64 ~0 87 3.5 Validation-sinusoid 1 Hz, 5 Hz 20% of chest depth 63 ~0 88 3.6 Step and hold-failure Pulley Failure 3.7 Step and hold-failure Cable Failure 3.8 Step and hold-failure Cable slipped off pulley 3.9 Step and hold-failure 1.5 m/s 40% of chest depth 42 25 70 STRUCTURAL MODELING: Displacements for this test series were obtained from Vicon markers on the center sternum of each PMHS, Vicon markers along the centerline of the belt, and the anchor pulleys. From this information, it was possible to calculate the posterior component of the tension in the two belt cables. This sternum displacement and the posterior component of the applied force from the belt were modeled using the formulation described below. The force response, F(δ,t), was analyzed for each ramp-and-hold test using a quasilinear viscoelastic mathematical framework as (Fung, 1993):
''
)'(),(0
dtdtd
ddFttGtF
et
redδ
δδ −= ∫ (1)
IRCOBI Conference – Bern (Switzerland) – September 2008 77

where Gred is a reduced relaxation function, Fe is the instantaneous elastic force, δ is the sternal displacement, t is the time, and t’ is a dummy convolution variable for integration. An exponential expression was used for the instantaneous elastic force:
]1[)( −= δδ Be eAF (2) where A and B are the instantaneous elastic parameters. The reduced relaxation function was expressed as a summed exponential function:
nt
nnred eGGtG τ/
4
1)( −
−∞ ∑+= where G1 + G2 + G3 + G4 +G∞ = 1 (3).
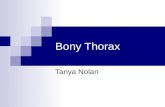
G∞ is the steady-state relaxation coefficient, and τn are the time constants corresponding to each of the relaxation coefficients, Gn. In this study, five relaxation coefficients were used. The hereditary integral (Eq. (1)) was numerically integrated while the instantaneous elastic parameters, A, B, the relaxation coefficients, Gn and G∞ and the time constants τn were found using a generalized reduced gradient technique (Solver from Microsoft Excel 2003) that minimized the sum-squared error between the model-predicted and measured force. For each specimen, all coefficients were determined from the ramp-hold test data and used to validate the viscoelastic parameters by predicting the response for either another ramp-hold test or an oscillatory validation test. The model fitting procedure is described in Kent et al. (2008). To simplify the model, the time constants were fixed after initial analysis. The time constants were optimized with the instantaneous elastic parameters and the relaxation coefficient for specimen 413. The approximate time constants determined from this model, τ1= 25 s, τ2= 0.25 s, τ3= 0.025 s, τ4= 0.001 s were fixed for the remainder of the analysis. The accuracy of the model was assessed using the sum-squared error and by using the correlation coefficient, R2, between the original relaxation function and simplified relaxation function. Model coefficients were determined for all six of the non-failure ramp-hold experiments as shown in Table 3. RESULTS The rate dependence of the three tested specimens is shown in Figure 3. Shown is the percent change in load at 10% sternal deflection between the lower-rate and higher-rate ramp-hold tests on each subject. Each specimen exhibits an increase in force response as the input displacement rate increases, illustrating the need for a rate-dependent model.
0
25
50
75
100
Specimen 1 Specimen 2 Specimen 3
Perc
enta
ge In
crea
se in
Loa
d .
Figure 3. Increase in Force at 10% Sternal Deflection Owing to Changes in Deflection Rate.
Though forces were recorded for 60 seconds duration, displacement data was recorded for 9 seconds to capture the dynamic response. Longer term displacements fell within the resolution of the displacement data, so extrapolation of trend lines were used to characterize the full 60 seconds of the test. This was performed by extrapolating 9 seconds to 60 seconds using the linear trend line of the last 5 seconds of displacement data. The end of displacement data acquisition was well into the hold portion of all displacement waveforms, however, so the extrapolation in this manner was virtually indistinguishable from a waveform with constant displacement for 9 sec < t < 60 sec (Figure 4).
78 IRCOBI Conference – Bern (Switzerland) – September 2008

240
245
250
255
260
265
0 5 10 15 20 25 30 35Time (s)
Dis
plac
emen
t (m
m)
0
10
20
30
40
50
60
Bel
t Ang
le (d
egre
es)
.
Sternum Displacement
Upper Belt angle
Lower Belt angle
Figure 4. Example of Extending Displacement Data via Trend-line (Test 2.2)
Reasonable model fits were obtained for all ramp-hold experiments (Figure 5). Pronounced force relaxation behavior was observed in the raw force-time data, which is reflected in the model relaxation coefficients. The weighting factor, G4, associated with the fastest time constant (τ4 = 0.001 s) was the largest, indicating substantial relaxation early in the loading event (Table 4). The steady-state coefficient, G∞, indicated that the long-time force would be expected to be approximately 3% of the force developed by a step (infinitely fast) displacement input. Both the model coefficients and the raw data indicate that the steady-state force is more than half of the peak force measured at the end of the ramp input. Overall, the models fit the data well, with R2 values ranging from 0.94 to 0.98. The instantaneous elastic functions indicated virtually linear behavior for two of the PMHS specimens (B ≈ 0 mm-1), but moderate non-linearity in the third. For this reason, the non-linear elastic function was retained, though little degradation in model fit would result from the use of a fully linear model in any case.
Table 4. Model Parameters and R2 Values for the Six Ramp-hold Tests. Test ID G1
(τ1 = 25 s) G2
(τ2 = 0.25 s) G3
(τ3 = 0.025 s) G4
(τ4 = 0.001 s) G∞ A
(kN/mm) B
(mm-1) R2
1.2 0.0153 0.0164 0.0149 0.9151 0.0383 3,511 6.60E-5 0.941.3 0.0266 0.0307 0.0508 0.8524 0.0396 9.626 0.018 0.982.2 0.0091 0.0148 1E-6 0.9482 0.0279 153,400 6.08E-6 0.942.3 0.0107 0.0126 0.0126 0.9357 0.0284 110,500 9.95E-6 0.963.3 0.0086 0.0102 0.0034 0.9442 0.0336 18.46 0.032 0.983.4 0.0192 0.0155 0.0146 0.9042 0.0466 14.82 0.031 0.97
Post hoc assessment of the model using the “validation” series of sine waves at two frequencies illustrates the model’s ability to predict reasonably a waveform substantially different from that used to generate the model parameters (Figure 6). The model do, however, appear to exhibit increased rate sensitivity compared to the experimental data, with the model predicting approximately 15% to 30% greater force at 5 Hz compared to 1 Hz, while the experimental data reflect a smaller increase. This may be due to non-uniqueness in the model parameter identification strategy, as discussed later. The instantaneous elastic functions for all ramp-hold experiments were averaged on a point-wise basis to generate a “mean” behavior for the 3 subjects tested here (Figure 7a). To develop an ‘averaged model’, a new coefficient is defined that calculates a line from each test’s instantaneous elastic force using the “least squares” method. In this averaging, a linear form of the instantaneous elastic force is defined as
δδ ⋅= *)( EF e (4) and replaces Eq(2) in the QLV formulation. These coefficients are shown in Table 5. The reduced relaxation functions were virtually indistinguishable across tests, so those functions are shown in a composite (Figure 7b). As illustrated in the plots, the elastic behavior in 4 of the 6 tests is very close to linear, with only the large, young subject exhibiting non-linearity. It can also be
IRCOBI Conference – Bern (Switzerland) – September 2008 79

seen that the relaxation occurs in a very short time, with the relaxation function being virtually constant for times longer than ~0.002 second. (a)
0
100
200
300
400
500
600
700
0 0.1 0.2 0.3 0.4 0.5Time (s)
Forc
e (N
)
0
5
10
15
20
25
30
35
40
45
50
Dis
plac
emen
t (m
m)
Original ForceModel ForceDisp
(b)
0
200
400
600
800
1000
1200
1400
1600
1800
0 0.1 0.2 0.3 0.4 0.5Time (s)
Forc
e (N
)
0
5
10
15
20
25
30
35
40
45
50
Dis
plac
emen
t (m
m)
Original ForceModel ForceDisp
(c)
0
200
400
600
800
1000
1200
1400
0 0.1 0.2 0.3 0.4 0.5Time (s)
Forc
e (N
)
0
5
10
15
20
25
30
35
40
45
50
Dis
plac
emen
t (m
m)
Original ForceModel ForceDisp
(d)
0
500
1000
1500
2000
2500
3000
0 0.1 0.2 0.3 0.4 0.5Time (s)
Forc
e (N
)
0
5
10
15
20
25
30
35
40
45
50
Dis
plac
emen
t (m
m)
Original ForceModel ForceDisp
(e)
0
500
1000
1500
2000
2500
0 0.1 0.2 0.3 0.4 0.5Time (s)
Forc
e (N
)
0
5
10
15
20
25
30
35
40
45
50
Dis
plac
emen
t (m
m)
Original ForceModel ForceDisp
(f)
0
500
1000
1500
2000
2500
3000
3500
4000
0 0.1 0.2 0.3 0.4 0.5Time (s)
Forc
e (N
)
0
5
10
15
20
25
30
35
40
45
50
Dis
plac
emen
t (m
m)
Original ForceModel ForceDisp
Figure 5. Optimization of QLV Parameters to Match the Experimental Data From (a) Test 1.2, (b) Test 1.3, (c) Test 2.2, (d) Test 2.3, (e) Test 3.3, and (f) Test 3.4.
80 IRCOBI Conference – Bern (Switzerland) – September 2008

(a)
0
100
200
300
400
500
600
700
800
900
0 0.1 0.2 0.3 0.4 0.5Time (s)
Forc
e (N
)
0
5
10
15
20
25
30
35
40
45
50
Dis
plac
emen
t (m
m)
Original ForceModel ForceDisp
(b)
0
500
1000
1500
2000
2500
0 1 2 3 4 5 6Time (s)
Forc
e (N
)
0
5
10
15
20
25
30
35
40
45
50
Dis
plac
emen
t (m
m)
Original ForceModel ForceDisp
(c)
0
500
1000
1500
2000
2500
3000
3500
0 1 2 3 4 5 6Time (s)
Forc
e (N
)
0
5
10
15
20
25
30
35
40
45
50
Dis
plac
emen
t (m
m)
Original ForceModel ForceDisp
Figure 6. (a) Model Fit Coefficients from Test 1.3 Predicting Test 1.2; (b) Model Fit Coefficients
from Test 2.3 Predicting Test 2.4; (c) Model Fit Coefficients from Test 3.4 Predicting Test 3.5.
IRCOBI Conference – Bern (Switzerland) – September 2008 81

(a)
0
20
40
60
80
100
120
0 10 20 30 40 50 60 70
Displacement (mm)
Inst
anta
neou
s El
astic
For
ce (k
N)
2.3
2.2
3.4
3.3
1.31.2
point-wiseaverage
(b)
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0.0001 0.001 0.01 0.1 1Time (s)
G(t)
1.21.32.22.33.33.4
Figure 7. (a) Instantaneous Elastic and (b) Reduced Relaxation Functions for all Ramp-Hold Experiments.
Table 5. Mean and Standard Deviation Values for Model Coefficients and E*, where the
Instantaneous Elastic Force (Fe) is defined here as E*(δ) G1 G2 G3 G4 G∞ E*
Mean 0.0149 0.0167 0.0160 0.917 0.0357 738.6 St. Dev. 0.00702 0.00721 0.0181 0.0358 0.00720 408.8
The average model coefficients are plotted against the validation data from Test 3.5 and the predicted response is shown in Figure 8. In addition, the model coefficients plus/minus one standard deviation are also plotted in Figure 8. As can be seen, the validation data of Test 3.5 lies between the bounds defined by plus and minus one standard deviation, and therefore the model coefficients can be considered a good representation of the thoracic characterization for the test population. However, the spread of the response implied by the standard deviation values is large, indicating a wide range of overall viscoelastic responses from the thoraces of the PMHS.
-2000
-1000
0
1000
2000
3000
4000
5000
0 1 2 3 4 5 6
Time (s)
Forc
e (N
) .
Original Force (HThorax3.5)Average Model Coefficients (R2=0.89)Ave. Coeff. - St. Dev. (R2=0.90)Ave. Coeff. + St. Dev. (R2=0.89)
Figure 8. Averaged Model Coefficients (Including ±1 St. Dev.) Predicting the Validation Data of Test
3.5. Note Validation Data is Bounded by the ± 1 St. Dev. Prediction Curves. DISCUSSION This study found substantial variability in the instantaneous elastic response among the three test subjects. Subject 3 was much younger and larger than the other two subjects, and generated an elastic stiffness response approximately 5 times greater. This is consistent with the findings of Kent et al. (2003), and consistent with the larger bony structures of this subject. The degree to which age affects
82 IRCOBI Conference – Bern (Switzerland) – September 2008

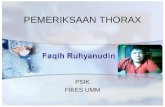
thoracic stiffness is not straightforward (e.g., Kent et al., 2005), but it is reasonable to expect that overall size is strongly correlated. The effect of aging on bone quality may have influenced the response of the two older specimens (Subject 1 and 2). These two older specimens exhibited the largest trend toward nonlinearity (see Table 4). As seen in Figure 7a, the instantaneous elastic force is lowest in the oldest specimen (Subject 1). As radiology was not available between tests, it is possible that progressive fractures may have occurred during ramp-hold tests that could not be identified through palpation. The role that fractures which cannot be identified through palpation play in the overall response of the thorax is still subject to debate, so this study recognizes this as a potential limitation of the model (Yoganandan et al., 2004; Kent et al., 2005). Interestingly, and again consistent with Kent et al. (2003), the reduced relaxation behavior was not substantially different among subjects. This may reflect the fact that thoracic response to restraint loading is dominated by the elastic characteristics of the chest, which are attributable primarily to the hard tissues of the thorax. Since these structures are larger in the larger subject, that subject generates a stiffer elastic response. The mechanisms of force relaxation in the thorax are less well understood. The bones, viscera, and joints of the body all exhibit force relaxation. Some of these behaviors may be influenced by factors associated with age or size, but overall the thoracic force relaxation behavior appears to be relatively insensitive to either of those PMHS traits. Additional testing will be required to evaluate this hypothesis. The raw force-deflection data generated in the ramp portion of this test series are consistent with the diagonal belt data of Kent et al. (2004) (Figure 9). The responses from subject 1 fall within the corridor, while the other two subjects are slightly above the corridor. This likely reflects two key differences in the experimental programs. The Kent corridor is based on the posterior reaction force, not on the posterior component of the applied belt force, which was used here. As discussed by Kent et al. (2004), the applied belt force contains an inertial force that is not present in the posterior reaction force. Second, the highest rate tested in the current study was slightly greater than the rate used by Kent et al.
0
500
1000
1500
2000
2500
3000
3500
4000
0 10 20 30 40 50Displacement (mm)
Forc
e (N
)
2.3
2.2
3.4
3.3
1.3
1.2
Figure 9. Raw force-deflection data compared to the diagonal belt response corridor by Kent et al. (2004) (dashed lines) based on posterior reaction force. While the study here presented a 7-parameter QLV model of the structural response, the nature of the underlying data suggest that the complexity and number of model parameters could be reduced. In particular, the non-linearity in the instantaneous elastic response could be represented by a linear model with little loss of model fit. It is also likely that the relaxation behavior could be represented adequately with fewer time constants over the 60-second time interval considered here. Finally, it is important to appreciate the model fitting strategy that was employed here to account for the use of a ramp input as opposed to an instantaneous step input. The separation of elastic and relaxation behaviors as done in this study is a result not only of the experimental data, but also of the model parameter identification strategy. For example, the similar tests by Kent et al. (2003) found less reduced force relaxation and less stiff elastic response, though the raw force-deflection data were similar to that measured in this test series. The difference is likely due in part to the differences in model parameter identification. This limitation in the model parameter identification technique is a possible explanation for the model’s slightly increased sensitivity to rate as compared to the test data in the 1-Hz and 5-Hz sine wave “validation” experiments (see Figure 6c). It has not been shown that
IRCOBI Conference – Bern (Switzerland) – September 2008 83

the approach used here generates a unique separation of the response, and future work should consider other techniques for fitting a model to ramp-hold data (e.g., Mattice et al. 2006). Several discontinuities are seen in the load history plots (see Figures 5, 6) that cannot necessarily be attributed to rib fracture. By analyzing strain gages placed at multiple rib locations along the thorax, no rib/sternum fractures were detected. Some costo-chondral separation may have occurred during the sub-failure ramp and hold tests, but could not be detected through palpation or analysis of the strain gage data. One possible cause of the loading discontinuities could be artifactural forces from the test rig. Force limiters were attached to the upper arms to reduce the chance of shoulder dislocation, and this may have caused the load discontinuities. As the rig was subjected to unsymmetrical loads, some binding of the fixture may have also caused these load effects. CONCLUSIONS This paper has presented an experimental and analytical framework for characterizing thoracic belt loadings on realistically postured PMHS in a configuration comparable to that seen in a 48 km/h automobile sled test at the time of maximum chest deformation. The bench-top environment used in this study provided a clearly defined loading environment and an experimentally tractable method for characterizing the chest. The analytical model was based on a viscoelastic model frequently used on biological materials; the model coefficients from three approximately 50% male PMHS were averaged, and in the case of the instantaneous elastic coefficients, linearized to provide the best fit model. Model fits to ramps of different magnitudes indicated that the assumption of temporal linearity was reasonable over the range of inputs in this study. In agreement with previous studies, the spatial (force-deflection) response was only slightly non-linear, indicating that a fully linear model would be reasonable up to the deflection levels used here. Pronounced variability in the instantaneous elastic behavior was observed, among the test subjects; the relaxation behavior exhibited less variability. Limitations There are several approximations that may influence the overall thoracic response properties when compared with the response recorded by an occupant in a vehicle crash. First, the occupant posterior remains unsupported during impact, allowing the ribs to rotate and deflect freely. The position of the PMHS on the test fixture may not adequately allow the restraint loading and subsequent response of the shoulder and clavicle. Similarly, the test fixture does not reproduce the changes in spinal curvature seen in occupants during an impact event, or the transient direction of the resultant restraint force vector acting on the occupant. In addition, motion of the internal viscera and the inertial loads generated as the anterior thorax arrests this motion in a frontal impact are not simulated in this bench-top environment. Finally, the location of the internal viscera depends to some degree on the orientation of the torso relative to the gravity vector, and this orientation on the bench-top is approximately perpendicular to that in an automotive environment. This test series, however, does obtain the thoracic response required for finite element model validation, and shows the potential for spinal fixation in bench-top tests. Belt positions did slightly vary between tests due to the amount of lung inflation and tissue relaxation. Acknowledging the effects of belt position can alter the response of the thorax (Murakami et al., 2006), every effort was made to document the exact position of the belts. While the variation of belt position may have had an affect on the QLV analysis, the calculated corridors are to be considered an averaged representation of the test population. REFERENCES Arbogast, K, Maltese, M, Nadkarni, V, Steen, P, Nysaether, J. (2006) Anterior-posterior thoracic
force-deflection characteristics measured during cardiopulmonary resuscitation: comparison to post-mortem human subject data. Stapp Car Crash Journal 50:131-45.
Crandall, J, Kent, R, Patrie, J, Fertile, J, Martin, P. (2000) Rib fracture patterns and radiologic detection – a restraint-based comparison. Annual Proceedings/Association for the Advancement of Automotive Medicine; 44:235-59.
84 IRCOBI Conference – Bern (Switzerland) – September 2008

Forman, J., Kent, R., Crandall, J., Bostrom, O., Haland, Y. Toward the Optimization of Belt Force Limit in an X-Type 3+2 Harness. Proc. of the 2005 IRCOBI Conference on the Biomechanics of Impact, Prague, Czech Republic.
Fung YC. Biomechanics: Mechanical Properties of Living Tissues. Springer, New York, NY. 1993. Kent, R, Bass, C, Woods, W, Sherwood, C, Madeley, N, Salzar, R, Kitagawa, Y. (2003) Muscle
tetanus and loading condition effects on the elastic and viscous characteristics of the thorax. Traffic Injury Prevention; 4(4):297-314.
Kent, R., Crandall, J., Bolton, J. Prasad, P., Nusholtz, G., Mertz, H. (2001) The influence of superficial soft tissues and restraint condition on thoracic skeletal injury prediction. Stapp Car Crash Journal, 45:375-396.
Kent, R., Lessley, D., Sherwood, C. (2004) Thoracic Response to Dynamic, Non-impact Loading from a Hub, Distributed Belt, Diagonal Belt, and Double Diagonal Belt. Stapp Car Crash Journal, 48, pp.
Kent, R., Lee, S., Darvish, K., Wang, S., Poster, C., Lange, A., Brede, C., Lange, D., Matsuoka, F. (2005) Structural and material changes in the aging thorax and their role in reduced thoracic injury tolerance. Stapp Car Crash Journal 49:231-249.
Kent, R., Woods, W., Salzar, R., Damon, A., Bass, C. (2008) The transient relationship between pressure and volume in the pediatric pulmonary system, Respiratory Physiology and Neurobiology, (submitted).
Kroell, C., Gadd, C., Schneider, D. (1974) Biomechanics in Crash Injury Research. ISA Transactions, 13 (3), pp 183-198.
Lau, I, Horsch, J., Viano, D. (1987) Biomechanics of Liver-Injury by Steering Wheel Loading. Journal of Trauma-Injury Infection and Critical Care, 27 (3), pp. 225-235.
Lessley, D. J., Salzar, R., Crandall, J., Kent, R., Bolton, J., Bass, C., Forman, J. (2008) Kinematics of the thorax under dynamic belt loading conditions. IRCOBI Conference on the Biomechanics of Impact.
Lobdell, T., Kroell, C., Schneider, D., Hering, W., Nahum, A. (1973) Impact Response of the Human Thorax in Proceedings of the Symposium Human Impact Response Measurement and Simulation. Edited by King W and Mertz H. General Motors Research Laboratories, Warren Michigan. Plenum Press New York, London, 1973, pp 201-245.
Mattice, J., Lau, A., Oyen, M., Kent, R. (2006) Spherical indentation load-relaxation of soft biological tissues. Journal of Materials Research , 21(8):2003-2010.
Mulligan, G.W.N., Pizey, G., Lane, D., Andersson, L., English, C., Kohut, C. (1994) An introduction to the understanding of blunt chest trauma. In Biomechanics of Impact Injury and Injury Tolerances of the Thorax-Shoulder Complex, ed. Backaitis, S., pp. 11-36, Society of Automotive Engineers publication PT-45.
Murakami, D., Kobayashi, S., Torigaki, T., Kent, R. (2006) Finite element analysis of hard and soft tissue contributions to thoracic response: sensitivity analysis of fluctuations in boundary conditions. Stapp Car Crash Journal 50:169-190.
Shaw, G., Lessley, D., Evans, J., Crandall, J., Shin, J., Portier, P., Paoloni, G. (2007) Quasi-Static and Dynamic Thoracic Loading Tests: Cadaveric Torsos. IRCOBI Conference on the Biomechanics of Impacts.
Viano, D. (1987) The Role of Biomechanics in Vehicle Design for Control of Injury. Public Health Reports, 102 (6), pp. 595-599.
Wang, N., Stevens, M., Doty, D., Hammond, E. (2000) Blunt chest trauma: an experimental model for heart and lung contusion. Journal of Trauma, 54(4):744-8.
Yoganandan, N., Pintar, F., Gennarelli, T. (2004) Small female-specific biomechanical corridors in side impacts. Proc. IRCOBI.
IRCOBI Conference – Bern (Switzerland) – September 2008 85