Virtual Reality for Enriched Rehabilitation of …1157294/...Virtual Reality for Enriched...
87
Virtual Reality for Enriched Rehabilitation of Stroke Patients with Spatial Neglect Diagnostics and the Rehabilitation Effect on Spatial Attention and Neuronal Activity Helena Fordell Department of Pharmacology and Clinical Neuroscience Department of Radiation Sciences Umeå University 2017
Transcript of Virtual Reality for Enriched Rehabilitation of …1157294/...Virtual Reality for Enriched...

Virtual Reality for Enriched Rehabilitation of Stroke Patients with Spatial Neglect
Diagnostics and the Rehabilitation Effect
on Spatial Attention and Neuronal Activity
Helena Fordell
Department of Pharmacology and Clinical Neuroscience Department of Radiation Sciences
Umeå University 2017

This work is protected by the Swedish Copyright Legislation (Act 1960:729)
Dissertation for PhD
ISBN 978-91-7601-792-0ISBN: 978-91-7601-792-0
ISSN 0346-6612
New Series Number 1929
Electronic version available at: http://umu.diva-portal.org/
Printed by: UmU Print Service, Umeå University
Umeå, Sweden 2017

Dedicated to all those
whose lives have been affected by stroke
.


Abstract Background
Approximately a third of all stroke patients develop spatial neglect, a debilitating symptom associated with poor outcome. Spatial neglect is clinically defined as a deficit in processing and responding to stimuli presented on the contralesional side of the body, or the space surrounding that side of the body. The heterogenetic, multi-sensory nature of the symptoms renders it difficult to diagnose and treat; therefor effective methods for screening and intervention for neglect are needed. Virtual reality (VR) is a method of brain–computer interaction that involves real-time simulation of an environment, scenario or activity that allows for user interaction and targets multiple senses. We hypothesize that VR can facilitate identification of spatial neglect in stroke patients and that training with this interface will improve patient’s functional outcome, through stimulation to neuronal networks including those controlling attention.
Objective The objective was to construct and validate a computerized test battery for spatial neglect and to investigate its usability in stroke patients. Also to design and develop a VR rehabilitation method for spatial neglect and to evaluate its effects on spatial attention and on neuronal activity in the brain.
Method We designed, developed and evaluated a new concept for assessment (VR-DiSTRO®) and training (RehAtt®) of spatial attention, using VR technology. The hardware consisted of a PC, monitor, 3D-glasses and a force feedback device to control the tasks (i.e., a robotic pen). The software enabled targets to be moved, rotated and manipulated in the 3D environment using the robotic pen. RehAtt® made it possible to combine intense visual scanning training, multi-sensory stimulation (i.e., audio, visual, tactile) and sensory-motor activation of the contralesional arm. In a first study on 31 stroke patients we performed a construct validation of VR-DiSTRO® against Rivermead Behavioural Test Battery (BIT) and

investigated the usability. In a second study, 15 subjects with chronic spatial neglect (symptoms >6 month) had self-training, 3 x 1 hour for 5 weeks using RehAtt®. Outcome were measured by changes in neglect tests and in Cathrine Bergego Scale (CBS). Training-related changes in neuronal activity of the brain was studied using fMRI during task and in resting state.
Results VR-DiSTRO® correctly identified all patients with neglect. The sensitivity was 100% and the specificity 82% for VR-DiSTRO® compared to BIT. Usability was high and no side-effects were noted. Using repeated measurement analysis, improvements due to the RehAtt® intervention were found for Baking tray task (p < 0.001), Star cancellation test (p = 0.006) and Extinction test (p = 0.05). Improvements were also seen in the Posner task as fewer missed targets (p = 0.024). Improvement in activities of daily living (CBS) was shown immediately after training (p < 0.01) and patients still reported improvement at 6 months follow-up. Training-related changes in neuronal activity were seen as an increased task-evoked brain activity in prefrontal and temporal cortex, mainly outside the attention network but in related cortical areas. During resting state, changes in network connectivity were seen after intervention with RehAtt® in the Dorsal Attention Network (DAN) and interhemispheric connectivity.
Conclusion VR-DiSTRO® identified visuospatial neglect in stroke patients quickly and with a high accuracy. RehAtt® training improved in spatial attention in chronic neglect with transfer to functions in daily living. Increased neuronal brain activity was found in and between attention networks and related brain structures. This could represent a compensatory effect in addition to sign of a restorative effect from the RehAtt training. The results obtained in this study are promising, encourage further development of the methods and merit for further studies.

i
Table of Contents Abbreviations ............................................................................. iiPublications and Manuscripts .................................................... iiiBackground ................................................................................. 1
Stroke and Spatial Neglect .............................................................................................. 1Neglect ............................................................................................................................ 3Pathophysiology of Neglect after Stroke and its Recovery ............................................ 6Diagnostics of Neglect .................................................................................................... 9Rehabilitation of Neglect ............................................................................................... 12Virtual Reality ................................................................................................................ 15VR-Diagnostics for Spatial Neglect ............................................................................... 16VR Rehabilitation for Neglect ....................................................................................... 17Research Rationale ........................................................................................................ 18
Aims ......................................................................................... 20Materials and Methods .............................................................. 21
VR-DiSTRO® ................................................................................................................ 27RehAtt® ......................................................................................................................... 28Validation and Evaluation ............................................................................................. 31fMRI Evaluation of RehAtt ........................................................................................... 32MRI Methods ................................................................................................................ 32Statistics ........................................................................................................................ 35
Results ....................................................................................... 37Results Paper I. Validation of VR-DiSTRO® ............................................................... 37Results Paper II. Training with RehAtt in Chronic Neglect ......................................... 38Results Paper III and IV Changes in Neural Activity ................................................... 41
Discussion ................................................................................. 47VR-DiSTRO® ................................................................................................................ 47RehAtt® ......................................................................................................................... 49Restorative or compensatory effect? ............................................................................ 52Methodological Considerations and Limitations ......................................................... 55Future Directions ........................................................................................................... 57
Conclusions .............................................................................. 58Sammanfattning på svenska ..................................................... 59Acknowledgements ................................................................... 63References ................................................................................ 69

ii
Abbreviations 3D Three-dimensionalACC AnteriorcingulatecortexADL ActiviesofdailylivingBI BarthelindexBIT RivermeadBehaviouralTestbatteryBOLD BloodoxygenationleveldependentBTT BakingTraytaskCBS CathrineBergegoscaleDAN DorsalattentionnetworkDARTEL DiffeomorphicanatomicalregistrationusingexponentialalgebraDLPFC DorsolateralprefrontalcortexEPI EchoplanarimagingEXT ExtinctiontestFEF FrontaleyefieldfMRI FunctionalmagneticresonanceimagingIPS IntraparietalsulcusISO InternationalOrganizationforStandardizationLB LinebisectionMMSE MinimentalstateexaminationMNI MontrealneurologicalinstitutemRS ModifiedRankinScalems MillisecondsMT Middletemporalgyrin NumberNIBS Non-invasivebrainstimulationtechniquesNIH-SS NationalInstituteofHealthStrokeScaleRCT RandomizedcontrolledtrialRT ReactiontimeRehAtt® VirtualrealitytrainingbatterySCT StarCancellationtestSLF SuperiorlongitudinalfasciculusSTG SuperiortemporalgyriTPJ Temporal-parietaljunctionUF UncinatefasciculusVAN VentralattentionnetworkVFC VentralfrontalcortexVR VirtualrealityVR-DiSTRO® Virtualrealitydiagnosticbattery

iii
Publications and Manuscripts This thesis is based on the following papers, which are referred to by their Roman numerals in the text:
I. Fordell H, Bodin K, Bucht G, Malm J. A virtual reality test battery for assessment and screening of spatial neglect. Acta Neurol Scand 2011;123(3):167-174.
II. Fordell H, Bodin K, Eklund A, Malm J. RehAtt — scanning training for neglect enhanced by multi-sensory stimulation in Virtual Reality. Top Stroke Rehabil 2016;23(3):191-199.
III. Ekman U*, Fordell H*, Eriksson J, Lenfeldt N, Wåhlin A, Eklund A, Malm J. Increase of frontal neuronal activity in chronic neglect after multi-sensory scanning training in virtual. (submitted)
IV. Wåhlin A**, Fordell H**, Ekman U, Lenfeldt N, Malm J. Rehabilitation of chronic spatial neglect strengthens functional connectivity between nodes of the dorsal attention network. (submitted)
*, Ekman and Fordell contributed equally to the work.
**, Wåhlin and Fordell contributed equally to the work.
Paper I is printed with permission from the publishers John Wiley & Sons Ltd, ACTA Neurologica Scandinavia 2011;123(3):167-174, and II from Taylor & Francis, Journal of Topics of Strokerehabilitation 2016;23(3)

iv

1
Background
Stroke and Spatial Neglect Spatial neglect is a common and debilitating consequence of stroke.(1-3) A stroke is the sudden loss of neurological function due to an interruption in blood supply to the brain tissue, caused by either a clot or an eruption of a blood vessel.(4) It is the main cause of long-term disability due to persistent motor and cognitive impairments.(5) If the stroke occurs in the left side of the brain, it impacts the functions of the right side of the body; persisting symptoms often include paralysis, numbness, and cognitive problems such as aphasia and apraxia. If the stroke occurs in the right side of the brain, the paresis affects the left side of the body and the most common cognitive consequence is spatial neglect.(6, 7) Spatial neglect, or simply neglect, is a heterogenetic and multi-sensory phenomenon(8) and is therefore difficult to diagnose and treat.(9) There is a lack of effective screening and treatment methods.(10) Neglect is defined as a deficit in processing and responding to stimuli presented on the contralesional side of the body – or the space surrounding that side of the body.(11) More than 30% of all stroke patients have neglect at onset and spontaneous recovery can occur during the first 12 weeks after the stroke.(1, 6, 12) This is also the best time window for effective rehabilitation due to brain plasticity.(13) The neglect is considered chronic when symptoms persist beyond six months after the stroke. Chronic neglect affects 15% of stroke survivors.(1, 14, 15) There are theories that Virtual Reality (VR) can serve as an enriched environment and have restorative effects on stroke rehabilitation.(16-18) We aim to design and develop new methods towards assessing and improving symptoms of neglect by combining the latest knowledge on neglect mechanisms and the use of VR. We also wanted to elucidate possibilities for effective rehabilitation in chronic neglect and further the understanding of the neurological mechanisms.

2
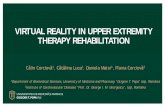
Figure 1. Fronto-parietal networks controlling spatial attention. (A) Three distinct white-matter tracts in the superior longitudinal fasciculus (SLF) are related to the fronto-parietal networks controlling spatial attention. (B) Their projection sites in both the parietal and frontal cortex correspond to the division into a dorsal attention network (DAN) typically associated with endogenous and spatial components of orienting, and a ventral attention network (VAN) associated with more reflexive, stimulus-driven, and non-spatial components. The SLF II might contribute to integrate activity between the VAN and the DAN by connecting inferior parietal with superior frontal areas. (C) Depiction of SLF in relation to another major white tract connecting posterior with anterior brain regions: inferior longitudinal fasciculus (ILF) and inferior fronto-occipital fasciculus (IFOF; unpublished data.) Printed with permission from author Patrik Vuilleumier and from publisher, “Mapping the functional neuroanatomy of spatial neglect” Annals of New York Academy of Sciences 2013;1296:50-74.
Vuilleumier Spatial neglect and the parietal lobe
Figure 2. Fronto-parietal networks controlling spatial attention. (A) Parietal and frontal areas involved in spatial attention arelinked by three distinct white-matter tracts in the superior longitudinal fasciculus (SLF). (B) Their projection sites in both theparietal and frontal cortex correspond to the division into a dorsal attention network (DAN) typically associated with endogenousand spatial components of orienting, and a ventral attention network (VAN) associated with more reflexive, stimulus-driven, andnonspatial components. The SLF II might contribute to integrate activity between the VAN and the DAN by connecting inferiorparietal with superior frontal areas. (C) Depiction of SLF in relation to another major white tract connecting posterior with anteriorbrain regions: inferior longitudinal fasciculus (ILF) and inferior fronto-occipital fasciculus (IFOF; unpublished data). A and Badapted, with permission, from Ref. 159.
including orienting and disengaging from currentfocus of attention in exogenous attention condi-tions. By contrast, more superior regions in theintraparietal sulcus (IPS) have been linked withvoluntary shifting and/or maintaining attention torelevant locations or objects.45 This anatomical dis-tinction has therefore led to an influential model ofspatial attention (Fig. 2) comprising both a dorsalfronto-parietal network linking the IPS with supe-rior frontal cortex (frontal eye fields, FEF), and aventral network linking the TPJ with the inferiorfrontal gyrus (operculum/insula). According to thismodel, damage to the ventral system would not only
impair contralesional exogenous orienting but alsoinduce subsequent dysfunction in the dorsal systemand hence additional endogenous orienting biasestoward the ipsilesional side, leading to full-blownspatial neglect.15 Moreover, damage to the TPJ re-liably correlates with the presence of extinction onbilateral visual stimulation,46,47 consistent with thenotion that this phenomenon may reflect exogenouscapture by ipsilesional distractors and impaired re-orienting to the contralesional side.42
However, recent work suggests that thisfunctional–anatomical dichotomy in attentionbetween dorsal and ventral attention areas
55Ann. N.Y. Acad. Sci. 1296 (2013) 50–74 C⃝ 2013 New York Academy of Sciences.

3
Neglect
Spatial neglect affects not only spatial attention but also the general capacity for attention, therefore the prefixes spatial, hemispatial and unilateral can make the nomenclature unclear. Spatial neglect affects the ability to explore the environment, search and orientate; and it causes impairment to be attentive to the contralesional arm (i.e., opposite side to the stroke lesion) and that side of space surrounding the body. For people with neglect, it becomes difficult to find objects placed on their left side and they may bump into objects on the left with the risk of falling. In traffic situations, they may fail to observe traffic coming from the left. The left side of their own body may become unfamiliar and the ability to control the left arm might be missing. The left side of their face may be neglected when grooming, shaving or putting on makeup. The left side of objects seem to disappear; thus they may leave food placed on this side of the plate; they may be unable to read since they are missing the left start point. Neglect, is commonly accompanied with some other co-factors that complicate the rehabilitation, such as; lack of awareness or recognition of contralesional side of body (anosognosia), unawareness of impairments from the stroke (anosodiaphoria), visual field defects (hemianopia), impaired working memory and behavior problems including a repetitive way of acting (perservations) and low motivation and drive for rehabilitation.(19)
The heterogenicity of impairments in neglect should be a major consideration when choosing methods for diagnosis and rehabilitation. The prognosis for patients with neglect is poor in terms of both motor and cognitive rehabilitation.(3) Neglect is a major hindrance in regaining independence in everyday life, prolongs the length of hospital stay and seriously affects on-going quality of life.(1, 20-24) Spatial attention is essential to many perceptual, cognitive, and motor functions and its absence contributes to many problems during rehabilitation. Thus, there is a need for more effective and comprehensive screening, assessment and rehabilitation methods for neglect.

4
Summary of Symptoms of Neglect
Symptoms of neglect are heterogeneous but can be characterized by three main entangled components of impairment; 1. spatial attention and orientation; 2. spatial awareness and 3. non-spatial attention.(7, 19, 25, 26) These core deficits and symptoms can be listed as;
Deficits in spatial attention and orientation Difficulties to attend to, orient to and explore the contralesional (opposite side to the stroke lesion) environment, within both peri-personal space (within an arm´s length) and extra-personal space (beyond an arm-length). Impaired perception which gives difficulty to attend to, locate, understand and interact with visual, auditory, and tactile information, especially when presented on the contralesional side of the body.
Defect spatial awareness In personal hemi neglect the lack of awareness affects the caring for and the attention to the left side of the body (upper and/or lower extremities). A balance problem is common with a pushing behavior towards the left and a rotation of gaze, head and trunk to the right. By not having awareness of peri- and extra-personal hemispace, patients fail to scan and orient to the left side.
Impaired mental spatial representation. For instance, left side is missing when patient describe their “mental” images of objects. Two different reference frames, which often coexist are described in hemispatial neglect. The main frame is spatial neglect from an egocentric perspective, a body-midline-centered spatial neglect. There is also an allocentric (object-centered). Having allocentric, spatial neglect makes them leave out for example the left of two objects or left part of an object placed in any position left or right from their body midline.

5
Impaired function of visuomotor exploring causing limitations in movement of hands and gaze towards the space surrounding the contralesional side of the body. Motor neglect as an inability to activate the remaining motor function in a paretic arm or leg, spontaneously or in response to a command or stimuli.
Non-spatial attention deficits,
The low level of arousal and vigilance affects the ability to stay alert and sustain focus. It is part of the non-spatial attention deficits in neglect. This impairs the ability to switch on a goal-driven top-down control of attention, the function to initiate an endogen function to be ready to act. This also affects and reduce the ability to stay alert and to shift and re-orientate attention quickly when an object appears from an unexpected direction. The reaction time to a new or salient stimulus are prolonged.
There is an impaired function of stimuli driven control of attention (bottom-up). There is also an impaired function of cognitive control to be ready to react without warning (intrinsic alertness) and also to be ready to increase responsewill, for example the capacity to act after a warning cue (phasic alertness). There is limited capacity, of general spatial attention i.e., an inability to shift and divide attention between two stimuli when presented simultaneously on the left and right side. The ipsilateral focus will then dominate and the stimuli (visual, audio or and tactile) presented on contralesional side disappears (extinction).

6
Pathophysiology of Neglect after Stroke and its Recovery
Stroke and Recovery
After acute stroke, a chain of different mechanisms causes motor and cognitive dysfunction. There are then several potential mechanisms for the recovery of function. The first three months after stroke represent a critical period of brain plasticity, resulting spontaneously or in relation to challenges within a training program.(27) Recovery involves many neurological processes including; reverse diaschisis (incoming neuronal traffic to connected areas causes increased excitation in these regions after a time of hypo-metabolism due to loss of incoming signals), nerve cell regeneration, neurogenesis, angiogenesis, dendritic and axonal arborization, increased numbers and strengthening of neuronal synapses and an increased number of receptors.(28) There is a plateau after three months of spontaneous recovery, however important structural and functional reorganization from training still can take place. Furthermore, after six months, despite this being referred to as the chronic phase, some effective rehabilitation of function can be obtained.(14, 29, 30) The training-related changes of neuronal activation involved in the chronic phase beg further elucidation.(31) One recurrent question is whether improvements from training are due to restorative effect or compensatory responses.(15, 31, 32)
Structural Lesions and Functional Breakdown
Neglect is mainly associated with stroke injuries in the right hemisphere.(14) The right-sided dominance of neglect follows the anatomy of partly lateralized function of attention to the right hemisphere´s ventral regions.(33) Particularly causative for neglect are stroke lesions located in the right; superior and middle temporal gyri, (STG, MT) basal ganglia (BG), and especially in the white matter tracts (Fig. 1.) superior longitudinal fasciculus (SLF) and uncinate fasciculus (FU), but also lesions in frontal areas. Lesions in the same critical structures causes chronic neglect.(14, 26, 34, 35) However, lesions

7
mapping studies using MR has shown that neglect symptoms can only partly be explained by the location and size of the structural lesions.(26) For example, small sub-cortical lesions in white matter structures as SLF II, connecting frontal and parietal areas, can cause a wide range of neglect symptoms.(36) Indicating that loss of function in key nodes responsible for the neuronal traffic within the attention network can be important components in the mechanism of neglect. These networks involve distant frontal and parietal regions in both the right and left hemispheres.(33) Neglect is thus rather caused by a breakdown in the function of integrating non-spatial and spatial attention.(33)
Attention Networks
The neuronal attention networks can be studied by using functional neuroimaging methods. Functional magnetic resonance imaging (fMRI) measures the blood oxygen level dependent (BOLD) signal, during performance of tasks and gives a temporal correlation interpreted as co-(37)neuronal activity provides information about activity in brain regions and brain networks that are related to specific functions (e.g. vision, attention, motor). Almost the same pattern of synchronized neuronal activation for a task can be identified at rest, in the absence of any task or stimuli (resting state networks).(38) Studying changes in the neuronal activity during a task and the connectivity in brain networks at rest, over time or the change before and after intervention, provides a window to study physiological function. This can illuminate spontaneous as well as training-related changes in neuronal activity in neglect.(12, 39-43) To study the changes in pattern of connectivity in and between Dorsal Attention Network DAN and Ventral Attention Network VAN, as well as intra and interhemispheric connectivity is thus a possibility for understanding the function of spatial attention and its recovery after stroke.(33, 42, 44) (Fig. 2.) The VAN is primarily connecting right temporal-parietal junction (TPJ) and the ventral frontal cortex (VFC). It is a bottom-up, multi-sensory stimuli driven part of the attention networks, localized in the ventral part of the right hemisphere. The VAN is mainly responsible for reorientation, alertness and vigilance. The DAN

8
connects frontoparietal regions including intraparietal sulcus (IPS) and frontal eye field (FEF). It provides a top-down, goal driven control of spatial attention located in both hemispheres, mainly responsible for controlling and directing spatial attention, and for coding stimulus selection and its salience.(33)
Training-related Changes in Neuronal Activity
In the critical sub-acute phase for post stroke recovery, fMRI analysis (42, 45) revealed a key pattern of enhanced connectivity within the DAN as being favorable for recovery from neglect.(33, 45) A pattern of strengthened inter-hemispheric activity is also important, as well as rebalanced activation between functionally homologus regions in lesioned and non-lesioned hemisphere.(33, 45) Enhanced activation of the functionally homologue DAN regions in the left hemisphere has been reported as a non-favorable activation pattern for symptom recovery.(42) Contradictorily, activation of posterior parietal regions of the DAN located in the left hemisphere was reported as favorable for neglect recovery in a longitudinal study.(12)
Studying changes in neuronal activity in relation to behavioral effect from training methods, could give guidance in the design of new rehabilitation methods for neglect.(26, 37, 46, 47) In the literature, there are a few studies showing neglect training-related neuronal changes identified with fMRI. Visual alertness training (AIXTENT) performed on a computer screen, has revealed increased activity in frontoparietal regions.(48) Optokinetic stimulation (OKS) is also a computerised neglect training that induced changes in more posterior brain regions.(46) Saj and Vuilleumier studied neuronal effect after one treatment wearing right deviated prism glasses, Prism Adaptation (PA).(37, 49) An increased activation was seen in the bilateral parietal, frontal, and occipital cortices during tasks of bisection and visual search directly after exposure(37)

9
Diagnostics of Neglect Severe neglect in a patient at a stroke ward is easily observed and identified from the patient’s behavior; however, mild or moderate neglect may be overlooked.(19, 50) According to recommendations in stroke guidelines, scanning for cognitive impairments including neglect should be a clinical routine.(51-54) The NIH-Stroke Scale (items No 3 and 11 are for neglect)(55) is the most commonly used screening test for neglect in the emergency settings. It is easy to use, but its sensitivity for finding neglect is low. By using NIH-SS to identify neglect only 43% in a study of 1200 stroke patients with acute right-sided lesion were diagnosed.(56) Instead, by using a set of paper-and-pen tests, such as cancellation tests and object copying or drawing, neglect diagnosis frequency increased to 85% in those with right-sided lesions(9) Despite an extensive body of research on neglect assessment tools, there is currently no recommended single test that correctly identifies stroke subjects with neglect, resulting in a battery of tests being necessary.(26, 57, 58)
In research environments, the Rivermead Behavioral Inattention Test (BIT, 15 subtests)(59) is often considered the standard criterion, or gold standard, for spatial neglect.(59, 60) However, the clinical use is limited because it takes about one hour to investigate the patient plus 30 minutes for scoring by a neuropsychologist or occupational therapist. Only patients having a high functional level manage to concentrate for this long. Another disadvantage is that the BIT battery is language dependent. As BIT is complicated to perform, a consequence has been that investigators prefer to use one or a selection of paper-and-pencil tests from BIT. This create the risk of missing subjects with mild spatial neglect or neglect in chronic phase.(61-63)
There is a recommendation to use structural methods for assessment of spatial neglect behavior in activities of daily living (ADL).(10, 50, 64) The Catherine Bergego Scale (CBS)(50) or the further improved version for more standardized scoring, the Kessler Foundation-NAP(65), are examples of scales that include scoring for impaired spatial attention.

10
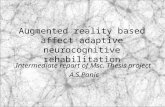
Figure 2 The ventral network mainly lateralized to the right hemisphere. Internetwork depicted by bidirectional arrows. Interhemispheric connections between homologue areas are not shown. FEF = frontal eye fields; IPS = intraparietal sulcus; VFC = ventral frontal cortex; TPJ = temporoparietal junction; V = visual cortex.
Figure 3. Neglect shown in a Star Cancellation Test, as an example of how a computerized test may give more information than a paper and pen tests.

11
These include assessment of factors such as visual scanning, direction of gaze and acting to sound stimuli. Focus is paied to awareness and care of contralesional side of the body and to the near peripersonal space in grooming, dressing and during a meal. Also, awareness of the surrounding hemispace, orientation ability and risk of collision to obstacles on contralesional side are examples of tasks included in these scales. CBS consists of a three-part questionnaire for patient, next to kin and therapist.(50)
In a Canadian survey, 28 different diagnostic tests for neglect were used by occupational therapists.(66) Most of them paper and pen tests that had a low sensitivity for detection.(9) BIT subtests such as Cancellation and Line Bisection tests are still among the most recommended neglect tests. Their sensitivity and specificity are varying and even when combined, their predictability for neglect is low depending of definition of neglect. Learned compensatory strategies might cover for true deviation of their focus to the right side. This might give a test result that masks impairments significant in spatial behavior in activity.(50, 64, 67)
The Posner Cueing test, a reaction time index, is likely a more sensitive test for mild neglect then the traditional pen-and-paper tests.(62) Extinction tests (NIH-SS#3 and #9)(68) are important to capture the limited capacity of attention in different sensory modalities.(8) (73). The pen-and-paper tests assess neglect in near-peri-personal space only. Neglect extending into extra-personal space might be missed, with dangerous impacts on behaviour (e.g. traffic situations).
Pen-and-paper tests do not reflect the multisensory complexity and perceptual-attention part of the neglect phenomenon (8), nor do they assess the sensorimotor exploring behaviour as in impaired movements to act towards left-sided stimuli.(19) Baking Tray task has been suggested as a sensitive test for neglect behavioural.(69, 70) Transforming conventional pen-and-paper tests to computer applications is known to

12
improve the test sensitivity and specificity.(71, 72) Computerized tests give more information as it is possible to register start point, scanning pattern, and end point.(71) (Fig. 3.) In summary, there is a recommendation to use a comprehensive battery of tests that cover the different domains of spatial neglect and these should be combined with a structural assessment of neglect behaviour in activities of daily living. (Page 4-5. Fig 4.)
Rehabilitation of Neglect Even though many different treatment methods for neglect have been suggested, there is insufficient evidence to recommend any specific interventions to increase independence.(10) In neglect rehabilitation research, there are methodological problems, for instance a general lack of consistence in outcome parameters and especially lack of evaluation parameters describing transfer of improved function to activities of daily life (ADL).(10) In the Cochrane review, effect of training was defined as persistent improvement of spatial attention in ADL.(10) The main intervention approaches are functional training, sensory stimulation, strategy training and task repetition.(19, 73) In summary, rehabilitation of neglect should focus on:(19, 73) Learning a strategy for visuospatial scanning(74), activation of the contralesional arm(75) and tasks for perceptual treatment (i.e., paper and pen tasks, reading, copy pictures).(73, 76) There are novel approaches and therapy methods for neglect, these can broadly be classified into four categories; 1. Non-Invasive Brain Stimulation techniques, NIBS (as Transcranial Magnetic Stimulation and Transcranial Direct Current Stimulation)(77), 2. drugs (cholinergic, dopaminergic and noradrenergic stimulating treatments)(78); 3. Prism Adaptation(79) and VR methods(80).(81)
So far a general agreement seems to be that rehabilitation program for neglect should include daily task-specific training.(51, 52, 54) Suggested training time to relearn a function and achieve persistent improvement is totally 40 hours of therapist led training.(76) This is difficult to achieve in real reality at a stroke ward as the hospital stay in modern stroke care is

13
short. There is a need of more research to provide evidence for more specific recommendations for treatment of neglect. Many neglect rehabilitation studies are small and do not have a randomised controlled trial design, RCT design. Independent of training method, the intensity, frequency and total amount of training differs between studies.(10) Knowledge about training effect in patients with chronic neglect needs to be elucidated, as rehabilitation effect mainly is evaluated in the first months after stroke.
The suggested rehabilitation methods for neglect have been categorized as either top-down methods (relearning strategies, i.e., scanning training) or bottom-up stimulating techniques (to improve perceptual awareness, i.e., optic kinetic stimulation). (10)Examples of bottom-up methods that have proven effective are Optic Kinetic Stimulation (79, 82, 83), audio and tactile cues(74, 84), visuomotor activation(75) Prism Adaptation(25, 79, 83), pleasant music (85) and VR games(80, 86).(10) Scanning training, i.e., top-down stimulation, has shown improvement in acute and chronic phase neglect.(74) In the ACRM, American Congress of Rehabilitation guidelines there are recommendations to use top-down scanning training to help patients learn strategies to compensate for their impairment, this performed in combination with visuo spatial tasks.(73) From a theoretical perspective there are now suggestions to combine top-down and bottom-up methods in order to stimulate the VAN and DAN network mechanisms to further improve the outcome of training.(33)

14
.
Figure 4. Different lesioned regions in relation to neglect tests Illustration from a meta-analysis of 20 lesion-mapping studies of neglect symptoms illustrate the likelihood of lesions peaks for different for neglect tests. A battery of tests is needed to cover for different behavioral manifestations of spatial neglect.
Printed with permission from author Patrik Vuilleumier and publisher,“Mapping the functional neuroanatomy of spatial neglect”. Annals of New York Academy of Sciences 2013;1296:50-74."
."

15
Virtual Reality Virtual reality (VR) can be defined as a user-computer interface that implements real-time simulations that the user perceives as a computer-produced environment. The user can experience and interact within the VR environment via visual, audio, tactile or olfactory modalities.(16) VR techniques can be more or less immersed, i.e., a feeling of being present and fully involved. The immersed experience can range from a low-level in commercial 2D computer games to high-level in desktop 3D interfaces, to full immersed experience by using head-mounted displays. A fully immersive technique means that the user is presented as an avatar, an 3D image of the player acting within the VR environment.(80, 87, 88) The computer controlled 3D image follows the user´s movements (i.e. the motion of the device) in the environment and this is presented on the display. The immersed experience is thought to give increased access to mental capacity, such as “hyperfocused” attention.(89) Adding multi-sensory feed-back options in VR causes the immersed feeling to rise and the environment may be experienced as fun and enriched. Enriched environment is known to have a positive effect on stroke rehabilitation (90), especially in combination with intense repetitions of the tasks (29, 30).
Interactions are made with a mouse, joystick, keyboard or sensors on the body. Other options for interaction devices are gloves with attached wires. Examples of such devices are Cyber glove® and Cyber grasp® that is used for hand-training as well as Eye toy® and Leap motion® devices. Haptic devices like Phantom Omni® (Geomagic touch®) are used in VR, giving a forced feedback to the hand. Thus, visual objects can be manipulated, moved and rotated. Depending on setup, this can provide a realistic experience of resistance, weight and force to the hand. This interaction is made possible by software that produces real-time physics. Immersed VR-applications are now available even in smartphones. Recently, more sophisticated VR technologies have become more readily available and affordable.(80, 90)

16
In the design of different VR set-ups for stroke patients, and especially those with neglect, it is important to evaluate the feasibility. This means that ergonomic aspects and side :ffects such as motion sickness, nausea or stress must be studied. It is also necessary to customize the VR-environment and training tasks for people with impaired attention capacity and various other deficits from stroke lesions as paresis. VR and robotically-assisted training have been found to be beneficial in stroke-rehabilitation in improving upper limb function with transfer to improved function in ADL.(91-93) There are also some evidence for positive effects from using VR for neglect rehabilitation.(76, 80, 81, 94, 95)
VR-Diagnostics for Spatial Neglect
The number of neglect studies using VR for diagnostic and training purposes is rapidly increasing.(80, 95) A multi-sensory approach may be beneficial in the testing and treatment of spatial neglect.(8) Using VR technology in development of diagnostic methods for neglect offers several benefits.(80, 95) For instance, tracking and recording of eye movements, head and limb movements are possible in VR applications. Behavior and response can be recorded and measured in accordance to stimuli.(80)(91)
Other benefits by using VR technology are how the test situation can be designed to display and dynamically regulate multi-sensory stimuli in peri- and extra-personal space within a 3D environment.(80) VR tasks can also involve registration of behavior in more challenging and dynamic types of tasks compared to paper-and-pen tests. For instance, tests can be creates within an ecological 3D environment as in traffic situation or during a walk in the park.(96, 97)

17
VR Rehabilitation for Neglect There is limited evidence of improvement of spatial neglect from training in VR(80, 95) In a RCT (98) a therapy method was evaluated where left hemi-body was activated in a 2D video game environment, visual feedback was given from limb activation. This was shown to be more effective than conventional scanning therapy. Since the 1990s VR technology has been used to construct methods for diagnostics, assessment and treatment of neglect. However, it has mainly been evaluated in small studies.(80, 95)
An interesting option with VR is learning a strategy as visual-scanning-training in a motivating and ecologically relevant VR environment. VR enables training situations that otherwise would not be possible in the hospital rehabilitation environment: scanning traffic to safely cross a street, training for driving, visual search in shops, visits in virtual restaurants and parks.(80)
VR makes it possible to enhance learning effect of a scanning strategy from the multisensory guiding cues and the high intensity of repetitions with increasing level of difficulty that will likely be favourable compared to the training in daily life activities.(29) It might diminish the needed volume of training time recommended to establish a persistent effect of improved function.
The recommended methods of limb activation to improve spatial attention, can be included in a VR method for neglect by using robotics. (75) This might be a way to improve the awareness and motor function in the contralesional paretic limb.(99) Methods constructed as self-instructional and motivating by using game rewards might be used as self-training and then reduce time of support from occupational therapist. The perceptual training of spatial awareness in VR can be designed to include the crucial multi-sensory aspects of spatial neglect in the tasks.(100) In the design of a VR-game applications for spatial neglect one can also include advanced tasks for top-down activity. For example, moving 3D puzzle and construction tasks are high level perceptual visuo-spatial training. Guidance during the task by visual, audio and tactile cues might

18
enhance effect by step-wise directing attention towards targets appearing in the neglected surrounding space, both near and far. The emerging prospect for neglect training using VR is to see how to combine recommended methods towards developing an enriched optimal rehabilitation for the patient.(29)
The question remains whether the positive effect on function from neglect training originates from a compensatory or restorative processes or in the brain.(27, 28) We find it important to illuminate that question in this study by analysing training-related changes in neuronal activity using fMRI techniques.
Research Rationale Neglect is a common cognitive impairment that seriously hinders stroke patients´ability to regain independence in daily life. A substantial part of stroke survivor’s experiences long-standing attention impairments regarded as chronic neglect. Thus, there is an urgent need for improved methods to screen for neglect, and effective training methods that could improve the care for stroke patients that have neglect. Little is known about training-related neuronal changes related to neglect, especially in those whose impairments of spatial attention is regarded as chronic.
We have found VR to be a promising technical platform to use in the construction of conceptually new methods for assessment and rehabilitation of spatial neglect. VR computerized versions may give standardized and repeatable test situations compared to conventional neglect tests. They offer better control of stimuli and registration of response. A selection of tests pinpointing different domains of neglect could be created using VR methodology, which would probably make it more efficient to screen for neglect among stroke patients, compared to using a large standard criterion test battery. The usability and feasibility of such a VR tool needs to be evaluated. VR-technology used in the construction of a training method would make it possible to combine a sample of bottom-up techniques giving visual, audio and tactile

19
stimulation, methods that previously have showed effects in RCT. Activation of the contralesional arm is possible by using a haptic device. Altogether this may create an enriched training environment known to enhance training effects after stroke. Adding a selection of top-down tasks pinpointing spatial, non-spatial and motor attentional domains would thereby create an enriched rehabilitation for neglect.
This dissertation will focus on identifying the best design, to develop and evaluate a VR-neglect test-battery and a VR-training battery. The hypothesis was that a top-down learning of a visual scanning strategy enhanced by bottom-up multi-sensory stimulation in VR would improve spatial attention behavior in chronic neglect in tests and in activities of daily life. Effect from the VR-method would give a training-related change in or between attention networks and related areas.

20
Aims A general aim of this thesis project was to design, develop and evaluate a new method of assessment and training for spatial neglect using virtual reality technology and to study the pathophysiological features of its effect in chronic neglect. Specific aims were;
I
To propose, construct and validate a computerised test battery VR-DiSTRO® for spatial neglect and to investigate its usability in elderly patients with stroke.
II
To design and develop RehAtt®, a virtual reality training battery for spatial neglect based on evidence based theory and in a clinical study to evaluate the battery regarding improvement in spatial attention.
III and IV
To describe how RehAtt® training changes brain function by analyzing task and resting state fMRI, collected before and after training.

21
Materials and Methods Table 1. Study overview
I II III IV
Patient cohort 1. 2. 2. 2.
Stroke subjects(n)
Ischemic infarcts
Intracerebral
haemorrhages
Lesion in right
hemisphere
Patients with
neglect (n)
Type of neglect
31
28
3
19/31
9
subacute
15
15
0
15/15
15
chronic
12
12
0
12/12
12
chronic
13
13
0
13/13
13
chronic
BIT
(Behavioral
Inattention test )
Paper-and-pen and
conventional tests
x
x
VR-DiSTRO®
computerised
neglect test battery
x x x x
RehAtt®
VR intervention for
neglect
x x x
MRI
Structural MRI
fMRI Posner´s task
fMRI resting state
Yes
Yes
Yes
Yes
Yes
Yes
Yes

22
Summary of Study Design
Two VR methods were designed and developed: VR-DiSTRO®, for the diagnostic and assessment of spatial neglect, and RehAtt® for the training of neglect patients. (Table 1.) Paper I concerns a construct validation of the computerised neglect test battery VR-DiSTRO® to Rivermead Behavioral Inattention Test (BIT 15 subtests) used as a criterion of spatial neglect. The accuracy of VR-DiSTRO® to the BIT and a comparison of each computerised tests to the corresponding conventional tests was made. Each computerised test was also compared to the BIT. This study was performed in an acute stroke ward, evaluating patients who had suffered both left- and right-sided ischemic and hemorrhagic strokes.
In Paper II intervention with RehAtt® was proposed and evaluated in a cohort of stroke patients with chronic spatial neglect. Baseline investigations consisted of a battery of neglect tests repeated three times during five weeks and were then repeated after the intervention. To evaluate the effect of RehAtt® on the activities of daily life, CBS was used to assess spatial attention before and after intervention and again six months later. Paper III and IV refer to the same patient population as in paper II but seek to evaluate changes in neuronal activity before and after training with RehAtt® in relation to different MRI techniques. Paper III present an analysis of cortical activation during the task sequence fMRI, and Paper IV is an analysis of connectivity in the patient’s neuronal network during the resting state in fMRI.
Figure 5. Study design for paper II-IV, fMRI data collected for III and IV.

23
Subjects
All subjects in Paper I-IV had a stroke defined according to the WHO criteria.(101) (Table 1.) Patients included in cohort one for the evaluation of VR-DiSTRO® were 31 stroke patients (9 women, 22 men; mean age 74.1±11 years±SD) recruited consecutively from the stroke ward at the Umea University Hospital. Inclusion criteria were an ischemic or hemorrhagic lesion (left or right hemisphere) and able to participate in a test-session for one hour.
Subjects included in cohort two for the evaluation of RehAtt® (Paper II-IV) were invited to participate after being identified from their medical record as having reported signs of impaired spatial attention. Patients were not eligible if they had severe visual impairment, severe medical illness, severe depression, or cognitive dysfunction. All of them had received regular rehabilitation for neglect at the time of their stroke onset. Fifteen subjects (4 women, 11 men; mean age = 72.7±6.1) were included. They had persisting symptoms of neglect more than six months after a right-sided ischemic lesion (range 6–120 months after ictus, mean = 41 months). (Table 2.) (Fig 8)
Papers III and IV refer to the same patients as in paper II. Fourteen of the fifteen subjects performed an MRI scan before and after intervention with RehAtt® of whom twelve patients fulfilled the task fMRI protocol in Paper III and thirteen fulfilled the Resting State MRI protocol in paper IV. There were no dropouts. One of fifteen had contraindication for MR, a heart implant.

24
Ethics
All subjects were given oral and written information and signed a written
consent. The Ethical Review Board at Umeå University approved this
research (06-078 and 2010-266-31M).
Investigations
At start of the studies, all subjects (Paper I-IV) were investigated with the National Institutes of Health Stroke Scale (NIH-SS)(68), the Mini Mental State Examination (MMSE)(101), Humphrey perimetry, the Barthel index (BI) and the modified Rankin Scale (mRS)(102). The education level and computer experience were registered. (Table 2).
Definition of spatial neglect
In the first study cohort (paper I), spatial neglect was defined according to the The Rivermead Behavioral Inattention Test (BIT with 15 subtests).(59) In cohort two (Paper II-IV), patients were defined as having spatial neglect if they failed one or more of the four subtests in the VR-DiSTRO® (Star Cancellation Task, Line bisection Task, Extinction test or Baking Tray Task)(103) and had impairment of spatial attention in activities of daily living, measured by the Catherine Bergego Scale (CBS).(50)
Test situation
All test sessions were performed in a quiet room. Patients were sitting with tests presented in their body midline. Instructions were given in a similar structured way following the manuals for computerized tests and conventional tests. No time limits were used. In Paper I the time for the test procedures were measured for VR-DiSTRO® and for BIT. Performance was overlooked from outside the room for computerized tests. A psychologist performed the BIT test battery. The investigators were blinded regarding diagnosis in Paper I.

25
The instrument set-up for VR-DiSTRO® and RehAtt®
A desktop computer (EMS Shuttle P4 3GHz; EMS, Umeå, Sweden), graphics card (Nvidia Quadro FX, Santa Clara, CA, USA), headphones, 3D stereo shutter glasses (Crystal Eyes; Stereographics⁄RealD, Beverly Hills, CA, USA), a robotic pen (Phantom Omni haptic device; SensAble Technologies, Woburn MA, USA), a monitor and numeric keyboard. The software used in the project was initially based on the open source platform Colloseum3D VRlab, Umeå University, Sweden.(104) This provides the basic functionality for scripted 3D-graphics, physics-based simulation, audio and haptic feedback. (Fig. 7.)
Posner Cueing task
The Posner Cueing task was used in studies II-IV. (Fig. 6.) This is a computerised task for goal directed spatial attention and was performed as an ad-on test to VR-DiSTRO® (1x40 trials) at the three baseline test sessions and after intervention. The same task was also used in the MRI scanner before and after RehAtt® intervention (2 x 40 trials) to study changes in cortical activation. (Fig 6.)
Test performance.
The participants looked at a red fixation cross at the centre of a screen. (regressor) A new trial was started by a change of colour from red to green, an arrow “a cue” pointing either left or right appeared signalling ready to act and directed attention towards upcoming stimuli. After a random delay a target appeared to either left- or right-side on the screen. These left and right targets that were either congruent with the cue (arrow had pointed correct direction towards target in 75%) or incongruent (arrow distractingly pointed in opposite direction in 25%). Target detection was indicated with a right-hand key-press. (Fig 6.)

26
Figure 6. Posner´s cuing task.
Behavioral performances before and after RehAtt® intervention on the Posner cueing task were measured in accuracy (% misses left and right), and reaction time (RT) in ms for targets to left and right side, for targets appearing after a congruent respectively non-congruent cue respectively.
Table 2. Demographic and clinical features in paper II-IV
15 Subjects Mean, SD ± (range)
Age, years 72.8±5.7 (62-82)
Time post stroke, months 41±27 (6-120)
NIH-SS, total score 6.31 (1-15)
NIH-SS, 5a left motor arm score 1.6 (0-4)
mRS, score 3.3±0.7 (1-4)
Barthel, points 67.7±10,6 (25-100)
MMSE, points 26.8±2.1 (23-29)
Education post elementary 2.5 (0-7) years
Computer experience (no/yes) 8 / 7
Visual impairments Quadrantanopsia: 3, Hemianopsia:2
Sex (Female/Male) 4 / 11
Abbreviations: NIH-SS, National Institute of Health Stroke Scale; mRS, modified Rankin scale. MMSE, Mini Mental State Estimations. In paper III and IV 3 respectively 2 patients were excluded by 1, MRI incompatible heart valve device and 2, incomplete technical data from MRI scanning session.

27
VR-DiSTRO®
The design
The VR-DiSTRO® was designed and constructed to include four neglect tests pinpointing different attention domains (See Fig. 4.) that are disturbed in spatial neglect; (i) VR-Star Cancellation Test for egocentric neglect and visual scanning; (ii) VR-Line Bisection for allocentric neglect and spatial judgement; (iii) VR-Visual Extinction to measure attention capacity and distinguish between attention and sensory factors and finally; (iv) VR-Baking Tray Task as a functional measure of spatial judgement and visuomotor exploring. In VR-Star Cancellation Test, and VR-Line Bisection the robotic pen was used to point to the screen like if using a touch screen. The healthy hand controlled the pen in test situations and a touch sensation and a realistic force feedback was perceived. The robotic pen was seen on the screen. The cubes in VR-Baking Tray Task could be moved, replaced and manipulated, also in depth by the virtual reality technology. The friction to the tray was experienced by force feedback from the robotic pen and simultaneously the events were seen in front of the screen in 3D. For the performance of VR-Visual Extinction a chin-support was used to keep a fixed field of view of 60´ and a separate keyboard was used to indicate reply. The same instrument and set up was used for Posner cueing task outside the scanner.

28
RehAtt®
The design
The RehAtt® method (Fig. 9.) was designed and constructed to combine an intense visual scanning training with multisensory stimulation and activation of the contralesional arm. Using a battery of different applications with visuo and audio spatial tasks a self-training was performed in a 3D virtual reality (VR) game environment. The robotic pen (Fig. 7.) was used with the contralesional arm (arm support used when needed) to act towards targets appearing in the 3D space in front of the monitor. The VR software technology creates the interaction in the computerised environment, this means the targets and objects can all be moved, rotated and manipulated, physically felt with force feedback. The collision of objects was experienced through the robotic pen to the contralesional hand by force feedback and creates tactile, vibration and proprioceptive input. Using the battery, an individually choice of training tasks was made and an individualised increasing level of difficulty were given. Visual scanning was performed in the RehAtt® application Haptris, developed from the well-known concept of the Tetris computer game. (Fig. 10.) Another training application was the 3D Mental rotation task. During an active pause the subjects listened to pleasant music in an audio spatial training application. The RehAtt® training battery menu is shown in Fig. 10.

29
Figure 7. RehATT®-training battery for neglect, the research set-up.
Figure 8. Paper II-IV Overlap of the distribution of the right-sided lesions, the color (1-10) illustrates number of patients with a corresponding ischemic lesion. Printed with permission from from Taylor & Francis, Journal of Topics of Strokerehabilitation 2016;23(3)

30
Figure 9. RehAtt® set-up, support by occupational therapist when needed.
Figure 10. A selection of training tasks in the RehAtt® menu.

31
Validation and Evaluation Validation of the new virtual reality methods (Paper I and II) was made in two prospective clinical trials. In the first study (Paper I), the total score of the computerised neglect test battery VR-DiSTRO® was compared to the total score of the BIT battery. The individual computerised tests were also compared to the corresponding conventional test, i.e., VR-Star Cancelletion Task, VR-Line Bisection, VR-Visual Extinction and VR-Baking Tray. (Fig. 13.)
The Paper II-IV study is outlined in Figure 5. It evaluated improvement in spatial behavior in neglect tests and activities of daily life before and after a VR intervention with RehAtt®. The intervention consisted of self-training with RehAtt® (Fig. 9, 10.) for 15 h (3x1hr sessions/week for 5 weeks). Baseline investigations (using VR-DiSTRO® as described above), assessed each patient before training started and were repeated three times during a five-week period, at intervals of one to two weeks. This multiple baseline design was used to both confirm the chronicity of neglect symptoms and to create a stable baseline for post-intervention comparisons and also to control for test-re-test learning effects. After the intervention, all test procedures were repeated.
The computerised attention test Posner Cuing Task (Fig. 6.) was included in all test sessions and also used in the MRI scanner to evaluate change in neuronal activation after RehAtt® intervention. CBS was used before and after the intervention and at the follow-up six months later. Validation of usability for the VR-methods (Paper I) was assessed according to ISO 9241-11 using a multiple-choice questionnaire.

32
fMRI Evaluation of RehAtt® Intervention
We investigated neuronal plasticity from RehAtt® intervention in chronic neglect using fMRI. fMRI was performed before and after the intervention in the same sample of chronic neglect patients presented in Paper II. For this purpose, we designed a fMRI protocol including sequences during a task of goal directed attention and during resting state.
To measure the change in cortical activation during attention processes we firstly used the Posner cueing task. (Paper III) (Figure 14, 15). During this task we studied the change of localisation and intensity of the BOLD signal after RehAtt intervention. The Posner cueing task includes different aspects of spatial attention as goal and stimuli driven processes. We evaluated change in cortical activation during goal directed attention to a central arrow, a cue signalling to be ready to act on a target soon appearing to either the right or to the left-hand side. (See figure 6 and paper III for details). The cue, pointing either right or left was in 25% of the cases guiding to wrong visual field. We also evaluated changes training related changes during the target part of the test and the behavioral performance as in percent misses of targets and reaction times.
To further study neuronal plasticity from intervention, we evaluated the changes of connectivity in brain networks during resting state. (Paper IV) We studied change in connectivity in three steps, firstly from regions of interest in dorsal attention network (DAN) for this sample of subjects, identified from the previous task activation during cue (Paper III). Secondly, we compared connectivity in general in eight key neuronal networks throughout the brain before and after the RehAtt intervention.
MRI Methods All structural and functional data were collected on a 3 Tesla General Electric MRI system (HD750) with a 32-channel head coil. Details in Paper III BOLD signal was quantified using collected T2*-weighted images single-shot gradient echo planar imaging (EPI) sequence (37 interleaved axial slices, in-plane matrix size 96 x 96 interpolated to 128 x

33
128: 3.4 mm, gap: 0.5 mm, TR 2000 ms, TE 30 ms, flip angle 80°, field of view 25 x 25 cm). To allow steady-state imaging prior to image acquisition, ten dummy scans were executed. A total of 740 volumes per session were collected for the Posner Cueing task and a total of 170 volumes per session for the resting state scan.
All BOLD fMRI data were corrected for acquisition time differences between slices in each volume and each volume was realigned to account for patient motion between scans. Using diffeomorphic anatomical registration using exponential algebra (105), the realigned fMRI images were normalized to the sample-specific group template, smoothed using an 8.0-mm full width at half maximum Gaussian filter and affine-aligned into stereotactic Montreal Neurological Institute (MNI) space. Finally, to limit the impact of task-correlated motion ArtRepair (v.4 School of Medicine, Stanford University, Palo Alto, CA, USA) was used for BOLD fMRI data for the Posner Cueing task (Paper III).
Analysis of the fMRI activation BOLD signal
Imaging acquisition protocol and analysis of Posner Cueing task. (Posner cuing task is illustrated in Fig6.) Right and left cue and target were contrasted with the red-cross baseline condition for each individual (the first-order analyses). Then cortical activation for cue conditions (pointing to left or right side) and target condition (appearing to the left and right side after as well incongruent as congruent cues) were contrasted with the red-cross baseline condition at the pre-intervention test in fMRI. Then estimations from each individual were input to a second-level visual field (right and left)-by session (pre- and post-RehAtt® intervention) analysis. This describes a top-down goal-directed attentional processing including DAN. For bottom-up stimuli attentional processing, including the VAN and redirecting attention processes, estimations of a congruency by session for the target condition was analysed and averaged across visual fields.

34
Resting State Region-of-Interest Analyses, Dorsal Attention Network
From the activation during Posner Cueing task fMRI (Paper III) above, a group DAN activation map was constructed. With the focus on activation peaks in the DAN, a ROI analysis was performed by constructing four spheres of 4 mm radius in the main peaks. These were located in the left and right frontal eye fields (lFEF and rFEF) and in the left and right intraparietal sulcus (lIPS and rIPS). (Fig. 16) Using the resting state fMRI scan we calculated functional connectivity as the temporal correlation (Pearson r) between all ROI pairs. (Fig. 17)
Concordance analyses
We performed an analysis of topological reorganization in the DAN compared to other resting state networks. Using a previously published atlas, we reconstructed individual level representations of two networks that collectively comprised the DAN as well as the primary visual network. Longitudinal similarity was calculated for the network using a spatial concordance correlation measure.(106) Here we expected that DAN components would show lower concordance between time points compared to the primary visual network that we considered unlikely to be influenced by the intervention.

35
Statistics In Paper I the computerized tests were compared to corresponding conventional using the Cohen´s kappa coefficient. For each subtest and for the VR-DiSTRO® a comparison was made to the neglect criterion BIT, where sensitivity, specificity, positive predictive value and a likely hood ratio test was calculated.
In Paper II. To evaluate the behavioral, effect a repeated measurement ANOVA, with Huynh-Feldt adjustment was used. A simple contrast was used to compare results for each test after training with results at each of the three baseline test sessions. To study differences between the baseline assessments the same test was used. If there were no differences in the pairwise comparisons between the three scores from the repeated tests occasions at the baseline, it was interpreted as there was no significant test-retest learning effect. An adjustment was made for multiple T-tests using the Holm Bonferroni method. To compare CBS observer score before and after training the Paired T-test was used. In the Posner test, the Wilcoxon signed-rank test was used for analysis of percent missed targets. The statistical significance was set as p < 0.05. The SPSS statistical package (SPSS Inc, Chicago, IL, USA) was used for calculations.
In Paper III. In the first-order fMRI analyses, within each subject, the BOLD signal was modeled as a set of regressors representing the conditions in the Posner task. We modeled baseline fixation, left and right cue conditions (arrow pointing either left or right) as well as congruent and incongruent targets. Six motion parameters (three representing rotation and three representing translation) were included in the model. Model estimates were passed to second level ANOVAs for (1) cue direction (left and right) by time (pre- and post-intervention) and (2) target (congruent and incongruent) by time (pre- and post-intervention). The first ANOVA was constructed to test changes in top-down attention processes and the second ANOVA was set up to test bottom-up attention processes. In the whole-brain analyses the statistical threshold was set to p < 0.001 at the voxel level in conjunction with p < 0.05 FWE correction at the cluster level.

36
In Paper IV. Increases in connectivity were assessed with paired t-tests. We applied a Bonferroni corrected threshold of p=0.0125 since there were four possible combinations of ROIs that formed an interhemispheric connection within the DAN. A paired samples t-test was selected to determine if spatial concordance was lower for the DAN than a primary visual network. Here we applied p=0.05 as threshold of significance.

37
Results
Results Paper I. Validation of VR-DiSTRO® Duration for the assessment of spatial neglect using VR-DiSTRO® was 15 minutes, compared to 50 min for the BIT battery. Comparisons of the VR-DiSTRO® (four tests) to BIT (15 subtests) are shown in Table 3. In summary, VR-DiSTRO® showed a sensitivity of 100% and a specificity of 82% to identify spatial neglect and thus the VR-DiSTRO® correctly diagnosed all patients with spatial neglect. The two VR-DiSTRO® subtests VR-baking tray (r = 0.80) and VR-extinction test (r = 0.87) had the highest correlation to BIT, corresponding R2 can be seen in table 3.
Table 3. Results Paper I, printed with permission from the publishers John Wiley & Sons Ltd, ACTA Neurologica Scandinavia 2011;123(3):167-174,”

38
The following kappa values were found when correlating the subtests of VR-DiSTRO with the corresponding conventional tests: VR-Extinction (Kappa = 0.65; P = 0.005), VR- Line Bisection (Kappa = 0.47; P = 0.012), VR- Star Cancellation Task (Kappa = 0.56; P = 0.004) and VR-Baking Tray Task (Kappa = 0.85; P = 0.001).
According to ISO 9241-11 standard (i.e., questions about usability), VR-DiSTRO® showed to be easy to learn and use, and no subjects reported nausea or side effect when using the VR-method. The experience of 3D VR was reported as interesting and no one reported discomfort.
Results Paper II. Training with RehAtt in Chronic Neglect Stability of symptoms were confirmed by revealing similar results from three repeated baseline investigations using VR-DiSTRO® and the Posner cuing task. (See paper II, table 2. for posthoc analysis). After RehAtt® intervention, subjects improved in three of four subtests as shown in Figure 11. A-D: Star Cancellation Task, mean improvement +6.43% (repeated measurement ANOVA, p<0.006); Baking tray task, +16.1% (p<0.001), Extinction + 13,9% (p<0.05).
After the RehAtt® training, improvement in spatial attention in daily activities was reported in CBS by the observer (p = 0.01) and by self-reports (p = 0.02), but not by next of kin. The subjects still reported improvement six months after the training session.
Regarding Posner cuing task, an improvement (p < 0.05) was seen in the analysis of percent missed targets (See paper II). The comparison of the post- to the mean of the tree pre-training scores is illustrated in Figure 12. However, no improvement was seen in reaction time (Posner unified index). These results were also valid for the 13 subjects available for task fMRI analysis. (Paper III)

39
Figure 11 (A)–(D) Behavioral results at the three repeated baselines visits and after RehAtt® training in four neglect tests. (A) Star cancellation test; (B) Baking tray task; (C) Extinction test; (D) Line bisection.
Figure 12. Behavioral Results %- Neglect tests scores, after training compared to mean of the 3 baseline values before training.

40
.
Figure 13. Baking Tray Task, conventional test and computerised in VR-DiSTRO using real time physics. With permission from K Thamm

41
Results Paper III and IV Changes in Neural Activity
fMRI data during Posner cueing condition (Paper III)
Cue condition First the evaluation of cortical activation for the cue condition compared to baseline rest condition was evaluated. The task activation during cue showed that the subjects recruited their bilateral IPS, their bilateral frontal eye field (i.e., the Dorsal Attention Network DAN) and their bilateral occipito-temporal cortex, and also parts of their dorsolateral prefrontal cortex (DLPFC) bilaterally. At the next step, we compared BOLD-signal intensity before and after intervention during this cue condition.(Fig.14) A significant difference as main effect of RehAtt® was observed in an extended cortical network. This included their anterior cingulate cortex (ACC), their DLPFC, and also their temporal cortex bilaterally. Compared to the task activation seen before intervention it only partially overlapped. (Fig. 14). After training, an increased activation was also seen in an extended fronto-temporal network when the arrow cue pointed to the left compared to when it was pointing to the right. (Fig.15.) A post-hoc analysis revealed that no reversed effects were shown.
Target condition During the part of Posner cuing task that include targets and target conditions, the participants primarily recruited following areas; superior motor cortex, the DLPFC, their middle temporal cortex and their cingulum. They also recruited Ventral Attention Network nodes such as the anterior insula, the temporal parietal junction TPJ, and the superior temporal sulcus. After the RehAtt® intervention, no significant main effect of training was revealed at this part of the Posner cuing task.

42
fMRI data during resting state (Paper IV)
The resting state interhemispheric functional connectivity between rFEF and lIPS increased following training (mean±SD, 0.33±0.17 vs 0.45±0.13 for pre and post rehabilitation session respectively, p=0.004), see Figure 17. This effect was still observed when removing patients with lesions at the rFEF coordinate (mean±SD, 0.35±0.17 vs 0.51±0.14, pre and post rehabilitation sessions respectively, p=0.002, N=8).
The two network maps that collectively represented the DAN showed a lower concordance between time points compared to the primary visual network (0.27±0.13 for left-hemisphere dominant and 0.29±0.12 for right-hemisphere dominant DAN networks versus 0.41±0.20 for the primary visual p=0.025 and p=0.025, respectively) supporting that the DAN had higher topological remapping compared to a network expected to remain stable.

43
Figure 14. Increased training-related BOLD-signal intensity during Posner cue condition
Figure 15. The main effect of VF during the cue conditions
A. Left B. Dorsal
D. Plots of training-related change0,5
0,40,3
0,2
0,10
-0,1-0,2
-0,3-0,4
-0,5-0,6
Pre-test Post-test
Beta
val
ues
C. Right F values45
40
30
20
14
35
25
A. Left B. Dorsal C. Right
D. Plots of main effect of VF
Beta
val
ues
Pre-test Post-test
0,4
0,2
0
-0,2
-0,4
-0,6
-0,8
F values
30
20
28
26
24
22
18
16
14

44
Figure legends to Fig. 14. (Previous page) Increased training-related BOLD-signal intensity during Posner cue condition. The task-activation pattern (cue activation > baseline resting condition) from the pre-test scanning is presented as a green outline to illustrate the contrast between the Posner cue condition and the resting baseline condition. (A-C) A significant training-related increased BOLD-signal response was observed within an extended cortical network including the ACC, the DLPFC, and the bilateral temporal cortex. (D) Mean beta values (estimated parameter values) from the cluster showing training-related effects are presented as plots contrasting Posner cue condition with the baseline resting condition when the arrow was pointing to the left (blue) or to the right (orange) VFs both at pre- and post-test. Error bars = standard errors.
Figure legends to Fig. 15. (Previous page) The main effect of VF during the cue conditions A significant main effect of VF indicates that the participants recruited the presented regions to a larger extent when the arrow cue was pointing to the left than to the right VF. (D) Mean beta values are presented as plots contrasting Posner cue condition with the baseline resting condition when the arrow was pointing to the left (blue) or the right (orange) VFs at the pre- and the post-test. Error bars = standard error.

45
Figure 16. Activation map for the que condition during the fMRI Posner task masked at t>2.8 for visualization purposes. The cluster peak coordinates of frontal eye fields and superior parietal lobules were used to construct region of interests for the connectivity analyses
Figure 17. Connectivity mean (SD) before (first row) and following rehabilitation (second row) between regions of interest within the dorsal attention network. Right and left frontal eye fields (lFEF and rFEF respectively) as well as the intraparietal sulcus (lIPS and rIPS respectively). P-values denote statistical difference comparing pre and post rehabilitation values.
0.45 (0.15)0.49 (0.17)
p=0.27
0.35 (0.17)0.39 (0.13)
p=0.11
0.51 (0.18)0.50 (0.20)
p=0.44
0.54 (0.09)0.53 (0.16)
p=0.39
0.33(0.17)
0.45(0.13)
p=0.004*0.34 (0.15)
0.37 (0.13)
p=0.24
R-FEFL-FEF
L-IPS R-IPS

46

47
Discussion Given the deeply damaging impact of spatial neglect on a third of all stroke patients, there is a need for new, effective and theory-based methods of diagnosis and rehabilitation.(76) This is challenging, because spatial neglect after stroke is a complex phenomenon and a multi-sensory impairment related to a breakdown in the brain’s attention networks. We addressed this void by developing an innovative form of test and training battery using virtual reality technology. The construct evaluation of the diagnostic part, VR-DiSTRO®, showed promising results regarding feasibility and accuracy in 31 stroke patients. Evaluation of RehAtt®, the training battery, in a sample of 15 subjects with chronic neglect revealed improved spatial attention both in tests and in activities of daily life. Training-related changes in brain neuronal activity that were seen in the fMRI evaluation, might indicate compensatory or restorative effects in targeted networks. VR-DiSTRO® and RehAtt® represents new concepts for the assessment and rehabilitation of spatial neglect. These new VR methods seem to have the potential to contribute to an improvement in the care of stroke patients.
VR-DiSTRO® In Paper I, we report the validation of VR-DiSTRO®, a computerised neglect test battery. The main results from Paper I indicate that the test battery components of VR-DiSTRO® showed moderate to high correlation when compared to the corresponding conventional tests. VR-DiSTRO® also identified all nine patients with neglect in a sample of 31 stroke patients. The usability was high and VR-DiSTRO® took a third of the time to perform compared to testing with the BIT battery.
The combination of tests in the VR-DiSTRO® was chosen to cover for different cognitive domains of the neglect phenomenon. The battery included a test for stimuli driven spatial attention (Extinction test), for goal-driven spatial attention (Star Cancellation test), and for visuomotor exploring (Baking Tray task, BTT) in an egocentric frame, also for

48
allocentric spatial awareness (Line Bisection), all performed in peripersonal space. The tests in VR-DiSTRO® could accurately identify neglect, using the BIT battery as criterion for neglect. Among the individual neglect tests included in the VR-DiSTRO®, VR-BTT had the highest kappa value, when compared to its conventional counterpart VR-BTT had the highest kappa value, when compared to its conventional counterpart. BTT is an example of a neglect test assessing impairment in visuomotor exploration in peripersonal space; it simulates the placement of buns on a tray, which is a functional test suitable for VR-environment (69). The moderate correlation between VR-Extinction test and “double simultaneous stimulation", compared to the wiggling fingers used in conventional Extinction (NIH-SS No 9)(107) might be caused by a more precise and controlled presentation of stimuli and collecting of response data using VR-DiSTRO®. Whether the extinction phenomenon should be included as part of the spatial neglect phenomenon has however been debated. (108-110) We consider that the computerised extinction test should stay as test in VR-DiSTRO® as it measures a limited attention capacity and exogenous attention.(111) In this study, VR-Extinction had high sensitivity to identify neglect.
We assume that the lower (moderate) kappa value for VR-SCT and VR-LB compared to conventional tests could be caused by a well-known weakness of low repeatability, especially for LBS, in test-re-test evaluations in acute/sub-acute stroke.(50) It could also be the different context; paper and pen compared to robotic pen and screen. Still, the cancellation test for neglect, to identify a skewed scanning pattern and impaired skill to identify targets/ figures spread among distractors is considered to be one of the most sensitive tests to identify impaired spatial attention.(112, 113) To include a cancellation tests is inevitable as part of the neglect test battery, and there are different ways to do this in VR-DiSTRO®. A cancellation test that includes identification of each targets left and right side would probably augment the VR-DiSTRO® to further measure for allocentric neglect (stimuli-centered). Adding tests similar to the Appletest (113) or Copy Picture test to the VR-DiSTRO® could also improve its capacity to assess allocentric neglect. The inclusion of LBS in

49
a test battery is disputed due to low and variable sensitivity and specificity as indicated by our results, but in this study, it has covered some for the allocentric part of the neglect.(114)
Because spatial attention is essential to many perceptual, cognitive, and motor functions there is a need for new easy to use screening methods for spatial neglect. Screening in stroke care is important in order to early identify patients with neglect for acute treatment, rehabilitation and to record improvement of neglect over time. VR-DiSTRO® is a novel, promising screening method with the potential to become a useful tool for neglect diagnosis.
RehAtt® RehAtt®, an intense scanning training enhanced by multi-sensory stimulation, was constructed into a 3D-game environment, designed according to current knowledge of neglect pathophysiology.(33) In Paper II, the effect of a five-week training with RehAtt® on long-standing neglect after stroke was evaluated. Outcome was assessed using the VR-DiSTRO® neglect-test battery described in Paper I, and with CBS for activities of daily living. In summary, visuospatial behaviour improved in tests and in activities of daily living, with a lasting effect reported six months after training.
The objective for Paper II was to create an effective and motivating training method for neglect. This was done by combining scanning training (top-down), a cluster of multi-sensory stimulating techniques (bottom-up), and activation of the paretic left hand using a haptic device. The training tasks were designed to stimulate the attention networks .(33)
VR as an enriched environment could be a primer for neuronal plasticity and contribute towards mending the broken brain.(29, 30, 115) Which single or combination of components in the RehAtt® design contribute the positive outcome of Paper II is not known. RehAtt® design combines a cluster of stimulating techniques (bottom-up) built into the 3D game environment. Audio, visual, and tactile cues guide patients towards the

50
contralesional peripersonal VR space.(116, 117) This was built into spatial attention training tasks designed to activate neuronal traffic in and between both DAN and VAN networks.(33) Bottom-up features included in RehAtt® are optokinetic stimulation, music, active 3D glasses, interactive force feedback including touch, and manipulation of 3D objects and rewards.
In Paper II, after training with RehAtt®, we found improvement in Star Cancellation test, Extinction test, and Posner Cueing test. This might result from the intense repetitions in scanning training (top-down tasks) in an enriched environment.(29) The intense training of a top-down scanning strategy, once well learned, might compensate so the person having long-standing neglect learns to be aware, for instance to consciously look to the left.(19) Such compensatory strategies might explain the improved performance in SCT and improved spatial attention seen in activities of daily living.
In Paper III and IV, we investigate whether the main cause of improvement seen from the RehAtt® training is due to a compensatory effect or if the method generates a more restorative mending effect in the brain, but this requires further study.
Even if promising results are seen in this sample of chronic neglect, ours is still a small study and the results must be confirmed in a prospective RCT. We trained only subjects with persistent symptoms of neglect in chronic phase after stroke, but RehAtt® should be applicable to the subacute stroke phase, within the first three months, when the potential and plausible training effect is known to be most effective.(28) The common use of the term “chronic neglect” should be considered.
Most of the literature about neglect rehabilitation is focused on the first few months after stroke. Regarding training effect achieved in chronic neglect, there are mainly case studies in the literature. From this standpoint, it is interesting that we could see improvements on spatial attention in chronic neglect after only 15 hours of training. In future

51
studies, it is highly important to evaluate persistence of training effects over time and generalization beyond tests to improvements in daily and social life.(1, 10)
Currently, there are no evidence-based methods to recommend for neglect rehabilitation.(10) Due to the available evidence, there are still recommendations to perform scanning training, general perception training in task and activity, and visuomotor activation of paretic arm.(73) The importance of individual training due to the heterogenicity profile of neglect symptoms are highlighted, and an enriched rehabilitation with a combination of methods is recommended.(19, 76) British, European, and American stroke guidelines recommend task-specific training for spatial neglect to be performed in stroke rehabilitation.(52-54, 58) This should preferably be done during the subacute phase due to knowledge of optimal brain plasticity window after stroke, but the majority of stroke survivors need to improve their function in the chronic phase.
In Paper II, we found a transfer from skills gained during training to activities of daily life. Other studies using VR have found different degree of transfer: In a study by Katz’, VR street-crossing training did not transfer to daily life (118); Kim et al. found training transfer after three weeks from activation of the non-paretic right arm using a 2D computer game in acute neglect patients(119); Van Kessel et al. did not find enhanced effects from using VR in driving simulator tasks(120). A recent meta-analysis of VR based training for spatial neglect states that VR methods are promising but further studies are needed, as well as the development of the optimal concept of VR hardware and software for neglect rehabilitation.(80, 95) VR for stroke rehabilitation has already been found to be significantly more effective than conventional therapy in improving upper limb motor function.(90)
Prism Adaptation (PA) (121) as being the probably most studied method for neglect by now, is known to improve several neglect symptoms, and in some studies gives a long-standing effect on skill transfer; but there remains a need to find out more about the neuronal mechanisms of

52
adaptation and what part of the population with neglect can benefit from the method.(83, 122, 123) As in RehAtt®, PA also targets visuomotor activation. In PA the non-paretic ipsilateral arm is used for pointing and in RehAtt® the paretic arm is activated with robotics. In PA, prism goggles are used and RehAtt® uses active 3D shutter glasses. RehAtt® is based on guided self-training in enriched VR game environments (enriched rehabilitation) that can be modulated by an assistant when needed. PA is always a therapist-led training but only requires prism googles and a pointing tool. RehAtt® was built from standard hardware components, has been designed for home rehabilitation and is suited for support using telemedicine. The equipment could be made available at stroke units and offered for home loans. In combination with the diagnostic VR-DiSTRO®, neglect could be assessed and improvement registered with repeated investigations.
The RehAtt®-training battery was designed and constructed to offer an intense, stimulating, and motivating self-training for neglect. The results of this study are promising and merit further development. Next steps include independent verification of our results in a randomized controlled multicentre trail. RehAtt® has the potential to become an effective intervention tool in hospitals and for in-home rehabilitation.
Restorative or compensatory effect? Spatial neglect is related to neuronal dysfunction in and between the brain’s attention networks. A key question raised in this study was whether the improved spatial attention was because patients learned a compensatory strategy (top-down) or if the training made a change in neuronal activity, i.e., a restorative effect (showed by an improved connectivity in and between attention networks and related cortical areas). Thus, we hypothesized that the improvement after RehAtt® training could be caused by either a compensatory or a restorative effect, or a combination.

53
The question was illuminated by two fMRI techniques: A. evaluation of change in neuronal activity from RehAtt® training by collecting data during task, and B. evaluation of connectivity in and between neuronal network during rest. By studying the change in fMRI signal during an attention task, we could assess a pattern of training related neuronal activation pointing towards a compensatory effect, i.e. activation outside the task network that we interpreted as compensatory recruitment of brain function to perform the task.
Training-related changes in neuronal activity were found during the cueing phase of the task activation when participants are hinted on the location of the stimuli that they are about to experience. Such tasks are conceived as assessing top-down modulatory systems of attention.(42) The changes could thus be interpreted as a sign of improved strategic compensatory function learned from RehAtt®. This was further supported by the prefrontal cortex localization of the new activation, mainly in the DLPFC and ACC areas, known to be activated in executive function.(124, 125) The activation of the prefrontal regions was in line with previous studies related to guiding attention and goal-directed behaviour.(126, 127) An interesting finding was that the BOLD signal intensity was enhanced when the cue pointed to the left side, potentially indicative of improved attention to the neglected side that also was seen in spatial behaviour outside the scanner.
Compensatory cortical activation from rehabilitation interventions has previously also been reported in chronic stroke patients with large cortical lesions, for instance after training of aphasia or arm paresis.(128) In a small study using fMRI to evaluate the effect of PA on spatial neglect, enhanced activity was found in multiple brain regions outside attention networks, indicating signs of compensatory effects.(37) RehAtt® was designed to train a compensatory scanning strategy by using VR, and thus the fMRI results during task in Paper III. are compatible with these intentions.

54
Possible training-related brain changes were also evaluated with resting state fMRI. Specifically, we examined resting state connectivity within key DAN regions that were localized using peak activations from the fMRI study (Paper III). Such connectivity has been shown to be indicative of neglect severity and amelioration in the acute phase.(33) We detected a longitudinal increase in interhemispheric DAN connectivity following the rehabilitation scheme. Next, we used a network similarity analysis (concordance) to assess possible changes in connectivity occurring outside the DAN. This analysis confirmed that the primary changes in the resting state connectivity occurred in the DAN. The detected increase in DAN connectivity concerned the right FEF and the left iPS. One possible interpretation of this observation is that the scanning training component of the rehabilitation scheme caused a restorative effect on attention networks improving control of eye movements and direction of spatial attention. In summary, fMRI investigation in this sample of chronic neglect patients revealed improved spatial attention from RehAtt® training, changes indicative of a compensatory effect by increasing top-down activation in prefrontal cortex, and a restorative effect seen as improved connectivity in attention networks.

55
Methodological Considerations and Limitations The main objective in paper I was to develop a technical platform for assessment of neglect. We performed a construct validation, a pilot study in a small sample of stroke patients. Further studies are needed, after an upgrade of the current version of VR-DiSTRO®, to establish a new assessment method for neglect. The testing of patients with coexisting neglect and left-sided hemianopsia is a special problem and needs to be addressed in upgrades of the VR-DiSTRO®.
Paper II-IV was an exploratory study of RehAtt® with main objective to design and technically develop the VR-method and also to evaluate its training effects in a small sample of subjects with chronic neglect. Due to limited economical resources, we could not perform a large-scale randomized controlled study. In this early stage of evaluation of a new method, we decided to use a multiple baseline design with a sample of chronic neglect subjects, in order to confirm a stable baseline.(46) According to the power analysis, we planned to recruit 40 subjects. However, due to insufficient data about neglect in the medical records, we had difficulties to identify patients that fulfilled the criteria. Another obstacle was the inclusion criteria requiring subjects to be able to visit the hospital in total 23 times. No drop out was reported in paper II-IV.All but one subject could be evaluated with MRI. Even if the study sample was small, we found significant training-related changes in neuronal activity in paper III and IV, indicating an effect of RehAtt®. This merit and stimulate to proceed with further research and development using this methodology. A control group had been desirable in the MRI papers, as well as in Paper II. A shortcoming is the lack of diffusion tensor imaging with detailed information about structural lesions and symptom mapping analysis. In paper III, the Posner cuing test was chosen because it has been used in previous neglect studies.(33) However, this task has limitations and future tasks in fMRI may be improved by relating to ecological effects. We had problems with movement artefacts in paper III. A benefit using resting state, as in paper IV, is that there is no need for subjects to interact and thus, movement artefact may be reduced.

56
Figure 18. VR, from top;1. the author is supervising the Swedish King Carl XVI Gustaf, using VR- RehAtt, wearing 3D-glasses and holding the haptic device. Middle: next generation Augmented Reality;(HoloLens), semi immersed VR wherein the room becomes the canvas for VR holograms. Bottom; fully immersed VR(Oculus Rift). The screens allow observers to see what the user of VR is seeing. 1.Printed with permission Mikael Hansson.

57
Future Directions VR for stroke rehabilitation is a rapidly growing field.(80) A flood of new VR methods are now being evaluated in small and exploratory studies. (95) To confirm the true potential of VR therapies in various clinical populations, it is important that positive results from these studies are established in large, longitudinal and randomized trials. For patients and relatives, it is also important that the training effect could be generalized to improved function in daily living. To establish best-practice guidelines for neglect treatment with VR methods, it is important to standardize the methodology. For instance, type of neglect symptoms has to be described in detail and related to pathophysiological mechanisms. The technology should be described as immersed to non-immersed VR. Exposed field of view, interaction, proprioceptive input, the gamification and if reward systems should also be included. In the development of new VR-methods the need of therapist support should be evaluated as future rehabilitation will probably mainly be performed at home. The VR-technology offers great opportunities to enhance task specific training.
The future winning concept of VR-therapy for neglect rehabilitation is the combination of training methods, for example motor and cognitive dysfunction. By creating an enriched environment in VR it might become an excellent method to stimulate brain neuroplasticity. The future direction seems to be to enhance training effect by combining VR -methods with neurostimulation. This could be done by non-invasive brainstimulation, pharmacological, neuro-feedback techniques and in combination with neuroimaging.(81)These first evaluations of VR-DiSTRO® and RehAtt®, pilots ahead of larger trials, have given useful guidance how to further develop the methods, as well as insights into research design.
One winning concept to create effective and useful methods for neglect patients is to embrace the necessity and potential of interdisciplinary collaboration between scientists, neurologists, occupational therapists, physiotherapists, psychologists and engineers. Then new methods will emerge that will improve the daily living for those affected by stroke.

58
Conclusions I. A diagnostic VR battery, VR-DiSTRO®, was constructed. The VR-DiSTRO® identified visuospatial neglect quickly and with high sensitivity and specificity. The computerised tests correlated well with conventional tests and had a high usability. In the future, VR-DiSTRO® has the potential to become a useful tool for the screening and assessment of spatial neglect.
II. A VR training battery, RehAtt®, was constructed. After training, patients showed improvement in spatial attention on behavioural tests and improved function in daily activities, both immediately and reported at six months follow up after training. In the future, RehAtt® can become an effective training tool in stroke rehabilitation for inpatients and outpatients and for in-home rehabilitation.
III. Training with RehAtt® revealed increased task-evoked brain activity in an extended network including prefrontal and temporal cortex during attention cueing, indicative of a compensatory effect.
IV. RehAtt® that improved left side awareness in chronic stroke patients also increased intrinsic, resting state interhemispheric connectivity within the DAN. Interestingly a region for eye movements became more integrated with the left posterior parietal cortex. The improved connectivity in attention networks can be interpreted as a restorative neural effect from training. These results merit for further studies.

59
Sammanfattning på svenska Stroke är den vanligaste orsaken till hjärnskada och långvarig funktionsnedsättning. Förutom förlamning så orsakar stroke kognitiva svårigheter. Det kan innebära svårigheter att tala, tänka, minnas, lösa problem och att fatta beslut. Var tredje strokepatient drabbas av en uppmärksamhetsstörning som kallas spatialt neglekt. Spatialt neglekt är för många ett svårt men dolt handikapp som kan ge en livslång funktionsnedsättning. Det påverkar möjligheten att bli självständig och oberoende igen efter stroke.
Definitionen av spatialt neglekt är svårigheter att reagera, förstå och agera på ljud-, känsel- och synintryck som kommer mot den sida av kroppen som är motsatt den där man fått sin hjärnskada, oftast högersidig skada. Spatialt neglekt, eller neglekt, är ett komplext fenomen som omfattar mer än enbart nedsatt rumslig uppmärksamhet till vänster. Det omfattar även en generell uppmärksamhetsstörning med svårigheter att vara alert, koncentrera sig och skifta fokus. Det innebär även en nedsatt medvetenhet om, och en nedsatt kontroll av vänster sida av kroppen. Det här leder till svårigheter att röra sig på ett säkert sätt, att hitta i sin omgivning, ta sig fram i trafik, att hänga med i samtal, läsa och klara sina vardagssysslor. Det saknas effektiva metoder för att diagnostisera tillståndet, vilket innebär att man kan missa möjlighet till akutbehandling och rehabilitering. Det saknas vetenskapligt underlag för effektiv rehabilitering. Hälften av de som har neglekt vid insjuknandet drabbas av bestående funktionsnedsättning, s.k. kroniskt neglekt (> sex månader efter insjuknandet). Detta trots att de fått traditionell strokerehabilitering som t.ex. kan vara att träna avsökning, aktivering och stimulering av vänster sida i vardagsaktiviteter. Neglekt är ett vanligt och allvarligt tillstånd som påverkar livskvalitet efter stroke. Därför finns ett stort behov av att ta fram mer effektiv screening och specifik behandling för neglekt.
Idag finns kunskap om hur man kan påverka hjärnans fortsatta läkningsförmåga många år efter en stroke. Med rätt stimulans och högintensiv träning kan funktion förbättras i det som ännu kallas för

60
”kronisk fas” efter stroke. Att träna i en berikad och stimulerande rehabiliteringsmiljö (s.k. enriched environment) har setts förstärka träningseffekt. Virtual reality (VR) är en teknologi som visat sig effektiv för att träna upp funktion i en förlamad hand efter stroke. I VR kan man skapa en dataproducerad miljö som man kan interagera i. VR lämpar sig väl som plattform för att utveckla tester och träningsmetoder för uppmärksamhet. Fördelar med tester i VR är att varje testtillfälle blir lika och repeterbart, samt att resultat och beteende registreras direkt av datorn.
Möjliga fördelar med träning i VR är att träningseffekten bör kunna förstärkas i och med att man tränar intensivt i en stimulerande och motiverande miljö som inkluderar flera sinnen. Intensiv träning av en funktion som görs i en berikad miljö, t.ex. i form av neglekttränng i VR-spel, kan bli en form av berikad rehabilitering att användas som ett tillägg till vardagsrehabilitering. Teoretiskt bör utformning av test och träningsuppgifter för rumslig uppmärksamhet bygga på kunskap om de av hjärnans mekanismer har skadats när man uppvisar neglekt. Man vet att ”signaltrafiken” då är störd inom och mellan nyckelområden i hjärnan. Dessa regioner i både höger och vänster hjärnhalva behöver samverka i funktionella neuronala uppmärksamhetsnätverk. När stroke skadar hjärnans strukturer störs signaltrafiken även till och inom oskadda områden.
Nya träningsmetoder för neglekt har föreslagits. Dessa bör kombinera metoder som att lära en strategi för avsökning (dvs. medveten inlärning, s.k. top-down) med stimulering av sinnen (s.k. bottom-up). För att utvärdera effekt av nya metoder kan funktionell magnetkamera (fMRI) teknik användas. Då kan man indirekt följa skillnad i aktiveringsmönster (BOLD-signal) när man löser en uppgift (task). Även neuronal trafik i vila (resting state) före och efter träningsperioden kan undersökas. I den här avhandlingen använder vi fMRI för att studera en ny träningsmetod och hur den påverkar neuronal aktivering i och mellan de två bakre (DAN) och det högersidiga främre (VAN) uppmärksamhetsnätverken och relaterade regioner.

61
Detta avhandlingsarbete fokuserar på att designa, utveckla och utvärdera nya metoder för neglekt med stöd av VR-teknik i form av ett testbatteri och ett träningsbatteri. Hypotesen var att att med fyra datoriseriserade neglekttester, som undersöker olika uppmärksamhetsfunktioner snabbt och säkert kunna identifiera vilka strokepatienter som har neglekt jämfört med att göra 15 tester i BIT (Behavioral Inattention Test battery). Genom att träna med en VR-metod som kombinerar inlärning av en sökstrategi med en simulerande träningsmiljö och aktivering av förlamad arm med robotik bör uppmärksamhetsfunktionen kunna förbättras även i vid neglekt i den s.k. kroniska fasen. Förbättrad uppmärksamhet av VR-metoden bör kunna ses i tester och i vardagsaktiviteter, även i förstärkt signaltrafik i hjärnan.
I det här avhandlingsarbetet utvecklades ett nytt koncept med VR teknik för diagnostik (VR-DiSTRO®) och träning (RehAtt®) av neglekt. Hårdvaran bestod av en dator, bildskärm och 3D-glasögon. För att styra uppgifterna användes en utrustning som gav kraftåterkoppling, en s.k. robotpenna (Phantom Omni). Programvaran (Colosseum 3D) möjliggjorde att objekt kunde flyttas, roteras och placeras i 3D-miljön med robotpennan. RehAtt gjorde det möjligt att kombinera intensiv visuell skanningsträning, (strategi för avsökning) med multisensorisk stimulering (dvs. syn, hörsel och känsel) och sensorimotor-aktivering av den förlamade armen. Tester utfördes med frisk arm. I den första studien genomfördes en konstruktvalidering av testbatteriet VR-DiSTRO mot BIT på 31 strokepatienter. Metodens användbarhet utvärderades även enligt ISO standard. Till Studie II-IV inkluderades 15 personer med kvarstående neglekt efter i medeltal 3,3 år, efter ischemiskt stroke i höger hjärnhalva. De fick under en fem veckor lång baslinjeperiod utföra fem neglekt-tester vid tre tillfällen, för att säkerställa stabila besvär. Därigenom uteslöts även en eventuell effekt av att upprepade tester. Därefter kom de för träning med VR-metoden RehAtt® 15 timmar totalt (3 x 1 tim per vecka under 5 veckor). Direkt efter utvärderades effekt med testbatteriet igen. En bedömning av metodens effekt på uppmärksamhet i vardagsaktiviteter gjordes med Catherine Bergego Scale (CBS), där en uppföljning också gjordes sex månader efter träningsperioden. Före och efter

62
träningsperioden gjordes en fMRI-undersökning av hjärnans aktivitet dels när de utförde en uppgift, dels i vila.
I delarbete I utvecklades och utvärderades ett datoriserat testbatteri VR-DiSTRO®. Jämfört med ett omfattande testbatteri med 15 tester kunde dessa fyra tester hitta alla nio patienter med neglekt bland 31 strokepatienter. Med VR-DiSTRO® tog det 15 minuter att utföra jämfört med 50 minuter för BIT. Varje datoriserat test jämfördes också med motsvarande standardtest och jämförelsen visade mycket god till måttlig överensstämmelse. Användbarheten för VR-metoden bedömdes hög, metoden var lätt att lära och hade inga negativa bieffekter. I delarbete II observerades en förbättring av uppmärksamhetsfunktion i fyra av fem neglekttester efter träningsperioden. Förbättrad uppmärksamhet sågs i vardagsaktivitet och patienterna rapporterade en bestående förbättring efter sex månader.
I delarbete III observerades med fMRI, efter träningsperioden, en förstärkt hjärnaktivering när patienten utförde en uppgift (task). Nya aktiveringsområden observerades även i den främre delen av hjärnan. I delarbete IV, efter träningsperioden, fann vi en förstärkt signaltrafik när patienten vilade (rest). Förstärkningen sågs till områden som hör till bakre uppmärksamhetsnätverket i den vänstra hjärnhalvan.
VR-DiSTRO® kunde snabbt och säkert identifiera strokepatienter med neglekt. Efter träning med RehAtt® förbättrades patienterna i såväl uppmärksamhet som ADL-funktioner. En förstärkt hjärnaktivering sågs i och mellan uppmärksamhetsnätverk och relaterade hjärnområden. Detta kan ses som tecken på möjlig kompensatorisk effekt och även en läkningseffekt av RehAtt®. Resultaten i den här avhandlingen är lovande och uppmuntrar till nästa steg att konfirmera resultaten i en större randomiserad kontrollerad studie.

63
Acknowledgements I wish to express my sincere gratitude to everyone who in any way has supported me in this project. First and foremost, thank you to my main supervisor, Jan Malm. Thank you for being bold and brilliant and giving scientific guidance with inexhaustible patience as you challenged me to be my best. Thank you for the time and financial support that enabled me to turn my vision of researching virtual reality into reality. A thousand thanks also to my excellent co-supervisor Anders Eklund for generously giving me all the support and time needed. Thank you both for helping me to grasp the precision and details required in scientific thinking and writing. Thanks for encouraging me to set the bar high. You make an impressive team. To my excellent co-authors, Urban Ekman and Anders Wåhlin, I offer a sincere and warm thank you for your substantial contribution to the fMRI works presented in this thesis, for incisive analysis and fruitful discussions and co-writing. Thank you for being great collaborators and for your ceaseless positivity. Thanks to Johan Eriksson, for reflective and analytic input in paper III. Thanks to Gösta Bucht for your support at the very first steps with the project and part in paper I. Thanks to Niklas Lenfeldt for your contribution to funding the fMRI, for valuable comments and analytic insights. Sincere gratitude to Aina Ågren Vilson who so generously contributed to funding and for your steady support.
Thanks to you who believed in me, encouraged and supported me at the Department of Integrative Medical Biology (IMB); Lars Nyberg for important guidance in the project and insightful comments. Thanks to Roland Johansson and Benoni Edin for important encouragement and discussions about design at the start point, to Mikael Andersson for technical support and to Göran Westling for constructing MR compatible equipment. Thanks to the team at Department of Radiation Sciences, the MR staff for unweariedly supporting (sometimes weary) neuroscientists and strained participants. A special thanks to Richard Birgander for help with lesion analysis, your encouragement, and for sharing thoughts about life.

64
I am also grateful for the important collaboration of computer scientists Kenneth Bodin and Anders Backman at the start of this research project. By entering into a technical collaboration with the VR-lab and HPC2N, they helped to ensure the technical competence of this project. Thanks to all the computer engineers during these years whose invaluable effort developed the technical platform.
A special warm thank you to occupational therapist Eva Lundström for your wise and insightful advice in method design to make it effective. Also thank you dear teammate Birgitta Johansson, who taught me the most important lessons about neglect and VR and for sharing your experience in how best to improve screening assessment and training for neglect to make it useful. Thanks to all you national and international pioneers in VR who so generously shared with me your experiences in using VR for rehabilitation.
Thanks to local colleagues in stroke research for seeing the possibilities in my project idea. To Bo Carlberg for teaching me how to make a start. To the team that included Weigang Gu and Per Dahlquist, for the encouragement and discussions about how to study brain plasticity after stroke and the impact of environmental enrichment. Thanks to Xiao-Lei Hu, Eva-Lotta Glader, Johanna Pennlert, Marie Eriksson, Anna Bråndahl, Charlotte Häger, Laleh Zarrinkob, Elias Johansson and Thomas Gu. Thank you for being bold and brilliant, crossing borders, let us continue to build multidisciplinary stroke research. I look forward to future work, collaborations, and further development of telemedicine for stroke home rehabilitation where a special thank you goes to Käte Alrutz and Thomas Molén for pioneering work in E-health: seeing the possibilities and realising them. Thank you all my lovely teammates at Strokecenter Norrlands Universitetssjukhus since 2002 – noone mentioned and noone forgotten - who have been there and cheered me up and made me proud to be part of a fantastic team that always puts patients first. A special thanks to Monika, Anna, Sara, Britta, Bim, Maria and Åsa for your never-ending enthusiasm to improve our work and supporting ongoing research

65
projects. Thanks Neurorehab Sävar for your support and pioneering work as a centre using VR, with special thanks to Lena Lundman Myrlund.
To my stroke colleagues whose support and friendship means a lot, let us continue to work together to cross borders, to be brave and brilliant and to seek to give the best care and evidence based treatment to our stroke patients. Thank you Maj Mattson for sharing your passion in working to rehabilitate stroke patients with love, respect and a good sense of humour. Thanks for being visionary fifteen years ago about how VR-technology could meet neuroscience to create effective, fun and motivating attention training, and assess neglect symptoms. Thanks to all of you taking my share on the ward when I needed time for research.
Sincere gratitude to my bosses Hans Lindsten and Johan Jacobsson for your support and for having confidence in me.To my neuro-colleagues who took an interest and encouraged me throughout the time it took to write this thesis, especially Peter Andersen. Thanks to Marwan Hariz for inviting me to London and pointing out directions toward new horizons. Thanks to Elisabeth Lindmark and Per Åke Ridderheim for your steady support and your love. Thanks to Kicki Nyman and Jörgen Andersson for being there whenever I needed you.
A special thanks to Camilla Heyl. The fact that no study participant dropped out is evidence of how outstanding you were. A warm thank you to each patient who participated in the trials and to their relatives for their support. For all of you who stayed onboard throughout this journey, a great big thank you! Thanks to all and everyone who contributed to this project by thinking hard and taking part in discussions that led this work forward. I am grateful to all of my tireless collaborators who were the best I could have asked for.
And a special thanks to my steady teammate Derny Häggström, local pioneer in the use of simulation technology. Thank you, Derny, for your endless support in all weathers.

66
Special and heartfelt thanks to my dear children: Liv, Leo and Vidar and partners for your support, patience and love. Thanks also to Mom and Dad, Thomas, Ulla, Oscar and Åsa for your love, care and encouragement. To Maria my lovely wise friend for helping me find my bearings when I needed to and to everyone in my circle of dear friends for loving me as I am.
To my darling and tutor Sebastian Secker Walker, thank you for giving me endless love and encouragement, for giving me new perspectives and making every single day a Happy Day. I adore you!

67

68
.
Grants
Financial support was provided through a regional agreement between Umeå University and Västerbotten County Council (ALF), Neurologens forskningsfond, “Strokeforskning i Norrland- insamlingsstiftelse”. Swedish Stroke Association, Neuro Sweden Association and EU founding Objective One.
Disclosure:
Helena Fordell is founder of a start-up company in order to correctly assign the research results to the company Brain Stimulation AB, partly owned and financed by Umeå University Holding AB.
RehATT®- and VR-DiSTRO® are registred trademarks protected by law.

69
References 1. Chen P, Hreha K, Kong Y, Barrett AM. Impact of spatial neglect on stroke
rehabilitation: evidence from the setting of an inpatient rehabilitation facility. Arch Phys Med Rehabil. 2015;96(8):1458-66.
2. Gillen R, Tennen H, McKee T. Unilateral spatial neglect: relation to rehabilitation outcomes in patients with right hemisphere stroke. Arch Phys Med Rehabil. 2005;86(4):763-7.
3. Jehkonen M, Laihosalo M, Kettunen JE. Impact of neglect on functional outcome after stroke: a review of methodological issues and recent research findings. Restor Neurol Neurosci. 2006;24(4-6):209-15.
4. Sacco RL, Kasner SE, Broderick JP, Caplan LR, Connors JJ, Culebras A, et al. An updated definition of stroke for the 21st century: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2013;44(7):2064-89.
5. GBD 2015 Neurological Disorders Collaborator Group. Global, regional, and national burden of neurological disorders during 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Neurol. 2017;16(11):877-97.
6. Farne A, Buxbaum LJ, Ferraro M, Frassinetti F, Whyte J, Veramonti T, et al. Patterns of spontaneous recovery of neglect and associated disorders in acute right brain-damaged patients. J Neurol Neurosurg Psychiatry. 2004;75(10):1401-10.
7. Corbetta M, Ramsey L, Callejas A, Baldassarre A, Hacker CD, Siegel JS, et al. Common behavioral clusters and subcortical anatomy in stroke. Neuron. 2015;85(5):927-41.
8. Jacobs S, Brozzoli C, Farne A. Neglect: a multisensory deficit? Neuropsychologia. 2012;50(6):1029-44.
9. Azouvi P, Samuel C, Louis-Dreyfus A, Bernati T, Bartolomeo P, Beis JM, et al. Sensitivity of clinical and behavioural tests of spatial neglect after right hemisphere stroke. J Neurol Neurosurg Psychiatry. 2002;73(2):160-6.
10. Bowen A, Hazelton C, Pollock A, Lincoln NB. Cognitive rehabilitation for spatial neglect following stroke. The Cochrane database of systematic reviews. 2013(7):Cd003586.
11. Heilman KM BD, Valenstein E, Watson RT. . Hemispace and hemispatial neglect. Neurophysiological and neuropsychological aspects of spatial neglect, Jeannerod M (Ed). 1987;1987: 115-150:115-50.
12. Umarova RM, Nitschke K, Kaller CP, Kloppel S, Beume L, Mader I, et al. Predictors and signatures of recovery from neglect in acute stroke. Ann Neurol. 2016;79(4):673-86.
13. Cassidy JM, Cramer SC. Spontaneous and Therapeutic-Induced Mechanisms of Functional Recovery After Stroke. Translational stroke research. 2017;8(1):33-46.
14. Karnath HO, Rennig J, Johannsen L, Rorden C. The anatomy underlying acute versus chronic spatial neglect: a longitudinal study. Brain. 2011;134(Pt 3):903-12.

70
15. Nijboer TC, Kollen BJ, Kwakkel G. Time course of visuospatial neglect early after stroke: a longitudinal cohort study. Cortex. 2013;49(8):2021-7.
16. Bohil CJ, Alicea B, Biocca FA. Virtual reality in neuroscience research and therapy. Nat Rev Neurosci. 2011;12(12):752-62.
17. Cramer SC. Repairing the human brain after stroke. II. Restorative therapies. Ann Neurol. 2008;63(5):549-60.
18. Barrett AM, Buxbaum LJ, Coslett HB, Edwards E, Heilman KM, Hillis AE, et al. Cognitive rehabilitation interventions for neglect and related disorders: moving from bench to bedside in stroke patients. J Cogn Neurosci. 2006;18(7):1223-36.
19. Riestra AR, Barrett AM. Rehabilitation of spatial neglect. Handb Clin Neurol. 2013;110:347-55.
20. Gerafi J, Samuelsson H, Viken JI, Blomgren C, Claesson L, Kallio S, et al. Neglect and aphasia in the acute phase as predictors of functional outcome 7 years after ischemic stroke. Eur J Neurol. 2017;24(11):1407-15.
21. Nijboer T, van de Port I, Schepers V, Post M, Visser-Meily A. Predicting functional outcome after stroke: the influence of neglect on basic activities in daily living. Front Hum Neurosci. 2013;7:182.
22. Jehkonen M, Laihosalo M, Koivisto AM, Dastidar P, Ahonen JP. Fluctuation in spontaneous recovery of left visual neglect: a 1-year follow-up. Eur Neurol. 2007;58(4):210-4.
23. Katz N, Hartman-Maeir A, Ring H, Soroker N. Functional disability and rehabilitation outcome in right hemisphere damaged patients with and without unilateral spatial neglect. Arch Phys Med Rehabil. 1999;80(4):379-84.
24. Jehkonen M, Ahonen JP, Dastidar P, Koivisto AM, Laippala P, Vilkki J, et al. Visual neglect as a predictor of functional outcome one year after stroke. Acta Neurol Scand. 2000;101(3):195-201.
25. Rode G PC, Huchon L, Rosetti Y, Pisella L. Semiology of neglect: An update. Ann Phys Rehabil Med. 2017;60(3):177-85.
26. Vuilleumier P. Mapping the functional neuroanatomy of spatial neglect and human parietal lobe functions: progress and challenges. Ann N Y Acad Sci. 2013;1296:50-74.
27. Cramer SC, Riley JD. Neuroplasticity and brain repair after stroke. Curr Opin Neurol. 2008;21(1):76-82.
28. Cramer SC. Repairing the human brain after stroke: I. Mechanisms of spontaneous recovery. Ann Neurol. 2008;63(3):272-87.
29. Corbett D, Nguemeni C, Gomez-Smith M. How can you mend a broken brain? Neurorestorative approaches to stroke recovery. Cerebrovasc Dis. 2014;38(4):233-9.
30. Corbett D, Jeffers M, Nguemeni C, Gomez-Smith M, Livingston-Thomas J. Lost in translation: rethinking approaches to stroke recovery. Prog Brain Res. 2015;218:413-34.
31. Levin MF, Kleim JA, Wolf SL. What do motor "recovery" and "compensation" mean in patients following stroke? Neurorehabil Neural Repair. 2009;23(4):313-9.

71
32. Krakauer JW, Carmichael ST, Corbett D, Wittenberg GF. Getting neurorehabilitation right: what can be learned from animal models? Neurorehabil Neural Repair. 2012;26(8):923-31.
33. Corbetta M, Shulman GL. Spatial neglect and attention networks. Annu Rev Neurosci. 2011;34:569-99.
34. Lunven M, Thiebaut De Schotten M, Bourlon C, Duret C, Migliaccio R, Rode G, et al. White matter lesional predictors of chronic visual neglect: a longitudinal study. Brain. 2015;138(Pt 3):746-60.
35. Thiebaut de Schotten M, Tomaiuolo F, Aiello M, Merola S, Silvetti M, Lecce F, et al. Damage to white matter pathways in subacute and chronic spatial neglect: a group study and 2 single-case studies with complete virtual "in vivo" tractography dissection. Cereb Cortex. 2014;24(3):691-706.
36. Carter AR, McAvoy MP, Siegel JS, Hong X, Astafiev SV, Rengachary J, et al. Differential white matter involvement associated with distinct visuospatial deficits after right hemisphere stroke. Cortex. 2017;88:81-97.
37. Saj A, Cojan Y, Vocat R, Luaute J, Vuilleumier P. Prism adaptation enhances activity of intact fronto-parietal areas in both hemispheres in neglect patients. Cortex. 2013;49(1):107-19.
38. Biswal B, Yetkin FZ, Haughton VM, Hyde JS. Functional connectivity in the motor cortex of resting human brain using echo-planar MRI. Magn Reson Med. 1995;34(4):537-41.
39. Baldassarre A, Ramsey L, Rengachary J, Zinn K, Siegel JS, Metcalf NV, et al. Dissociated functional connectivity profiles for motor and attention deficits in acute right-hemisphere stroke. Brain. 2016;139(Pt 7):2024-38.
40. Baldassarre A, Ramsey LE, Siegel JS, Shulman GL, Corbetta M. Brain connectivity and neurological disorders after stroke. Curr Opin Neurol. 2016;29(6):706-13.
41. Ramsey LE, Siegel JS, Baldassarre A, Metcalf NV, Zinn K, Shulman GL, et al. Normalization of network connectivity in hemispatial neglect recovery. Ann Neurol. 2016;80(1):127-41.
42. He BJ, Snyder AZ, Vincent JL, Epstein A, Shulman GL, Corbetta M. Breakdown of functional connectivity in frontoparietal networks underlies behavioral deficits in spatial neglect. Neuron. 2007;53(6):905-18.
43. Corbetta M, Kincade MJ, Lewis C, Snyder AZ, Sapir A. Neural basis and recovery of spatial attention deficits in spatial neglect. Nat Neurosci. 2005;8(11):1603-10.
44. Mesulam MM. A cortical network for directed attention and unilateral neglect. Ann Neurol. 1981;10(4):309-25.
45. Corbetta M, Kincade MJ, Lewis C, Snyder AZ, Sapir A. Neural basis and recovery of spatial attention deficits in spatial neglect. Nat Neurosci. 2005;8(11):1603-10.
46. Thimm M, Fink GR, Kust J, Karbe H, Willmes K, Sturm W. Recovery from hemineglect: differential neurobiological effects of optokinetic stimulation and alertness training. Cortex. 2009;45(7):850-62.
47. Sturm W, Thimm M, Kust J, Karbe H, Fink GR. Alertness-training in neglect: behavioral and imaging results. Restor Neurol Neurosci. 2006;24(4-6):371-84.

72
48. Thimm M, Fink GR, Kust J, Karbe H, Sturm W. Impact of alertness training on spatial neglect: a behavioural and fMRI study. Neuropsychologia. 2006;44(7):1230-46.
49. Rossetti Y, Rode G, Pisella L, Farne A, Li L, Boisson D, et al. Prism adaptation to a rightward optical deviation rehabilitates left hemispatial neglect. Nature. 1998;395(6698):166-9.
50. Azouvi P, Olivier S, de Montety G, Samuel C, Louis-Dreyfus A, Tesio L. Behavioral assessment of unilateral neglect: study of the psychometric properties of the Catherine Bergego Scale. Arch Phys Med Rehabil. 2003;84(1):51-7.
51. Socialstyrelsen. Nationella riktlinjer för vård vid stroke 2017 [Available from: http://www.socialstyrelsen.se/publikationer2017/2017-5-13.
52. Bernhardt J, Hayward KS, Kwakkel G, Ward NS, Wolf SL, Borschmann K, et al. Agreed Definitions and a Shared Vision for New Standards in Stroke Recovery Research: The Stroke Recovery and Rehabilitation Roundtable Taskforce. Neurorehabil Neural Repair. 2017;31(9):793-9.
53. C. HE. Cognitive Rehabilitation Manual: Translating Evidence-Based Recommendations into Practice. Arch Clin Neuropsychology 2012;Dec(8):931–2.
54. Winstein CJ, Stein J, Arena R, Bates B, Cherney LR, Cramer SC, et al. Guidelines for Adult Stroke Rehabilitation and Recovery: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2016;47(6):e98-e169.
55. Tulsky DS, Carlozzi NE, Cella D. Advances in outcomes measurement in rehabilitation medicine: current initiatives from the National Institutes of Health and the National Institute on Disability and Rehabilitation Research. Arch Phys Med Rehabil. 2011;92(10 Suppl):S1-6.
56. Halligan PW, Marshall JC, Wade DT. Visuospatial neglect: underlying factors and test sensitivity. Lancet. 1989;2(8668):908-11.
57. Azouvi P, Bartolomeo P, Beis JM, Perennou D, Pradat-Diehl P, Rousseaux M. A battery of tests for the quantitative assessment of unilateral neglect. Restor Neurol Neurosci. 2006;24(4-6):273-85.
58. London: ISWP, Royal College of Physicians. National clinical guideline for stroke, 5th edition. Royal College of Physicians, 2016. 2016;5th edition(https://www.strokeaudit.org/Guideline/Historical-Guideline/National-Clinical-Guidelines-for-Stroke-fourth-edi.aspx).
59. Wilson B, Cockburn J, Halligan P. Development of a behavioral test of visuospatial neglect. Arch Phys Med Rehabil. 1987;68(2):98-102.
60. Ten Brink AF, Visser-Meily JMA, Nijboer TCW. Dynamic assessment of visual neglect: The Mobility Assessment Course as a diagnostic tool. J Clin Exp Neuropsychol. 2017:1-12.
61. Vallat-Azouvi C, Dana-Gordon C, Mazaux JM, Ponsford J, Azouvi P. Psychometric properties of the French version of the Rating Scale of Attentional Behaviour. Neuropsychol Rehabil. 2017:1-14.
62. Rengachary J, d'Avossa G, Sapir A, Shulman GL, Corbetta M. Is the posner reaction time test more accurate than clinical tests in detecting left neglect in acute and chronic stroke? Arch Phys Med Rehabil. 2009;90(12):2081-8.
63. Azouvi P. The ecological assessment of unilateral neglect. Ann Phys Rehabil Med. 2017;60(3):186-90.

73
64. Chen P, Hreha K, Fortis P, Goedert KM, Barrett AM. Functional assessment of spatial neglect: a review of the Catherine Bergego scale and an introduction of the Kessler foundation neglect assessment process. Top Stroke Rehabil. 2012;19(5):423-35.
65. Chen P, Chen CC, Hreha K, Goedert KM, Barrett AM. Kessler Foundation Neglect Assessment Process uniquely measures spatial neglect during activities of daily living. Arch Phys Med Rehabil. 2015;96(5):869-76.e1.
66. Menon-Nair A, Korner-Bitensky N, Ogourtsova T. Occupational therapists' identification, assessment, and treatment of unilateral spatial neglect during stroke rehabilitation in Canada. Stroke. 2007;38(9):2556-62.
67. Buxbaum LJ, Palermo MA, Mastrogiovanni D, Read MS, Rosenberg-Pitonyak E, Rizzo AA, et al. Assessment of spatial attention and neglect with a virtual wheelchair navigation task. J Clin Exp Neuropsychol. 2008;30(6):650-60.
68. Brott T, Adams HP, Jr., Olinger CP, Marler JR, Barsan WG, Biller J, et al. Measurements of acute cerebral infarction: a clinical examination scale. Stroke. 1989;20(7):864-70.
69. Tham K. The baking tray task: a test of spatial neglect. Neuropsychol Rehabil. 1996;6(1):19-26.
70. Appelros P, Karlsson GM, Thorwalls A, Tham K, Nydevik I. Unilateral neglect: further validation of the baking tray task. J Rehabil Med. 2004;36(6):258-61.
71. Potter J, Deighton T, Patel M, Fairhurst M, Guest R, Donnelly N. Computer recording of standard tests of visual neglect in stroke patients. Clin Rehabil. 2000;14(4):441-6.
72. Broeren J, Samuelsson H, Stibrant-Sunnerhagen K, Blomstrand C, Rydmark M. Neglect assessment as an application of virtual reality. Acta Neurol Scand. 2007;116(3):157-63.
73. Haskins EC. The ACRM Cognitive Rehabilitation Manual;. American Congress of Rehabilitation Medicin. 2012(ISBN: 978-0615538877).
74. Pizzamiglio L, Guariglia C, Antonucci G, Zoccolotti P. Development of a rehabilitative program for unilateral neglect. Restor Neurol Neurosci. 2006;24(4-6):337-45.
75. Luukkainen-Markkula R, Tarkka IM, Pitkanen K, Sivenius J, Hamalainen H. Rehabilitation of hemispatial neglect: A randomized study using either arm activation or visual scanning training. Restor Neurol Neurosci. 2009;27(6):663-72.
76. Kerkhoff G, Schenk T. Rehabilitation of neglect: an update. Neuropsychologia. 2012;50(6):1072-9.
77. Cappon D, Jahanshahi M, Bisiacchi P. Value and Efficacy of Transcranial Direct Current Stimulation in the Cognitive Rehabilitation: A Critical Review Since 2000. Front Neurosci. 2016;10:157.
78. van der Kemp J, Dorresteijn M, Ten Brink AF, Nijboer TC, Visser-Meily JM. Pharmacological Treatment of Visuospatial Neglect: A Systematic Review. J Stroke Cerebrovasc Dis. 2017;26(4):686-700.
79. De Wit L, Ten Brink AF, Visser-Meily JM, Nijboer TC. Does prism adaptation affect visual search in spatial neglect patients: A systematic review. J Neuropsychol. 2016.

74
80. Ogourtsova T, Souza Silva W, Archambault PS, Lamontagne A. Virtual reality treatment and assessments for post-stroke unilateral spatial neglect: A systematic literature review. Neuropsychol Rehabil. 2017;27(3):409-54.
81. Fasotti L, van Kessel M. Novel insights in the rehabilitation of neglect. Front Hum Neurosci. 2013;7:780.
82. Kerkhoff G, Keller I, Ritter V, Marquardt C. Repetitive optokinetic stimulation induces lasting recovery from visual neglect. Restor Neurol Neurosci. 2006;24(4-6):357-69.
83. Barrett AM, Goedert KM, Basso JC. Prism adaptation for spatial neglect after stroke: translational practice gaps. Nat Rev Neurol. 2012;8(10):567-77.
84. Ishihara M, Revol P, Jacquin-Courtois S, Mayet R, Rode G, Boisson D, et al. Tonal cues modulate line bisection performance: preliminary evidence for a new rehabilitation prospect? Front Psychol. 2013;4:704.
85. Soto D, Funes MJ, Guzman-Garcia A, Warbrick T, Rotshtein P, Humphreys GW. Pleasant music overcomes the loss of awareness in patients with visual neglect. Proc Natl Acad Sci U S A. 2009;106(14):6011-6.
86. Rizzo AA, Buckwalter JG. Virtual reality and cognitive assessment and rehabilitation: the state of the art. Stud Health Technol Inform. 1997;44:123-45.
87. Riva G, Rizzo A, Alpini D, Attree EA, Barbieri E, Bertella L, et al. Virtual environments in the diagnosis, prevention, and intervention of age-related diseases: a review of VR scenarios proposed in the EC VETERAN Project. Cyberpsychology & behavior : the impact of the Internet, multimedia and virtual reality on behavior and society. 1999;2(6):577-91.
88. Rose FD, Attree EA, Johnson DA. Virtual reality: an assistive technology in neurological rehabilitation. Curr Opin Neurol. 1996;9(6):461-7.
89. Riva G, Castelnuovo G, Mantovani F. Transformation of flow in rehabilitation: the role of advanced communication technologies. Behav Res Methods. 2006;38(2):237-44.
90. Lohse KR, Hilderman CG, Cheung KL, Tatla S, Van der Loos HF. Virtual reality therapy for adults post-stroke: a systematic review and meta-analysis exploring virtual environments and commercial games in therapy. PLoS One. 2014;9(3):e93318.
91. Broeren J, Bjorkdahl A, Claesson L, Goude D, Lundgren-Nilsson A, Samuelsson H, et al. Virtual rehabilitation after stroke. Stud Health Technol Inform. 2008;136:77-82.
92. Broeren J, Rydmark M, Bjorkdahl A, Sunnerhagen KS. Assessment and training in a 3-dimensional virtual environment with haptics: a report on 5 cases of motor rehabilitation in the chronic stage after stroke. Neurorehabil Neural Repair. 2007;21(2):180-9.
93. Laver KE, George S, Thomas S, Deutsch JE, Crotty M. Virtual reality for stroke rehabilitation. The Cochrane database of systematic reviews. 2015;2:CD008349.
94. Tsirlin I, Dupierrix E, Chokron S, Coquillart S, Ohlmann T. Uses of virtual reality for diagnosis, rehabilitation and study of unilateral spatial neglect: review and analysis. Cyberpsychology & behavior : the impact of the

75
Internet, multimedia and virtual reality on behavior and society. 2009;12(2):175-81.
95. Pedroli E, Serino S, Cipresso P, Pallavicini F, Riva G. Assessment and rehabilitation of neglect using virtual reality: a systematic review. Front Behav Neurosci. 2015;9.
96. Peskine A, Rosso C, Box N, Galland A, Caron E, Rautureau G, et al. Virtual reality assessment for visuospatial neglect: importance of a dynamic task. J Neurol Neurosurg Psychiatry. 2011;82(12):1407-9.
97. Buxbaum LJ, Dawson AM, Linsley D. Reliability and validity of the Virtual Reality Lateralized Attention Test in assessing hemispatial neglect in right-hemisphere stroke. Neuropsychology. 2012;26(4):430-41.
98. Kim C, Kroger JK, Kim J. A functional dissociation of conflict processing within anterior cingulate cortex. Hum Brain Mapp. 2011;32(2):304-12.
99. Reinhart S, Schmidt L, Kuhn C, Rosenthal A, Schenk T, Keller I, et al. Limb activation ameliorates body-related deficits in spatial neglect. Front Hum Neurosci. 2012;6:188.
100. Grivaz P, Blanke O, Serino A. Common and distinct brain regions processing multisensory bodily signals for peripersonal space and body ownership. Neuroimage. 2017;147:602-18.
101. Folstein MF, Folstein SE, McHugh PR. "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189-98.
102. Sulter G, Steen C, De Keyser J. Use of the Barthel index and modified Rankin scale in acute stroke trials. Stroke. 1999;30(8):1538-41.
103. Fordell H, Bodin K, Bucht G, Malm J. A virtual reality test battery for assessment and screening of spatial neglect. Acta Neurol Scand. 2011;123(3):167-74.
104. Backman. Colosseum3d – authoring framework for virtual environments. EUROGRAPHICS Workshop IPT& EGVE Workshop. 2005;2005;1::225–6.
105. Ashburner J. A fast diffeomorphic image registration algorithm. Neuroimage. 2007;38(1):95-113.
106. Ovadia-Caro S, Villringer K, Fiebach J, Jungehulsing GJ, van der Meer E, Margulies DS, et al. Longitudinal effects of lesions on functional networks after stroke. J Cereb Blood Flow Metab. 2013;33(8):1279-85.
107. Geeraerts S, Lafosse C, Vandenbussche E, Verfaillie K. Asynchronous stimulus presentation in visual extinction: a psychophysical study. J Neuropsychol. 2010;4(Pt 2):167-79.
108. Vossel S, Eschenbeck P, Weiss PH, Weidner R, Saliger J, Karbe H, et al. Visual extinction in relation to visuospatial neglect after right-hemispheric stroke: quantitative assessment and statistical lesion-symptom mapping. J Neurol Neurosurg Psychiatry. 2011;82(8):862-8.
109. Brozzoli C, Dematte ML, Pavani F, Frassinetti F, Farne A. Neglect and extinction: within and between sensory modalities. Restor Neurol Neurosci. 2006;24(4-6):217-32.
110. Rorden C, Jelsone L, Simon-Dack S, Baylis LL, Baylis GC. Visual extinction: the effect of temporal and spatial bias. Neuropsychologia. 2009;47(2):321-9.

76
111. Umarova RM, Saur D, Kaller CP, Vry MS, Glauche V, Mader I, et al. Acute visual neglect and extinction: distinct functional state of the visuospatial attention system. Brain. 2011;134(Pt 11):3310-25.
112. al KGe. Continuing issues in the assessment of neglect. Neuropsychol Rehabil. 1995;5:239-58.
113. Bickerton WL, Samson D, Williamson J, Humphreys GW. Separating forms of neglect using the Apples Test: validation and functional prediction in chronic and acute stroke. Neuropsychology. 2011;25(5):567-80.
114. Luukkainen-Markkula R, Tarkka IM, Pitkanen K, Sivenius J, Hamalainen H. Comparison of the Behavioural Inattention Test and the Catherine Bergego Scale in assessment of hemispatial neglect. Neuropsychol Rehabil. 2011;21(1):103-16.
115. Pekna M, Pekny M, Nilsson M. Modulation of neural plasticity as a basis for stroke rehabilitation. Stroke. 2012;43(10):2819-28.
116. Kennett S, Eimer M, Spence C, Driver J. Tactile-visual links in exogenous spatial attention under different postures: convergent evidence from psychophysics and ERPs. J Cogn Neurosci. 2001;13(4):462-78.
117. Tinga AM, Visser-Meily JM, van der Smagt MJ, Van der Stigchel S, van Ee R, Nijboer TC. Multisensory Stimulation to Improve Low- and Higher-Level Sensory Deficits after Stroke: A Systematic Review. Neuropsychol Rev. 2016;26(1):73-91.
118. Katz N, Ring H, Naveh Y, Kizony R, Feintuch U, Weiss PL. Interactive virtual environment training for safe street crossing of right hemisphere stroke patients with unilateral spatial neglect. Disabil Rehabil. 2005;27(20):1235-43.
119. Kim YM, Chun MH, Yun GJ, Song YJ, Young HE. The effect of virtual reality training on unilateral spatial neglect in stroke patients. Annals of rehabilitation medicine. 2011;35(3):309-15.
120. van Kessel ME, van Nes IJ, Geurts AC, Brouwer WH, Fasotti L. Visuospatial asymmetry in dual-task performance after subacute stroke. J Neuropsychol. 2013;7(1):72-90.
121. Mizuno K, Kato K, Tsuji T, Shindo K, Kobayashi Y, Liu M. Spatial and temporal dynamics of visual search tasks distinguish subtypes of unilateral spatial neglect: Comparison of two cases with viewer-centered and stimulus-centered neglect. Neuropsychol Rehabil. 2016;26(4):610-34.
122. Chen P, Goedert KM, Shah P, Foundas AL, Barrett AM. Integrity of medial temporal structures may predict better improvement of spatial neglect with prism adaptation treatment. Brain imaging and behavior. 2014;8(3):346-58.
123. Gossmann A, Kastrup A, Kerkhoff G, Lopez-Herrero C, Hildebrandt H. Prism adaptation improves ego-centered but not allocentric neglect in early rehabilitation patients. Neurorehabil Neural Repair. 2013;27(6):534-41.
124. Duncan J, Owen AM. Common regions of the human frontal lobe recruited by diverse cognitive demands. Trends Neurosci. 2000;23(10):475-83.

77
125. Mansouri FA, Tanaka K, Buckley MJ. Conflict-induced behavioural adjustment: a clue to the executive functions of the prefrontal cortex. Nat Rev Neurosci. 2009;10(2):141-52.
126. Knudsen EI. Fundamental components of attention. Annu Rev Neurosci. 2007;30:57-78.
127. Miller EK, Cohen JD. An integrative theory of prefrontal cortex function. Annu Rev Neurosci. 2001;24:167-202.
128. Turkeltaub PE, Messing S, Norise C, Hamilton RH. Are networks for residual language function and recovery consistent across aphasic patients? Neurology. 2011;76(20):1726-34.