Virology Laboratory Managementof Patients · THE VIROLOGY LABORATORY AND DIAGNOSIS OF CNS DISEASE...
14
CLINICAL MICROBIOLOGY REVIEWS, Jan. 1989, p. 1-14 Vol. 2, No. 1 0893-8512/89/010001-14$02.00/0 Copyright © 1989, American Society for Microbiology Role of the Virology Laboratory in Diagnosis and Management of Patients with Central Nervous System Disease TASNEE CHONMAITREE,l2* CONSTANCE D. BALDWIN,' AND HELEN L. LUCIA'2 Departments of Pediatrics' and Pathology,2 University of Texas Medical Branch at Galveston, Galveston, Texas 77550 INTRODUCTION ......................................................................1 CNS DISEASES CAUSED BY VIRUSES .....................................................................2 Enteroviruses ......................................................................2 Normal host ......................................................................2 Compromised host ......................................................................3 Togaviruses, Bunyaviruses, and Reoviruses ...................................................................... 4 Herpesviruses ......................................................................4 HSV .................................................................... 4 VzV .................................................................... 4 EBV .................................................................... 4 CMV ......................................................................4 Mumps, Measles, and Rubella ......................................................................5 Lymphocytic Choriomeningitis Virus ......................................................................5 Rabies ..................................................................... 5 HIV ......................................................................5 DIAGNOSTIC METHODS FOR ENTEROVIRUSES ......................................................................5 Rapid Diagnosis ......................................................................5 Isolation of Virus ......................................................................6 Specimen collection and transport ......................................................................6 Cell culture ......................................................................6 Animal inoculation ......................................................................7 Identification of isolates ......................................................................7 Serology ......................................................................7 DIAGNOSTIC METHODS FOR NONENTEROVIRUSES ................................................................7 Togaviruses, Bunyaviruses, and Reoviruses ...................................................................... 7 Herpesviruses ......................................................................8 Mumps, Measles, and Rubella .......................................................................8 Lymphocytic Choriomeningitis Virus .......................................................................8 Rabies ...................................................................... 8 HIV .......................................................................8 MANAGEMENT OF PATIENTS WITH CNS VIRAL INFECTION ...................................................9 Aseptic Meningitis .......................................................................9 Meningoencephalitis .......................................................................9 Enteroviral Meningoencephalitis Associated with Agammaglobulinemia ............................................9 INFLUENCE OF THE VIROLOGY LABORATORY ON PATIENT MANAGEMENT ..........................9 CONCLUSION ...................................................................... 10 ACKNOWLEDGMENTS ...................................................................... 11 LITERATURE CITED ...................................................................... 11 INTRODUCTION Before antiviral therapy became available, viral diagnosis was used clinically primarily to identify a community out- break of viral disease and to provide prognostic information to the patient. The delayed reports of viral culture results dictated that diagnostic information was generally not avail- able until the patient's illness was over. Because demand for the technology was limited, diagnostic virology facilities were, until recently, available only in reference laboratories and some university hospitals. In a survey published 12 years ago, only 60% of 115 U.S. medical centers reported on-site viral diagnosis (60). Physicians avoided using these laboratories because results were delayed and often not * Corresponding author. useful for patient care, costs were high, and collection and transport of specimens were difficult. Physicians were more likely to use a viral laboratory if it was located within their institution. The discovery of many types of antiviral therapy has mandated the establishment of more accessible facilities for viral diagnosis and development of more rapid diagnostic techniques. At present, increasing numbers of diagnostic facilities are becoming available at university medical cen- ters, Veterans Administration hospitals, and even some community hospitals (81, 98, 110, 128). In addition, some central laboratories have reached out to offer viral diagnostic facilities to the surrounding community (124, 128). These laboratories vary in size and emphasis on diagnostic meth- ods. The laboratory can now operate on a modest scale, be tailored to the needs of the patients it serves, and provide 1 on February 29, 2020 by guest http://cmr.asm.org/ Downloaded from
Transcript of Virology Laboratory Managementof Patients · THE VIROLOGY LABORATORY AND DIAGNOSIS OF CNS DISEASE...

CLINICAL MICROBIOLOGY REVIEWS, Jan. 1989, p. 1-14 Vol. 2, No. 10893-8512/89/010001-14$02.00/0Copyright © 1989, American Society for Microbiology
Role of the Virology Laboratory in Diagnosis and Management ofPatients with Central Nervous System Disease
TASNEE CHONMAITREE,l2* CONSTANCE D. BALDWIN,' AND HELEN L. LUCIA'2Departments of Pediatrics' and Pathology,2 University of Texas Medical Branch at Galveston, Galveston, Texas 77550
INTRODUCTION......................................................................1CNS DISEASES CAUSED BY VIRUSES .....................................................................2
Enteroviruses ......................................................................2Normal host......................................................................2Compromised host......................................................................3
Togaviruses, Bunyaviruses, and Reoviruses ...................................................................... 4Herpesviruses......................................................................4HSV .................................................................... 4VzV.................................................................... 4EBV .................................................................... 4CMV......................................................................4
Mumps, Measles, and Rubella ......................................................................5Lymphocytic Choriomeningitis Virus......................................................................5Rabies ..................................................................... 5HIV ......................................................................5
DIAGNOSTIC METHODS FOR ENTEROVIRUSES ......................................................................5Rapid Diagnosis......................................................................5Isolation of Virus ......................................................................6
Specimen collection and transport......................................................................6Cell culture......................................................................6Animal inoculation ......................................................................7Identification of isolates ......................................................................7
Serology......................................................................7DIAGNOSTIC METHODS FOR NONENTEROVIRUSES ................................................................7
Togaviruses, Bunyaviruses, and Reoviruses ...................................................................... 7Herpesviruses......................................................................8Mumps, Measles, and Rubella .......................................................................8Lymphocytic Choriomeningitis Virus.......................................................................8Rabies ...................................................................... 8HIV .......................................................................8
MANAGEMENT OF PATIENTS WITH CNS VIRAL INFECTION ...................................................9Aseptic Meningitis.......................................................................9Meningoencephalitis.......................................................................9Enteroviral Meningoencephalitis Associated with Agammaglobulinemia ............................................9
INFLUENCE OF THE VIROLOGY LABORATORY ON PATIENT MANAGEMENT ..........................9CONCLUSION ...................................................................... 10ACKNOWLEDGMENTS ...................................................................... 11LITERATURE CITED ...................................................................... 11
INTRODUCTION
Before antiviral therapy became available, viral diagnosiswas used clinically primarily to identify a community out-break of viral disease and to provide prognostic informationto the patient. The delayed reports of viral culture resultsdictated that diagnostic information was generally not avail-able until the patient's illness was over. Because demand forthe technology was limited, diagnostic virology facilitieswere, until recently, available only in reference laboratoriesand some university hospitals. In a survey published 12years ago, only 60% of 115 U.S. medical centers reportedon-site viral diagnosis (60). Physicians avoided using theselaboratories because results were delayed and often not
* Corresponding author.
useful for patient care, costs were high, and collection andtransport of specimens were difficult. Physicians were morelikely to use a viral laboratory if it was located within theirinstitution.The discovery of many types of antiviral therapy has
mandated the establishment of more accessible facilities forviral diagnosis and development of more rapid diagnostictechniques. At present, increasing numbers of diagnosticfacilities are becoming available at university medical cen-ters, Veterans Administration hospitals, and even somecommunity hospitals (81, 98, 110, 128). In addition, somecentral laboratories have reached out to offer viral diagnosticfacilities to the surrounding community (124, 128). Theselaboratories vary in size and emphasis on diagnostic meth-ods. The laboratory can now operate on a modest scale, betailored to the needs of the patients it serves, and provide
1
on February 29, 2020 by guest
http://cmr.asm
.org/D
ownloaded from

2 CHONMAITREE ET AL.
TABLE 1. Recognized human enterovirus serotypes
Virus Types
Polioviruses .................... 1-3Group A coxsackieviruses'.................... 1-24Group B coxsackieviruses .................... 1-6Echoviruses".................... 1-34Enteroviruses'.................... 68-72
Type 23 is the same as echovirus 9.Type 10 is reclassified as a reovirus: type 28 is a rhinovirus.EnteroviruLs type 72 is hepatitis A virus.
important information for patient management (81, 94, 157).This article reviews acute central nervous system (CNS)diseases caused by viruses and the usefulness of the virologylaboratory in diagnosis and management of patients withthese diseases. The more common enteroviral diseases areemphasized.
CNS DISEASES CAUSED BY VIRUSES
Viral infections of the CNS have two major clinicalpresentations: aseptic meningitis, which is by far the mostfrequent, and viral meningoencephalitis. The enterovirusescause most acute viral infections of the CNS (35 to 83%).with mumps a distant second (1 to 40%), worldwide (9, 20,42, 44, 116, 146). Herpesviruses, togaviruses. bunyaviruses.lymphocytic choriomeningitis virus, and measles and rubellaviruses can also cause CNS disease. More recently. the roleof human immunodeficiency virus (HIV) in the etiology ofCNS disease has been recognized (48).
Enteroviruses
Enteroviruses constitute a genus of the Picornaviridaefamily which currently includes 69 serotypes made up of
polioviruses, coxsackieviruses, echoviruses, and enterovi-rus types 68 to 72 (Table 1). This review will exclude fromthe discussion of enteroviral diseases poliomyelitis and otherdiseases caused by the three types of polioviruses.
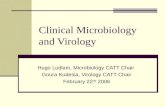
Enteroviruses have a worldwide distribution, with in-creased prevalence in temperate climates during the warmmonths of the year (54, 102. 103. 115). A recent survey fromthe Centers for Disease Control showed that the temporalpattern of isolation of nonpolio enteroviruses differs amongregions of the United States. However, a mean of 84% and arange of 65 to 93%c of virus isolations in a region were madebetween July and January (143). Figure 1 shows the seasonalprevalence of enteroviruses isolated in the Clinical VirologyLaboratory of The University of Texas Medical Branch(UTMB) in Galveston, Tex., from 1983 to 1987. Althoughoutbreaks of disease associated with a single serotype ofenteroviruses are often reported (12. 29, 72, 144), the farmore common pattern is endemic infection caused by sev-eral enterovirus types (28, 107. 157). The predominant typesmay vary yearly and may vary by locality even within thesame year.Normal host. Enteroviral diseases in normal hosts are
most often seen in young infants and children (54). Entero-viruses are mainly spread by the fecal-oral route. Theincubation period ranges from 1 day to 3 weeks but isgenerally 3 to 5 days. CNS disease is a common manifesta-tion of infections caused by a variety of nonpolio enterovi-ruses, with aseptic meningitis being the most common. Lesscommon diseases include encephalitis, paralysis, Guillain-Barre syndrome, cerebellar ataxia, and peripheral neuritis(10, 26, 29, 41-43. 54. 69, 133). CNS disease sometimesoccurs as a part of disseminated enteroviral infection, withviremia and involvement of heart, liver, kidneys, adrenalglands, and the blood coagulation system (14, 26, 56, 71, 75,77).
150
140-
130-
120U) 110-4)Co 100o 90
%I- 80
70-4) 6
M~~~~~~Mnh
E 50-
Z 40
30-
20-
10
Jan. Feb. Mar. Apr. May June July Aug. Sept. Oct. Nov. Dec.
MonthsFIG. 1. Seasonal prevalence of enteroviruses as represented by number of enteroviruses (including polioviruses) isolated by month from
clinical specimens submitted to the Clinical Virology Laboratory. UTMB. 1983 to 1987. In two separate outbreaks in 1984. echoviruses 9
(April to July) and 11 (September to December) predominated.
CLIN. MICROBIOL. REV.
on February 29, 2020 by guest
http://cmr.asm
.org/D
ownloaded from

THE VIROLOGY LABORATORY AND DIAGNOSIS OF CNS DISEASE
TABLE 2. Age distribution of 103 children with enteroviralmeningitis diagnosed at UTMB, 1983 to 1987"
Age group No. of Cumulative %cases
<1mo 20 191-3 mo 31 504 mo-1 yr 20 692-5 yr 18 86>6 yr 14 100
" All had an enterovirus in the CSF. Data were collected by Cheryl Banks.
Approximately 3,200 to 12,700 cases of aseptic meningitiswere reported annually to the Centers for Disease Controlbetween 1973 and 1983 (24), but its actual incidence isprobably severalfold higher. Enteroviruses account for themajority of the identified agents causing aseptic meningitis,and yearly peak occurrences of the disease closely coincidewith periods of most frequent enterovirus isolation (20, 24).Enteroviral aseptic meningitis caused by numerous types ofcoxsackieviruses, echoviruses, and enterovirus 71 (26, 29)occurs in both epidemics and isolated cases. In general,enteroviral meningitis is more common in young patients,especially those under 1 year of age. Age ranges of 103children with enteroviral meningitis diagnosed at UTMBfrom 1983 to 1987 are shown in Table 2.
Clinical signs and symptoms of enteroviral CNS disease inyoung children are mostly nonspecific and mimic those ofbacterial sepsis or meningitis or both. Onset of illness can beabrupt or gradual. Fever is the most common presentingsymptom, followed by irritability, lethargy, anorexia, gas-trointestinal or respiratory symptoms or both, otitis media,and rash (15, 36, 137, 157, 160). In one study, apnea occurredin 9% of children with enteroviral meningitis (157). Specificsigns and symptoms of CNS disease, such as nuchal rigidityand bulging fontanelle, may or may not be present. Seizuresoccur in <10% of patients (137, 157). Focal neurologicalabnormalities are rare, but transient ataxia or paralysisoccasionally occurs (29, 88, 137). In older children, head-ache is common and CNS signs and symptoms are moreprominent.
Laboratory findings vary widely. Initial peripheral bloodand cerebrospinal fluid (CSF) results from 103 children withenteroviral meningitis diagnosed at UTMB are reported inTable 3. Peripheral total and differential leukocyte countsusually cannot be clearly distinguished from those seen inpatients with bacterial sepsis or meningitis. The CSF leu-kocyte count varies from none to several thousand cells permm3, but most often is <1,000. Although monocytes-mac-rophages are generally the most numerous cells in CSF, the
predominance of premature or segmented neutrophils iscommon, especially early in the disease. Performance of asecond lumbar puncture 5 to 8 h after the first is generally nothelpful in demonstrating a shift of CSF leukocyte composi-tion from a neutrophil to a monocyte predominance (57).
In most patients with enteroviral meningitis, CSF totalprotein content is within normal limits, but in a smallpercentage it may be slightly or even markedly elevated.CSF glucose content is usually normal but can be diminishedin up to 18% of cases (137, 157). The measurement of CSFconcentrations of C-reactive protein, lactic acid dehydroge-nase, and alpha interferon to differentiate between bacterialand viral meningitis is not generally feasible, although somestudies suggest that these tests may be helpful (1, 2, 34, 50,62, 111).
Diagnosis of enteroviral meningitis is especially difficultwhen CSF pleocytosis is absent, a phenomenon which hasbeen variably reported to occur in 3 to 40% of patients (28,58, 74, 79, 157, 159). In these cases, viral culture of the CSFis the only reliable method currently available to diagnosemeningitis. Therefore, it should be kept in mind that, whenclinical signs and symptoms suggest the diagnosis of entero-viral meningitis, even if the CSF contains no leukocytes, an
enterovirus may still be present.Accurate diagnosis of enteroviral meningitis is important,
given the potential of the disease to lead to neurologicalsequelae. Although data on these outcomes are conflicting(11, 46, 122, 134, 161), some evidence suggests that childrenwith enteroviral meningitis, especially at young ages, mayhave long-term neurological abnormalities, including smallerhead size, deficits in speech and language development, andlower intelligence. Because most of the studies involved asmall number of patients and used different research meth-odologies, these data are not yet conclusive. These studiessuggest, however, that enteroviral meningitis, especially inyoung infants, is not a benign disease, and accurate diagno-sis may allow predictable prognosis and follow-up strategies.Compromised host. Enteroviral infections in patients with
antibody deficiencies, especially X-linked agammaglobuline-mia, can be severe. Two clinical syndromes of enteroviralinfection in these patients include vaccine-associated para-lytic poliomyelitis (162, 163) and the more commonly re-ported chronic enteroviral meningoencephalitis (5, 32, 45,51, 86, 91, 92, 149, 152, 158). Enteroviral meningoencepha-litis associated with agammaglobulinemia is most frequentlycaused by echoviruses, although group A and B coxsackie-viruses have also been implicated (32, 91). Neurologic pre-sentations may resemble those of acute onset meningoen-cephalitis or aseptic meningitis, with fever, headache,altered mental status, and seizures. Approximately 30% of
TABLE 3. Initial peripheral blood and CSF findings for 103 patients with enteroviral meningitis diagnosed at UTMB, 1983 to 1987a
Source Leukocytes/mm3 % Neutrophils % % Protein GlucoseSegmented Premature Lymphocytes Monocytes (mg/dl) (mg/dl)
Peripheral bloodMedian 11,700 46 8 31 6Range 4,800-29,800 4-90 0-41 5-76 0-18
CSFbMedian 100 38 0 15 26 40 57Range 0-3,100 0-90 0-10 0-100 0-90 5-472 28-100
a CSF culture was positive for an enterovirus in all cases.b CSF data came from 83 atraumatic taps, with <100 erythrocytes per mm3. Data were collected by Cheryl Banks.
VOL. 2, 1989 3
on February 29, 2020 by guest
http://cmr.asm
.org/D
ownloaded from

4 CHONMAITREE ET AL.
patients present with edema or dermatomyositislike syn-drome, which is marked by peripheral edema, erythematousrashes, and evidence of inflammation in skin and musclebiopsy specimens (91). Regardless of the clinical manifesta-tions at the time of onset, over the prolonged course of thedisease, nearly all reported patients eventually develop someovert neurological symptoms, including headache, seizures,hearing loss, lethargy or coma, weakness, ataxia, paresthe-sias, diminished intellectual acuity, developmental delay,hemiparesis, cranial nerve palsies, episodic confusionalstates, and symptoms consistent with transient ischemicepisodes (91). Other reported manifestations of this syn-drome include personality changes, dysarthria, aphasia,hepatitis, and arthritis (89, 91).The diagnosis of enteroviral meningoencephalitis in these
patients requires the isolation of enterovirus from the CSF.Virus may not be detected in the CSF until after the onset ofsymptoms and CSF abnormalities; even after detection ofthe virus in the CSF, negative results of viral cultures can beobtained sporadically without a change in therapy (91, 158).
Togaviruses, Bunyaviruses, and Reoviruses
Viral encephalitis due to togavirus, bunyavirus, and reo-virus infection occurs sporadically. These viruses are trans-mitted by the bites of mosquitoes or ticks. The Togaviridaefamily contains eastern equine encephalitis, western equineencephalitis, Venezuelan equine encephalitis, and St. Louisencephalitis viruses, all of which are found in the UnitedStates (35). The group also includes Murray Valley fever(Australia), Japanese encephalitis (Japan), and several tick-borne varieties of encephalitis (in Europe, especially theSoviet Union). The Bunyaviridae family contains the Cali-fornia group viruses, notably La Crosse virus, which is seenin the United States (113).A period of viremia precedes the onset of clinical neuro-
logic disease. Incubation periods range from 2 to 14 days.Viral infection of brain tissue results in fever, headache,coma, and paralysis. Eastern equine encephalitis is mostsevere, with fatality rates of 50 to 75%; 30% or more of thesurvivors have neurologic sequelae severe enough to requireinstitutionalization. Of symptomatic cases, the fatality rateof Western equine encephalitis is 10%, that of Venezuelanequine encephalitis is <1%, and that of St. Louis encepha-litis is 10 to 20%. La Crosse virus infection is also mild; mostmanifestations are nonspecific viral syndromes rather thanencephalitis, and mortality and residual morbidity occur infewer than 2% of the patients with clinical encephalitis (35,113).Colorado tick fever, caused by a reovirus, is endemic in
the Rocky Mountain region of the United States and Canada.It is a zoonosis of rodents and is transmitted by ticks. Thevirus enters erythroid precursors and circulates inside ma-ture erythrocytes, where it is protected from antibodies.Thus, the disease results in prolonged viremia. The diseaseis denguelike in presentation; occasionally, children willdevelop aseptic meningitis. The disease is self-limiting andseldom results in death (90).
Herpesviruses
HSV. Herpes simplex virus (HSV) is responsible forneonatal and adult encephalitis and viral meningitis. Neona-tal HSV infection is acquired by passage of infants throughthe birth canal of infected mothers, especially those withprimary infection. The frequency of occurrence is 26 of
100,000 deliveries. Infection may be limited to the skin, butmore often is disseminated, with liver, lung, or CNS involve-ment. The CNS disease with or without dissemination isdevastating. Without treatment, mortality is 50 to 85% andmorbidity is 100% (6). With modern antiviral therapy usingacyclovir or vidarabine, mortality has been reduced to 10 to57%, but up to 86% of the survivors still suffer neurologicsequelae (6).HSV encephalitis in adults is usually an isolated CNS
infection, localized to the temporal lobes of the brain. Thisviral disease is the most common fatal viral encephalitis; itoccurs in 1 of 500,000 of the population. When it is leftuntreated, mortality is 70%, with sequelae in the majority ofsurvivors. With acyclovir treatment, mortality is now 13 to19% and morbidity is 44 to 62% (6). Aseptic meningitiswithout encephalitis also occurs, typically during primarygenital infection with HSV type 2. Occasionally the patientwill not have cutaneous or mucosal lesions (123, 142).VZV. Neurologic involvement is unusual during primary
varicella infection (chicken pox). Isolated cerebellar ataxia isthe most common CNS abnormality (50%), with nausea,vomiting, headache, and ataxia occurring 5 to 13 days afterthe onset of the rash and lasting from 2 to 4 weeks. Thefrequency has been reported to be 0.1 to 0.75% in cases ofchicken pox. The mortality is low (0.5%), and the majority ofchildren recover completely (6). A less frequent, but moresevere complication is postinfectious meningoencephalitis orcerebritis, which is attributable to host response reactions.Patients present with headache, fever, and vomiting, withalerted sensorium. Seizures occur in up to 50% of thepatients. The mortality is low (about 5%), and 80% ofsurvivors have no sequelae (6, 141).A number of neurological syndromes have been noted
during recurrent varicella-zoster virus (VZV) infection(zoster or shingles). Cranial and peripheral nerve palsies inthe infected dermatome are seen in 1 to 6% of cases.Encephalitis, the most common CNS abnormality, occursprimarily in immunocompromised patients and is attribut-able to systemic dissemination of the virus from cutaneouslesions. Mortality is high (30 to 50%), but many deaths aredue to concurrent VZV pneumonia, not the CNS disease.Neurological sequelae are present in as many as 30% ofsurvivors (6). In one study, myelitis occurred as an unusualcomplication of VZV infection (1 of 1,210 cases) (147), asdoes herpes ophthalmicus with contralateral hemiplegia.Even in uncomplicated VZV infection, the CSF may showpleocytosis and increased protein concentration (112).EBV. Epstein-Barr virus (EBV) infection can present with
neurologic syndromes. Serious nervous system disordershave been estimated to affect approximately 1 to 5% ofhospitalized patients with infectious mononucleosis. Al-though neurologic symptoms may be the sole manifestationof an EBV syndrome, most appear during the course of thisdisease. The CNS infection may be encephalitis, asepticmeningitis, Guillain-Barre syndrome, neuritis, or subacutesclerosing panencephalitis. The encephalitis is usually mildand transient, but rarely can be fatal. Complete recovery ofneurologic function occurs in almost all survivors (13, 55,136).CMV. Although it is a common cause of neurological
damage during congenital infection, cytomegalovirus (CMV)encephalitis is vanishingly rare as a complication of CMVinfection acquired postnatally by hosts with normal immunefunction. However, this infection has become extremelycommon in immunocompromised patients with acquired
CLIN. MICROBIOL. REV.
on February 29, 2020 by guest
http://cmr.asm
.org/D
ownloaded from

THE VIROLOGY LABORATORY AND DIAGNOSIS OF CNS DISEASE
immunodeficiency syndrome (AIDS). It is characterized byrelentless progression of dementia and eventual death (105).
Mumps, Measles, and Rubella
Clinically apparent CNS involvement occurs in about 15%ofmumps cases, although CSF abnormalities are much morecommon (19, 21). Although on a worldwide basis mumpsremains the second leading cause of aseptic meningitis andencephalomyelitis (20, 42, 44, 116, 146), the incidence hasdecreased dramatically in the United States with the intro-duction of large-scale immunization. Mumps has decreased98% in incidence, and in 1983, the last year for which theCenters for Disease Control collected statistics on mumpsencephalomyelitis, seven cases were reported in the UnitedStates (23). The symptoms range from headache and list-lessness to seizures with altered states of consciousness.Complications include meningitis, encephalitis, and menin-goencephalitis. In the absence of parotitis, the meningoen-cephalitis is clinically indistinguishable from enteroviral in-fection (70).
Measles encephalitis complicates approximately 1 per1,000 cases of measles (22, 65, 78). Since the introduction ofmeasles vaccine, the incidence has declined in parallel to thedecline of measles. The risk of encephalitis rises with the ageof the patient. CNS symptoms usually appear after theeruption of the rash, with abrupt recurrence of fever, head-ache, lethargy, irritability, and confusion. The majority ofpatients improve and return to normal after 2 to 3 days, butapproximately 30% progress to coma, which may persist fordays or weeks. Attempts to recover infectious measles virusfrom the CSF are seldom successful; this syndrome isprobably caused by a host response reaction. Some 10 to15% of the cases are fatal, and 25% have severe permanentCNS sequelae. Rubella can also cause postinfectious en-cephalitis (1 of 6,000 cases). The symptoms are similar to butmilder than those seen with measles, and persisting morbid-ity occurs in <10% of cases; mortality is very low (141, 151).
Lymphocytic Choriomeningitis Virus
Lymphocytic choriomeningitis virus is an arenaviruswhich is endemic in mice and can be transmitted to humans.Infections with lymphocytic choriomeningitis virus have aninfluenzalike prodromal illness, with arthralgias, anorexia,nausea, light-headedness, and pneumonitis. CNS symptomsinclude headache, nuchal rigidity, and, rarely, coma anddeath (2 of 79 cases) (3, 4, 97).
Rabies
Rabies infection of the CNS is an encephalitis. The virus isa zoonosis; humans usually acquire the infection from thebite of infected animals, although infection through therespiratory route may also occur. This infection is extremelyrare in the United States, where most disease is associatedwith wild-animal infection. However, in many parts of theworld where domestic dogs are not vaccinated routinely,rabies remains a feared disease (151). Mortality is 100%.
HIV
HIV has recently been recognized as a significant CNSviral pathogen. The disease can present as a transient asepticmeningitis early in infection. An insidious progressive en-cephalitis ultimately resulting in dementia and death can also
occur. As we begin to control the secondary infections ofpatients with AIDS, this chronic encephalitis is assuminggreater clinical significance. Clinical evidence of this diseasehas been reported in 65% of patients with AIDS. Postmor-tem studies suggest that CNS infection is always present,even when it is not clinically apparent (48).
DIAGNOSTIC METHODS FOR ENTEROVIRUSES
Rapid Diagnosis
Methodologies for rapid diagnosis of enteroviral meningi-tis and encephalitis by means other than cell culture are stillunder development. Detection of CNS enteroviral infectionis technically difficult for two reasons. Enteroviruses arefrequently present in body fluids in low concentrations; CSFmay contain only 10 to 103 50% tissue culture infective dosesper ml during infection (160). In addition, different enterovi-ruses express relatively few common antigenic determinants(R. H. Yolken and J. F. Modlin, Pan Am. Gr. Rapid ViralDiagn. Newsl. 12:1-2, 1986), so any detection method whichdepends on recognizing viral antigen must include a largenumber of reagents and multiple tests. Despite these diffi-culties, development of rapid diagnostic methods for thesepathogens has made significant recent progress.Immunofluorescent (IF) staining of CSF leukocytes during
enteroviral meningitis has been demonstrated (145), withdetection and identification of the infecting enterovirus in 36of 40 specimens within 2 h. By this method, the virus can beidentified on days 6 through 10 of infection, when growth incell culture is no longer possible. The disadvantages of themethod are the need for maintaining a large number ofantisera, the low sensitivity of the reagents under the re-quired dilutions, and, in some samples, the lack of a suffi-cient number of leukocytes in the CSF for measurement(145). In addition, frequent nonspecific fluorescence of CSFlymphocytes has been reported by subsequent workers (52).Counterimmunoelectrophoresis has been used to detect
bacterial antigens in CSF. However, attempts to detectenteroviral antigen by this method were unsuccessful, prob-ably because of the small quantity of antigen present (17).Complementary deoxyribonucleic acid probes have been
used in more recent attempts to detect enterovirus (67, 68,125, 126, 148). These probes have identified enteroviruses,which were artificially added to CSF, and subgenomicprobes detected a number of different serotypes of entero-viruses, suggesting that a small number of probes, perhapsas few as two, might be able to detect the wide range ofenterovirus serotypes (126). However, the limit of sensitivityof the probes was 106-24 50% tissue culture infective dosesper ml, which is not enough to be clinically useful. It hasbeen suggested that nucleic acid hybridization methodscould be used after concentration of the virus by immuno-precipitation, but the large number of antisera needed wouldlimit the practicality of this procedure (148).Another possible approach would be to search for entero-
viruses in specimens other than those from the CNS. Therehave been reports of rapid detection of enteroviruses inserum, using monoclonal antibodies against epitopes of VPIpeptide which are shared by all enteroviruses except hepa-titis A (166, 167). Although the test is highly sensitive, themonoclonal antibody is not widely available. Since themajority of children with enteroviral meningitis have cultur-able virus in their stool, probably at a higher titer than inCSF, searching for enteroviruses in stool may provide someclue to the diagnosis. By using an enzyme-linked immuno-
5VOL. 2, 1989
on February 29, 2020 by guest
http://cmr.asm
.org/D
ownloaded from

6 CHONMAITREE ET AL.
sorbent assay (ELISA), virus was detected in 8 of 11 stoolsfrom which coxsackievirus was grown (165). The largenumber of serotypes makes this method cumbersome, with24 microdilution tray wells required for each specimen, but itis especially useful for detecting group A coxsackieviruses,which grow poorly in culture (164). With a complementarydeoxyribonucleic acid probe, an enterovirus was detected inseven of eight culture-positive stools (67). The single probe,which copied about two-thirds of the coxsackievirus B3genome, was able to detect a number of different enterovi-ruses, suggesting the possibility that relatively few reagents
would be required to detect this group. An additional methodfor detection of enteroviruses uses protein A-gold immuno-electron microscopy. This method is reported to be 200- to
1,000-fold more sensitive than direct electron microscopy
and 2- to 40-fold more sensitive than immunoelectron mi-croscopy. However, it requires specific antisera, whichlimits the practical utility of the method (63). Unfortunately,all techniques which detect enteroviruses in stool havelimited value because asymptomatic children commonlyshed enteroviruses, including vaccine polioviruses, in stool.CNS infection would, therefore, have to be confirmed bysome other means.
Isolation of Virus
Isolation in cell culture is currently the most sensitive andreliable method for detecting enteroviruses in clinical spec-
imens, except for most serotypes of group A coxsackievi-ruses. These viruses do not grow in cell culture and must beinoculated into newborn mice or guinea pig embryos (61, 93,94). In general, the cytopathic effect (CPE) produced byenteroviruses in standard cell culture is quite distinctive andcan be recognized fairly early and with accuracy by experi-enced technicians (59, 61, 94). A rapid report of a presump-
tive diagnosis of enterovirus infection based on CPE in cellculture, without waiting for the specific typing of the isolate,can have an impact on patient management (28, 157). If thelaboratory aims to provide such rapid reporting, the cellculture should be observed for enterovirus CPE daily and atleast once during the weekend for the first 4 to 5 days of theculture and then less frequently for 10 to 14 days thereafter.Use of a multiple cell culture system to grow enterovirusescan also increase the sensitivity as well as the speed ofenterovirus isolation (38; T. Chonmaitree, C. Ford, C.Sanders, and H. Lucia, Abstr. Annu. Meet. Am. Soc.Microbiol. 1988, C84, p. 346). This technique is discussedbelow.Specimen collection and transport. Clinical specimens
should be collected as soon after the onset of clinicalsymptoms as possible. For enteroviral CNS infection, CSFis the most specific specimen used, although some types ofenteroviruses such as enterovirus 71 are infrequently iso-lated from CSF (29, 131). The isolation rate of enterovirusesfrom CSF of patients with presumptive enteroviral meningi-tis varies from 43 to 77% in different geographic areas andwith different predominant enterovirus serotypes (28, 100,157). CSFs containing a few or no cells have also beenreported to yield enteroviruses in a significant number ofcases (28, 74, 79, 157, 159); therefore, these CSFs shouldalso be cultured for the viruses when clinical signs andsymptoms of the patient suggest the diagnosis of enteroviralCNS disease, especially during an epidemic period. Throatswab and rectal swab or stool specimens, although not fromCNS-specific sites, can give an early (28, 157) and sometimesthe only clue to diagnosis. Because infants and children with
enteroviral meningitis may also have viremia (37), bloodculture for detection of virus in mononuclear leukocytes orserum or both (117) from a febrile child may also be useful inmaking a definitive diagnosis.
Enteroviruses are relatively stable and survive well attemperatures of 4 to -70'C, but measurable loss of activityoccurs when the specimens are kept at room temperature formany hours or allowed to dry (93, 95). Throat and rectalswab specimens should be placed in viral transport medium,which is provided by most virology laboratories, and storedrefrigerated or frozen if necessary. Fresh stool specimenscan be transported in conventional containers.
Cell culture. The cell types used most widely to growenteroviruses include primary monkey (rhesus, cynomolgus,or African green) kidney cells (PMK) and human diploidfibroblast cells such as WI-38 or MRC-5 (66, 93, 95). Othercell types include continuous human heteroploid cells (HeLaand HEp-2), primary or diploid human embryonic kidney,human fetal kidney, human amnion, human rhabdomyosar-coma (RD), chicken embryo, and the BGM line of Africangreen monkey cells (66, 93, 95).The growth requirements of different groups of enterovi-
ruses vary considerably. All three types of polioviruses growwell in PMK, human embryonic kidney, human diploidfibroblast, HeLa, BGM, and RD cells (66, 93, 95). The CPEdevelops quickly and often destroys the monolayer within 3days. While many serotypes of group A coxsackievirusesrequire animal inoculation, some serotypes (A7 and A9)grow readily in PMK cells. Coxsackievirus A21 grows bestin HeLa and HEp-2 cells. Other group A coxsackieviruses,including A2, A4, All, A13, A15, A16, A18, A20, and A24,can also be isolated in human amnion, chicken embryo, orhamster kidney cells (84, 93, 135, 153). Group B coxsackie-viruses do not replicate well in human diploid fibroblasts andRD cells but grow well in PMK and BGM cells (95).No single cell culture system is suitable for recovery of all
common human enteroviruses. The more cell types used, themore serotypes of enteroviruses will be detected. For prac-tical purposes, however, three or four cell types are proba-bly the maximum that most clinical laboratories can handle.Combined use of three or four cell types can significantlyincrease yield and speed of virus recovery from clinicalspecimens (38, 61, 79, 137) compared with use of onlystandard culture. Use of BGM, a continuous African greenmonkey kidney cell line, increases speed and efficiency ofrecovery for group B coxsackieviruses (39, 96, 130). RDcells are particularly useful for echoviruses and some se-rotypes of group A coxsackieviruses (7, 38, 130, 150). Use ofsubpassages of primary human embryonic kidney cells in-creases the isolation rate of both echoviruses and group Bcoxsackieviruses (Chonmaitree et al., Abstr. Annu. Meet.Am. Soc. Microbiol. 1988). In a study during two consecu-tive enterovirus seasons (38), use of BGM and RD, inaddition to the standard cell culture repertoire of PMK andhuman diploid fibroblast cells, increased the isolation rate ofenteroviruses from clinical specimens by 18%. Furthermore,35% of specimens which were positive in BGM, RD, or bothwere recognized 1 day earlier than in the standard cell lines.In our experience, the speed of recovery and the recoveryrate of enteroviruses are increased by 11% when BGM andhuman embryonic kidney cells, in addition to PMK andhuman diploid fibroblast cells, are used (Chonmaitree et al.,Abstr. Annu. Meet. Am. Soc. Microbiol. 1988). Table 4demonstrates the speed of recovery of several enteroviruses;the data are from studies published between 1971 and 1987.Cumulative percentages of positive cultures ranged from 37
CLIN. MICROBIOL. REV.
on February 29, 2020 by guest
http://cmr.asm
.org/D
ownloaded from

THE VIROLOGY LABORATORY AND DIAGNOSIS OF CNS DISEASE
TABLE 4. Speed of enterovirus recovery by observation of CPE in cell culture
No.of ~~~~Cumulative % posiitive at day:Study (reference). yr published Cell lines used" Nso. 1fC2 4 7isolates I 3 4 7
Herrmann (59). 1971 Standard, HeLa 756 3 20 37 53 82Chonmaitree et al. (28). 1982 Standard. BGM 73 13 32 49 67 97Rubin (128), 1984 Standard NA" 5 25 45 55 90Dagan and Menegus (38), 1986 Standard. BGM. RD 417 10 42 59 69 89Wildin and Chonmaitree (157), 1987 Standard, BGM 123 2 22 52 69 87
" Standard cell culture was PMK and human diploid fibroblast cells. BGM is a continuous cell line of African green monkey kidney cells, and RD is humanrhabdomyosarcoma cells."NA. Not available.
to 59% by day 3 and from 82 to 97% by day 7, depending oncell types used.Animal inoculation. Inoculation into newborn mice is the
method of choice for primary isolation of most group Acoxsackieviruses (66, 93, 95). Although group B coxsackie-viruses and some newer enterovirus serotypes are alsopathogenic in newborn mice, it is easier to grow them in cellculture. Group A coxsackieviruses cause generalized myo-sitis accompanied by a flaccid type of paralysis. Group Bviruses cause focal myositis and typical lesions in theinterscapular fat pad and brain and occasionally producemyocarditis, endocarditis, hepatitis, and necrosis of acinartissue of the pancreas (93).
Identification of isolates. An isolate can be identified as anenterovirus with reasonable certainty on the basis of char-acteristic CPE in cell culture, combined with other informa-tion such as specimen source, time of year, and clinicalhistory of the patient (61, 95). When an enterovirus isisolated from CSF or blood from a patient with no recenthistory of poliovirus vaccination, it is safe to assume that theisolate is a nonpolio enterovirus and is the cause of thedisease. If the isolate grows in cell cultures inoculated witha throat swab, rectal swab, or stool specimen, both nonpolioenterovirus, which is probably causing the disease, andshedding of vaccine polioviruses must be considered. Aspecific identification of the serotype can be accomplishedby virus neutralization (NT), using intersecting virus antise-rum pools (85). If only vaccine polioviruses need to beseparated from nonpolio enteroviruses, a simple NT test canbe performed with pooled antisera to the three types ofpoliovirus (95).
Serology
Serologic diagnosis of enteroviral infection classicallyrelies upon comparison of neutralizing antibody activity (25)in acute- and convalescent-phase sera. A fourfold increase inneutralizing antibody titer against the suspected strain ofvirus is considered consistent with infection. The titer ofantibody against other strains may also rise because ofcross-reactivity. Use of an ELISA method to detect thepresence of immunoglobulin M (IgM) antibody during acuteinfection has been tested. At 2 weeks after infection, 16 of 19patients had detectable IgM titers against a pooled enterovi-rus antigen. Of 16 patients, 10 had IgM specific for theenterovirus causing the infection, while 6 had a heterotypicresponse (25). Similar heterotypic responses have beennoted by workers who used counterimmunoelectrophoresis(99) and immunodiffusion (132).
During an outbreak of echovirus type 33 infection inFrance, after no reports of the disease for more than 15years, tests for IgM detected 85% (33 of 39) of patients with
viral infection. The unusual circumstances made use of asingle reagent feasible (27). Because 3 to 21 days are neededfor a patient to generate either an 1gM or an IgG response(25, 47, 99, 132), serology is useful for retrospective studiesrather than routine diagnoses.One group of workers took advantage of the cross-reac-
tivity between enteroviral strains and developed a general-screening ELISA for enteroviral infection, using coxsackie-virus B1-5 antigens with specimens from 45 patients withaseptic meningitis (8). Twenty-one patients had an enterovi-rus recovered from CSF, feces, or sera, while 30 hadpositive ELISAs. The method was useful for both detectinginfection in culture-negative patients and confirming sys-temic infection in patients with virus recovered only fromfeces. The viruses isolated were coxsackievirus B5 andechoviruses 5, 6, 7, and 11. The disadvantage of the test wasthe need to use all five antigens, which made the procedureexpensive. The authors stressed the need for a single,cross-reactive reagent that could be used in these tests.
DIAGNOSTIC METHODS FOR NONENTEROVIRUSES
Togaviruses, Bunyaviruses, and Reoviruses
No rapid diagnostic methods have been developed fortogavirus, bunyavirus. and reovirus infections (52). Becauseof the relatively long period of time between infection andthe development of neurologic disease (5 to 14 days), virus isno longer present in blood when the patient is symptomatic(35). Venezuelan and western equine encephalitis viruseshave relatively shorter incubation periods (2 to 10 days), andfor the first 2 to 3 days after onset of illness, viremia may stillbe present. Virus has also been isolated from nasopharyn-geal secretions in Venezuelan equine encephalitis. In fatalcases, virus can be isolated from brain tissue. The specimenscan be inoculated intracranially into suckling mice or cellcultures of primary duck embryo, Vero, LLC-MK2, or BHKcells (35, 87. 113). Arthropod cell cultures have also beenused (138).
Serologic testing is the routine method of diagnosis. Com-plement fixation. hemagglutination inhibition, or plaque re-duction NT are performed on acute and convalescent (2 to 5weeks) sera. Because of the long incubation periods, hem-agglutination inhibition and NT are frequently positive earlyin the disease. Complement-fixing antibody appears later ormay fail to develop. The complement fixation test also showscross-reaction with other arboviruses. so that for peoplefrom endemic areas, or those who have received yellowfever vaccine, hemagglutination inhibition and NT are moreuseful (35).
VOL. 2, 1989 7
on February 29, 2020 by guest
http://cmr.asm
.org/D
ownloaded from

8 CHONMAITREE ET AL.
Herpesviruses
In disseminated neonatal HSV infection, several diagnos-tic procedures are possible. When skin lesions are present,infection with HSV can be confirmed by detecting viralantigen in smears of lesion scrapings or biopsies, using IF,immunoperoxidase, or ELISA procedures (80, 83, 104, 108).Sensitivity of these methods varies from 50 to 96% andspecificity varies from 91 to 100%. Detection of viral anti-gens is much easier in vesicular fluid than in swabs of cervixor other contaminated sites. A modification of the simpleELISA, the enzyme immunofiltration staining assay, isreportedly more sensitive with both vesicular fluid andcontaminated specimens. However, this procedure is not yetcommercially available (30, 31). Virus isolation is possibleby using lesion, throat, eye, and umbilical swabs, blood, andCSF. Over 90% of HSV grow in human diploid fibroblastcells within 4 days. Use of rabbit kidney or guinea pigembryo cells enhances rapidity of isolation by 1 to 2 days(18, 82, 129). Rapid detection by use of human fetal fibro-blast cell lines, combined with IF or immunoperoxidasestaining of inoculated cells, usually permits recognition ofthe virus after an overnight incubation (106, 109). A methodcombining cell culture and staining is the shell vial centrifu-gation method. This technique detects HSV within 16 to 48h after inoculation (49, 114, 120, 154). Serologic examinationis of no assistance is diagnosing neonatal infection due toHSV (6, 119).
Adult HSV meningoencephalitis is not usually associatedwith the peripheral presence of virus. Fever of any etiologycan cause reactivation of mucocutaneous HSV lesions; thus,patients with encephalitis caused by other viruses may haveperipheral HSV lesions. Brain biopsy is recommended forthe diagnosis of encephalitis before therapy is started, bothto confirm the diagnosis and to exclude other treatableinfections which often mimic signs and symptoms of HSVencephalitis. The biopsy should be of the involved area(usually the temporal lobe) recognized by either electroen-cephalography or computerized tomographic scan. The tis-sue should be divided, with part being sent to the histologylaboratory for immunoperoxidase staining and the rest inoc-ulated into cell culture as described above. CSF is notusually positive for virus (52). Although development ofmethods to detect specific viral glycoprotein in CSF is inprogress (127), no such procedures are currently available.Serology is not useful for diagnosis (6, 33).The characteristic lesions of chicken pox or herpes zoster
are frequently sufficient for diagnosis of VZV infection.However, HSV will occasionally cause vesicles in an appar-ent dermatomal distribution, with lesions which are indistin-guishable from those of VZV infection. If the vesicularlesions are not recognizable, scrapings of the lesions may bestained by using IF procedures. Isolation of VZV from thevesicles can be performed in human fetal fibroblasts. Thevirus is relatively slow growing (4 to 7 days) and may bedifficult to isolate because of the presence of antibody orinterferon in the vesicle, especially in the case of herpeszoster. Virus has also been isolated from the CSF in somecases (123). Serologic recognition of the presence of specificIgM may be useful for diagnosing primary chicken pox but isnot useful with herpes zoster (52).
Infection with EBV can be rapidly recognized in serum byusing the Monospot procedure, if the heterophile antibodyhas been induced. This test can be confirmed by IF proce-dures for specific IgM to EBV capsid antigen. In children,the Monospot procedure is frequently negative, and the IF
procedure is necessary to recognize infection with EBV (52).Although it is possible to isolate virus from blood or CSF,the procedure is slow and requires cultivation of the virus inlymphocytes. It is used only for research purposes.
Recognition of CNS infection due to CMV in the immu-nocompromised host is extremely difficult. Toxoplasma andHIV encephalitis present with similar symptoms. Neitherpositive serology nor isolation ofCMV from peripheral sitesis sufficient for differential diagnosis. In one study, the viruswas isolated from CSF in two of nine patients with AIDS, sothis approach may provide some useful information forAIDS patients (105). Therapy with gancyclovir is sometimesbegun without proof of current active CMV infection, ifantibody to CMV is present in the serum.
Mumps, Measles, and Rubella
No rapid procedures are available for diagnosing mumps(52). Isolation of the virus from CSF can be done in PMK,human diploid fibroblast, or HeLa cells. Cytopathology canbe confirmed by a hemadsorption test within 6 to 7 days.Serologic diagnosis can be made by testing for complement-fixing, hemagglutination-inhibiting, or NT antibodies (64).
Rapid diagnosis of measles infection during the exanthe-matous period is achieved by detection of measles antigen byELISA or IF in the nasopharyngeal secretions prior to and atthe onset of rash and in skin biopsy up to a few days afteronset of the rash. The virus is not recoverable from CSF orbrain biopsy (101). Specific IgM to measles appears duringthe first days of the illness, peaks at 10 days, and isdetectable for 4 weeks or more (52). Similar procedures areavailable for rubella.
Lymphocytic Choriomeningitis Virus
No rapid methods have been developed to detect infectionwith LCM (52). The virus can be isolated from CSF or bloodwith Vero cells, but detection of positive cultures requires IFtechniques because CPE is not apparent. Therefore, infec-tion is usually diagnosed by a fourfold rise in complement-fixing antibodies 1 to 2 weeks after infection (123).
Rabies
Rapid diagnosis of rabies is possible by using biopsy of theskin of the posterior neck, or conjunctival smears, and IFprocedures to recognize viral antigen (151). Serologic diag-nosis, using mouse infection NT or the rapid fluorescent-focus inhibition test, can also be performed. Antibody ineither serum or CSF indicates infection in the absence ofpast immunization. These procedures are generally availablein reference laboratories, but not in most clinical virologylaboratories.
HIV
Infection with HIV is recognizable by serologic tests. Apositive screening ELISA for antibody, followed by a con-firming procedure, usually Western blot (immunoblot) exam-ination, is indicative of systemic HIV infection. Althoughisolation of virus is possible, this method is generally re-served for research use because of the time and difficultiesinvolved. There is currently no good means of antemortemdiagnosis of CNS disease. Postmortem, viral antigen can bedetected in brain tissue by immunoperoxidase techniques,but positive results have been noted in patients without CNS
CLIN. MICROBIOL. REV.
on February 29, 2020 by guest
http://cmr.asm
.org/D
ownloaded from

THE VIROLOGY LABORATORY AND DIAGNOSIS OF CNS DISEASE
symptoms. It is possible that all people infected with HIVhave CNS infection (16, 140).
MANAGEMENT OF PATIENTS WITH CNS VIRALINFECTION
Aseptic Meningitis
Because clinical signs, symptoms, and initial laboratoryfindings do not always distinguish bacterial from viral men-
ingitis, the main practical problem for the clinician iswhether to hospitalize the patient and administer intrave-nous (i.v.) antibiotics. In some instances, the diagnosis ofviral disease may be suggested by evidence of rash or
parotitis accompanying aseptic meningitis, especially whenthe disease occurs during an outbreak of aseptic meningitis(76). When a lumbar puncture is traumatic and in conse-
quence the CSF results are not interpretable or when thepatient is very young, the physician may choose to initiateantibiotic therapy and continue it until the diagnosis ofbacterial meningitis can be excluded or the diagnosis of viralmeningitis can be confirmed. However, when the patient hasbeen partially treated with antibiotics, positive viral cultureresults are needed to support termination of antibiotic ther-apy, since negative bacterial culture results are no longermeaningful.Rapid antigen detection of bacteria which commonly
cause meningitis, although widely used, makes little impacton patient management when the results are positive (53).When the result is negative, however, it may in some cases
suggest the diagnosis of viral meningitis. Misdiagnosis ofbacterial as viral meningitis can have devastating conse-quences (137), and every effort should be made to preventthis error. One approach is to hospitalize and initiate i.v.antibiotic therapy in every patient with the diagnosis ofmeningitis, especially young infants, until a bacterial diag-nosis is excluded or a viral diagnosis is confirmed. Thispractice, although very popular, is also very costly. Further-more, the patient carries all the risks of hospital-relatedmorbidity, complications of parenteral fluid therapy andantibiotics, iatrogenic diagnostic and therapeutic mishaps,and family stress caused by separation from the youngpatient and loss of work productivity (36, 40). Rapid confir-mation of the viral etiology of the disease will thereforegreatly benefit the patient. The proven benefits will bereviewed in the following section.There is no specific treatment for viral meningitis except
when it is caused by HSV. Only supportive and symptomatictreatment such as rest, analgesics, and antipyretics, if nec-
essary, is recommended.
Meningoencephalitis
Specific drug therapy is available only for HSV encepha-litis; treatment of other forms of viral meningoencephalitis islargely supportive (121). Vidarabine was the first antiviraldrug shown to be effective in treatment of HSV encephalitis(156). Subsequently, two independent groups, one fromSweden (139) and the other from the NIAID CollaborativeAntiviral Study Group (155), demonstrated the superiority ofacyclovir over vidarabine. The current recommendation is togive acyclovir i.v. three times a day for at least 10 days. Theefficacy of acyclovir in CNS disease caused by VZV, EBV,or CMV has not been demonstrated. Supportive therapy forviral meningoencephalitis consists of control of increasedintracranial pressure, control of seizures, and general mea-
sures such as maintenance of fluid and electrolyte balance,oxygenation, pulmonary toilet, skin care, and ventilatorysupport if necessary. In most instances, appropriate antibi-otics for bacterial meningitis are administered until CSFculture is negative for bacteria, after the usual 48- to 72-hincubation period.
Enteroviral Meningoencephalitis Associated withAgammaglobulinemia
The treatment for enteroviral meningoencephalitis associ-ated with agammaglobulinemia is empiric; there is no currentconsensus on the best therapy. Because no specific drugagainst enteroviruses is available, the only therapeutic mo-dality with efficacy is the administration of specific neutral-izing antibody, usually as part of a mixed immunoglobulinpreparation. Some reports suggest that administration of i.v.immunoglobulin, plasma, or immune serum with a high titeragainst the causative virus could improve outcome (91, 118,158). Others have been successful in using intrathecal orintraventricular immunoglobulin in combination with i.v.immunoglobulin (45, 73, 91).
INFLUENCE OF THE VIROLOGY LABORATORY ONPATIENT MANAGEMENT
For a diagnostic virology laboratory to make an impact onpatient management, ample communication between thephysicians and the laboratory is required. The laboratoryfaces the challenge of educating physicians to order appro-priate tests, carry out appropriate specimen collection andtransportation, and interpret the results correctly. Physi-cians, in turn, can provide information about the diseasesthey commonly deal with, so the laboratory can emphasizetests that optimize the physician's management of the pa-tient. An on-site virology laboratory, if available, is the mostuseful because it enhances physician-laboratory communi-cation. In addition, specimen transport time is reduced to aminimum, allowing early inoculation with specimens thathave the highest virus titer. When an on-site laboratory isnot available, however, appropriate specimen collection andrapid transport can provide similar yields (124).The usefulness of a diagnostic test in patient management
depends on the sensitivity and specificity of the test, its easein execution, and the cost and timely availability of theresults (53). In general, the sooner the results are provided,the more helpful they can be in patient management. Rapiddiagnosis such as microbial antigen detection from clinicalspecimens is therefore preferred for initial patient manage-ment. However, because of the problems with sensitivity,specificity, and availability of rapid antigen detection tests,isolation of the microbial organism remains the standard fordiagnosis in most instances. Rapid antigen detection, whenavailable, is generally performed in parallel with culture, anda definite diagnosis is generally not made until culture resultsare available. To ensure that viral culture results are mosteffective in patient management, the laboratory, with thephysician's cooperation, can maximize the speed of virusisolation by increasing the amount of virus in the specimen(appropriate collection and transport), using a combinationof cell types appropriate for the virus to be recovered,increasing the frequency with which cultures are examined,and reporting results rapidly to the physicians as soon asthey are available.Many clinical virology laboratories are capable of provid-
ing diagnostic information on diseases caused by enterovi-
9VOL. 2, 1989
on February 29, 2020 by guest
http://cmr.asm
.org/D
ownloaded from

10 CHONMAITREE ET AL.
ruses, herpesviruses, and HIV. For viral diagnosis of CNSinfections caused by togaviruses, bunyaviruses, reoviruses,mumps, measles, rubella, lymphocytic choriomeningitis vi-rus, and rabies, reference laboratories are generally con-sulted. While laboratory diagnosis of many CNS viral infec-tions is not specifically required for supportive andsymptomatic treatment of the diseases, direct benefits to thepatient can result from a timely diagnosis of HSV CNSinfection, a treatable disease, and enteroviral infection, themost common viral infection of the CNS.The virology laboratory plays a direct role in management
of patients with herpes simplex encephalitis, the same way abacteriology laboratory directs the management of patientswith bacterial meningitis. When a patient is considered tohave HSV CNS disease, specimens are collected frombiopsied brain tissue or CSF or both. Direct IF or ELISAstaining of brain tissue, using specific HSV antibody, can beperformed, and results are available within a few hours (80,83, 104, 108, 128). Culture results for confirmation aregenerally available in 1 to 5 days (94).
Although there is no specific treatment for enteroviraldisease, immunocompromised patients with CNS diseasebenefit from immunoglobulin therapy. The virology labora-tory can play a direct role in making a diagnosis of entero-viral infection. If NT is available, the laboratory can help toidentify which high-titer immunoglobulins are needed for thespecific virus serotype. More commonly, the laboratory canmake a diagnosis of enteroviral meningitis, a disease encoun-tered by most physicians dealing with children, especiallyduring the summer and fall months. Early evidence suggest-ing that a diagnosis of enteroviral meningitis might affectpatient management was first reported by Pearson et al. in1972 (110). During a 1970 epidemic of aseptic meningitisattributed primarily to echovirus 3, the epidemiologic diag-nosis provided by the virology laboratory caused physiciansto change their practice style. During the first half of theepidemic, all of the patients with meningitis were hospital-ized and 60% of them were given antibiotics. During thesecond half of the epidemic, after many cases of enteroviralmeningitis had been identified, less than half of meningitispatients were hospitalized and only a few of these were giveni.v. antibiotics. Singer et al. (137) subsequently used viralculture results to develop a protocol for management of CNSinfections during an epidemic of enteroviral aseptic menin-gitis. These reports demonstrated the usefulness of thevirology laboratory in general management of patients dur-ing epidemics of enteroviral disease, although they did notdirectly affect management of the individual patient.
Enteroviruses are by far the most common pathogenscausing hospitalization for suspected sepsis in young infantsduring the summer and fall in the United States (37, 74).Making a viral diagnosis in these infants early in the courseof hospitalization provides tremendous benefits to the pa-tients themselves, as well as helping to identify a communityoutbreak, guiding in infection control, and educating physi-cians regarding the diseases they are dealing with. In Roch-ester, N.Y., during the summer and fall months of 1979 and1980, 111 patients were diagnosed as having aseptic menin-*gitis or meningoencephalitis or both (28). Enteroviruseswere identified as the cause of meningitis in 46 cases (41%).The diagnosis of enteroviral meningitis was based on posi-tive viral culture of CSF, throat swab, and/or rectal swab orstool samples. By using standard cell cultures and BGM, theviruses were isolated from these specimens within 1 to 14days. The isolation of enteroviruses from these 46 patientsdirectly influenced the diagnosis and management of 22
cases (48%) and confirmed the diagnosis as well as specifiedthe etiologic agent in the other 24 cases (52%).The effects of virus isolation on the diagnosis, manage-
ment, and prognosis of patients with enteroviral meningitisare as follows.* Early withdrawal of antibiotics* Early hospital discharge* Avoidance of i.v. administration and complications* Avoidance of unnecessary tests and their complications* Diagnosis of meningitis in patients without CSF
pleocytosis* Specification of etiologic agent of meningitis* Indication for prognosis* Ability to diagnose and guide high-titer immunoglobulin
therapy for immunocompromised patientsNeonates, patients who had received oral antibiotics beforea lumbar puncture was performed, and patients with ques-tionable CSF findings were all hospitalized and treated withi.v. antibiotics until an enterovirus was isolated. Virusisolation resulted in withdrawal of antibiotics and earlydischarge of these patients, saving thousands of dollars andhelping to avoid the potential complications of i.v. drugadministration and unnecessary tests. In addition, positiveenteroviral culture results helped identify young infants whowould not otherwise have been diagnosed as having a CNSdisease, such as infants with no CSF pleocytosis or thosewhose spinal taps were uninterpretable. The prognosis inthese cases was altered because of the possible sequelae ofthe disease in this age group (11, 46, 122, 134, 161). AtUTMB in Galveston, the virology laboratory has beenshown to have a similar influence on patient management(157). From 1983 to 1985, 69 patients under 18 years of agewere diagnosed and treated for enteroviral meningitis. Withthree cell types, including BGM, cultures of CSF, throatswab, and/or rectal swab or stool specimens were foundpositive for an enterovirus within 1 to 11 days. Half of the 49patients in whom the diagnosis was made, based on positiveCSF culture, benefited directly from the viral culture results.From the point of view of cost-effectiveness, viral diagno-
sis is highly advantageous. The cost of viral culture atUTMB is comparable to that of bacterial blood culture orrapid bacterial antigen detection. Although the laboratorytests required for making or excluding the diagnosis ofbacterial sepsis, with or without meningitis, include only aCSF examination and blood and CSF bacterial culture,numerous other tests are often ordered. These includenonspecific tests such as complete leukocyte count anddifferential, platelet count, urinalysis, urine bacterial cul-ture, and serum electrolytes. Rapid bacterial antigen detec-tion for three to four common bacteria from CSF or urine orboth is also frequently performed, although results rarelychange patient management (53). If the patient continues tohave fever while on antibiotic therapy, tests such as chest Xrays, computerized tomographic scan, and repeat examina-tion of CSF may be obtained. All of these tests are costly andput the patient at risk for untoward effects. Positive entero-viral culture results, especially early in the course of thedisease, provide a definitive diagnosis which can save thepatient from unnecessary investigations and treatment andsometimes indicate a different prognosis.
CONCLUSION
Numerous types of viruses cause CNS infection. Amongthese, enteroviruses are by far the most common cause ofacute CNS infection, a disease that mimics sepsis and
CLIN. MICROBIOL. REV.
on February 29, 2020 by guest
http://cmr.asm
.org/D
ownloaded from

THE VIROLOGY LABORATORY AND DIAGNOSIS OF CNS DISEASE
bacterial meningitis, especially in infants and young chil-dren. CNS infection caused by HSV, although not common,is now treatable. Provided that results can be obtainedexpeditiously, the virology laboratory can play an importantrole in the diagnosis and management of both enteroviral andHSV CNS infection, while it provides diagnosis and guidesin supportive therapy for other CNS viral diseases. It ishoped that knowledge of the impact of the virology labora-tory on management of patients as presented here willstimulate an increased and more intelligent use of virologylaboratories, improved communication and cooperation be-tween laboratory and physician, and an increased demandfor the establishment of these laboratories at institutionswhere none are currently available.
ACKNOWLEDGMENTS
We thank Lynn Burke of the Clinical Library Service, Universityof Texas Medical Branch, and Melba Nessler for assistance inpreparing this manuscript.
LITERATURE CITED1. Abbott, R. J., I. Bolderson, and P. J. Gruer. 1987. Assessment
of an immunoassay for interferon-alpha in cerebrospinal fluidas a diagnostic acid in infections of the central nervous system.J. Infect. 15:153-160.
2. Abbott, R. J., I. Bolderson, P. J. K. Gruer, and R. C. Peatfield.1987. Immunoreactive IFN-gamma CSF in neurological disor-ders. J. Neurol. Neurosurg. Psychiatry 50:882-885.
3. Adair, C. V., R. L. Gauld, and J. E. Smadel. 1953. Asepticmeningitis, a disease of diverse etiology: clinical and etiologicstudies on 854 cases. Ann. Intern. Med. 39:675-704.
4. Armstrong, C. 1941. Studies on choriomeningitis and poliomy-elitis. Bull. N.Y. Acad. Med. 17:295-318.
5. Bardelas, J. A., J. A. Winkelstein, D. S. Y. Seto, T. Tsai, andA. D. Rogol. 1977. Fatal ECHO 24 infection in a patient withhypogammaglobulinemia: relationship to dermatomyositis-likesyndrome. J. Pediatr. 90:396-399.
6. Barnes, D. W., and R. J. Whitley. 1986. CNS diseases associ-ated with varicella zoster virus and herpes simplex virusinfection: pathogenesis and current therapy. Neurol. Clin. 4:265-283.
7. Bell, E. J., and B. P. Cosgrove. 1980. Routine enterovirusdiagnosis in a human rhabdomyosarcoma cell line. Bull.W.H.O. 58:423-428.
8. Bell, E. J., R. A. McCartney, D. Basquill, and A. K. R.Chaudhuri. 1986. Mu antibody capture ELISA for the rapiddiagnosis of enterovirus infections in patients with asepticmeningitis. J. Med. Virol. 19:213-217.
9. Benson, C. A., and A. A. Harris. 1986. Acute neurologicinfection. Med. Clin. N. Am. 70:987-1011.
10. Berg, R., and H. Jelke. 1965. Acute cerebellar ataxia inchildren associated with Coxsackie viruses group B. ActaPaediatr. Scand. 54:497-502.
11. Bergman, I., M. J. Painter, E. R. Wald, D. Chiponis, A. L.Holland, and H. G. Taylor. 1987. Outcome in children withenteroviral meningitis during the first year of life. J. Pediatr.110:705-709.
12. Berkovich, S., and S. Kibrick. 1964. ECHO II outbreak innewborn infants and mothers. Pediatrics 33:534-540.
13. Bernstein, T. C., and H. G. Wolff. 1950. Involvement of thenervous system in infectious mononucleosis. Ann. Intern.Med. 33:1120-1138.
14. Berry, P. J., and J. Nagington. 1982. Fatal infection withechovirus 11. Arch. Dis. Child. 57:22-29.
15. Bowen, G. S., M. C. Fisher, A. Deforest, C. M. Thompson, Jr.,B. Kleger, and H. Friedman. 1983. Epidemic of meningitis andfebrile illness in neonates caused by ECHO type 11 virus inPhiladelphia. Pediatr. Infect. Dis. J. 2:359-363.
16. Britton, C. B., and J. R. Miller. 1984. Neurological complica-tions in acquired immunodeficiency syndrome (AIDS). Neurol.Clin. 2:315-339.
17. Bromberg, K., P. R. Shank, S. H. Zinner, and G. Peter. 1983.Inability of counterimmunoelectrophoresis to detect echovirusin cerebrospinal fluid. Am. J. Clin. Pathol. 80:383-385.
18. Callihan, D. R., and M. A. Menegus. 1984. Rapid detection ofherpes simplex virus in clinical specimens with human embry-onic lung fibroblast and primary rabbit kidney cell cultures. J.Clin. Microbiol. 19:563-565.
19. Center for Disease Control. 1977. Mumps vaccine. Morbid.Mortal. Weekly Rep. 26:393-394.
20. Center for Disease Control. 1979. Aseptic meningitis surveil-lance. Annual summary 1976. U.S. Government Printing Of-fice, Atlanta.
21. Centers for Disease Control. 1980. Mumps vaccine. Morbid.Mortal. Weekly Rep. 29:87-88, 93-94.
22. Centers for Disease Control. 1981. Measles encephalitis-United States, 1962-1979. Morbid. Mortal. Weekly Rep.30:362-364.
23. Centers for Disease Control. 1984. Mumps surveillance, Jan.1977-Dec. 1982. U.S. Government Printing Office, Atlanta.
24. Centers for Disease Control. 1984. Annual summary 1983:reported morbidity and mortality in the United States. Morbid.Mortal. Weekly Rep. 32:15, 114-116.
25. Chan, D., and G. W. Hammond. 1985. Comparison of serodi-agnosis of group B coxsackievirus infections by an immuno-globulin M capture enzyme immunoassay versus microneutra-lization. J. Clin. Microbiol. 21:830-834.
26. Cherry, J. D. 1987. Enteroviruses: polioviruses (poliomyelitis),coxsackieviruses, echoviruses, and enteroviruses, p. 1729-1790. In R. D. Feigin and J. D. Cherry (ed.), Textbook ofpediatric infectious diseases. W. B. Saunders Co., Philadel-phia.
27. Chomel, J. J., D. Thouvenot, V. Fayol, and M. Aymard. 1985.Rapid diagnosis of echovirus type 33 meningitis by specificIgM detection using an enzyme linked immunosorbent assay(Elisa). J. Virol. Methods 10:11-19.
28. Chonmaitree, T., M. A. Menegus, and K. R. Powell. 1982. Theclinical relevance of 'CSF viral culture.' A two-year experi-ence with aseptic meningitis in Rochester, NY. J. Am. Med.Assoc. 247:1843-1847.
29. Chonmaitree, T., M. A. Menegus, E. M. Schervish-Swierkosz,and E. Schwalenstocker. 1981. Enterovirus 71 infection: reportof an outbreak with two cases of paralysis and a review of theliterature. Pediatrics 67:489-493.
30. Cleveland, P. H., and D. D. Richman. 1987. Enzyme immuno-filtration staining assay for immediate diagnosis of herpessimplex virus and varicella-zoster virus directly from clinicalspecimens. J. Clin. Microbiol. 25:416-420.
31. Cleveland, P. H., D. D. Richman, D. C. Redfield, D. R.Disharoon, P. S. Binder, and M. N. Oxman. 1982. Enzymeimmunofiltration technique for rapid diagnosis of herpes sim-plex virus eye infection in a rabbit model. J. Clin. Microbiol.16:676-685.
32. Cooper, J. B., W. R. Pratt, B. K. English, and W. T. Shearer.1983. Coxsackievirus B3 producing fatal meningoencephalitisin a patient with x-linked agammaglobulinemia. Am. J. Dis.Child. 137:82-83.
33. Corey, L., and P. G. Spear. 1986. Infections with herpessimplex viruses. N. Engl. J. Med. 314:749-757.
34. Corrall, J. C., J. M. Pepple, E. R. Moxon, and W. T. Hughes.1981. C-reactive protein in spinal fluid of children with menin-gitis. J. Pediatr. 99:365-369.
35. Craven, R. B. 1984. Togaviruses, p. 599-648. In R. B. Belshe(ed.), Textbook of human virology. P.S.G. Publishing Co.,Inc., Littleton, Mass.
36. Dagan, R., J. A. Jenista, and M. A. Menegus. 1985. Clinical,epidemiological and laboratory aspects of enterovirus infectionin young infants, p. 123-151. In L. M. de la Maza and E. M.Peterson (ed.), Medical virology IV. Lawrence Erlbaum Asso-ciates, Hillsdale, N.J.
37. Dagan, R., J. A. Jenista, S. L. Prather, K. R. Powell, and M. A.Menegus. 1985. Viremia in hospitalized children with entero-virus infections. J. Pediatr. 106:397-401.
38. Dagan, R., and M. A. Menegus. 1986. A combination of four
11VOL. 2, 1989
on February 29, 2020 by guest
http://cmr.asm
.org/D
ownloaded from

12 CHONMAITREE ET AL.
cell types for rapid detection of enteroviruses in clinicalspecimens. J. Med. Virol. 19:219-228.
39. Dahling, D. R., G. Berg, and D. Berman. 1974. BGM, acontinuous cell line more sensitive than primary rhesus andAfrican green kidney cells for the recovery of viruses fromwater. Health Lab. Sci. 11:275-282.
40. DeAngelis, C., A. Joffe, M. Wilson, and E. Willis. 1983.iatrogenic risks and financial costs of hospitalizing febrileinfants. Am. J. Dis. Child. 137:1146-1149.
41. Dery, P., M. I. Marks, and R. Shapera. 1974. Clinical manifes-tations of Coxsackievirus infections in children. Am. J. Dis.Child. 128:464-468.
42. Diebel, R., and T. D. Flanagan. 1979. Central nervous systeminfections: etiologic and epidemiologic observations in NewYork State, 1976-1977. N.Y. State J. Med. 79:689-695.
43. Domok, I., and E. Molnar. 1960. An outbreak of meningoen-cephalomyocarditis among newborn infants during the epi-demic of Bornholm disease of 1958 in Hungary. II. Aetiologicalfindings. Ann. Pediatr. 194:102-114.
44. Donald, P. R., P. J. Burger, and W. B. Becker. 1986. Paediatricmeningitis in the Western Cape. S. Afr. Med. J. 70:391-395.
45. Erlendsson, K., T. Swartz, and J. M. Dwyer. 1985. Successfulreversal of echovirus encephalitis in x-linked hypogamma-globulinemia by intraventricular administration of immuno-globulin. N. Engl. J. Med. 312:351-353.
46. Farmer, K., B. A. MacArthur, and M. M. Clay. 1975. Afollow-up study of 15 cases of neonatal meningoencephalitisdue to coxsackie virus B5. J. Pediatr. 87:568-571.
47. Forsgren, M. 1968. Studies of echovirus type 6 antigens inimmunodiffusion. 3. Antibody response against echovirus 6antigens in human infections with homologous and heterolo-gous enteroviruses. Acta Pathol. Microbiol. Scand. 74:611-623.
48. Gabuzda, D. H., and M. S. Hirsch. 1987. Neurologic manifes-tations of infection with human immunodeficiency virus: clin-ical features and pathogenesis. Ann. Intern. Med. 107:383-391.
49. Gleaves, C. A., D. J. Wilson, A. D. Wold, and T. F. Smith.1985. Detection and serotyping of herpes simplex virus inMRC-5 cells by use of centrifugation and monoclonal antibod-ies in 16 h postinoculation. J. Clin. Microbiol. 21:29-32.
50. Goldberg, F., and L. B. Weiner. 1981. Cerebrospinal fluidwhite blood cell counts and lactic acid dehydrogenase inenterovirus type 71 meningitis. Clin. Pediatr. 20:327-330.
51. Gotoff, S. P., R. D. Smith, and 0. Sugar. 1972. Dermatomyo-sitis with cerebral vasculitis in a patient with agammaglobuli-nemia. Am. J. Dis. Child. 123:53-56.
52. Grandien, M., and E. Olding-Stenkvist. 1984. Rapid diagnosisof viral infections in the central nervous system. Scand. J.Infect. Dis. 16:1-8.
53. Granoff, D. M., T. V. Murphy, D. L. Ingram, and K. L. Cates.1986. Use of rapidly generated results in patient management.Diagn. Microbiol. Infect. Dis. 4:157S-166S.
54. Grist, N. R., E. J. Bell, and F. Assaad. 1978. Enteroviruses inhuman disease. Prog. Med. Virol. 24:114-157.
55. Grose, C., W. Henle, G. Henle, and P. M. Feorino. 1975.Primary Epstein-Barr virus infections in acute neurologic dis-eases. N. Engl. J. Med. 292:392-395.
56. Halfon, N., and S. A. Spector. 1981. Fatal echovirus type 11infections. Am. J. Dis. Child. 135:1017-1020.
57. Harrison, S. A., and W. L. Risser. 1988. Repeat lumbarpuncture in the differential diagnosis of meningitis. Pediatr.Infect. Dis. J. 7:143-145.
58. Haynes, R. E., H. G. Cramblett, and H. J. Kronfol. 1969.Echovirus 9 meningoencephalitis in infants and children. J.Am. Med. Assoc. 208:1657-1660.
59. Herrmann, E. C., Jr. 1971. Efforts toward a more useful viraldiagnostic laboratory. Am. J. Clin. Pathol. 56:681-686.
60. Herrmann, E. C., Jr., and J. A. Herrmann. 1976. Survey ofviral diagnostic laboratories in medical centers. J. Infect. Dis.133:359-362.
61. Herrmann, E. C., Jr., D. A. Person, and T. F. Smith. 1972.Experience in laboratory diagnosis of enterovirus infections inroutine medical practice. Mayo Clin. Proc. 47:577-586.
62. Ho-Yen, D. O., and D. Carrington. 1987. Alpha-interferonresponses in cerebrospinal fluid of patients with suspectedmeningitis. J. Clin. Pathol. 40:83-86.
63. Hopley, J. F. A., and F. W. Doane. 1985. Development of asensitive Protein A-gold immunoelectron microscopy methodfor detecting viral antigens in fluid specimens. J. Virol. Meth-ods 12:135-147.
64. Hopps, H. E., and P. D. Parkman. 1979. Mumps virus, p. 633-653. In E. H. Lennette and N. J. Schmidt (ed.), Diagnosticprocedures for viral, rickettsial, and chlamydial infections, 5thed. American Public Health Association, Washington, D.C.
65. Hoyne, A. L., and E. L. Slotkowski. 1947. Frequency ofencephalitis as a complication of measles. Am. J. Dis. Child.73:554-558.
66. Hsiung, G. D. (ed.). 1982. Diagnostic virology, 3rd ed., p. 89-109. Yale University Press, New Haven, Conn.
67. Hyypia, T., and U. Pettersson. 1985. Spot hybridization for thedetection of adenoviruses and enteroviruses. Symposium onnucleic acid probes and monoclonal antibodies. Clin. Lab.Med. 5:491-501.
68. Hyypia, T., P. Stalhandske, R. Vainionpaa, and U. Pettersson.1984. Detection of enteroviruses by spot hybridization. J. Clin.Microbiol. 19:436-438.
69. Johnson, D. A., and A. W. Eger. 1967. Myelitis associated withan echovirus. J. Am. Med. Assoc. 201:637-638.
70. Johnstone, J. A., C. A. C. Ross, and M. Dunn. 1972. Meningitisand encephalitis associated with mumps infection; a 10 yearsurvey. Arch. Dis. Child. 47:647-651.
71. Kibrick, S., and K. Benirschke. 1958. Severe generalizeddisease (encephalohepatomyocarditis) occurring in the new-born period and due to infection with coxsackie virus, group B.Pediatrics 22:857-874.
72. King, D. L., and D. T. Karzon. 1962. An epidemic of asepticmeningitis syndrome due to ECHO virus type 6. Pediatrics 29:432-437.
73. Kondoh, H., K. Kobayashi, Y. Sugio, and T. Hayashi. 1987.Successful treatment of echovirus meningoencephalitis in sex-linked agammaglobulinaemia by intrathecal and intravenousinjection of high titre gammaglobulin. Eur. J. Pediatr. 146:610-612.
74. Krober, M. S., J. W. Bass, J. M. Powell, F. R. Smith, andD. S. Y. Seto. 1985. Bacterial and viral pathogens causing feverin infants less than 3 months old. Am. J. Dis. Child. 139:889-892.
75. Krous, H. F., D. Dietzman, and C. G. Ray. 1973. Fatalinfections with echovirus types 6 and 11 in early infancy. Am.J. Dis. Child. 126:842-846.
76. Krugman, S., S. L. Katz, A. A. Gershon, and C. M. Wilfert(ed.). 1985. Infectious diseases of children, 8th ed., p. 167-173.C. V. Mosby, St. Louis.
77. Kurnetz, R., A. Cacciarelli, R. Egerer, and S. S. Yang. 1981.Neonatal infection. J. Pediatr. 99:822-826.
78. La Boccetta, A. C., and A. S. Tornay. 1964. Measles enceph-alitis. Report of 61 cases. Am. J. Dis. Child. 107:247-255.
79. Lake, A. M., B. A. Lauer, J. C. Clark, R. L. Wesenberg, and K.McIntosh. 1976. Enterovirus infections in neonates. J. Pediatr.89:787-791.
80. Land, S. A., I. J. Skurrie, and G. L. Gilbert. 1984. Rapiddiagnosis of herpes simplex virus infection by enzyme-linkedimmunosorbent assay. J. Clin. Microbiol. 19:865-869.
81. Landry, M. L., and G. D. Hsiung. 1981. The virus diagnosticlaboratory: its function in a VA medical center. Conn. Med.45:417-422.
82. Landry, M. L., D. R. Mayo, and G. D. Hsiung. 1982. Compar-ison of guinea pig embryo cells, rabbit kidney cells, and humanembryonic lung fibroblast cell strains for isolation of herpessimplex virus. J. Clin. Microbiol. 15:842-847.
83. Lawrence, T. G., D. B. Budzko, and B. W. Wilcke. 1984.Detection of herpes simplex virus in clinical specimens by anenzyme-linked immunosorbent assay. Am. J. Clin. Pathol. 81:339-341.
84. Lenahan, M. F., and H. A. Wenner. 1960. Propagation ofentero- and other viruses in renal cells obtained from non-
CLIN. MICROBIOL. REV.
on February 29, 2020 by guest
http://cmr.asm
.org/D
ownloaded from

THE VIROLOGY LABORATORY AND DIAGNOSIS OF CNS DISEASE
primate hosts. J. Infect. Dis. 107:203-212.85. Lim, K. A., and M. Benyesh-Melnick. 1960. Typing of viruses
of combinations of antiserum pools. Application to typing ofenterovirus (coxsackie and ECHO). J. Immunol. 84:309-317.
86. Linnemann, C. C., Jr., D. B. May, W. K. Schubert, C. T.Caraway, and G. M. Schiff. 1973. Fatal viral encephalitis inchildren with x-linked hypogammaglobulinemia. Am. J. Dis.Child. 126:100-103.
87. Luby, J. P., C. V. Sanders, and S. E. Sulkin. 1971. Interferonassays and quantitative virus determinations in a fatal infectionin man with western equine encephalomyelitis virus. Am. J.Trop. Med. Hyg. 20:765-769.
88. Magoffin, R. L., E. H. Lennette, and N. J. Schmidt. 1961.Association of coxsackie viruses with illnesses resembling mildparalytic poliomyelitis. Pediatrics 28:602-613.
89. Mailer, H. M., D. F. Powars, R. E. Horowitz, and B. Portnoy.1%7. Fatal myocarditis associated with ECHO virus, type 22,infection in a child with apparent immunological deficiency. J.Pediatr. 71:204-210.
90. McKee, K. T., Jr., C. J. Peters, R. B. Craven, and D. B.Francy. 1984. Other viral hemorrhagic fevers and ColoradoTick Fever, p. 649-677. In R. B. Belshe (ed.), Textbook ofhuman virology. P.S.G. Publishing Co., Littleton, Mass.
91. McKinney, R. E., S. L. Katz, and C. M. Wilfert. 1987. Chronicenteroviral meningoencephalitis in agammaglobulinemic pa-tients. Rev. Infect. Dis. 9:334-356.
92. Mease, P. J., H. D. Ochs, and R. J. Wedgwood. 1981. Success-ful treatment of echovirus meningoencephalitis and myositis-fascilitis with intravenous immune globulin therapy in a patientwith x-linked agammaglobulinemia. N. Engl. J. Med. 304:1278-1281.
93. Melnick, J. L., H. A. Wenner, and C. A. Phillips. 1979.Enteroviruses, p. 471-534. In E. H. Lennette and N. J.Schmidt (ed.), Diagnostic procedures for viral, rickettsial, andchlamydial infections. American Public Health Association,Washington, D.C.
94. Menegus, M. A. 1984. Diagnostic virology, p. 179-191. In R. B.Belshe (ed.), Textbook of human virology. P.S.G. PublishingCo., Littleton, Mass.
95. Menegus, M. A. 1985. Enteroviruses, p. 743-746. In E. H.Lennette, A. Balows, W. J. Hausler, Jr., and H. J. Shadomy(ed.), Manual of clinical microbiology, 4th ed. American Soci-ety for Microbiology, Washington, D.C.
96. Menegus, M. A., and G. E. Hollick. 1982. Increased efficiencyof group B coxsackievirus isolation from clinical specimens byuse of BGM cells. J. Clin. Microbiol. 15:945-948.
97. Meyer, H. M., Jr., R. T. Johnson, I. P. Crawford, H. E.Dascomb, and N. G. Rogers. 1960. Central nervous systemsyndromes of "viral" etiology. Am. J. Med. 29:334-347.
98. Michalski, F. J. 1984. Diagnostic virology in a communityhospital. Yale J. Biol. Med. 57:743-749.
99. Minor, T. E., P. B. Helstrom, D. B. Nelson, and D. J. D'Alessio.1979. Counterimmunoelectrophoresis test for immunoglobulinM antibodies to group B coxsackievirus. J. Clin. Microbiol. 9:503-506.
100. Mintz, L., and W. L. Drew. 1980. Relation of culture site to therecovery of nonpolio enterovirus. Am. J. Clin. Pathol. 74:324-326.
101. Modlin, J. F. 1984. Measles virus, p. 333-360. In R. B. Belshe(ed.), Textbook of human virology. P.S.G. Publishing Co.,Littleton, Mass.
102. Moore, M. 1982. Enteroviral disease in the United States,1970-1979. J. Infect. Dis. 146:103-108.
103. Morens, D. M., R. M. Zweighaft, and J. M. Bryan. 1979.Non-polio enterovirus disease in the United States, 1971-1975.Int. J. Epidemiol. 8:49-54.
104. Morgan, M. A., and T. F. Smith. 1984. Evaluation of anenzyme-linked immunosorbent assay for the detection of her-pes simplex virus antigen. J. Clin. Microbiol. 19:730-732.
105. Morgello, S., E. S. Cho, S. Nielsen, 0. Devinsky, and C. K.Petitio. 1987. Cytomegalovirus encephalitis in patients withacquired immunodeficiency syndrome: an autopsy study of 30cases and a review of the literature. Hum. Pathol. 18:289-297.
106. Myer, M. P., and A. J. Amortegui. 1984. Rapid detection ofherpes simplex virus using a combination of human fibroblastcell cultures and peroxidase-antiperoxidase staining. Am. J.Clin. Pathol. 81:43-47.
107. Nelson, D., H. Hiemstra, T. Minor, and D. D'Alessio. 1979.Non-polio enterovirus activity in Wisconsin based on a 20-yearexperience in a diagnostic virology laboratory. Am. J. Epide-miol. 109:352-361.
108. Nerurkar, L. S., M. Namba, G. Brashears, A. J. Jacob, Y. J.Lee, and J. L. Sever. 1984. Rapid detection of herpes simplexvirus in clinical specimens by use of a capture biotin-streptav-idin enzyme-linked immunosorbent assay. J. Clin. Microbiol.20:109-114.
109. Nerurkar, L. S., M. Namba, and J. L. Sever. 1984. Comparisonof standard tissue culture, tissue culture plus staining, anddirect staining for detection of genital herpes simplex virusinfection. J. Clin. Microbiol. 19:631-633.
110. Pearson, G., A. Valdmanis, J. D. Mann, M. E. Becker, andK. R. Wilcox, Jr. 1972. The impact of viral diagnostic studieson medical practice: a report of three years' experience withenterovirus isolation in a hospital laboratory. Am. J. Clin.Pathol. 58:349-357.
111. Peltola, H. 0. 1982. C-reactive protein for rapid monitoring ofinfections of the central nervous system. Lancet i:980-982.
112. Peters, A. C. B., J. Versteeg, G. T. A. M. Bots, J. Lindeman,and R. E. H. Smeets. 1979. Nervous system complications ofherpes zoster: immunofluorescent demonstration of varicella-zoster antigen in CSF cells. J. Neurol. Neurosurg. Psychiatry42:452-457.
113. Peters, C. J., and J. W. LeDuc. 1984. Bunyaviruses, phlebovi-ruses and related viruses, p. 547-598. In R. B. Belshe (ed.),Textbook of human virology. P.S.G. Publishing Co., Littleton,Mass.
114. Peterson, E. M., B. L. Hughes, S. L. Aarnaes, and L. de LaMaza. 1988. Comparison of primary rabbit kidney and MRC-5cells and two stain procedures for herpes simplex virus detec-tion by a shell vial centrifugation method. J. Clin. Microbiol.26:222-224.
115. Phillips, C. A., M. D. Aronson, J. Tomkow, and M. E. Phillips.1980. Enteroviruses in Vermont, 1969-1978: an importantcause of illness throughout the year. J. Infect. Dis. 141:162-164.
116. Ponka, A., and T. Pettersson. 1982. The incidence and aetiol-ogy of central nervous system infections in Helsinki in 1980.Acta Neurol. Scand. 66:529-535.
117. Prather, S. L., R. Dagan, J. A. Jenista, and M. A. Menegus.1984. The isolation of enteroviruses from blood: a comparisonof four processing methods. J. Med. Virol. 14:221-227.
118. Prentice, R. L., A. G. Dalgleish, P. A. Gatenby, R. H. Loblay,S. Wade, N. Kappagoda, and A. Basten. 1985. Central nervoussystem echovirus infection in Bruton's x-linked hypogamma-globulinemia. Aust. N. Z. J. Med. 15:443-445.
119. Prober, C. G., and A. M. Arvin. 1987. Perinatal viral infec-tions. Eur. J. Clin. Microbiol. 6:245-261.
120. Pruneda, R. C., and I. Almanza. 1987. Centrifugation-shell vialtechnique for rapid detection of herpes simplex virus cytopath-ic effect in Vero cells. J. Clin. Microbiol. 25:423-424.
121. Rakusan, T. A., and T. Chonmaitree. 1988. Viral meningoen-cephalitis, p. 786-788. In R. E. Rakel (ed.), Conn's currenttherapy. W. B. Saunders Co., Philadelphia.
122. Rantakallio, P., A. L. Saukkonen, U. Krause, and K. Lapin-leimu. 1970. Follow-up study of 17 cases of neonatal coxsackieB5 meningitis and one with suspected myocarditis. Scand. J.Infect. Dis. 2:25-28.
123. Ratzan, K. R. 1985. Viral meningitis. Med. Clin. N. Am. 69:399-413.
124. Ray, C. G., and L. L. Minnich. 1982. Regional diagnosticvirology services: Are satellite laboratories necessary? J. Am.Med. Assoc. 247:1309-1310.
125. Rotbart, H. A., M. J. Levin, and L. P. Villarreal. 1984. Use ofsubgenomic poliovirus DNA hybridization probes to detect themajor subgroups of enteroviruses. J. Clin. Microbiol. 20:1105-1108.
VOL. 2, 1989 13
on February 29, 2020 by guest
http://cmr.asm
.org/D
ownloaded from

14 CHONMAITREE ET AL.
126. Rotbart, H. A., M. J. Levin, L. P. Villarreal, S. M. Tracy, B. L.Semler, and E. Wimmer. 1985. Factors affecting the detectionof enteroviruses in cerebrospinal fluid with coxsackievirus B3and poliovirus 1 cDNA probes. J. Clin. Microbiol. 22:220-224.
127. Rubin, S. J. 1983. Detection of viruses in spinal fluid. Am. J.Med. 75(Suppl. 1B):124-128.
128. Rubin, S. J. 1984. Diagnostic virology laboratory within amicrobiology setting. Yale J. Biol. Med. 57:735-741.
129. Rubin, S. J., and S. Rogers. 1984. Comparison of culture setand primary rabbit kidney cell culture for the detection ofherpes simplex virus. J. Clin. Microbiol. 19:920-922.
130. Schmidt, N. J., H. H. Ho, J. L. Riggs, and E. H. Lennette. 1978.Comparative sensitivity of various cell culture systems forIsolation of viruses from wastewater and fecal samples. Appl.Environ. Microbiol. 36:480-486.
131. Schmidt, N. J., E. H. Lennette, and H. H. Ho. 1974. Anapparently new enterovirus isolated from patients with diseaseof the central nervous system. J. Infect. Dis. 129:304-309.
132. Schmidt, N. J., R. L. Magoffin, and E. H. Lennette. 1973.Association of group B coxsackieviruses with cases of pericar-ditis, myocarditis, or pleurodynia by demonstration of immu-noglobulin M antibody. Infect. Immun. 8:341-348.
133. Scott, T. F. M. 1961. Clinical syndromes associated withenterovirus and reovirus infections. Adv. Virus Res. 8:165-197.
134. Sells, C. J., R. L. Carpenter, and C. G. Ray. 1975. Sequelae ofcentral nervous system enterovirus infections. N. Engl. J.Med. 293:1-4.
135. Shaw, M. 1952. Cultivation of Coxsackie virus in embryonatedeggs and in chick tissue cultures. Proc. Soc. Exp. Biol. Med.79:718-720.
136. Silverstein, A., G. Steinberg, and M. Nathanson. 1972. Nervoussystem involvement in infectious mononucleosis: the heraldingand/or major manifestation. Arch. Neurol. 26:353-358.
137. Singer, J. I., P. R. Maur, J. P. Riley, and P. B. Smith. 1980.Management of central nervous system infections during anepidemic of enteroviral aseptic meningitis. J. Pediatr. 96:559-563.
138. Singh, K. R. P. 1972. Growth of arboviruses in arthropod tissueculture. Adv. Virus Res. 17:187-206.
139. Skoldenberg, B., K. Alestig, L. Burman, A. Forkman, K.Lorgren, R. Norrby, G. Stiernstedt, M. Forsgren, T. Berg-strom, E. Dahlqvist, A. Fryden, K. Norlin, E. Olding-Stenkvist,I. Uhnoo, and K. DeVahl. 1984. Acyclovir versus vidarabine inherpes simplex encephalitis: randomised multicentre study inconsecutive Swedish patients. Lancet ii:707-711.
140. Snider, W. D., D. M. Simpson, S. Nielsen, J. W. M. Gold, C. E.Metroka, and J. B. Dosner. 1983. Neurologic complications ofacquired immune deficiency syndrome: analysis of 50 patients.Ann. Neurol. 14:403-418.
141. Sriram, S., and L. Steinman. 1984. Postinfectious and postvac-cinial encephalomyelitis. Neurol. Clin. 2:341-353.
142. Stalder, H., M. N. Oxman, D. U. Dawson, and M. J. Levin.1973. Herpes simplex meningitis: isolation of herpes simplexvirus type 2 from cerebrospinal fluid. N. Engl. J. Med. 289:1296-1298.
143. Strikas, R. A., L. J. Anderson, and R. A. Parker. 1986.Temporal and geographic patterns of isolates of nonpolioenterovirus in the United States, 1970-1983. J. Infect. Dis. 153:346-351.
144. Swender, P. T., R. J. Shott, and M. L. Williams. 1974. Acommunity and intensive care nursery outbreak of coxsackie-virus B5 meningitis. Am. J. Dis. Child. 127:42-45.
145. Taber, L. H., R. R. Mirkovic, V. Adam, S. S. Ellis, M. D. Yow,and J. L. Melnick. 1973. Rapid diagnosis of enterovirus men-ingitis by immunofluorescent staining of CSF leukocytes. In-tervirology 1:127-134.
146. Tardieu, M., E. Dussaix, P. Lebon, and P. Landrieu. 1986.Etude prospective de 59 meningites virales de l'enfant diagnos-tic clinique et virologique. Epidemiologie et physiopathologie.Arch. Fr. Pediatr. 43:9-14.
147. Thomas, J. E., and F. M. Howard. 1972. Segmental zosterparesis: a disease profile. Neurology 22:459-466.
148. Tracy, S., and A. Latham. 1986. Rapid identification of cox-sackie B viruses after immunoprecipitation and nucleic acidhybridization. Diagn. Microbiol. Infect. Dis. 4:327-333.
149. Webster, A. D. B., J. H. Tripp, A. R. Hayward, A. D. Dayan,R. Doshi, E. H. Macintyre, and D. A. J. Tyrrell. 1978. Echo-virus encephalitis and myositis in primary immunoglobulindeficiency. Arch. Dis. Child. 53:33-37.
150. Wecker, I., and V. terMeulen. 1977. RD cells in the laboratorydiagnosis of enteroviruses. Med. Microbiol. Immunol. 163:233-240.
151. Weiner, L. P., and J. 0. Fleming. 1984. Viral infections of thenervous system. J. Neurosurg. 61:207-224.
152. Weiner, L. S., J. T. Howell, M. P. Langford, G. J. Stanton, S.Baron, R. M. Goldblum, R. A. Lord, and A. S. Goldman. 1979.Effect of specific antibodies on chronic echovirus type 5encephalitis in a patient with hypogammaglobulinemia. J.Infect. Dis. 140:858-863.
153. Wenner, H. A. 1962. Problems in working with enteroviruses.Ann. N.Y. Acad. Sci. 101:343-356.
154. Winter, G. F., J. M. Inglis, and H. A. Cubie. 1987. Rapiddiagnosis of herpes simplex virus infections in conventionaland shell vial cell cultures using monoclonal antibodies. J.Virol. Methods 15:329-330.
155. Whitley, R. J., C. A. Alford, M. S. Hirsch, R. T. Schooley, J. P.Luby, F. Y. Aoki, D. Hanley, and A. J. Nahmias, S. J. Soong,and the NIAID Collaborative Antiviral Study Group. 1986.Vidarabine versus acyclovir therapy in herpes simplex enceph-alitis. N. Engl. J. Med. 314:144-149.
156. Whitley, R. J., S. J. Soong, R. Dolin, G. J. Galasso, L. T.Chien, C. A. Alford, and the Collaborative Study Group. 1977.Adenine arabinoside therapy of biopsy-proved herpes simplexencephalitis: National Institute of Allergy and Infectious Dis-eases collaborative antiviral study. N. Engl. J. Med. 297:289-294.
157. Wildin, S., and T. Chonmaitree. 1987. The importance of thevirology laboratory in the diagnosis and management of viralmeningitis. Am. J. Dis. Child 141:454-457.
158. Wilfert, C. M., R. H. Buckley, T. Mohanakumar, J. F. Griffith,S. L. Katz, J. K. Whisnant, P. A. Eggleston, M. Moore, E.Treadwell, M. N. Oxman, and F. S. Rosen. 1977. Persistent andfatal central-nervous system echovirus infections in patientswith agammaglobulinemia. N. Engl. J. Med. 296:1485-1489.
159. Wilfert, C. M., B. A. Lauer, M. Cohen, M. L. Costenbader, andE. Myers. 1975. An epidemic of echovirus 18 meningitis. J.Infect. Dis. 131:75-78.
160. Wilfert, C. M., S. N. Lehrman, and S. L. Katz. 1983. Entero-viruses and meningitis. Pediatr. Infect. Dis. J. 2:333-341.
161. Wilfert, C. M., R. J. Thompson, T. R. Sunder, A. O'Quinn, J.Zeller, and J. Blacharsh. 1981. Longitudinal assessment ofchildren with enteroviral meningitis during the first threemonths of life. Pediatrics 67:811-815.
162. Wright, P. F., M. H. Hatch, A. G. Kasselberg, S. P. Lowry,W. B. Wadlington, and D. T. Karzon. 1977. Vaccine-associ-ated poliomyelitis in a child with sex-linked agammaglobuline-mia. J. Pediatr. 91:408-412.
163. Wyatt, H. V. 1973. Poliomyelitis in hypogammaglobulinemics.J. Infect. Dis. 128:802-806.
164. Yolken, R. H., and R. J. Leggiadro. 1986. Immunoassays forthe diagnosis of viral enteric pathogens. Diagn. Microbiol.Infect. Dis. 4:61S-69S.
165. Yolken, R. H., and V. M. Torsch. 1981. Enzyme-linked im-munosorbent assay for detection and identification of coxsack-ieviruses A. Infect. Immun. 31:742-750.
166. Yousef, G. E., G. F. Mann, I. N. Brown, and J. F. Mowbray.1987. Clinical and research application of an enterovirus group-reactive monoclonal antibody. Intervirology 28:199-205.
167. Yousef, G. E., G. F. Mann, D. G. Smith, E. J. Bell, V.Murugesan, R. A. McCartney, and J. F. Mowbray. 1988.Chronic enterovirus infection in patients with postviral fatiguesyndrome. Lancet i:146-150.
CLIN. MICROBIOL. REV.
on February 29, 2020 by guest
http://cmr.asm
.org/D
ownloaded from