
Viral Haemorrhagic Fevers Craig Corcoran NHLS Virology, Groote Schuur Hospital.
64
Viral Haemorrhagic Fevers Craig Corcoran NHLS Virology, Groote Schuur Hospital
-
Upload
clinton-golden -
Category
Documents
-
view
218 -
download
0
Transcript of Viral Haemorrhagic Fevers Craig Corcoran NHLS Virology, Groote Schuur Hospital.

Viral Haemorrhagic Fevers
Craig Corcoran
NHLS Virology, Groote Schuur Hospital

VHF- what is it all about?• VHF’s attract the attention of
medical professionals and the general public for a variety of reasons
• They are high on the public mind as they are thought of as highly infectious, killing their victims in a dramatic way
• Mysteries remain as to the source of some of them

“Viral Haemorrhagic Fever”
An acute febrile illness characterized by malaise, myalgia, and prostration dominated by generalized abnormalities of vascular permeability, and regulation. Bleeding manifestations often occur, particularly in severe cases; they are usually diffuse and reflect widespread vascular damage rather than life-threatening volume loss.
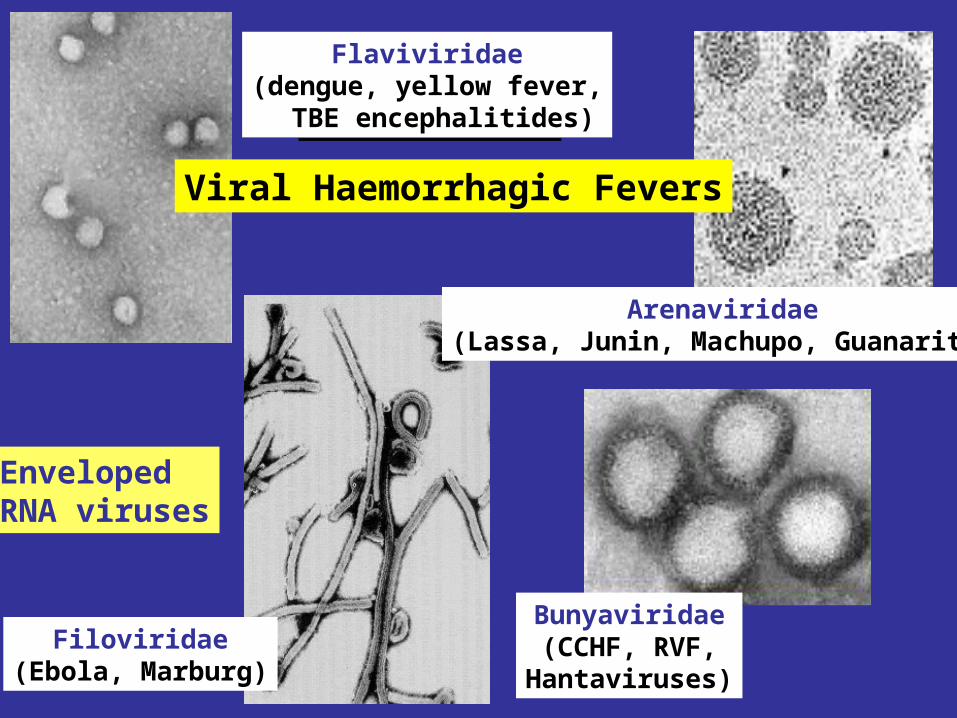
Filoviridae(Ebola, Marburg)
Arenaviridae(Lassa, Junin, Machupo, Guanarito)
Bunyaviridae(CCHF, RVF,
Hantaviruses)
Viral Haemorrhagic Fevers
Flaviviridae(dengue, yellow fever, TBE encephalitides)
EnvelopedRNA viruses

These viruses share a number of features:
• They are all RNA viruses and are enveloped (i.e covered in a fatty (lipid) coating
• Their survival is dependent on an animal or insect host called the natural reservoir
• They are geographically restricted to areas where their host species live
• Humans are not the natural reservoir for any of these viruses. Humans are infected when they come into contact with infected hosts, and with some viruses, can transmit the virus to one another
• Human outbreaks occur sporadically and irregularly. These outbreaks cannot be easily predicted
• With few exceptions, there is no cure or established drug treatment for VHFs

• VHF and other infectious diseases travel quickly nowadays

• Early clinical signs and symptoms may be very discrete and cannot easily be distinguished from those of other illnesses

• Clinical signs and symptoms are easier to interpret once the disease has progressed already

VHF-clinical picture
• Short incubation period• Non-specific onset of illness• Headache, myalgia, arthralgia• Pharyngitis, conjunctival injection/bleed• GIT discomfort/disturbances• Impaired consciousness• Haemorrhages• Proteinuria• Jaundice• Rash, exanthema

VHF-differential diagnosis
• VHF vs. VHF:– clinical picture-unreliable, epidemiology-approximate, laboratory-
proof
• VHF vs. bacterial infections– Typhoid, leptospirosis, tick-bite fever, shigellosis, purulent
pharyngitis, sepsis (streptococcal, staphylococcal, meningococcal), plague
• VHF vs. parasitic diseases– Malaria, african trypanosomiasis, amoebiasis
• VHF vs. viral diseases– Viral hepatitis, herpes simplex

Dengue fever
• Main hosts- non human primates
• Human-to-human transmission through Aedes spp.
• 2.5 billion individuals at risk
• 40-80 million infected each year with thousands of deaths

Dengue-clinical features
• Fever, headache, back pain , chills, musculoskeletal pain, rash, leucopaenia, thrombocytopaenia
• Usually lasts 4-10 days• Dengue haemorrhagic fever/Dengue shock syndrome
– Acute vascular hyperpermeability plus abnormal haemostasis– Rapid deterioration after 2-5 days– Scattered petechiae, ecchymoses, easy bruising/bleeding,
hepatomegaly, epigastric pain
• Pathogenesis: enhancing antibodies- maternal in infants, second infection with a different serotype
• Supportive treatment, vaccine in development

dengue tourniquet test DHF

Yellow Fever
• Historic illness stretching back 400 years
• yellow: jaundice affecting certain patients
• Mosquitos (Aedes and haemogogus) are the true reservoir and vector
• Estimated 200 000 cases/year, 30 000 deaths
• Symptoms vary from mild to severe with haemorrhagic manifestations
Africa and South America only
• ‘acute’ phase- fever, headache, muscle pain, GIT disturbance
• 15% enter a ‘toxic’ phase and rapidly develop jaundice with bleeding manifestations and renal failure. 50% die within 10-14 days
• Supportive treatment• Prevention: vaccine- 17D
live attenuated, safe and highly effective

Filoviruses: Ebola HF
• 1976- Simultaneous large outbreaks in Yambuku (Zaire, now DRC) and Nzara/Maridi (Sudan)
• Originally thought to be one outbreak
• Virology now recognises 2 distinct viruses
• EBO-Z: 318 cases; 88% fatal• EBO-S: 284 cases; 53% fatal

1979, 20041979, 2004
4,0002,000
kilometers
0
DRCDRCDRCDRCDRCDRCDRCDRCDRC(formerly Zaire)(formerly Zaire)(formerly Zaire)(formerly Zaire)(formerly Zaire)(formerly Zaire)(formerly Zaire)(formerly Zaire)(formerly Zaire)
GabonGabonGabonGabonGabonGabonGabonGabonGabon
South AfricaSouth AfricaSouth AfricaSouth AfricaSouth AfricaSouth AfricaSouth AfricaSouth AfricaSouth Africa
UgandaUgandaUgandaUgandaUgandaUgandaUgandaUgandaUganda
SudanSudanSudanSudanSudanSudanSudanSudanSudan
Ivory CoastIvory CoastIvory CoastIvory CoastIvory CoastIvory CoastIvory CoastIvory CoastIvory Coast19941994
1994, 1996, 19961994, 1996, 1996
1976, 19951976, 1995
1996*1996*
20002000
1976, 1979, 1976, 1979, 2004 2004
*Doctor returningfrom Gabon
Ebola Outbreaks
Congo2003


Filoviruses: Marburg HF
• 1967: Marburg, Frankfurt & Belgrade– African green monkeys from Uganda
• 25 primary
• 6 secondary– 1 sexual transmission from husband to wife
85 days after onset of illness, virus cultured from semen
• 7 deaths

Marburg outbreaks

Routes of transmission: filoviruses
• Contact with body fluids of an ill patient– HCW and relatives
• Infected carcasses (handling/cutting of dead primates)
• Needle transfer• Preparation of body for burial• Sexual transmission• Laboratory accident• Aerosol infectivity potential demonstrated
experimentally in monkeys (Ebola)
Reservoir of infection
• Not identified in terrestrial animals or in insects
• Non-human primates suffer but are not the reservoir
• Association with caves and mines make bats suspects for Marburg
• Fruit bats- ? reservoir for Ebola and Marburg (antibodies and RNA found by researchers in Gabon)

Filoviruses: clinical presentation
• 1-2 week incubation• Abrupt onset fever, headache, myalgia• Non-pruritic papular erythematous
eruption becoming large coalescing macules and papules
• Palatal petechiae and haemorrhages• GI symptoms, chest pain, delirium• Sever cases- haemorrhages from
venipuncture sites, mucous membranes and venipuncture sites
• 53-88% case-fatality• ~ 45% hemorrhage• Supportive treatment• Vaccines in development

Marburg blanching maculopapular rash, day 5, Johannesburg 1975

Marburg 2005: 335 cases, 283 deaths

ArenaviridaeArenaviridae
• Arenaviruses associated with human disease
Virus Origin of Name Year Distribution
Lassa Town, Nigeria 1969 West Africa
Junin Town, Argentina 1957 South America
Machupo River, Bolivia 1962 South America
Guanarito Area, Venezuela 1989 South America
Sabia Town, Brazil 1990 South America
LCMV Clinical disease 1933 Worldwide
• Arenaviruses associated with human disease
Virus Origin of Name Year Distribution
Lassa Town, Nigeria 1969 West Africa
Junin Town, Argentina 1957 South America
Machupo River, Bolivia 1962 South America
Guanarito Area, Venezuela 1989 South America
Sabia Town, Brazil 1990 South America
LCMV Clinical disease 1933 Worldwide

Lassa: general facts
• Viral hemorrhagic fever caused by the Arenavirus Lassa
• Transmitted from rodents to humans
• Discovered in Nigeria, 1969
• Endemic in portions of West Africa
• Seasonal clustering: Late rainy and early dry season
• Affects all age groups and both sexes

Lassa virus
“arenosus” (Latin “sandy”)

• Endemic in areas of West Africa, including Nigeria, Liberia, Sierra Leone, and Guinea
• Estimated 300,000-500,000 infections/year, with 5000 deaths
• Rodent-to-human transmission (the “multimammate rat”, Mastomys species-complex)
• Secondary human-to-human transmission with the potential for nosocomial outbreaks with high case-fatality
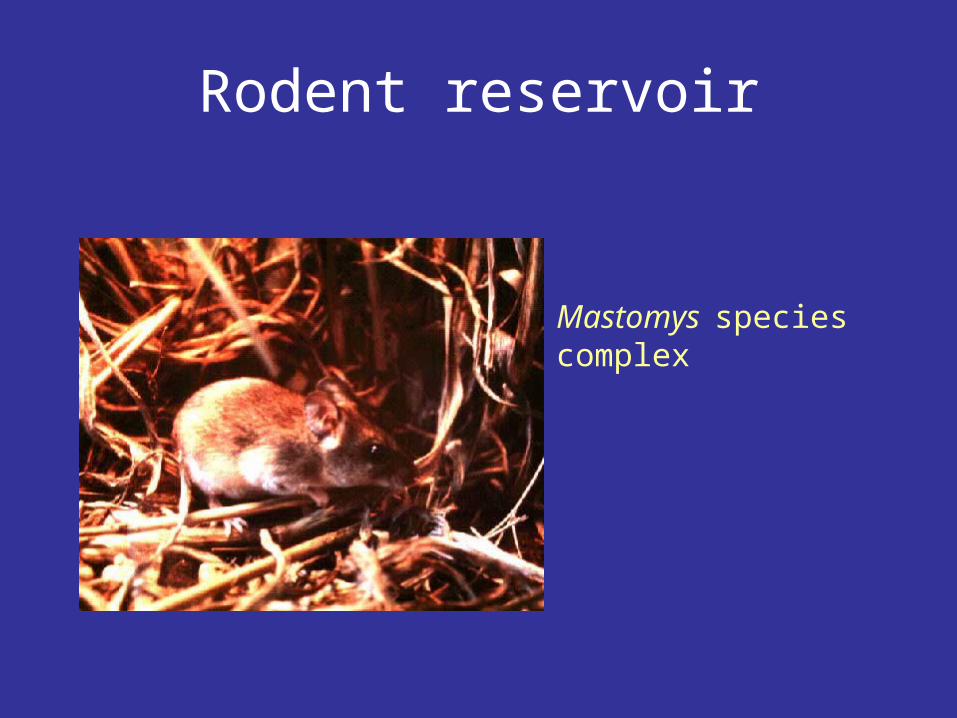
Rodent reservoir
Mastomys species complex

Lassa: Transmission
• Rodent-to-human:
– Inhalation of aerosolized virus
– Ingestion of food or materials contaminated by infected rodent excreta
– Catching and preparing Mastomys as a food source

Lassa: Transmission
• Human-to-human:
– Direct contact with blood, tissues, secretions or excretions of infected humans
– Needlestick or cut
– Inhalation of aerosolized virus– Sex– Breast feeding

Lassa: Clinical Aspects
• 80% asymptomatic• Incubation period of 5-21 days• Gradual onset of fever, headache, malaise and
other non-specific signs and symptoms• Pharyngitis, myalgias, retro-sternal pain, cough and
gastrointestinal symptoms typically seen• A minority present with classic symptoms of
bleeding, neck/facial swelling and shock• Case fatality of hospitalized cases: 15-20%• Particularly severe in pregnant women and their
offspring• Deafness a common sequela

Lassa: Treatment
• Supportive measures
• Ribavirin
– Guanosine nucleoside analog:
blocks viral replication by inhibiting IMP dehydrogenase – Licensed for treatment of RSV and HCV
– Potential adverse effects:
• Dose dependent reversible anemia
• Pancreatitis
• Teratogen in rodents
Crimean-Congo Haemorrhagic Fever

CCHF-some background
• 1944- Crimean peninsula- Crimean haemorrhagic fever (about 200 cases)
• 1956- Belgian Congo- 1 child- Congo Fever• Virus isolated in suckling mice in 1967• 1-10 cases diagnosed annually in South Africa• Case fatality rate 20-25%, 30-50% without proper medical
attention• Mid 1980’s- nosocomial outbreak at TBH- 8 cases, 2 deaths• 27 cases October 1996- Oudtshoorn ostrich abattoir workers

Distribution of CCHF virus

Distribution of the bont-legged ticks in South Africa
•reservoir and vector
Hyalomma marginatum rufipes
Hyalomma marginatum turanicum
Hyalomma truncatum


Hyalommas are two host ticks
- Lavae and nymphs feed on the first host
- Adults feed on the second host
-Cattle
-Sheep
-Goats
-Ostriches

So when are humans at risk?• Bitten by tick/s or crushed tick/s with bare hands• Direct contact with fresh blood or other tissues of
livestock or game animals (ear tagging, castration ect.)
• Direct contact with blood, secretions or excretions of a confirmed or suspected CCHF patient including needlestick injuries
• Resided in or visited a rural environment where contact with livestock or ticks was possible but a specific incident constituting exposure cannot be identified
• NB- incubation period usually 2-7 days hence exposure usually < 7days

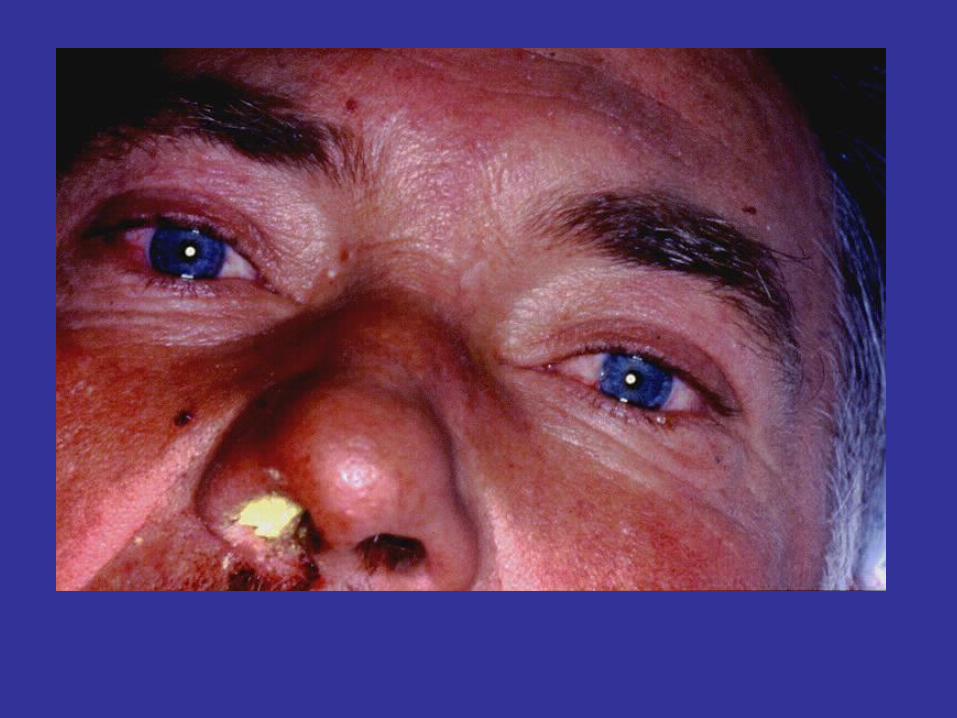
What are the clinical features?
• Sudden onset• Fever ≥ 38ºC on at least one occasion• Severe headache• Myalgia• Nausea and/or vomiting• Pharyngitis, conjunctivitis• Bleeding tendency: petechial rash, ecchymoses,
epistaxis, haematemesis, haematuria or melaena

Skin petechiae

Petechial haemorrhages on the palate

Large ecchymoses


CCHF- laboratory findings
• Leukopaenia or leukocytosis– WCC< 3 x 109/l or ≥ 9 x 109/l
• Thrombocytopaenia– Platelet < 150 x 109/l– Usually < 100 x 109/l
• Abnormal INR and APTT• Transaminitis
– AST ≥ 100iu/l– ALT ≥ 100iu/l

CCHF-differential diagnosis
• Malaria, tick bite fever, disseminated HSV, viral hepatitis, typhoid, rift valley fever, anthrax, brucellosis, Q fever…
• History of exposure, incubation period following exposure, signs and symptoms, laboratory findings

viremia
5
IgM
RT-PCR
ELISA IgM IgG IFA
CCHF : viral/antibody kinetics
Viral isolation
0 10
IgG
16
IgM duration: 2-3 months up to 6 months…

NICD, Johannesburg, BSL-4 (3)Viral detection: (blood specimen)
– RT-PCR (nested)– Cell culture (Vero E6 cells)– Innoculation of newborn mice
Antibody detection : (serum sample)- IFA - ELISA - NT
CCHF : laboratory diagnosisCCHF : laboratory diagnosis

Specific management
Supportive:monitoring of vital functionsblood, fluid replacementtreatment of DIC
Specific:
Ribavirin
?? Immune plasma
Isolation and barrier nursing

PREVENTION OF CCHF
• Ticks most active during Dec, Jan, Feb, March- avoid hiking/camping
• DEET repellents for skin
• Permethrin repellents for clothing –
(0.5% permethrin should be applied to clothing ONLY)
• Check for and remove ticks at least twice daily.
• If a tick attaches, do not injure or rupture the tick.
Remove ticks by grasping mouthparts at the skin surface
using forceps and apply steady traction.

PREVENTION OF CCHF
• Persons working with livestock- wear gloves and other protective clothing to prevent skin contact with infected tissue or blood
• Quarantine and treatment with an ascaricide prior to slaughter (ostriches)

Infection Control

Handling laboratory specimens from patients with suspected or confirmed VHF-non viral
diagnostic specimens
• Common sense- know the risks• Blood and other specimens are highly infectious• Risk of transmission through skin/mucous membrane
contact and needle stick injuries. ?? Respiratory transmission but avoid aerosolisation of specimens
• Limit laboratory testing to what is strictly necessary and where possible run specimens at a time when there is minimal disruption to routine work

• Useful to for two techs to work together- one to process the specimen, other to operate the instrument
• Protective clothing: disposable gown, 2 pairs of gloves, mask and eye protection
• Centrifuge with closed buckets and decontaminate after use
• Open buckets, specimens and load instrument racks in a BSL-2 cabinet
• Discard residual sample and sampling containers into 2% glutaraldehyde or sodium hypochlorite
• Decontaminate instruments according to manufacturers instructions
• Clean BSL-2 cabinet with glutaraldehyde or sodium hypochlorite
• Discard protective clothing, gloves, specimens, ect. Into a biohazard labelled autoclave bag. Double bag and send for autoclaving

• Haematology: – prepare slides in a BSL-2 cabinet, once fixed regard
as non-infectious– Regard air dried slides as infectious, decontaminate
microscope after use• Microbiology:
– protective clothing, process specimens in BSL-2 cabinet, discard residual specimen into 2% glutaraldehyde or sodium hypochlorite
– Process positive blood cultures in a BSL-2 cabinet– Referral of specimens- appropriate packaging, inform
receiving laboratory• Virology:
– Routine specimens- as above– VHF diagnosis- requires BSL 3-4 laboratory


BSL-2 cabinet ?
• provide personnel, environmental and product protection
• Approx 30% air exhausted, 70% re-circulated
A. front openingB. sashC. exhaust HEPA filterD. rear plenumE. supply HEPA filterF. blower

BSL-4 laboratory?• dangerous and exotic agents that
pose a high individual risk of aerosol-transmitted laboratory infections and life-threatening disease
• special engineering and design features to prevent microorganisms from being disseminated into the environment.
• Activities are confined to Class III biological safety cabinets, or Class II biological safety cabinets used with one-piece positive pressure personnel suits ventilated by a life support system.

Laboratory safety: BSL-4
In contrast to patient-care,
high-level protection required for:• Laboratory manipulation• Mechanical generation of aerosols• Concentrated infectious material• Viral culture

THANK YOU…








![INDEX [archive.opengazettes.org.za]...Groote Schuur Hospital (Neurology Department) GSH 21/2008 2008-11-21 307 307 Supply and delivery of various polyester wool and Barathea Broadcloth](https://static.fdocuments.us/doc/165x107/5e3a103e162162507d19ca42/index-groote-schuur-hospital-neurology-department-gsh-212008-2008-11-21.jpg)









