VILMA VELICKAITE - uu.diva-portal.orguu.diva-portal.org/smash/get/diva2:1294312/FULLTEXT01.pdf ·...
64
ACTA UNIVERSITATIS UPSALIENSIS UPPSALA 2019 Digital Comprehensive Summaries of Uppsala Dissertations from the Faculty of Medicine 1546 Analysis of regional atrophy on brain imaging compared with cognitive function in the elderly and in patients with dementia – cross-sectional and longitudinal evaluation VILMA VELICKAITE ISSN 1651-6206 ISBN 978-91-513-0586-8 urn:nbn:se:uu:diva-378578
Transcript of VILMA VELICKAITE - uu.diva-portal.orguu.diva-portal.org/smash/get/diva2:1294312/FULLTEXT01.pdf ·...

ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2019
Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1546
Analysis of regional atrophy onbrain imaging compared withcognitive function in the elderlyand in patients with dementia –cross-sectional and longitudinalevaluation
VILMA VELICKAITE
ISSN 1651-6206ISBN 978-91-513-0586-8urn:nbn:se:uu:diva-378578

Dissertation presented at Uppsala University to be publicly examined in Hedstrandsalen,Akademiska sjukhuset, ingång 70, Uppsala, Thursday, 25 April 2019 at 09:00 for thedegree of Doctor of Philosophy (Faculty of Medicine). The examination will be conductedin English. Faculty examiner: Professor Kathinka Kurz (Stavanger University, Norway).
AbstractVelickaite, V. 2019. Analysis of regional atrophy on brain imaging compared with cognitivefunction in the elderly and in patients with dementia – cross-sectional and longitudinalevaluation. Digital Comprehensive Summaries of Uppsala Dissertations from the Faculty ofMedicine 1546. 63 pp. Uppsala: Acta Universitatis Upsaliensis. ISBN 978-91-513-0586-8.
During aging, brain changes are not homogeneous throughout the entire brain, but are relatedto changes in the morphology of neurons, as well as to changes in the tissue density, and arespecific to each region of the brain. Dementia is a broad category of brain disorders with a setof symptoms including memory, visual-spatial and language problems. Most types of dementiaare slowly progressing, and by the time the person shows signs of the disorder, processes in thebrain are already advanced. Dementia reduces not only the person’s ability to perform everydayactivities, it also increases mortality rates significantly. Because of the increasing incidence ofdementia, possible prevention and treatment of dementia as early as possible are essential.
The aim of the PhD project is to compare a quantitative and qualitative image analysis ofregional cerebral atrophy with cognitive function in the elderly persons.
In paper I, 58 persons participated (84–88 years old) from the ULSAM (Uppsala LongitudinalStudy of Adult Men) cohort. They underwent CT of the brain, cognitive testing and LP. Thisstudy showed that AD biomarkers seem to be less informative in subjects with an advanced age.
In papers II–IV, the cohort included subjects from the PIVUS (Prospective Investigation ofthe Vasculature in Uppsala Seniors) study.
Paper II showed that at age 75, gender and education are confounders for MTA rating.Subjects with abnormal right MTA, but normal MMSE scores had developed worse MMSEscores 5 years later.
Paper III showed that automated rating of MTA could be used in clinical practice to supportthe radiological evaluation. Automated rating of PA and F-GCA should be tested in futurestudies.
In paper IV, we found a mild age-associated decrease in regional brain volumes in this healthycohort with well-preserved cognitive and executive functions.
In conclusion, the included studies in this thesis compare regional atrophy grades in thebrain on CT and MRI and clinical data and provide knowledge that may be used in futureinvestigations that aim to detect dementia in its early stages.
Keywords: Dementia, Brain Imaging, Visual rating, Volumetry, Cognition
Vilma Velickaite, Department of Surgical Sciences, Radiology, Akademiska sjukhuset, UppsalaUniversity, SE-75185 Uppsala, Sweden.
© Vilma Velickaite 2019
ISSN 1651-6206ISBN 978-91-513-0586-8urn:nbn:se:uu:diva-378578 (http://urn.kb.se/resolve?urn=urn:nbn:se:uu:diva-378578)

To all my family


List of Papers
This thesis is based on the following papers, which are referred to in the text by their Roman numerals.
I. Velickaite, V., Giedraitis, V., Ström, K., Alafuzoff, I., Zetterberg, H.,
Lannfelt, L., Kilander, L., Larsson, E-M., Ingelsson M. (2017). Cog-nitive function in very old men does not correlate to biomarkers of Alzheimer’s disease. BMC Geriatrics 17:208.
II. Velickaite, V., Ferreira, D., Cavallin, L., Lind, L., Ahlström, H., Ki-
lander, L., Westman, E., Larsson, E-M. (2018). Medial temporal lobe atrophy ratings in a large 75-year-old population-based cohort: gen-der-corrected and education-corrected normative data. European Ra-diology 28:1739-1747.
III. Velickaite, V., Ferreira, D., Cavallin, L., Lind, L., Ahlström, H., Ki-
lander, L., Westman, E., Larsson, E-M. (2019). Automated ratings and volumetry versus visual ratings of regional brain atrophy in an elderly population. Submitted.
IV. Velickaite, V., Ferreira, D., Lind, L., Ahlström, H., Kilander, L.,
Westman, E., Larsson, E-M. (2019). Visual rating versus volumetry of regional brain atrophy and longitudinal changes over a 5-year pe-riod in an elderly population. Manuscript.
Reprints were made with permission from the respective publishers.


Contents
Introduction ...............................................................................................13The aging brain .....................................................................................13Dementia ..............................................................................................13Diagnostics ...........................................................................................14
Cognitive testing ...............................................................................15Laboratory tests ................................................................................16Neuropathology ................................................................................16
Neuroimaging .......................................................................................17Morphological imaging .....................................................................17Evaluation of CT and MRI ................................................................18Metabolic imaging ............................................................................22Artificial intelligence ........................................................................23
Aims .........................................................................................................24General aim ..........................................................................................24Specific aims.........................................................................................24
Paper I ..............................................................................................24Paper II .............................................................................................24Paper III ...........................................................................................24Paper IV ...........................................................................................24
Methods ....................................................................................................25Paper I ..................................................................................................25
Subjects and methods .......................................................................25CT evaluation ...................................................................................25
Paper II .................................................................................................26Subjects and methods .......................................................................26MR protocol and evaluation ..............................................................26
Paper III ................................................................................................27Participants and MRI examinations ...................................................27Visual ratings of regional brain atrophy ............................................27Automated rating of atrophy and volumetric analysis ........................27
Paper IV................................................................................................28Participants .......................................................................................28MRI and visual ratings of regional brain atrophy ...............................28Volumetric analysis ..........................................................................28

Statistical analysis .....................................................................................29Paper I ..................................................................................................29Paper II .................................................................................................29Paper III ................................................................................................29Paper IV................................................................................................30
Results ......................................................................................................31Paper I ..................................................................................................31Paper II .................................................................................................34
Influence of gender and education on the MTA measures ..................35Normative data and cut-offs for MTA measures by gender and education ..........................................................................................36Clinical associations between MTA grade and cognitive tests at baseline and after 5 years ..................................................................36
Paper III ................................................................................................37Intra-rater and inter-rater reliability for visual rating .........................37Computed rating with cNeuroÒ versus visual rating .........................37Volumetry versus visual ratings ........................................................38Association between computed ratings, visual ratings and cognition..38
Paper IV................................................................................................39Visual atrophy rating and volumetry at baseline and after 5 years ......39Visual ratings versus volumetry ........................................................40Association between visual ratings, volumetry and cognition ............41
Discussion .................................................................................................42Paper I ..................................................................................................42Paper II .................................................................................................43Paper III ................................................................................................45Paper IV................................................................................................47
Conclusions ...............................................................................................50Paper I ..................................................................................................50Paper II .................................................................................................50Paper III ................................................................................................50Paper IV................................................................................................50
Future perspectives ....................................................................................51General perspectives .............................................................................51Specific perspectives .............................................................................51
Sammanfattning på svenska .......................................................................52Analys av regional atrofi vid hjärnavbildning jämfört med kognitiv funktion hos äldre och hos patienter med demens - tvärsnitts- och longitudinell utvärdering. ......................................................................52Resultat .................................................................................................53

Artikel 1 ...........................................................................................53Artikel 2 ...........................................................................................53Artikel 3 ...........................................................................................53Artikel 4 ...........................................................................................53
Acknowledgments .....................................................................................55
References .................................................................................................57

Abbreviations
Aβ42 Amyloid beta 42 protein AD Alzheimer’s Disease asyn alfasynuclein ASL Arterial Spin Labelling BTO Benton Temporal Orientation test CD Clock Drawing test CT Computed Tomography CSF Cerebrospinal Fluid DICOM Digital Imaging and Imaging in Medicine ECRT Enhanced Cued Recall Test FDG-PET Fluorodeoxyglucose Positron Emission Tomography F-GCA Frontal Global Cortical Atrophy FLAIR Fluid Attenuated Inversion Recovery FTD Frontotemporal Dementia GBD Global Burden of Diseases ICV Intracranial Volume LBD Lewy Body Dementia LP Lumbar Puncture MCI Mild Cognitive Impairment MI Myocardial Infarction MMSE Mini-Mental State Examination MPR Multi-Planar Reconstruction MRI Magnetic Resonance Imaging MTA Medial Temporal Lobe Atrophy NIA-AA National Institute of Aging and Alzheimer’s Association PA Posterior Atrophy PACS Picture Archiving and Communication System PET Positron Emission Tomography PIB Pittsburgh Compound B PIVUS Prospective Investigation of the Vasculature in Uppsala
Seniors p-tau phosphorylated tau protein QMRI Quantitative Magnetic Resonance Imaging SF Semantic Fluency SWI Susceptibility Weighted Imaging TMT Trail Making Test

t-tau total tau protein ULSAM Uppsala Longitudinal Study of Adult Men VBM Voxel-based morphometry


13
Introduction
The aging brain “Successful aging” is a physiological process that develops without concur-rent diseases [1]. During aging, the volume (or weight) of the brain decreases at a rate of around 5% per decade after age 40 years and at an increasing rate over the age of 70. Brain changes are not homogeneous throughout the entire brain, but are related to changes in the morphology of neurons, as well as to changes in the tissue density, and are specific to each region of the brain. Vol-ume changes normally begin in the prefrontal cortex followed by the temporal lobe, cerebellar structures and hippocampus. The occipital lobes seem to be least affected [2; 3].
Cortical thickness and subcortical volume decrease by 0.5–1% per year [3]. Hippocampus volume decreases around 1% per year in normal aging, assessed on imaging. In patients with Alzheimer’s disease (AD), this volume decrease is 4% per year [3; 4]. Atrophy of the hippocampus increases significantly after age 72 years [5].
These non-uniform changes in brain volume fit well with cognitive changes seen in aging, although some studies suggest that aging has the most pro-nounced effect on the hippocampus [2]. Reduction in specific cognitive abili-ties, such as executive functions and episodic memory, is also seen in healthy aging [3].
Dementia Dementia can be caused by a broad category of brain disorders that encompass a set of symptoms which include memory, visual-spatial and language prob-lems. Most types of dementia are slowly progressive, and by the time the per-son shows signs of the disorder, processes in the brain are already advanced. Dementia reduces not only the person’s ability to perform everyday activities, but can also cause changes in mood or behavior.
Dementia is not a specific disease. Many diseases can cause dementia, such as normal pressure hydrocephalus, brain tumors or even chronic subdural he-matomas.

14
Alzheimer's disease, Lewy body dementia (LBD) and frontotemporal de-mentia (FTD) are primary neurodegenerative disorders. Vascular dementia is usually due to extensive small vessel disease. Patients with Creutzfeldt-Jakob disease, Parkinson’s disease and Huntington’s disease may also develop de-mentia. These conditions can have similar and overlapping symptoms. How-ever, Alzheimer’s disease is the most common dementia disorder (60–80% of all cases).
Dementia is a constantly growing burden for the patient, the relatives and also for society. In 2005, it was estimated that 24.3 million people had demen-tia, with 4.6 million new cases every year (one new diagnosed case every 7 seconds) worldwide. It is calculated that this number will double every 20 years to 81.1 million by 2040 [6]. According to the Global Burden of Diseases (GBD)] for 2003, dementia contributed to 11.2% of years lived with disability in people older than 60 years. That is more than stroke, cardiovascular diseases and all types of cancer. With a growing percentage of older persons, especially in the more developed countries, this social and financial burden can be diffi-cult to manage.
The incidence of dementia increases significantly with age, affecting 5% of the population older than 65 and 20–40% of those older than 85.
Presently, there is no ultimate cure for dementia. During the last 10 years, a huge amount of research and many financial and social resources have been directed towards finding medication to alleviate symptoms and prevent de-cline of cognitive functions in patients with early dementia. During the last years, some new drugs came on the market with the potential to decrease/delay the symptoms of dementia.
Dementia causes not only disability, it also increases mortality rates signif-icantly. In 2013, dementia resulted in about 1.7 million deaths, compared with 0.8 million in 1990 [7].
These growing number of elderly people and the increasing incidence of dementia make early diagnosis, possible prevention and treatment of dementia as early as possible essential.
Diagnostics The diagnostics of dementia disorders is complex. In the first National Insti-tute of Neurological Disorders and Stroke-Alzheimer Disease and Related Disorders ( NINDS-ADRDA) criteria, published in 1984, the diagnosis of AD required that the presence of cognitive impairment was confirmed by neuro-psychological testing for a clinical diagnosis, and histopathologic confirma-tion was required for the definitive diagnosis [8]. Since then, understanding of the disease has advanced greatly, together with the diagnostic possibilities, which now include not only cognitive testing and post-mortem

15
histopathology. Recognized in vivo biomarkers of the disease include struc-tural changes in the brain, visible on imaging, usually computed tomography (CT) or magnetic resonance imaging (MRI), metabolic changes shown by pos-itron emission tomography (PET) and cerebrospinal fluid (CSF) biomarkers [9-11].
Cognitive testing There are some brief tests (5–15 minutes) that have reasonable reliability to screen for dementia.
Presently, the Mini Mental State Examination (MMSE) is the best studied and most commonly used screening method for the diagnosis of dementia [12].
Originally, MMSE was developed by Folstein in 1975 for psychiatric pa-tients. Later, based on this test, the presently used version was developed. The MMSE is a useful tool to support the diagnosis of dementia if the results are interpreted along with an assessment of a person’s personality, their ability to perform activities of daily living, and their behavior. The test itself is easy to administer, does not require special education or training for administration, although results can be affected by age and education. It includes simple ques-tions, such as the time and place of the test, repeating lists of words, arithmetic, language use and comprehension, basic motor skills, for example, copy a drawing of two interlocking pentagons. The maximum score is 30 points. Any score higher than 23 points indicates normal cognition. Below this level, scores can indicate severe (≤9 points), moderate (10–18 points) or mild (19–23 points) cognitive impairment. Although the maximal score of 30 points can never rule out dementia. Also, it was noted, that the test lacks sensitivity to mild cognitive impairment and fails to discriminate patients with mild AD from normal patients.
Another widely used screening test is the 7 Minute Neurocognitive Battery, which consists of four brief tests: Enhanced Cued Recall Test ( ECRT), tem-poral (or Benton) orientation (BTO), verbal (semantic) fluency (SF), and clock drawing (CD). In enhanced cued recall, the person has to identify 16 pictures, which are recalled immediately or after a brief interval. In the tem-poral orientation test, the orientation in time (year, month, date, day of the week) is measured and quantified in degree of error. During verbal fluency testing, the person has to name as many different animals as possible during 1 minute. The clock drawing test is a widely used cognitive test, where the sub-ject has to draw the face of a clock and place the hands at a fixed time. This test appears to be highly sensitive to AD [13]. The measured value is the time it took for individuals to complete this test. For persons with AD it takes a longer time than for subjects without or with mild cognitive decline [13; 14].

16
Another test used for detecting cognition disabilities is the Trail Making Test (TMT) A and B [15]. The TMT provides information on visual search, scanning, speed of processing, mental flexibility, and executive functions. Originally, it was part of the Army Individual Test Battery (1944) and sub-sequently was incorporated into the Halstead–Reitan Battery. The TMT con-sists of two parts. TMT-A requires an individual to draw lines sequentially connecting 25 encircled numbers distributed on a sheet of paper. Task require-ments are similar for TMT-B except the person must alternate between num-bers and letters (e.g., 1, A; 2, B; 3, C etc.). The score on each part represents the amount of time required to complete the task [16].
Laboratory tests Other diagnostic biomarkers of dementia are concentrations of Aβ42, total tau (t-tau) and phosphorylated tau (p-tau) in CSF. These proteins are associated with intracerebral deposition of neuritic plaques (amyloid) and reflect neu-ronal degeneration, caused by intraneuronal accumulation of neurofibrillary tangles, containing tau proteins. These changes are eventually accompanied by the damage and death of neurons. For example, in patients suffering from AD, CSF analysis shows low amyloid Aβ42 concentrations, increased t-tau or p-tau concentrations or a combination of all three findings [10].
Reduced CSF levels of Aβ42 peptides are believed to result from accumu-lation of this protein into insoluble plaques in the AD brain. Increased levels of tau proteins are thought to occur after their release from damaged and dying neurons containing dystrophic tau neurites and tangles.
The use of CSF biomarkers has been of great importance to identify sub-jects with mild cognitive impairment (MCI) that subsequently will convert to AD [17]. Although the combination of CSF Aβ42, t-tau and p-tau helps to differentiate AD from healthy controls with reasonable accuracy, the concen-tration of these CSF biomarkers overlaps between groups. Also, these markers are not suitable for monitoring clinical progression as they remain relatively stable throughout the disease process [18]. Moreover, it has been observed that the predictive and diagnostic value of CSF markers is limited in older populations, where a substantial part of the apparently cognitively healthy subjects has an AD CSF profile of decreased Aβ42 combined with increased levels of t-tau and p-tau [19; 20].
Neuropathology Amyloid-β (Aβ) plaques and neurofibrillary tangles of tau proteins are found in widespread areas of the post mortem brain. The hallmark of Alzheimer’s disease is the progressive accumulation of the protein fragment beta amyloid (plaques) outside neurons in the brain and twisted strands of the protein tau

17
(tangles) inside neurons [21; 22]. The distribution of amyloid-β (Aβ) plaques in the different areas of the brain is defined by Thal staging and the distribution of neurofibrillary tangles by Braak staging. Although some cognitively intact elderly subjects may display abundant protein deposition or cerebrovascular lesions at autopsy, a subgroup of patients with cognitive dysfunction may show a relatively mild neuropathology [23-28].
Some other entities, such as synuclein (a-syn), a soluble protein primarily expressed in neural tissue, are also noted in brains affected by dementia. Lev-els of a-synuclein are found to be higher in AD brains and correlate better with cognitive impairment than other proteins.
Neuroimaging In 2011, new NINCDS-ADRDA criteria were accepted; this time both CSF analyses and neuroimaging were included as supportive tools for criteria for probable AD.
The presence of volume loss in the hippocampi and entorhinal cortex on MRI has become a new feature in clinical dementia diagnostics. Specific pat-terns on functional imaging with PET is another possible criterion of dementia [9].
Morphological imaging In the modern clinical work-up of dementia, CT and MRI are used not only to exclude secondary causes of dementia, but also to detect patterns of atrophy that may be specific for different neurodegenerative diseases [29].
CT of the brain is included in the basic evaluation of patients with suspected dementia in Sweden. Examination of the brain with multidetector CT with thin slices and reconstructions in three planes (transverse, coronal, sagittal) is a faster, more widely available and cheaper method than MRI. The radiation dose for brain CT is small and is not a problem for elderly individuals.
MRI as an examination method is used in hospitals and centers with better MR scanner availability. MRI is more expensive and not so widely available and has longer scan time that CT, which can be problematic for persons with dementia. Different magnetic field strengths of MRI scanners can affect the interpretation, especially with regard to comparison of studies in longitudinal follow-up. Recommended sequences in Sweden are a T1-weighted 3D se-quence to assess structural changes, a T2-weighted fluid-attenuated inversion recovery (FLAIR), and a T2-weighted turbo spin echo sequence to detect other pathological changes, primarily white matter changes. T1-weighted 3D se-quences can be used not only for multiplanar reconstruction, but also, when downloaded to various software packages, for volumetry of different parts of

18
brain. Extra sequences, such as susceptibility weighted imaging (SWI) for de-tecting microbleeds, often seen in small-vessel disease as cause of dementia, can be included [29]. New sequences, such as arterial spin labeling (ASL), which can measure blood flow in the brain in neurodegenerative diseases without contrast agent injection, can be added. Initial data suggest that ASL may provide information similar to that provided by FDG-PET and can be-come a time-saving and radiation-free alternative in dementia diagnostics [30].
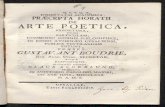
Evaluation of CT and MRI Visual assessment The grade of medial temporal lobe atrophy (MTA) is assessed using the es-tablished Scheltens scale, which is based on widening of the choroid fissure and temporal horn of lateral ventricle and loss of hippocampal volume. This scale is based on the evaluation of coronal images of the brain and has five grades (0 to 4). The evaluation criteria comprise the width of the choroid fis-sure, the width of the temporal horn and the height of the hippocampus [31]. Score 0 refers to no atrophy, score 1 shows widening of the choroid fissure, score 2 includes additional widening of the temporal horn of the lateral ven-tricle and slightly decreased hippocampal height, score 3 includes moderate loss of hippocampal volume, and 4 shows end-stage progression of all these findings (Fig. 1). It is based on MRI, but later it has been shown that the scor-ing can also be used in CT imaging if image quality is high and reconstructions are of sufficient quality, which is possible with the new multidetector CT scan-ners [32].

19
Figure 1. Medial temporal lobe atrophy (MTA) grade 0–4 according to Scheltens scale (images from our PIVUS cohort).
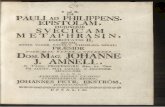
Later, other scales for evaluation of atrophy in posterior lobes (Koedam) or globally (Pasquier) have been developed [33; 34]. These scales have fewer steps (grades 0–3) and are based on the appearance of sulci in different parts of the brain. Grade 0 shows closed sulci, grade 1 opening/mild widening of sulci, grade 2 substantial widening of the sulci and grade 3 extreme widening of the sulci/ “knife blade” appearance of gyri (Fig. 2). These scales are not as widely known as the Scheltens scale, but are increasingly used for dementia evaluation, both in research and clinically.

20
Figure 2. Frontal cortical atrophy (F-GCA) and posterior atrophy (PA) grades 0–3 according to Pasquier and Koedam scales (images from our PIVUS cohort
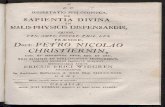
Volumetry Age-related atrophy of the brain and related enlargement of CSF spaces are present in normal old men and women [35]. Numerous cross-sectional studies with atrophy grading scales have shown correlation between age, atrophy grades and different kinds of dementia. These rating scales have several dis-advantages. Variation that exists in brain morphology affects the grading, and the grading is also very operator dependent, especially because it depends on the operator’s years of experience [36]. Volumetry of the brain can help to solve these issues. Volumetry is based on segmentation of different parts of the brain and calculation of volumes and loss during a specified time period. Separate parts of the brain can be measured, total brain parenchymal volume, separately grey matter volume or white matter volume, because it is based on dividing the brain into different parts, based, for example, on gyral patterns, such as described by Destrieux, Desikan–Killiany [37; 38]. These methods require additional software, few of the most popular being SPM and Free-Surfer [39]. These software programs allow normalization of structural vol-ume changes with intracranial volume (ICV), which reduces gender bias, premorbid brain size and inter-individual variations of head size (Fig. 3).

21
Figure 3. Morphological MRI image (a) and volumetric images from FreeSurfer (b) and cNeuro (c) softwares (images from our PIVUS cohort).
Other possible methods of volumetry are now included in clinically approved software packages, such as in synthetic MRI [40; 41].
In the early days of volumetry, manual methods of segmentation were used and were therefore very time and labor craving. These were the main reasons for volumetry not finding its way into clinical practice. Now, when automatic volumetry methods are developing very rapidly, we see more possibilities for implementing them into clinical practice, not only for measuring volumes of the brain lobes, but also in other clinical conditions, such as measuring volume of nodular changes in lungs or the burden of demyelinating plaques in the brain [42; 43]. A few software programs for automated volumetry of, e.g., the hippocampus, including comparison to a normal database, have recently been approved for clinical use, and brain images can be sent to different companies for evaluation on fee-for-service basis.
In several studies, it has been shown that the visual atrophy scale is com-parable with volumetric methods and is simpler and quicker to use in clinical practice [44-46].
There is now also software which allows us not only to perform volumetric measurements of the separate parts of the brain, but also to calculate/compute atrophy grades, which is more appropriate in clinical practice and comparable with known normal or pathological grades. It also allows, with input of known clinical data, possible diagnostic suggestions. This use of artificial intelligence (AI) can help us in the future to alleviate clinical work and to provide better reproducibility. This software, which is cleared by both the FDA and Euro-pean Medical Device Directive 93/42/EEC, is available commercially in Eu-rope for clinical use.

22
Metabolic imaging Molecular imaging techniques, such as positron emission tomography (PET), play now an important role in the work-up of dementia. FDG-PET is based on cortical glucose metabolism, which correlates to neuronal and synaptic activ-ity. 18F-FDG is a glucose analogue with the positron-emitting fluorine-18 substituted for one of the hydroxyl groups. It is distributed similar to glucose in the body and is taken up by cells with high glucose consumption. When intracellular, the molecule will be phosphorylated but not metabolized. During its incarceration in the cell, it will eventually emit the positron, with a half-life of 110 minutes. Thus, the PET scanner can trace the presence and location of tissues with high levels of glucose consumption.
FDG-PET is a robust and commonly used method, and is included in the criteria for diagnosis of AD, where it shows reduced glucose metabolism in the bilateral temporal and parietal regions that is characteristic for the disease. Patterns of focally reduced glucose consumption can reveal areas afflicted by neurodegenerative disease earlier than atrophy can be detected [47; 48]. The positive finding of impaired glucose metabolism has become an important di-agnostic supportive feature of the dementia work-up, and is often an important support for the clinician in differential diagnostics of patients with early and unspecific symptoms [9].
Other metabolites, such as Pittsburgh compound B (PiB), which shows am-yloid deposition, can also be used for diagnostics [49]. In patients with de-mentia, amyloid PET is recognized as a tool to differentiate AD, where amy-loid deposition is prominent, from frontotemporal dementia (FTD), where am-yloid deposition is much lower.
One of the most recent advances with regard to in vivo PET imaging is evaluation of the cerebral tau burden, which shows the relationship between tau burden and synaptic dysfunction, grey matter atrophy and cognitive defi-cits. Some studies show that tau PET was able to replicate neuropathological Braak staging, so it can be valuable for the in vivo staging of AD [50].
PET/MR or PET/CT scanners with simultaneous acquisition of both mo-dalities are also promising techniques for use in the clinical setting.
Evaluation of metabolic imaging Visual assessment of FDG-PET images for detecting neurodegenerative dis-ease is facilitated by the use of statistical mapping tools that show cortical areas with statistically reduced glucose metabolism in comparison with the findings in a cohort of healthy controls. There are several commercially avail-able software programs for this (e.g. BRASS, Cortex ID). The software con-ducts a spatial normalization of the patient’s images and highlights areas with reduced metabolism levels.

23
If amyloid or tau is looked for, PET maps with increased burden are used for evaluation.
One of the software programs, 3D-SSP, is used clinically for both FDG and amyloid imaging, and method optimization is ongoing [51]. However, there is still no commercially available software adapted for perfusion evaluation in suspected dementia.
Artificial intelligence Artificial intelligence in radiology was discussed already decades ago [52]. In radiology practice, trained radiologists visually assess medical images for the detection, characterization and monitoring of diseases. Radiological imaging data continue to grow at a disproportionate rate when compared with the num-ber of available trained readers. This has contributed to a dramatic increase in radiologists’ workloads. Studies report that, in some cases, an average radiol-ogist must interpret one image every 3–4 seconds in an 8-hour workday to meet workload demands [53]. With this workload, errors are inevitable.
An AI component within the imaging workflow would increase efficiency, reduce errors and achieve objectives with minimal manual input by providing trained radiologists with pre-screened images and identified features.
AI methods can help us automatically recognize complex patterns in imag-ing data and provide quantitative, rather than qualitative, assessments of radi-ographic characteristics [54].
The endpoint for now of AI in radiology is the so-called “end-to-end” so-lution, in which images are used as input, and the output is a draft radiology report encompassing all the salient features of the image that an expert radiol-ogist would include [55].

24
Aims
General aim The general aim of the thesis was to compare quantitative and qualitative find-ings of image analysis of regional cerebral atrophy and compare them with cognitive function in the elderly and in patients with early dementia.
Specific aims Paper I The aim of this study was to relate cognitive performance to the degree of brain atrophy on CT, CSF biomarker levels and neuropathology in a cohort of elderly men.
Paper II The aim of this study was to find cut-off values for different medial temporal lobe atrophy (MTA) measures (right, left, average, and highest) on MRI, ac-counting for gender and education, investigate their association with cognitive performance, and to compare them with decline of cognitive function over 5 years in a population-based cohort.
Paper III The aim of this paper was to investigate whether automated, computer-based rating and volumetry are comparable with visual rating of regional brain atro-phy and to study the association of atrophy ratings with cognitive test scores.
Paper IV Objectives of this paper were to compare visual rating and volumetry for as-sessment of regional brain atrophy in an elderly population over a 5-year pe-riod and to compare these parameters with cognitive test results.

25
Methods
Paper I Subjects and methods ULSAM represents a longitudinal epidemiological study based on all availa-ble men born 1920–1924 living in Uppsala County, Sweden, in the beginning of the 1970s. Full screening and official registry data are available in database (http://www.pubcare.uu.se/ulsam).
A total of 160 ULSAM individuals were invited to take part in the present study. Fifty-eight individuals (84–88 years old) agreed to participate. They underwent CT of the brain and cognitive testing by MMSE. Of these, 12 were diagnosed with AD or unspecified dementia, either at baseline (n = 4) or dur-ing the following 4 years (n = 8). In addition, for all subjects, ECRT data were available from the recently concluded examination of the 84-88-year-olds in the remaining cohort.
Fifty-two of the 58 subjects accepted to undergo LP, although investiga-tions could only be completed in 35. All 58 subjects were asked for a post mortem brain donation, and 24 of them gave their informed consent. Of these, 13 brains came to autopsy.
CT evaluation The CT images were independently reviewed by two neuroradiologists with regard to degree of medial temporal lobe atrophy (MTA), posterior atrophy (PA) and frontal atrophy (fGCA) [31; 33; 34]. Also, white matter changes and the presence of lacunar or cortical infarcts were defined. If the neuroradiolo-gists could not agree on a score, a consensus evaluation was made to reach the final scoring results.

26
Paper II Subjects and methods The Prospective Investigation of the Vasculature in Uppsala Seniors (PIVUS) is a population-based study of 1016 individuals recruited at age 70 years [56; 57]. The subjects were included randomly from the population register of the municipality, and previous or current diseases were not exclusion criteria. MRI of the brain was undertaken in 406 of these subjects (randomly selected) 5 years later, at age 75 years.
Cognitive evaluation of individuals at age 75 years was done with the Mini-Mental State Examination (MMSE), the 7 Minute Screening Battery, includ-ing Benton temporal orientation (BTO), enhanced cued recall test (ECRT) of 16 items, clock drawing test (CD), and semantic verbal fluency (SF), (animals per 1 min), and the Trail Making Test A and B (TMT- A and TMT-B) [12; 15]. None of the individuals had a diagnosis of dementia at the time of inclu-sion.
Subjects were stratified into two groups based on the level of education (up to 8 years of education was regarded as low education and 9 years or more as high education).
Only subjects with an available brain MRI and information about educa-tional level (390 individuals) were included in this study.
MR protocol and evaluation MRI of the brain was performed with a 1.5 T MR scanner (Intera, Philips Healthcare, Best, the Netherlands). A sagittal T1-weighted 3D gradient echo sequence (echo time 4.0 ms, repetition time 8.6 ms, flip angle 8°, resolution 0.94x0.94x1.2 mm and matrix 256x256x170) was interactively reconstructed to 1.2 mm thick images in a Picture Archiving and Communication System (VuePACS, Carestream; Carestream Health, Inc., Rochester, NY, USA) for visual assessment.
One operator (VV) using the Scheltens scale performed the visual rating. Randomly selected individuals (n = 50) were rated by a second operator (LC), and inter-rater reliability was calculated. Also, randomly selected individuals (n = 20) were rated again by the first operator (VV) and intra-rater reliability was calculated. Four scores were investigated in the current study: right and left sides MTA separately, average MTA and MTA highest (highest out of left and right score when they were different).

27
Paper III Participants and MRI examinations The same participants from the PIVUS cohort described in paper II were in-cluded in this study. As previously, we used MRI images of the brain obtained in 406 of these subjects (randomly selected) at age 75 years.
Visual ratings of regional brain atrophy One experienced neuroradiologist (VV) performed the visual rating of all sub-jects. For MTA rating, the Scheltens scale was used. For rating of parietal atrophy (PA) the Koedam and for frontal atrophy (F-GCA) the Pasquier scales were used.
Randomly selected subjects (n = 40) were rated twice by the same neuro-radiologist (VV) for studying intra-rater reliability. Also, 100 of randomly se-lected subjects were also rated by a second experienced neuroradiologist (LC) for studying inter-rater reliability.
Four scores were investigated in the current study: right and left MTA sep-arately, and PA and F-GCA total scores.
Automated rating of atrophy and volumetric analysis Automated rating of regional brain atrophy and volumetric analysis were per-formed with the cNeuroÒ (Combinostics Oy, Tampere, Finland) software package.
After visual evaluation and rating of atrophy in different brain regions in a clinical PACS system, all raw DICOM data images were uploaded to the cNeuroÒ program. After processing, the output table, which included com-puted ratings of regional brain atrophy and volumetric information, was pre-sented. All output images were inspected for errors by an experienced neuro-radiologist (VV). Images with processing errors were discarded.
Output of the volumetric analysis from cNeuroÒ included the volumes of hippocampus on the right and left sides separately, and the volumes of parietal and frontal lobes. We then normalized all selected volumes by dividing the region of interest by the total intracranial volume estimation from cNeuroÒ.
Totally, 318 subjects were included in the study.

28
Paper IV Participants Participants in this study included the same subjects as in paper III. MRI of the brain was repeated in 252 subjects who returned for a 5-year follow-up examination at age 80.
Cognitive evaluation of subjects at this age was performed both at age 75 and age 80 using the MMSE, TMT-A and TMT-B. All medical records were screened in order to identify subjects with diagnosed mild cognitive impair-ment or dementia disorders at baseline and follow-up.
MRI and visual ratings of regional brain atrophy MRI of the brain was performed as in study III.
One experienced neuroradiologist performed the visual ratings. Scans per-formed at age 75 were rated first. Then, the images obtained in the 80-year-olds were rated together with images and ratings obtained at age 75 for com-parison, like in a clinical context.
Volumetric analysis Volumetric analysis was performed with FreeSurferÒ (version 6.0.0).
All raw T1-weighted DICOM data images were uploaded to the Free-SurferÒ program, which processed and analyzed the data as fully detailed elsewhere [58; 59]. All output images were inspected for errors by an experi-enced neuroradiologist (VV). All volumes selected for further analysis were normalized by dividing the region of interest by the total intracranial volume estimation.

29
Statistical analysis
Paper I For the comparison between groups, the Mann–Whitney U test or Kruskal–Wallis ANOVA was used. All statistical analyses were performed with STA-TISTICA v13. Levels of quantitative variables are presented as mean ± SD or median and range. Two-tailed values of p < 0.05 were considered statistically significant.
Paper II Kendall rank and Spearman’s rank correlations were used to investigate asso-ciations between variables. Mann–Whitney U and Kruskal–Wallis tests were used for group comparisons, and one-way ANCOVA was used for group com-parisons while accounting for the effect of gender and education. The chi-squared test was used for categorical variables. Multiple linear regression and ordinal regression were used to investigate the effect of gender and education and their interaction on the different MTA measures. Mixed ANCOVA was used to test the interaction between a within-subjects factor and a between-subjects factor while accounting for the effect of gender and education. Inter-rater and intra-rater reliability were assessed with the weighted Kappa test [60]. All the results were considered significant when p ≤ 0.05.
Paper III Intra- and inter-rater reliability were assessed with the weighted Kappa test [60].
Spearman’s rank, Pearson’s and point-biserial correlations were used to in-vestigate associations between variables. To investigate differences between correlation coefficients, the correlation coefficients were inverted when nec-essary, and the Fisher’s r-to-z transformation test was performed. These re-sults were considered significant when p ≤ 0.05 (one-tailed).
To investigate correlations between automated ratings and ECRT-free, ECRT-cued and the SF tests, Pearson’s test was used. For other correlations we used Spearman test. p-values in the cognitive correlations were adjusted

30
with the Hochberg correction for multiple comparisons. Correlation results were considered significant when p ≤ 0.05 (two-tailed).
Paper IV Spearman’s rank and point-biserial correlations were used to investigate asso-ciations between variables.
Correlation results were considered significant when p ≤ 0.05 (two-tailed). Wilcoxon test and the paired t-test were used to analyze changes in atrophy
ratings and volume over the time. A repeated measures ANOVA was used to test the interaction between
changes in atrophy rating and volumetry with changes in cognitive tests re-sults.

31
Results
Paper I The median MMSE score was 28 for the whole group (25.5 for those who already had or were subsequently given a dementia diagnosis and 28 for those without a dementia diagnosis). For the object recall test, the median score for the whole group was 7 (4.5 for those with a dementia diagnosis). Only five out of 57 genotyped individuals were apolipoprotein (APOE) ε4 carriers (8.8%), and all of them were non-demented. Twelve subjects (21.1%), both demented and cognitively healthy, were carriers of the APOE ε2 allele.
On CT, the most severe atrophy grades according to the different scales were seen only in very few individuals. For the majority, there was an equal representation of MTA grades 1, 2 and 3, whereas grade 2 was the most com-mon degree of fGCA and PA. As for the white matter changes, Fazekas grades 2 and 3 were the most commonly found. When we subdivided the entire group into subjects with no cognitive dysfunction and demented subjects, there were no differences in the degree of different atrophy measures. The extent of me-dial temporal, global cortical and parietal atrophy was similar regardless of the clinical status. For the degree of white matter changes, there were also no differences between the groups. Distribution of atrophy grades can be seen in Fig. 4

32
Figure 4. Number of individuals with the different grades of MTA, fGCA, PA and white matter changes (Fazekas). MTA-medial temporal lobe atrophy, fGCA-frontal lobe atrophy, PA-posterior atrophy.
The CSF levels of the AD biomarkers ranged from 349 to 1343 pg/ml (median level 703 pg/ml) for Aβ42, 202–1121 pg/ml (median level 414 pg/ml) for t-tau and 29–122 pg/ml (median level 61 pg/ml) for p-tau. When comparing the levels between cognitively intact and demented subjects there were no differ-ences between the groups (Fig. 5a).
Next, we wanted to assess possible associations between the different cog-nitive, neuroradiological and biochemical markers. For these analyses we combined the individuals with MTA 1 or 2 and those with MTA 3 or 4. When comparing the CSF biomarker levels between these groups, we found no sig-nificant differences, either for Aβ42, t-tau or p-tau (Fig. 5b). A weak associa-tion could be found between MMSE and MTA, with lower MMSE scores among subjects with MTA grades 3 or 4 than among those with MTA grades 1 or 2 (p = 0.04). However, we did not find any correlation between the results on the object recall test and the degree of MTA. Similarly, there were no cor-relations between either of the two cognitive read-outs and the biochemical CSF markers.

33
Figure 5. Comparison of t-tau, p-tau and Aβ42 CSF concentrations between differ-ent groups. (a) Cognitively healthy (n = 27) and demented (n = 8) individuals (me-dian levels 715 vs 472 pg/ml for Aβ42, 414 vs 427 pg/ml for t-tau and 63 vs 60 pg/ml for p-tau). (b) Individuals with mild (grades 1–2, n = 24) and severe (grades 3–4, n = 11) MTA (median levels 643 vs 715 pg/ml for Aβ42, 441 vs 401 pg/ml for t-tau and 64 vs 53 pg/ml for p-tau). No significant differences observed between the groups for any of these biomarkers. The horizontal line on graphs indicates median levels. Dashed lines represent reference values.
Next, we hypothesized that APOE could have an impact on the degree of brain atrophy. However, no association could be found between the different APOE genotypes and the various neuroradiological measures.
Brain tissues were available from 13 subjects. Three of these had been given a clinical diagnosis of AD, whereas the remaining 10 had not been

34
clinically diagnosed with any neurodegenerative disorder. In all 13 subjects, tau pathology was seen, ranging from very sparse to Braak stage V. Pathology of Aβ was observed in 12 and of α-synuclein in two subjects. One of the cog-nitively unimpaired subjects fulfilled the criteria for primary age-related tauopathy (PART), whereas for the remaining nine cognitively unimpaired subjects, AD-related pathology at the low (four subjects) or intermediate (five subjects) level was observed. Two of the subjects with clinical diagnosis of AD fulfilled the criteria for high level of AD-related pathology. In one of those two subjects, a substantial concomitant α-synuclein pathology was observed. One of the AD patients displayed an intermediate level of AD-related pathol-ogy but also showed a type 1 CAA and vascular tissue alterations. None of the cases displayed any signs of hippocampal sclerosis.
Paper II Inter-rater reliability for visual MTA rating showed substantial agreement (weighted Kappa was 0.62 and 0.67 for the right and the left sides, respec-tively). Intra-rater reliability showed substantial to almost perfect agreement (weighted Kappa was 0.84 and 0.79 for the right and the left sides, respec-tively).
The distribution of MTA highest scores across our cohort is shown in Fig 6.
Figure. 6. Distribution of MTA highest scores across our cohort. MTA-medial tem-poral lobe atrophy.

35
Influence of gender and education on the MTA measures Among the 390 individuals, included in this study, the gender distribution was balanced (47% female, 53% male). Gender had a significant effect on the four MTA measures, with males having significantly higher scores than females. There were significantly more participants with low education (57% had less than 8 years of education, 43% had 9 or more years of education).
Scores for left MTA and average MTA were also significantly higher in highly educated individuals. The interaction between gender and education indicated that scores for MTA highest were lower in females, but only if they had low education (Fig. 7).
Figure. 7. Interaction between gender and education on MTA highest. Education is coded as low “<9 years of education” and high “≥9 years of education”. MTA = me-dial temporal atrophy. MTA = medial temporal atrophy.

36
Normative data and cut-offs for MTA measures by gender and education Based on the above-mentioned results, the sample was stratified into four groups: female + low education (n = 105); female + high education (n = 80); male + low education (n = 119); and male + high education (n = 86). The Kruskal–Wallis test confirmed the effect of gender and education on the MTA measures. Derived 10th percentile cut-off scores indicated that values between 2 and 3 (and higher) were abnormal, depending on the MTA measure, gender and education. By applying these cut-offs, MTA right was abnormal in 64 individuals (16%), MTA left in 83 individuals (21%), MTA average in 69 in-dividuals (18%), and MTA was highest in 88 individuals (23%). In 283 indi-viduals (73%), scores were normal for all MTA measures, and in 40 individ-uals (10%) scores were abnormal for all four MTA measures. Thus, findings were consistent in 323 individuals. Findings were inconsistent in 67 individu-als. In 19 individuals (5%), only the MTA left score was abnormal, in 19 in-dividuals (5%) scores in two MTA measures were abnormal, and in 29 indi-viduals (7%) scores in three MTA measures were abnormal. MTA highest de-tected all the consistent and inconsistent cases except for the 19 individuals detected only by MTA left.
Clinical associations between MTA grade and cognitive tests at baseline and after 5 years Individuals with abnormal MTA average had worse performance in the MMSE and TMT-B. TMT-B performance was also reduced in individuals with abnormal MTA highest.
Mixed ANCOVA suggested faster cognitive decline, measured by the MMSE, in the group with abnormal MTA right at baseline (Fig. 8). No signif-icant interactions between time and MTA status were found for MTA left, MTA average and MTA highest.

37
Figure 8. Changes in MMSE performance after 5 years related to MTA right. Values in the y-axis are the estimated means for MMSE from the mixed ANCOVA when including gender and education as covariates. MTA = medial temporal atrophy; MMSE = mini-mental state examination.
Paper III From the PIVUS participants with brain MRI, we included all who had avail-able data on cognitive tests, visual rating, computed rating and volumetry. The final sample was N = 318.
Intra-rater and inter-rater reliability for visual rating Intra-rater reliability for MTA was almost perfect: weighted kappa was 0.91 and 0.90 for right and left sides, respectively. Intra-rater reliability for PA was 0.70 (substantial) and for F-GCA 0.46 (moderate).
Inter-rater reliability for MTA was substantial: weighted kappa was 0.62 and 0.67 for right and left sides, respectively. Inter-rater reliability for PA was 0.46 (moderate) and for F-GCA 0.19 (slight).
Computed rating with cNeuroÒ versus visual rating Computed ratings were compared with visual ratings for all 318 included sub-jects.
Visual rating showed that majority of subjects (n = 194) had MTA score 1, followed by score 2 (n = 99) and score 3 (n = 25). Only a few subjects had a

38
score of 0 or 4 in any hemisphere. Comparing computed ratings of MTA with visual ratings, strong correlations were found both for the right and the left sides (rs = 0.65 and rs = 0.66 for the right and left sides, respectively, p < 0.001).
When visual rating of F- GCA was performed, none of the subjects had a score of 0 or 3. Thus, since only two scores were present (1 and 2), the variable was converted into a dummy variable, and point-biserial Pearson correlations were calculated. The correlation between the F-GCA computed ratings of cNeuroÒ and visual ratings by the neuroradiologist was weak, but statistically significant (rpb = 0.36, p < 0.001).
In visual rating of PA, none of the participants had a score of 3, only one individual had a score of 0, and the remaining had scores 1 or 2. The case with a score of 0 was removed, and the variable was converted into a dummy vari-able for point-biserial correlations. The correlation between the computed rat-ing of PA by cNeuroÒ with visual rating from the neuroradiologist was mod-erate but statistically significant (rpb = 0.46, p < 0.001).
Volumetry versus visual ratings Volumetric analysis performed by the cNeuroÒ was compared with visual rating by a neuroradiologist (VV).
Hippocampal volumetry correlated weakly and moderately, but statistically significantly, with visual ratings of the MTA performed by the neuroradiolo-gist (rs = −0.38 and rs = −0.43 for the right MTA and left MTA, respectively, p < 0.001).
As mentioned above, none of the subjects had a score of 0 or 3 in the visual rating of F-GCA. Correlation between volumetry of frontal lobes and visual ratings of F-GCA was very weak and not statistically significant (rpb = −0.06, p = 0.265).
In visual rating of PA, none of the participants had a score of 3, and only one individual had a score of 0, the rest having scores 1 or 2. Correlation be-tween volumetry of parietal lobes and visual ratings of PA was very weak and not statistically significant (rpb = 0.01, p = 0.895).
The correlation between computed ratings by cNeuroÒ and visual ratings performed by the neuroradiologist was significantly better than the correlation between volumetry and visual rating.
Association between computed ratings, visual ratings and cognition Overall, performance in the cognitive tests was high, reflecting the fact that we investigated a healthy cohort in this study.

39
A statistically significant correlation was found between the visual MTA scores and the ECRT tests (p = 0.035), SF (p = 0.024) and TMT-B (p < 0.020). No significant correlation was found between visual ratings of PA and F-GCA with cognitive tests. The correlation between automated ratings of atrophy and cognitive tests showed that the best correlation was between atrophy grading in all brain regions and the ECRT tests. In addition, statistically significant correlations were found between atrophy in the medial temporal lobe, the frontal lobe and the MMSE, TMT-B and SF tests.
Paper IV In this study we used data that included visual ratings of atrophy, volumetric analysis of all MRI scans with sufficient image quality, and cognitive tests in a cohort of subjects at ages 75 and 80. The final sample consisted of 201 sub-jects, 94 women and 107 men. At the age 75, none of the participants had dementia or mild cognitive impairment (MCI). After 5 years, only six of them had developed mild cognitive impairment or dementia: MCI in two, AD in two and unspecified dementia in two subjects.
Visual atrophy rating and volumetry at baseline and after 5 years At the age 75, the majority of subjects (63%) had MTA grade 1 on the worst side (127 out of 201). Only four subjects had MTA grade 0, and only two had grade 4. The median for MTA at age 75 was 1. After 5 years, the majority (51%) still had MTA grade 1 (103 out of 201), but the number of subjects with MTA grade 4 had increased to five, and those with grade 0 had decreased in two subjects. The median grade increased to 2, but only for MTA left.
At age 75, none had PA grade 3, and only one individual had PA grade 0. The majority (63%) (126 out of 201) had PA grade 1, and the rest (almost 37%) had PA grade 2. After 5 years, two subjects had PA grade 3, and the majority (71%) (142 out of 201) had PA grade 2. The median for PA increased from 1 at 75 years to 2 at 80 years.
As for F-GCA, at the age of 75, none had atrophy grade 0 or 3, and the majority (82%) (164 out of 201) had atrophy grade 1, while 18% of the sub-jects had grade 2. After 5 years, still none had atrophy grade 3 in the frontal lobes, but the number of subjects with grade 1 F-GCA decreased to 115 (57%), and those with grade 2 F-GCA increased to 37 (43%). The median for F-GCA was unchanged 1 at 75 and 80 years.
Changes in visual ratings of atrophy were examined using the Wilcoxon test, which showed that after 5 years the shift toward a higher grade of atrophy in all brain regions was small, but statistically significant (p < 0.001).

40
Changes in visual ratings of regional brain atrophy after 5 years in the whole cohort are shown in Figure 9.
Figure. 9. Changes in grades of MTA right (a), MTA left (b), PA (c) and F-GCA (d) at age 75 and at age 80. MTA: medial temporal lobe atrophy, PA: posterior atrophy, F-GCA: frontal lobe atrophy. Values in the x-axis show atrophy grades (MTA 0-4, PA and F-GCA 0-3). Values in the y-axis show number of subjects.
Among the six subjects who later developed MCI or dementia, only one had MTA grade 0 and one grade 1; the others had MTA grade 2 and grade 3, in equal distribution. None of them had MTA grade 4 at age 75. As for PA, four subjects had grade 1 PA, the other two grade 2 PA. All these six subjects had F-GCA grade 1 at age 75.
Volumetric analysis showed that hippocampal volume, measured both on the right and left sides, decreased by 5% over 5 years in the entire cohort. The volume of the parietal lobes, calculated on the right and left sides together, decreased by 3% over 5 years, and the volume of the frontal lobes decreased least of all, only by 2% over 5 years.
All changes in volumetry, evaluated using the paired t-test, were statisti-cally significant (p < 0.001).
The average decrease in total hippocampal volume in those six subjects who developed MCI or dementia was 17% over 5 years. The volume of the parietal lobes in these subjects decreased 6% and the volume of the frontal lobes 4% during the course of 5 years.
Visual ratings versus volumetry Visual ratings of atrophy were compared with volumetric analysis performed with FreeSurferÒ software in subjects at age 75 and age 80.

41
Visual ratings of MTA at age 75 correlated statistically significantly with hippocampal volumetry (rs = −0. 38, p < 0.001). At age 80, correlation be-tween visual rating of MTA and hippocampal volumetry increased to moder-ate on both sides (rs = −0.43, and rs = −0.45, p < 0.001 for the right MTA and left MTA, respectively).
There was no significant correlation between the visual ratings of PA and volumetry of parietal lobes at age 75 (p = 0.316). At age 80, a statistically significant correlation was found (rs = −0.16, p = 0.020).
Statistically significant correlation between visual ratings of F-GCA and volumetry of frontal lobes was found in 80-year-old subjects (rpb = 0.19, p = 0.006), but not in 75-year-olds.
Association between visual ratings, volumetry and cognition None of the subjects had clinically established cognitive impairment at the age of 75. After 5 years, only six subjects out of 201 (3%) developed MCI or de-mentia Further, results in all cognitive tests changed very little. The MMSE changed from 29 ± 1 to 28 ± 2 points. The time to complete the TMT-A in-creased from 53 ± 17 to 59 ± 32 s and the TMT-B from 140 ± 86 to 146 ± 75 s. In the six subjects who developed MCI or dementia, changes in cognition were more pronounced. The MMSE changed from 28 ± 1.7 to 23 ± 4.3 points. The time to complete the TMT-A increased from 72 ± 21.3 to 85 ± 35 s and the TMT-B from 134 ± 62 to 152 ± 200 s.
At baseline, statistically significant correlations were only found between the MMSE and MTA right (p = 0.053), the MMSE and parietal lobes volume-try (p = 0.003), and also between the TMT-B and the volumetry of the left hippocampus (p = 0.020) and the TMT-B and the parietal lobe volumetry (p = 0.02). No significant correlations were found between TMT-A and visual rating or volumetry or between any cognitive tests and F-GCA or frontal lobe volumetry.
At age 80 , a statistically significant correlation was found between the MMSE and left hippocampal volumetry (p = 0.014) and frontal lobe volume-try (p = 0.01), the TMT-A and hippocampal volumetry (p = 0.023 for right hippocampal and p = 0.016 for left hippocampal volumetry), the TMT-A and frontal lobe volumetry (p = 0.004), also between the TMT-B and right hippo-campal volumetry (p < 0.001), PA (p = 0.001) and frontal lobe volumetry (p = 0.01).
A repeated measures ANOVA showed statistically significant associations between changes in atrophy ratings and volumetry and results of cognitive tests except TMT-B after 5 years in all cases.

42
Discussion
Paper I The use of imaging and biochemical methods has become increasingly im-portant in the diagnostic work-up of patients with dementia. The disease bi-omarkers detected by these methods do not have a perfect sensitivity or spec-ificity for any of the neurodegenerative disorders, but do provide supportive information. Most notably, the presence of MTA on a CT or MRI scan and decreased Aβ42 together with increased t-tau and p-tau in CSF are indicative of AD. However, as the effects of normal aging on both brain imaging and the CSF biomarkers often mimic those that are seen in the AD brain, both of these diagnostic tools are less useful in a patient population of elderly individuals. [5; 17-20; 35; 61].
We were interested in assessing whether the same dissociation between brain pathology and cognitive function could be seen in the ULSAM cohort, which consisted of men between 86 and 92 years of age. Our study setup was advantageous because all participants could be recruited from this closely monitored and geographically well-defined age-homogeneous population-based cohort [62]. As another favorable feature, we could combine a broad set of different investigations – cognitive testing, brain imaging, CSF analyses and post mortem neuropathological evaluations – something that had not pre-viously been performed in such an aged cohort. As for the choice of imaging method, we decided to use CT instead of MRI, since this technique is more readily available and more commonly used as a part of the routine dementia investigation of elderly patients, at least in Sweden (data from the national Swedish Dementia Registry, www.svedem.se).
For this exploratory study, we aimed at including the largest possible num-ber of still surviving subjects of the ULSAM cohort. However, similar to pre-vious investigations, it was difficult to recruit such old individuals and the limited number of participants may have precluded us from detecting minor differences between the subgroups. Also, the included subjects were likely to be healthier than those who declined to participate, and thus did not represent any more advanced disease forms. This is the probable reason why the demen-tia prevalence in our study was slightly lower than what has been reported in the general population [63; 64].

43
Overall, our data generally confirm previous neuroradiological and CSF-biochemical observations among the elderly [10]. Moreover, the neuropatho-logical assessments enabled us to demonstrate that the brains at these ages regularly display some degree of either Aβ or tau pathology. Most often, they display a combined pathological picture that sometimes can be as severe as that seen in AD cases, even when no cognitive decline can be demonstrated. Also, these observations are in line with what has been previously observed [21].
As we analyzed a range of different neuroradiological and CSF parameters, we were able to assess the possible relationships between these measures. However, we could not find any correlations between any of the markers. Thus, our data suggest that there is an uncoupling between these structural and biochemical markers of brain integrity among very old individuals.
Moreover, there was only a weak correlation between cognitive perfor-mance and the degree of MTA. In addition, no correlation could be found be-tween cognition and the concentrations of the respective CSF biomarkers. These findings suggest that there also was a poor coupling between the cog-nitive functions and the structural/neurochemical alterations in the investi-gated age group.
As it has been suggested that APOE is associated with Aβ deposition and with APOE ε2 carriers displaying less pathology, we also investigated a pos-sible influence of APOE on the degree of brain atrophy [65; 66]. However, in this study we did not find any association between APOE and the various neu-roradiological measures.
Taken together, our data confirm that age-related degenerative processes seem to cause tissue atrophy and aggregation of altered proteins in the brain, but without the involvement of pathophysiological processes that result in the type of cognitive decline seen in AD and other neurodegenerative disorders. Alternatively, the results may be explained by the presence of unknown pro-tective factors in certain cognitively intact subjects whose brains are neverthe-less affected by an AD-like pathophysiology. Either way, the interpretation of an advanced MTA or of an AD-characteristic CSF profile should not neces-sarily be considered pathological in very old individuals.
Paper II In this study, we investigated the distribution of MTA scores in a homogene-ous 75-year-old population-based cohort and the association between MTA scores and cognitive performance, gender and education. The cohort was ho-mogeneous with regard to age, all were 75 years old, and gender distribution.
The present study shows that gender and education are important confound-ers when interpreting MTA scores and deriving clinical cut-offs at the age of

44
75 years. Gender is the main confounder, men having higher MTA scores than women. This is in line with previous studies that had shown that the volume of the hippocampus is smaller in healthy men than in women [67; 68].
Education is another confounder, although not as important as gender. In-dividuals with higher education have better cognitive tests results, even though they have higher MTA scores. This is supported by the theory regard-ing the cognitive reserve of the brain, which states that interindividual differ-ences in the effective usage of brain networks or cognitive processing strate-gies are relevant for preserving better cognition despite pathological pro-cesses. Previous studies have suggested that education compensates for the impact of MTA on cognition: individuals with less than 8 years of education have two times higher risk of developing dementia, and in well-educated in-dividuals the effect of MTA on cognition is weaker than in less well-educated subjects [69-71].
Subjects with normal MMSE scores and abnormal grade of MTA at age 75 years had developed worse MMSE scores 5 years later. This is in line with previous studies based on patients with known cognitive impairment [72-74]. As mentioned above, in well-educated individuals, cognitive reserve may to some degree compensate for more severe MTA, but when cognitive impair-ment emerges, the decline is more rapid. This has also been shown in other studies in normal populations [70].
Our results showed a slight asymmetry of atrophy scores on the right and left sides, with more cases with abnormal MTA on the left than on the right side. One possible explanation could be that the left hippocampus is more vul-nerable because of a smaller premorbid size. Previous studies have shown that asymmetry with smaller hippocampus on the left side is common in normal individuals without dementia, and also in term and preterm newborns [5; 75; 76].
We found a cut-off score of ≥2 for abnormal MTA in low-educated women, but for men and for high-educated women, the cut-off score was ≥2.5 (average of left and right) or ≥3 (highest of left and right). This is partly in agreement with previous studies showing that MTA score of >2 can be regarded as ab-normal in individuals older than 70 to 75 years [44; 77]. It should be empha-sized that cut-off values differ depending on gender and educational level. To our knowledge, this has not been addressed previously. A recent study re-ported that an optimal cut-off value for age 75 years is ≥2 [78]. However, that study was based on patients with AD and subjective cognitive impairment from a memory clinic, which was a different study population than our com-munity-based cohort.
Strengths of our study are that it is population-based, all subjects were of the same age, and the gender distribution was almost symmetrical. Thus, MTA grade and its correlation with education and gender are not affected by age. In addition, we have 5 years’ follow-up of the MMSE. We have provided data

45
not only for left and right MTA scores, but also for the average and the highest score, since they are all used clinically, but the level of cut-off values is not evident in the literature. In addition, we appear to be the first group to provide gender- and education-corrected cut-off values.
A limitation of this study is that we did not determine cut-off values and investigated diagnostic performance in a group of patients with clinical de-mentia. To circumvent this, our definition of abnormality was based on the 10th percentile, which is a common and also valid procedure in studies of this kind [79]. Complementarily, we demonstrated the prognostic value of right MTA for cognitive decline, although the clinical value of the other MTA measures remains questionable. Also, the clinical usefulness of the right MTA score for prediction of longitudinal cognitive decline could not be calculated because only seven individuals developed cognitive impairment (MMSE < 24) at follow-up. However, this further supports the fact that these cut-offs have been derived from a rather healthy and cognitively stable sample.
Paper III Many studies have shown that neurodegenerative diseases are associated with brain atrophy in various regions that can be identified by visual rating and supported by established rating scales and volumetric analysis. Implementa-tion of automated computed ratings and volumetric analysis into clinical prac-tice will provide more objective and reproducible quantitative information than is provided by visual rating by a neuroradiologist.
In the present study, we wanted to examine how well automated rating and volumetry of regional brain atrophy by a clinically approved commercial soft-ware correlated with visual rating of regional atrophy performed by an expe-rienced neuroradiologist.
First, intra- and inter-rater reliability between two experienced neuroradi-ologists were calculated. For MTA, intra-rater reliability was almost perfect, and inter-rater reliability was substantial. But for PA and F-GCA, intra-rater reliability was substantial and fair, and inter-rater reliability was only moder-ate and slight. Results similar to those in our study or slightly better have been found in some other studies [80; 81]. Thus, reliability for PA and F-GCA de-tection is often lower than for MTA, reflecting the fact that they are less used clinically [82; 83]. As a consequence, neuroradiologists have less experience with PA and F-GCA than with MTA, with also contributes to lower reliability. Additionally, F-GCA and PA are known to be more challenging to neuroradi-ologists because they assess larger brain regions than the MTA scale. In the frontal and parietal lobes, there is more sulcal variability and fewer increments in the scale, influencing the level of detail that can be captured by GCA and PA [33; 80]. So, it may be difficult for the human eyes to capture differences

46
between these close grades in a consistent and reproducible way. This may thus contribute to lower reliability. In our study, another explanation for the lower reliability of the F-GCA rating is that in our sample there was very little variability in F-GCA-F and PA rating results.
The correlation between the computed rating of atrophy and the visual rat-ing was strong for MTA. These findings agree with one previous study demonstrating that computed ratings by the same software performed better than visual rating scales currently in use [84]. This indicates that computed MTA scores could be used in the clinical setting [84; 85]. In the above-men-tioned study, the correlation between automated and visual ratings of global cortical atrophy was better than in our study. Weak or moderate correlation between automated and visual rating of F-GCA and PA in our results can probably be explained, as above, by the very low variability in the degree of atrophy in our cohort. Further studies with greater variability in atrophy grades can be helpful to improve correlation results. Also, as discussed above, the F-GCA and PA scales are not used widely, so, even for experienced neuroradi-ologists, it can be challenging to rate atrophy in these regions in a consistent way.
The correlation between the automated rating of atrophy and volumetry was better than the correlation between visual assessment and volumetry. The calculation of MTA used a combination of hippocampal volumes and the vol-ume of the inferior lateral ventricles. F-GCA and PA were estimated by using the volume of cortical gray matter in the frontal and parietal cortex of separate hemispheres. [84]. In the cNeuroÒ output data, the grades are presented as continuous variables. This can partially explain why visual rating of atrophy, in which grades of atrophy are in categorical variables, does not correlate very strongly with computed assessment, especially with regard to F-GCA and PA.
However, with the exception of hippocampal volume measurements, not many studies have been published on volumetry of other brain regions for clinical use. Few studies on MRI-based volumetry in normal populations have been published previously [44; 93; 94].
As expected, the verbal episodic memory tests ECRT-free and ECRT-cued correlated with visual rating of MTA left. The correlations between TMT-B and SF, i.e. measures of executive function, and MTA left were less expected. Lack of correlation between visual scoring of frontal and parietal atrophy and cognitive tests can be explained by the fact that we investigated a population-based cohort without dementia. Another explanation can be the lack of varia-bility in visual scoring of F-GCA and PA.
Correlations between automated ratings of atrophy in different brain re-gions and cognitive tests were better, showing that automated rating of atro-phy can be a better indicator of changes in cognition than visual rating, another reason that encourages implementing automated ratings into the clinical rou-tine.

47
Our results show that automated grading of MTA can be acceptable for use in clinical practice to support the radiologist. For implementation of auto-mated grading of atrophy in the frontal and parietal lobes, further studies with a larger variability in the visual assessment of atrophy scores are needed. Vol-umetric methods, when implemented into clinical practice, could help us to evaluate more subtle pathologic volume changes in the brain, especially when repeated follow-up examinations are performed or in longitudinal studies.
Strengths of our study are that it is population based and homogeneous with regard to age, so age as a confounder can be excluded. Also, we had the pos-sibility to compare not only regional volumetry, but also computer-based, au-tomated ratings of brain atrophy with visual ratings, which, to our knowledge, has only been done in one study previously [84]. In clinical practice, volume-try is presently used only in a limited number of cases. Much more often es-tablished visual scales are used to rate atrophy. In our study, we compared automated ratings of brain atrophy, done by a commercial software, with vis-ual ratings. Good results for rating of MTA in our study may encourage the use of automated ratings in clinical practice. As for automated ratings of F-GCA and PA, further studies with a greater variability of atrophy than in our study are needed to better evaluate and optimize the methods.
Weaknesses of our study are that that we did not include patients with MCI or dementia for comparison and that our cohort had a very limited variation of atrophy grades in the frontal and parietal lobes. Future studies with a more variable cohort may be useful.
Paper IV The present study tracked changes in visual rating and volumetry of regional brain atrophy and cognitive function from age 75 to age 80 in a population-based cohort, where the vast majority of subjects showed good performance on the cognitive tests.
Our study showed that in elderly adults, changes in brain volume, measured both by visual rating and volumetry, are not uniform. The magnitude of change varies across regions.
The visual rating of atrophy in different brain regions showed only minimal change, with slight increases in atrophy grade, mostly in MTA, less in PA and even less in F-GCA. The median value for MTA increased mostly, from grade 1 to grade 2. This is in partial agreement with studies that showed that the optimal cut-off value for MTA at age 75- 80 was grade 2. Those studies were cross-sectional, and to our knowledge no previous publication has evaluated the change of visual scoring grades over time. One of the studies was based on patients with diagnosed AD or MCI, and the other included both patients with diagnosed dementia and control subjects, while our study is population-

48
based, with cognitively intact subjects at baseline and with a minimal number (only six) of subjects who developed dementia at follow-up, which could not influence results.
PA increased with the same value as MTA, from median grade 1 to grade 2. One of the above-mentioned studies showed that the cut-off value for PA at both age 75 and age 80 should be grade 1, whereas our study showed a change toward a higher grade, which probably can be explained by the still quite rare use of this scale. The grade of F-GCA was the same at both time points, median 1, which is in agreement with the above-mentioned study.
The greatest changes, measured by volumetry, were observed in the tem-poral regions, and were less pronounced in the parietal and frontal lobes.
The hippocampal volume had decreased by 5% after 5 years, on average 1% per year, which is in agreement with previous studies, both cross-sectional and longitudinal [4; 95]. Loss of hippocampal volume in the six subjects who after 5 years developed MCI or dementia was more significant: 17% per 5 years, or 3.4% per year. This is less than in other published studies. One ex-planation may be that we examined a population-based cohort, not a cohort from a memory clinic, and a very small number of subjects progressed to MCI or dementia in our cohort [4].
The volume of the parietal lobes decreased by 3% and the volume of the frontal lobes by 2% over 5 years (0.6–0.4% per 1 year). Some earlier studies, based on subjects of various ages, showed more significant loss of gray matter with age [35; 93]. Other studies show volume rate loss (up to 0.32–0.5%) sim-ilar to what was found in our study [95-98]. Although, according to numerous studies, loss of cortex volume in frontal regions in healthy non-demented sub-jects is usually greater than in temporal or parietal regions [3; 96; 99-103]. Other studies show more effects of age on the parietal cortex [101; 103-106]. Our study, however, showed greater loss in volume in the hippocampus than in the frontal or parietal lobes. These controversies probably can be explained by the fact that in the many previous studies, the age range of the examined cohort and the measurements of examined regions were not the same as in our study.
Correlation between visual scoring of atrophy and volumetry at age 75 was found between only MTA and hippocampal volumetry. Similar results have been reported before, although with correlations of various strengths. For ex-ample, some studies showed a correlation strength similar to our study [44; 46; 107]. Another study, although cross-sectional, showed a much stronger correlation between MTA and hippocampal volumetry (−0.753 to −0.767) [107].
At the age of 80, correlation between MTA and hippocampal volumetry increased, and significant correlations, although very weak, were found be-tween PA and parietal lobe volumetry and between F-GCA and frontal lobe volumetry. Results in other studies show better correlations than in our study,

49
especially for the frontal region [102; 108]. Also, one study showed that atro-phy in frontal regions can be more visible only at later follow-up examina-tions, but not at earlier stages [109]. These discrepant results with our study probably can be explained by a very limited variation of atrophy grades in our visual rating, showing that the human eye is probably less sensitive in detect-ing small changes. It also supports the theory that machine-based analysis is more sensitive to subtle progressive changes in brain atrophy than the human eye, both in cross-sectional and longitudinal studies [90-92; 110].
Correlations between visual ratings of atrophy and cognitive tests were minimal. Our results partially agree with results that we described in our ear-lier publication [111]. One of the reasons for such minimal changes could be that in the current study we examined a cognitively healthy population in which none had dementia or MCI at the age of 75. In this cohort, performance in the tests showed no significant deterioration at follow-up.
In the whole cohort, analyzing changes in atrophy in association with changes in cognitive tests over 5 years, we found significant association be-tween atrophy developing and changes in cognitive tests MMSE and TMT-A. But, changes in atrophy, measured by visual grading or volumetry did not cor-related with changes in TMT-B, which usually shows decrease in executive functions and mental flexibility.
More severe cognitive decline in the subjects who developed MCI or de-mentia was associated with greater atrophy in all brain regions. This is in line with studies reporting that cognitive decline is often associated with more marked atrophy [99; 106]. Although, in our study, the very small number of subjects who developed dementia could not significantly affect the results of the whole cohort.
Longitudinal studies have several challenges. First, changes in the hard-ware and software of the scanner can affect the measurements. In this study, all subjects were examined with the same MRI scanner at both time points, with some inevitable routine upgrades between examinations, which is un-likely to bias our findings. Also, drop-out from a cohort can influence final results. Here, we analyzed the same participants at two time points. Longitu-dinal studies are important in determining the clinical relevance of observed brain changes and their relationship with cognitive decline.

50
Conclusions
Paper I In this cohort of aged men only a weak correlation could be seen between cognitive performance and MTA, whereas the various neuroradiological, bio-chemical and neuropathological measures did not correlate with each other. Thus, AD biomarkers seem to be less informative in elderly subjects.
Paper II At age 75, gender and education are confounders for MTA grading. A score of ≥ 2 is abnormal for low-educated women and a score of ≥ 2.5 is abnormal for men and high-educated women. Subjects with abnormal right MTA, but normal MMSE scores had developed worse MMSE scores 5 years later.
Paper III Automated ratings of MTA correlated strongly with visual ratings by a neuro-radiologist and could therefore potentially be used in clinical practice. Imple-mentation of volumetric methods into clinical practice after validation in co-horts with larger variability in atrophy than in our study may improve the ac-curacy of the radiological diagnosis and support evaluation by the neuroradi-ologist.
Paper IV We found a mild age-associated decrease in regional brain volumes in this healthy cohort with well-preserved cognitive and executive functions. Visual assessment may not be sufficient for detecting mild progression of brain atro-phy due to normal aging, but could be useful in the clinical evaluation of pa-tients with more pronounced atrophy.

51
Future perspectives
General perspectives To provide imaging biomarkers for early diagnosis and prognosis is important in suspected dementia. There is intensive ongoing research to develop new, more efficient treatment for Alzheimer's disease. In order to be able to develop and evaluate these new drugs, there is a need for biomarkers that are capable of improving early diagnosis and that also can evaluate the degree and speed of disease progression, as this is difficult to evaluate clinically. Patients with other types of dementia, such as frontotemporal dementia and vascular dementia, do not get the same treatment as patients with suspected Alzheimer's disease, and thus it is also important to improve the differential diagnosis between different types of dementia. Correct diagnosis is essential to ensure that patients receive adequate medication and care.
Specific perspectives At least one further study has been initiated as a result of this PhD project.
A hypothesis of this study is that the computer-based analysis can be used as decision support in clinical suspicion of a particular type of dementia and for differential diagnosis between different types of neurodegenerative de-mentia or vascular dementia.
The overall objective of the project is to evaluate computer-based analysis of magnetic resonance (MR) imaging of the brain to be used as decision sup-port in a prospective patient material in a memory clinic.
Patients will be asked if they want to participate in the study and will be investigated with MRI of the brain for evaluation by computer-based analysis.
The probable diagnosis from automated analysis alone will be compared with the clinical diagnosis made by the experienced geriatrician at the Memory Clinic. A separate comparison will be made between results from the automated analysis and visual evaluation of MRI made separately by an expe-rienced neuroradiologist blinded to clinical information.

52
Sammanfattning på svenska
Analys av regional atrofi vid hjärnavbildning jämfört med kognitiv funktion hos äldre och hos patienter med demens - tvärsnitts- och longitudinell utvärdering. "Framgångsrikt åldrande" är en fysiologisk process som utvecklas utan sam-tidiga sjukdomar. Under åldrandet är förändringar i hjärnan inte jämnt förde-lade utan är relaterade till förändringar i nervcellernas morfologi, och föränd-ringar i vävnadsdensitet är specifika för varje region i hjärnan. Volymredukt-ion börjar i prefrontal cortex följt av temporallob, cerebellära strukturer och hippocampus. Occipitalloberna verkar vara minst drabbade.
Dessa ojämna förändringar i hjärnvolymen är relaterade till kognitiva för-ändringar som ses vid åldrandet. Nedsättning av specifika kognitiva förmågor, såsom exekutiva funktioner och episodiskt minne ses också vid normalt åld-rande.
Demens kan orsakas av ett flertal olika sjukdomar i hjärnan med symptom med minnesproblem, förändringar i visuella-spatiella och språkförmågor. De flesta typer av demens utvecklas långsamt och när individen visar tecken på störning är processer i hjärnan redan avancerade. Demens minskar inte bara personens förmåga att utföra vardagliga aktiviteter, men kan också orsaka för-ändringar i humör eller beteende.
Demens orsakar inte bara funktionshinder, det ökar också dödligheten be-tydligt. Dessa tilltagande problem gör tidig diagnos och möjlig förebyggande och tidig behandling av demens mycket viktig.
Diagnosen av demenssjukdomar är komplex. I de första kriterierna från Nationella institutet för Neurologiska Sjukdomar och Stroke-Alzheimers Sjukdom och Relaterade Sjukdomar (NINDS-ADRDA), publicerad 1984, krävde diagnosen Alzheimers sjukdom att närvaron av kognitiv funktionsned-sättning bekräftades genom neuropsykologisk testning för klinisk diagnos och histopatologisk undersökning krävdes för slutlig diagnos. Sedan dess har sjuk-domsförståelsen utvecklats kraftigt, tillsammans med diagnostiska möjlig-heter. In vivo biomarkörer inkluderar strukturella förändringar i hjärnan, syn-liga på datortomografi (DT) eller magnetisk resonans (MRI), metaboliska för-ändringar som visas med positrontomografi (PET) och cerebrospinalvätska (CSF) biomarkörer. Dessa markörer för neurodegeneration kan nu

53
tillsammans med typisk symptombild och kognitiva testresultat ställa den kli-niska diagnosen Alzheimers sjukdom.
Huvudsyftet med avhandlingen var att jämföra kvantitativ och kvalitativ bildanalys av regional cerebral atrofi och jämföra med kognitiv funktion hos äldre individer och hos patienter med tidig demens.
I studie 1 deltog 58 individer (84–88 år) från ULSAM (Uppsala Longitudi-nal Study of Adult Men) kohort i studien. De genomgick DT av hjärnan, kog-nitiv testning och LP.
För arbete II-IV ingick personer från PIVUS kohorten (Prospective Inve-stigation of the Vasculature in Uppsala Seniors). De personerna har inklude-rats slumpmässigt från befolkningsregistret. MR av hjärnan och kognitiv test-ning utfördes hos 406 patienter vid 75 års ålder och 252 undersöktes vid 80 års ålder.
Resultat Artikel 1 I denna kohort av åldrade män kunde endast en svag korrelation ses mellan kognitiva tester och MTA, medan de olika neuroradiologiska, biokemiska och neuropatologiska åtgärderna inte korrelerade med varandra. Således verkar AD biomarkörer vara mindre informativa hos män med högre ålder.
Artikel 2 De flesta 75-åriga individer hade MTA-poäng ≤ 2. Män hade betydligt högre MTA-poäng än kvinnor. Resultat för vänster och genomsnittlig MTA var sig-nifikant högre hos högutbildade individer. Förhöjd MTA associerades med sämre resultat i kognitivt test och individer med förhöjd MTA hade snabbare progress av kognitiv nedsättning.
Artikel 3 Automatiserad gradering av MTA kan användas i klinisk praxis för att stödja den radiologiska utvärderingen. Datorbaserad bedömning av PA och F-GCA bör testas i framtida studier.
Artikel 4 Majoritet av kognitivt friska äldre delområden vid 75 års ålder endast har en mild hjärnatrofi med mycket liten ökning av atrofi graden över 5 år, bedömd genom visuell bedömning. Dessa små förändringar kan fångas bättre med

54
volumetri. Det var bara minimal minskning av kognitiva funktioner mellan åldrarna 75 och 80 år, vilket korrelerade med förändringar i hjärnvolymen.

55
Acknowledgments
I had no idea how it would like be when I started this project. But it is always better to try, fall and get on your feet again than not to try and be sorry that you never dared. This motto took me through a few crazy moments in my life. This PhD project was one of them, and, I promise you, not the last one.
There are many people I would like to present my greatest thanks and ap-preciation, people who drove me, helped, pushed, encouraged me through this journey, which took me here where I am.
First of all - my supervisors: Elna-Marie Larsson – thank you for everything. For your encouragement, pa-tience, never ending energy. One day, when I “grow-up”, I want to be like you. Eric Westman – co-supervisor and co-author. Thank you for your clear head and great diplomacy. Lena Kilander – co-supervisor and co-author. With your input human brain became even more exciting. To Daniel Ferreira- you are my guru in statistics. I admire your kindness and energy. Vilmantas Giedraitis- my co-author in paper I and one of few Lithuanians in Uppsala. Martin Ingelsson- my main supervisor in paper I. Your generosity helped me to start up! Lars Lind- my co-author in papers II-IV, thank you for your sharing your sci-entific knowledge and material for research. Håkan Ahlström- my co-author in papers II-IV, for your help in reviewing papers and sharing your scientific knowledge. Marcus Fahlström- for resolving all these technical problems I didn’t knew how to address to. Håkan Pettersson- IT wizard. For all your help, time and patience. Johan Wikström- our “new” professor. For your comments and answers, which were always “bullseye”. Ruta- my greatest friend. Thank you for all our “moments”, gossips, laughs and cries. Eric- for are best company!

56
Patrik, Rita, Robert, Anna, David, Nuno, Mahmoud- my current and former colleagues in neuroradiology department. Thank you all! All radiographers and nurses I work with- it is so good to have you beside. Adel Shalabi, the chairman of the Department of Radiology, for your support of research possibilities in our clinical environment. To all my Lithuanian gang- Audra and Donatas, Jolita, Raimonda and Gintu-kas, Egle ir Giedrius, Jonas. It so good to meet you every time. Mum and Dad- thank you that you for having me. Thank you that you allowed me to become who I am. My brother Mindaugas and his family- for not letting me to feel alone. Tomas, Aistis and Gabriele- you are my kids also. My Hans- my love, my love. My knight in shining armor, my pillow, my shoulder to cry and my biggest joy.

57
References
1 Mora F (2013) Successful brain aging: plasticity, environmental enrichment, and lifestyle. Dialogues Clin Neurosci 15:45-52
2 Peters R (2006) Ageing and the brain. Postgrad Med J 82:84-88 3 Fjell AM, Walhovd KB (2010) Structural brain changes in aging: courses,
causes and cognitive consequences. Rev Neurosci 21:187-221 4 Jack CR, Jr., Petersen RC, Xu Y et al (1998) Rate of medial temporal lobe
atrophy in typical aging and Alzheimer's disease. Neurology 51:993-999 5 Zhang Y, Qiu C, Lindberg O et al (2010) Acceleration of hippocampal atrophy
in a non-demented elderly population: the SNAC-K study. Int Psychogeriatr 22:14-25
6 Ferri CP, Prince M, Brayne C et al (2005) Global prevalence of dementia: a Delphi consensus study. Lancet 366:2112-2117
7 Mortality GBD, Causes of Death C (2015) Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 385:117-171
8 McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan EM (1984) Clinical diagnosis of Alzheimer's disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer's Disease. Neurology 34:939-944
9 Dubois B, Feldman HH, Jacova C et al (2007) Research criteria for the diagnosis of Alzheimer's disease: revising the NINCDS-ADRDA criteria. Lancet Neurol 6:734-746
10 Schoonenboom NS, van der Flier WM, Blankenstein MA et al (2008) CSF and MRI markers independently contribute to the diagnosis of Alzheimer's disease. Neurobiol Aging 29:669-675
11 Jack CR, Jr., Albert MS, Knopman DS et al (2011) Introduction to the recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement 7:257-262
12 Folstein MF, Folstein SE, McHugh PR (1975) "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12:189-198
13 Solomon PR, Hirschoff A, Kelly B et al (1998) A 7 minute neurocognitive screening battery highly sensitive to Alzheimer's disease. Arch Neurol 55:349-355
14 Meulen EF, Schmand B, van Campen JP et al (2004) The seven minute screen: a neurocognitive screening test highly sensitive to various types of dementia. J Neurol Neurosurg Psychiatry 75:700-705
15 Salthouse TA (2011) What cognitive abilities are involved in trail-making performance? Intelligence 39:222-232

58
16 Tombaugh TN (2004) Trail Making Test A and B: normative data stratified by age and education. Arch Clin Neuropsychol 19:203-214
17 Hansson O, Zetterberg H, Buchhave P, Londos E, Blennow K, Minthon L (2006) Association between CSF biomarkers and incipient Alzheimer's disease in patients with mild cognitive impairment: a follow-up study. Lancet Neurol 5:228-234
18 Bouwman FH, van der Flier WM, Schoonenboom NS et al (2007) Longitudinal changes of CSF biomarkers in memory clinic patients. Neurology 69:1006-1011
19 Shaw LM, Vanderstichele H, Knapik-Czajka M et al (2009) Cerebrospinal fluid biomarker signature in Alzheimer's disease neuroimaging initiative subjects. Ann Neurol 65:403-413
20 De Meyer G, Shapiro F, Vanderstichele H et al (2010) Diagnosis-independent Alzheimer disease biomarker signature in cognitively normal elderly people. Arch Neurol 67:949-956
21 Villemagne VL, Burnham S, Bourgeat P et al (2013) Amyloid beta deposition, neurodegeneration, and cognitive decline in sporadic Alzheimer's disease: a prospective cohort study. Lancet Neurol 12:357-367
22 Murray ME, Graff-Radford NR, Ross OA, Petersen RC, Duara R, Dickson DW (2011) Neuropathologically defined subtypes of Alzheimer's disease with distinct clinical characteristics: a retrospective study. Lancet Neurol 10:785-796
23 Savva GM, Wharton SB, Ince PG et al (2009) Age, neuropathology, and dementia. N Engl J Med 360:2302-2309
24 Brumback-Peltz C, Balasubramanian AB, Corrada MM, Kawas CH (2011) Diagnosing dementia in the oldest-old. Maturitas 70:164-168
25 Bennett DA, Wilson RS, Boyle PA, Buchman AS, Schneider JA (2012) Relation of neuropathology to cognition in persons without cognitive impairment. Ann Neurol 72:599-609
26 Corrada MM, Berlau DJ, Kawas CH (2012) A population-based clinicopathological study in the oldest-old: the 90+ study. Curr Alzheimer Res 9:709-717
27 Chui HC, Ramirez-Gomez L (2015) Clinical and imaging features of mixed Alzheimer and vascular pathologies. Alzheimers Res Ther 7:21
28 Serrano-Pozo A, Qian J, Monsell SE et al (2014) Mild to moderate Alzheimer dementia with insufficient neuropathological changes. Ann Neurol 75:597-601
29 Wahlund LO, Westman E, van Westen D et al (2017) Imaging biomarkers of dementia: recommended visual rating scales with teaching cases. Insights Imaging 8:79-90
30 Wolk DA, Detre JA (2012) Arterial spin labeling MRI: an emerging biomarker for Alzheimer's disease and other neurodegenerative conditions. Curr Opin Neurol 25:421-428
31 Scheltens P, Leys D, Barkhof F et al (1992) Atrophy of medial temporal lobes on MRI in "probable" Alzheimer's disease and normal ageing: diagnostic value and neuropsychological correlates. J Neurol Neurosurg Psychiatry 55:967-972
32 Wattjes MP, Henneman WJ, van der Flier WM et al (2009) Diagnostic imaging of patients in a memory clinic: comparison of MR imaging and 64-detector row CT. Radiology 253:174-183
33 Koedam EL, Lehmann M, van der Flier WM et al (2011) Visual assessment of posterior atrophy development of a MRI rating scale. Eur Radiol 21:2618-2625

59
34 Pasquier F, Leys D, Weerts JG, Mounier-Vehier F, Barkhof F, Scheltens P (1996) Inter- and intraobserver reproducibility of cerebral atrophy assessment on MRI scans with hemispheric infarcts. Eur Neurol 36:268-272
35 Tang Y, Whitman GT, Lopez I, Baloh RW (2001) Brain volume changes on longitudinal magnetic resonance imaging in normal older people. J Neuroimaging 11:393-400
36 Cavallin L, Loken K, Engedal K et al (2012) Overtime reliability of medial temporal lobe atrophy rating in a clinical setting. Acta Radiol 53:318-323
37 Destrieux C, Fischl B, Dale A, Halgren E (2010) Automatic parcellation of human cortical gyri and sulci using standard anatomical nomenclature. Neuroimage 53:1-15
38 Desikan RS, Segonne F, Fischl B et al (2006) An automated labeling system for subdividing the human cerebral cortex on MRI scans into gyral based regions of interest. Neuroimage 31:968-980
39 Sanchez-Benavides G, Gomez-Anson B, Sainz A, Vives Y, Delfino M, Pena-Casanova J (2010) Manual validation of FreeSurfer's automated hippocampal segmentation in normal aging, mild cognitive impairment, and Alzheimer Disease subjects. Psychiatry Res 181:219-225
40 Maitra R, Riddles JJ (2010) Synthetic magnetic resonance imaging revisited. IEEE Trans Med Imaging 29:895-902
41 Warntjes JB, Leinhard OD, West J, Lundberg P (2008) Rapid magnetic resonance quantification on the brain: Optimization for clinical usage. Magn Reson Med 60:320-329
42 Kim H, Park CM, Lee SM, Lee HJ, Goo JM (2013) A comparison of two commercial volumetry software programs in the analysis of pulmonary ground-glass nodules: segmentation capability and measurement accuracy. Korean J Radiol 14:683-691
43 Shinohara RT, Oh J, Nair G et al (2017) Volumetric Analysis from a Harmonized Multisite Brain MRI Study of a Single Subject with Multiple Sclerosis. AJNR Am J Neuroradiol 38:1501-1509
44 Cavallin L, Bronge L, Zhang Y et al (2012) Comparison between visual assessment of MTA and hippocampal volumes in an elderly, non-demented population
45 Westman E, Cavallin L, Muehlboeck JS et al (2011) Sensitivity and specificity of medial temporal lobe visual ratings and multivariate regional MRI classification in Alzheimer's disease. PLoS One 6:e22506
46 Boutet C, Chupin M, Colliot O et al (2012) Is radiological evaluation as good as computer-based volumetry to assess hippocampal atrophy in Alzheimer's disease? Neuroradiology 54:1321-1330
47 Drzezga A (2009) Diagnosis of Alzheimer's disease with [18F]PET in mild and asymptomatic stages. Behav Neurol 21:101-115
48 Brown RK, Bohnen NI, Wong KK, Minoshima S, Frey KA (2014) Brain PET in suspected dementia: patterns of altered FDG metabolism. Radiographics 34:684-701
49 Buckner RL, Snyder AZ, Shannon BJ et al (2005) Molecular, structural, and functional characterization of Alzheimer's disease: evidence for a relationship between default activity, amyloid, and memory. J Neurosci 25:7709-7717
50 Iaccarino L, Sala A, Caminiti SP, Perani D (2017) The emerging role of PET imaging in dementia. F1000Res 6:1830
51 Lilja J, Thurfjell L, Sorensen J (2016) Visualization and Quantification of 3-Dimensional Stereotactic Surface Projections for 18F-Flutemetamol PET Using Variable Depth. J Nucl Med 57:1078-1083

60
52 Kahn CE, Jr. (1994) Artificial intelligence in radiology: decision support systems. Radiographics 14:849-861
53 McDonald RJ, Schwartz KM, Eckel LJ et al (2015) The effects of changes in utilization and technological advancements of cross-sectional imaging on radiologist workload. Acad Radiol 22:1191-1198
54 Hosny A, Parmar C, Quackenbush J, Schwartz LH, Aerts H (2018) Artificial intelligence in radiology. Nat Rev Cancer 18:500-510
55 Zaharchuk G, Gong E, Wintermark M, Rubin D, Langlotz CP (2018) Deep Learning in Neuroradiology. AJNR Am J Neuroradiol 39:1776-1784
56 Barbier CE, Nylander R, Themudo R et al (2011) Prevalence of unrecognized myocardial infarction detected with magnetic resonance imaging and its relationship to cerebral ischemic lesions in both sexes. J Am Coll Cardiol 58:1372-1377
57 Hansen T, Wikstrom J, Johansson LO, Lind L, Ahlstrom H (2007) The prevalence and quantification of atherosclerosis in an elderly population assessed by whole-body magnetic resonance angiography. Arterioscler Thromb Vasc Biol 27:649-654
58 Fischl B (2012) FreeSurfer. Neuroimage 62:774-781 59 (2013) FreeSurfer. Available via https://surfer.nmr.mgh.harvard.edu 60 Landis JR, Koch GG (1977) The measurement of observer agreement for
categorical data. Biometrics 33:159-174 61 Erten-Lyons D, Dodge HH, Woltjer R et al (2013) Neuropathologic basis of
age-associated brain atrophy. JAMA Neurol 70:616-622 62 Franzon K, Zethelius B, Cederholm T, Kilander L (2015) Modifiable midlife
risk factors, independent aging, and survival in older men: report on long-term follow-up of the Uppsala Longitudinal Study of Adult Men cohort. J Am Geriatr Soc 63:877-885
63 Winblad B, Amouyel P, Andrieu S et al (2016) Defeating Alzheimer's disease and other dementias: a priority for European science and society. Lancet Neurol 15:455-532
64 Chene G, Beiser A, Au R et al (2015) Gender and incidence of dementia in the Framingham Heart Study from mid-adult life. Alzheimers Dement 11:310-320
65 Grothe MJ, Villeneuve S, Dyrba M, Bartres-Faz D, Wirth M, Alzheimer's Disease Neuroimaging I (2017) Multimodal characterization of older APOE2 carriers reveals selective reduction of amyloid load. Neurology 88:569-576
66 Berlau DJ, Corrada MM, Robinson JL et al (2013) Neocortical beta-amyloid area is associated with dementia and APOE in the oldest-old. Alzheimers Dement 9:699-705
67 Barnes J, Ridgway GR, Bartlett J et al (2010) Head size, age and gender adjustment in MRI studies: a necessary nuisance? Neuroimage 53:1244-1255
68 Pruessner JC, Collins DL, Pruessner M, Evans AC (2001) Age and gender predict volume decline in the anterior and posterior hippocampus in early adulthood. J Neurosci 21:194-200
69 Perneczky R, Wagenpfeil S, Lunetta KL et al (2009) Education attenuates the effect of medial temporal lobe atrophy on cognitive function in Alzheimer's disease: the MIRAGE study. J Alzheimers Dis 17:855-862
70 Stern Y (2012) Cognitive reserve in ageing and Alzheimer's disease. Lancet Neurol 11:1006-1012
71 Koepsell TD, Kurland BF, Harel O, Johnson EA, Zhou XH, Kukull WA (2008) Education, cognitive function, and severity of neuropathology in Alzheimer disease. Neurology 70:1732-1739

61
72 Visser PJ, Verhey FR, Hofman PA, Scheltens P, Jolles J (2002) Medial temporal lobe atrophy predicts Alzheimer's disease in patients with minor cognitive impairment. J Neurol Neurosurg Psychiatry 72:491-497
73 Duara R, Loewenstein DA, Potter E et al (2008) Medial temporal lobe atrophy on MRI scans and the diagnosis of Alzheimer disease. Neurology 71:1986-1992
74 Henneman WJ, Sluimer JD, Barnes J et al (2009) Hippocampal atrophy rates in Alzheimer disease: added value over whole brain volume measures. Neurology 72:999-1007
75 Lucarelli RT, Peshock RM, McColl R et al (2013) MR imaging of hippocampal asymmetry at 3T in a multiethnic, population-based sample: results from the Dallas Heart Study. AJNR Am J Neuroradiol 34:752-757
76 Thompson DK, Wood SJ, Doyle LW, Warfield SK, Egan GF, Inder TE (2009) MR-determined hippocampal asymmetry in full-term and preterm neonates. Hippocampus 19:118-123
77 Barkhof F (2011) Neuroimaging in dementia 78 Claus JJ, Staekenborg SS, Holl DC et al (2017) Practical use of visual medial
temporal lobe atrophy cut-off scores in Alzheimer's disease: Validation in a large memory clinic population. Eur Radiol. 10.1007/s00330-016-4726-3
79 Jack CR, Jr., Knopman DS, Weigand SD et al (2012) An operational approach to National Institute on Aging-Alzheimer's Association criteria for preclinical Alzheimer disease. Ann Neurol 71:765-775
80 Scheltens P, Pasquier F, Weerts JG, Barkhof F, Leys D (1997) Qualitative assessment of cerebral atrophy on MRI: inter- and intra-observer reproducibility in dementia and normal aging. Eur Neurol 37:95-99
81 Vanhoenacker AS, Sneyers B, De Keyzer F, Heye S, Demaerel P (2017) Evaluation and clinical correlation of practical cut-offs for visual rating scales of atrophy: normal aging versus mild cognitive impairment and Alzheimer's disease. Acta Neurol Belg 117:661-669
82 Harper L, Barkhof F, Fox NC, Schott JM (2015) Using visual rating to diagnose dementia: a critical evaluation of MRI atrophy scales. J Neurol Neurosurg Psychiatry 86:1225-1233
83 Harper L, Fumagalli GG, Barkhof F et al (2016) MRI visual rating scales in the diagnosis of dementia: evaluation in 184 post-mortem confirmed cases. Brain 139:1211-1225
84 Lotjonen J (2017) COMPUTED RATING SCALES FOR COGNITIVE DISORDERS FROM MRI,
85 Lotjonen JM, Wolz R, Koikkalainen JR et al (2010) Fast and robust multi-atlas segmentation of brain magnetic resonance images. Neuroimage 49:2352-2365
86 Chow TW, Gao F, Links KA et al (2011) Visual rating versus volumetry to detect frontotemporal dementia. Dement Geriatr Cogn Disord 31:371-378
87 Scheltens P, Launer LJ, Barkhof F, Weinstein HC, van Gool WA (1995) Visual assessment of medial temporal lobe atrophy on magnetic resonance imaging: interobserver reliability. J Neurol 242:557-560
88 Suarez J, Tartaglia MC, Vitali P et al (2009) Characterizing radiology reports in patients with frontotemporal dementia. Neurology 73:1073-1074
89 Reid MW, Hannemann NP, York GE et al (2017) Comparing Two Processing Pipelines to Measure Subcortical and Cortical Volumes in Patients with and without Mild Traumatic Brain Injury. J Neuroimaging 27:365-371

62
90 Ross DE, Ochs AL, DeSmit ME, Seabaugh JM, Havranek MD, Alzheimer's Disease Neuroimaging I (2015) Man Versus Machine Part 2: Comparison of Radiologists' Interpretations and NeuroQuant Measures of Brain Asymmetry and Progressive Atrophy in Patients With Traumatic Brain Injury. J Neuropsychiatry Clin Neurosci 27:147-152
91 Ross DE, Ochs AL, Seabaugh JM, Shrader CR, Alzheimer's Disease Neuroimaging I (2013) Man versus machine: comparison of radiologists' interpretations and NeuroQuant(R) volumetric analyses of brain MRIs in patients with traumatic brain injury. J Neuropsychiatry Clin Neurosci 25:32-39
92 Tuokkola T, Koikkalainen J, Parkkola R, Karrasch M, Lotjonen J, Rinne JO (2018) Longitudinal changes in the brain in mild cognitive impairment: a magnetic resonance imaging study using the visual rating method and tensor-based morphometry. Acta Radiol 59:973-979
93 Kruggel F (2006) MRI-based volumetry of head compartments: normative values of healthy adults. Neuroimage 30:1-11
94 Carne RP, Vogrin S, Litewka L, Cook MJ (2006) Cerebral cortex: an MRI-based study of volume and variance with age and sex. J Clin Neurosci 13:60-72
95 Scahill RI, Frost C, Jenkins R, Whitwell JL, Rossor MN, Fox NC (2003) A longitudinal study of brain volume changes in normal aging using serial registered magnetic resonance imaging. Arch Neurol 60:989-994
96 Jack CR, Jr., Shiung MM, Weigand SD et al (2005) Brain atrophy rates predict subsequent clinical conversion in normal elderly and amnestic MCI. Neurology 65:1227-1231
97 Chan D, Fox NC, Jenkins R, Scahill RI, Crum WR, Rossor MN (2001) Rates of global and regional cerebral atrophy in AD and frontotemporal dementia. Neurology 57:1756-1763
98 Mueller EA, Moore MM, Kerr DC et al (1998) Brain volume preserved in healthy elderly through the eleventh decade. Neurology 51:1555-1562
99 Leong RLF, Lo JC, Sim SKY et al (2017) Longitudinal brain structure and cognitive changes over 8 years in an East Asian cohort. Neuroimage 147:852-860
100 Raz N, Lindenberger U, Rodrigue KM et al (2005) Regional brain changes in aging healthy adults: general trends, individual differences and modifiers. Cereb Cortex 15:1676-1689
101 Resnick SM, Pham DL, Kraut MA, Zonderman AB, Davatzikos C (2003) Longitudinal magnetic resonance imaging studies of older adults: a shrinking brain. J Neurosci 23:3295-3301
102 Driscoll I, Davatzikos C, An Y et al (2009) Longitudinal pattern of regional brain volume change differentiates normal aging from MCI. Neurology 72:1906-1913
103 Fjell AM, Westlye LT, Amlien I et al (2009) High consistency of regional cortical thinning in aging across multiple samples. Cereb Cortex 19:2001-2012
104 Good CD, Johnsrude IS, Ashburner J, Henson RN, Friston KJ, Frackowiak RS (2001) A voxel-based morphometric study of ageing in 465 normal adult human brains. Neuroimage 14:21-36
105 Salat DH, Buckner RL, Snyder AZ et al (2004) Thinning of the cerebral cortex in aging. Cereb Cortex 14:721-730
106 Brickman AM, Habeck C, Zarahn E, Flynn J, Stern Y (2007) Structural MRI covariance patterns associated with normal aging and neuropsychological functioning. Neurobiol Aging 28:284-295

63
107 Persson K, Barca ML, Cavallin L et al (2018) Comparison of automated volumetry of the hippocampus using NeuroQuant(R) and visual assessment of the medial temporal lobe in Alzheimer's disease. Acta Radiol 59:997-1001
108 Ferreira D, Cavallin L, Granberg T et al (2016) Quantitative validation of a visual rating scale for frontal atrophy: associations with clinical status, APOE e4, CSF biomarkers and cognition. Eur Radiol 26:2597-2610
109 Raz N, Ghisletta P, Rodrigue KM, Kennedy KM, Lindenberger U (2010) Trajectories of brain aging in middle-aged and older adults: regional and individual differences. Neuroimage 51:501-511
110 Tuokkola T, Koikkalainen J, Parkkola R, Karrasch M, Lotjonen J, Rinne JO (2016) Visual rating method and tensor-based morphometry in the diagnosis of mild cognitive impairment and Alzheimer's disease: a comparative magnetic resonance imaging study. Acta Radiol 57:348-355
111 Velickaite V, Ferreira D, Cavallin L et al (2018) Medial temporal lobe atrophy ratings in a large 75-year-old population-based cohort: gender-corrected and education-corrected normative data. Eur Radiol 28:1739-1747

Acta Universitatis UpsaliensisDigital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1546
Editor: The Dean of the Faculty of Medicine
A doctoral dissertation from the Faculty of Medicine, UppsalaUniversity, is usually a summary of a number of papers. A fewcopies of the complete dissertation are kept at major Swedishresearch libraries, while the summary alone is distributedinternationally through the series Digital ComprehensiveSummaries of Uppsala Dissertations from the Faculty ofMedicine. (Prior to January, 2005, the series was publishedunder the title “Comprehensive Summaries of UppsalaDissertations from the Faculty of Medicine”.)
Distribution: publications.uu.seurn:nbn:se:uu:diva-378578
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2019