View
58
Chest pain of unknown Chest pain of unknown origin (CPUO): role of origin (CPUO): role of the esophagus the esophagus Richard I. Rothstein, MD Richard I. Rothstein, MD Chief, Section of Gastroenterology and Chief, Section of Gastroenterology and Hepatology Hepatology Dartmouth Hitchcock Medical Center Dartmouth Hitchcock Medical Center Professor of Medicine Professor of Medicine Dartmouth Medical School Dartmouth Medical School
-
Upload
patrick89 -
Category
Health & Medicine
-
view
548 -
download
0
description
Transcript of View

Chest pain of unknown Chest pain of unknown origin (CPUO): role of the origin (CPUO): role of the
esophagusesophagus
Richard I. Rothstein, MDRichard I. Rothstein, MDChief, Section of Gastroenterology and HepatologyChief, Section of Gastroenterology and Hepatology
Dartmouth Hitchcock Medical CenterDartmouth Hitchcock Medical CenterProfessor of MedicineProfessor of Medicine
Dartmouth Medical SchoolDartmouth Medical School

Chest Pain of Unknown OriginChest Pain of Unknown Origin

Prognosis for angina-like pain with Prognosis for angina-like pain with normal coronary anatomynormal coronary anatomy
Chambers, Prog Cardiovasc Dis 1990
Kemp, Am J Med 1973

Functional Status – normal Functional Status – normal coronary anatomycoronary anatomy
Ockene N Engl J Med 1980

Reflux common in pts Reflux common in pts withwith coronary diseasecoronary disease
Singh, Ann Intern Med,1992; 117:824-30n = 30, 164 chest pain episodes

Abnormal esophageal motilityAbnormal esophageal motility
(n = 910) (n = 255)
Katz, Ann Intern Med, 1987; 106:593-7

Edrophonium TestingEdrophonium Testing
80 mcg/Kg IV

Diagnostic Yield of Esophageal Diagnostic Yield of Esophageal TestingTesting
Katz, Ann Intern Med, 1987; 106:593-7

Intraesophageal Balloon Inflation:Intraesophageal Balloon Inflation:Esophageal HypersensitivityEsophageal Hypersensitivity
n = 30 NCCP, 30 controls Richter, Gastroenterol, 1986; 91:845-52

Provocative TestingProvocative Testing
Barrish, Dig Dis Sci, 1986; 31:1292-8

WithWithEsophagealEsophagealSymptomsSymptoms
IsolatedIsolatedChestChestPainPain
Subgroups of Patients With Chest Subgroups of Patients With Chest PainPain
Anxiety/SomatizationAnxiety/SomatizationNeurosisNeurosis

• Rare for esophageal pathologyRare for esophageal pathology• Question the “non-cardiac”Question the “non-cardiac”• Reassurance, tincture of timeReassurance, tincture of time
Subgroups of Patients With Chest Subgroups of Patients With Chest PainPain
IsolatedIsolatedChestChestPainPain

• HeartburnHeartburn
• RegurgitationRegurgitation
• DysphagiaDysphagia
• Water brashWater brash
• NauseaNausea
• VomitingVomiting
Evaluate or treat for recognized esophageal disordersEvaluate or treat for recognized esophageal disorders
WithWithEsophagealEsophagealSymptomsSymptoms
Subgroups of Patients With Chest Subgroups of Patients With Chest PainPain

EndoscopyEndoscopy
Detection of Esophageal Disorders Detection of Esophageal Disorders Potentially Responsible for Potentially Responsible for
SymptomsSymptoms
pHpH • EGD-negative GERDEGD-negative GERD
Barium swallow ± Barium swallow ± manometrymanometry
• Esophageal stricture/webEsophageal stricture/web
• AchalasiaAchalasia
• Esophageal spasmEsophageal spasm
• Reflux esophagitisReflux esophagitis
• Infectious esophagitisInfectious esophagitis
• Pill esophagitisPill esophagitis
• Esophageal cancerEsophageal cancer
• Esophageal stricture/webEsophageal stricture/web

pH testing - Conventional pH testing - Conventional
Catheter Based:Catheter Based:
Patient IntolerancePatient Intolerance UncomfortableUncomfortable Pharyngeal and Throat Pharyngeal and Throat
DiscomfortDiscomfort Runny NoseRunny Nose
Artifact ProneArtifact Prone Alters Regular Diet and Alters Regular Diet and
ActivityActivity

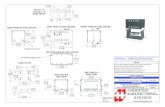
Catheter-Free pH Monitoring System
pH Capsule attached to the esophageal wall transmits data to pager-sized Receiver
Eliminates uncomfortable 24-hr trans-nasal catheter
Allows normal activities, showering and does not interfere with sleeping
Bravo pH System™Bravo pH System™

pH Capsule
Catheter
Handle
Bravo pH Capsule with Bravo pH Capsule with Delivery SystemDelivery System

Step 1
Position Bravo Capsule
Step 2
Apply Suction
Step 3
Advance Pin
Step 5
Begin pH Recording
Step 4
Release Capsule
Capsule Attachment

pH Capsule transmits data to pager-sized Receiver
pH Capsule
Receiver
Bravo pH ReceiverBravo pH Receiver

Use Digital Radio-Telemetry
Capsule measures pH every 6 sec and transmits data to receiver every 12 sec
Keep the receiver within 1m to prevent data loss (range up to 3m)
Digital Radio-TelemetryDigital Radio-Telemetry



Esophageal Testing in 123 Patients with Chest Pain Esophageal Testing in 123 Patients with Chest Pain and Normal Coronary Arteriogramsand Normal Coronary Arteriograms
TestTest% Abnormal% Abnormal
Ambulatory pH monitoringAmbulatory pH monitoring 8282
Esophageal motilityEsophageal motility 2929
Bernstein TestBernstein Test 1010
EdrophoniumEdrophonium 66
EndoscopyEndoscopy 55
Balloon distentionBalloon distention 44
Treadmill with pH monitorTreadmill with pH monitor 44
Chenan P, et al Dis Esophagus 1995; 8:129Chenan P, et al Dis Esophagus 1995; 8:129

Atypical presentations of Atypical presentations of GERDGERD
PulmonaryPulmonaryAsthmaAsthmaBronchitisBronchitisAspiration pneumoniaAspiration pneumoniaApneaApneaAtelectasisAtelectasisPulmonary fibrosisPulmonary fibrosis
ENTENTHoarsenessHoarsenessCoughCoughGlobusGlobusHalitosisHalitosisVocal cord granuloma Vocal cord granuloma Laryngeal stenosisLaryngeal stenosisLaryngeal cancerLaryngeal cancerLoss of dental enamelLoss of dental enamelSinusitis, otitisSinusitis, otitisChest PainChest Pain

Esophageal Chest Pain Work-UpEsophageal Chest Pain Work-Up
TraditionallyTraditionally EndoscopyEndoscopy pH probepH probe ManometryManometry Provocative testingProvocative testing
Emerging role for up-front Emerging role for up-front empiricismempiricism

Fass et al. Fass et al. GastroenterologyGastroenterology. 1998;115:42-49.. 1998;115:42-49.
GERD-PositiveGERD-Positive• n=23n=23• 78% response78% response
GERD-NegativeGERD-Negative• n=14n=14• 14% response14% response
PPI Trial in GERD Patients With PPI Trial in GERD Patients With Non-Cardiac Chest PainNon-Cardiac Chest Pain
37 patients with daily chest pain and negative cardiologic 37 patients with daily chest pain and negative cardiologic evaluationevaluation
Categorized as GERD+ or GERD- by EGD and pH studyCategorized as GERD+ or GERD- by EGD and pH study Randomized to omeprazole (40 mg q AM and 20 mg q PM for 7 Randomized to omeprazole (40 mg q AM and 20 mg q PM for 7
days) or placebo then crossed over after washoutdays) or placebo then crossed over after washout 50% reduction in symptoms constituted positive response50% reduction in symptoms constituted positive response

Characteristics of the PatientsCharacteristics of the Patients
Patients with NCCPPatients with NCCP
GERD-positiveGERD-positive GERD-negativeGERD-negative
Fass R, et al Gastroenterol 1998; 115:42-9Fass R, et al Gastroenterol 1998; 115:42-9
SubjectsSubjects 23231414
Age (yr)Age (yr) 58.2±58.2±2.32.3 61.6±61.6± 2.82.8
Range (yr) 35-76 47-83Range (yr) 35-76 47-83
Sex (M / F) 22 / 1 14 / 0Sex (M / F) 22 / 1 14 / 0
Upper endoscopy resultsUpper endoscopy results
Normal (grade 0-1)Normal (grade 0-1) 771414
Erosive esophagitis (grade 2-5)Erosive esophagitis (grade 2-5) 1616
Ambulatory 24-h esophageal pHAmbulatory 24-h esophageal pH
monitoring (%)*monitoring (%)*
MeanMean 9.6±9.6±1.81.8 1.2±1.2± 0.30.3
Range 0.5-29.1 0.0-2.9Range 0.5-29.1 0.0-2.9
*% total time pH<4*% total time pH<4

EnrollmentEnrollment
Upper endoscopy &Upper endoscopy &Ambulatory 24-hour esophageal pH Ambulatory 24-hour esophageal pH
monitoringmonitoring
GERD + GERD -GERD + GERD -
Baseline symptom assessmentBaseline symptom assessment
RandomizationRandomization
Placebo Placebo OmeprazoleOmeprazole(40 mg AM + 20 mg PM)(40 mg AM + 20 mg PM)
Washout periodWashout period
Baseline symptom assessmentBaseline symptom assessment
Omeprazole Omeprazole Placebo Placebo (40 mg AM + 20 mg PM)(40 mg AM + 20 mg PM)
Week 1Week 1
Week 2Week 2
Week 3Week 3
Week 4Week 4
Week 5Week 5Fass R, et al Fass R, et al
Gastroenterol 1998; Gastroenterol 1998; 115:42-9115:42-9

Omeprazole Test in NCCPOmeprazole Test in NCCP
18/23 GERD-positive (78%)18/23 GERD-positive (78%) 2/14 GERD-negative (14%)2/14 GERD-negative (14%)
Sensitivity 78.3%Sensitivity 78.3% Sensitivity 85.7%Sensitivity 85.7%
59% reduction in number of diagnostic 59% reduction in number of diagnostic procedures procedures ($573 savings per patient evaluation)($573 savings per patient evaluation)
Fass R, et al Gastroenterol 1998; 115:42-9Fass R, et al Gastroenterol 1998; 115:42-9
Positive Positive OTOT

Results of Economic AnalysisResults of Economic Analysis
ConventionalConventionalwork-upwork-up OTOT DifferenceDifference % Change% Change
Cost ($)Cost ($) 20252025 1452145257357328 Reduction28 Reduction
No. of endoscopies/No. of endoscopies/ 1000 patients1000 patients 10001000 19019081081081 Reduction81 Reduction
No. of ambulatoryNo. of ambulatory 24-hr pH tests/24-hr pH tests/ 1000 patients1000 patients 650650 14014051051079 Reduction79 Reduction
No. of esophagealNo. of esophageal motility tests /motility tests / 1000 patients1000 patients 310310 470470-160-16052 Increase52 Increase
Total no. of diagnosticTotal no. of diagnostic procedures / procedures / 1000 patients1000 patients 19601960 8008001160116059 Reduction59 Reduction
Fass R, et al Gastroenterol 1998; 115:42-9Fass R, et al Gastroenterol 1998; 115:42-9

Omeprazole Test in NCCPOmeprazole Test in NCCP
Generalizability?Generalizability? Male, veteran populationMale, veteran population High % esophagitis, GERD symptomsHigh % esophagitis, GERD symptoms Pain pattern of frequent chest pain (≥ 3x/wk)Pain pattern of frequent chest pain (≥ 3x/wk) Small numbers, short course treatmentSmall numbers, short course treatment
Medication dosing, strengthMedication dosing, strength
Role of endoscopyRole of endoscopy Reassurance factorReassurance factor Once-in-a-lifetime Barrett’s checkOnce-in-a-lifetime Barrett’s check
IssuesIssues


LA Grade CLA Grade C LA Grade DLA Grade D
One or more mucosal breaks no longer than 5mm, not bridging the tops of mucosal folds
One or more mucosal breaks no longer than 5mm, not bridging the tops of mucosal folds
One or more mucosal breaks bridging the tops of mucosal folds involving <75% of the circumference
One or more mucosal breaks bridging the tops of mucosal folds involving <75% of the circumference
One or more mucosal breaks bridging the tops of mucosal folds involving >75% of the circumference
One or more mucosal breaks bridging the tops of mucosal folds involving >75% of the circumference
One or more mucosal breaks longer than 5mm, not bridging the tops of mucosal folds
One or more mucosal breaks longer than 5mm, not bridging the tops of mucosal folds
LA Grade BLA Grade BLA Grade ALA Grade A
Los Angeles (LA) Grade Los Angeles (LA) Grade Classification of Erosive EsophagitisClassification of Erosive Esophagitis
Lundell et al. Gut. 1999;45:172-180.Lundell et al. Gut. 1999;45:172-180.

The spectrum of heartburn frequency The spectrum of heartburn frequency and severity is similar in GERD patients and severity is similar in GERD patients
with and without esophagitiswith and without esophagitis
Severe
Moderate
Mild
Patients without esophagitisSeverity ofheartburn
Smout 1997
Patients with esophagitis

GERD Therapeutic OptionsGERD Therapeutic Options
ProkineticsProkinetics
OTC or prescription OTC or prescription H2RAsH2RAs
““First - aid” : Life-First - aid” : Life-style modifications style modifications
and antacidsand antacids
Endoscopic techniquesEndoscopic techniques
(plication, RF, implant)(plication, RF, implant)
SurgerySurgery
(Lap Nissen fundoplication)(Lap Nissen fundoplication)OTC or prescription PPIsOTC or prescription PPIs
TreatmentsTreatments

Life-style ModificationsLife-style Modifications
Reduce weightReduce weight
Elevate head of Elevate head of bedbed
Stop smokingStop smoking
Eat small meals, no Eat small meals, no late meals, reduce fatlate meals, reduce fat
Consider alternatives to reflux-Consider alternatives to reflux-promoting drugs e.g., theophilline, promoting drugs e.g., theophilline,
anticholinergicsanticholinergics
Avoid reflux-promoting agents e.g, alcohol, coffee; some Avoid reflux-promoting agents e.g, alcohol, coffee; some foodsfoods
Not evidence-basedNot evidence-based
ModificationsModifications


POSITION AND REFLUXPOSITION AND REFLUX
Rig
ht s
ide
dow
nL
eft s
ide
dow
npH
pH
0
0
4
4
8
8
(Katz,LC. Et al, J Clin Gastro 1994;18(4):280-3

GERD HEALING AND ACID CONTROLGERD HEALING AND ACID CONTROL
(Bell et al. Digestion. 1992;51(suppl 1):59-67.)(Bell et al. Digestion. 1992;51(suppl 1):59-67.)
Pa
tie
nts
Hea
led
(%
)P
ati
en
ts H
eale
d (
%)
Duration Intragastric pH >4.0 (Hours)Duration Intragastric pH >4.0 (Hours)
100100
8080
6060
4040
2020
0022 44 66 88 1010 1212 1414 1616 1818 2020 2222

Medical Rx OutcomesMedical Rx Outcomes(with H2RAs)(with H2RAs)
Relief of symptoms Relief of symptoms 50%50% Healing esophagitisHealing esophagitis <50%<50% Prevent complicationsPrevent complications --- --- RemissionRemission 25%25%

Medical Rx Outcomes (PPIs)Medical Rx Outcomes (PPIs)
Relief of symptoms Relief of symptoms 85-95%85-95% Healing esophagitisHealing esophagitis 85-95%85-95% Prevent complicationsPrevent complications 80%80% RemissionRemission 90%90%

GERD: Endoscopic TherapiesGERD: Endoscopic Therapies
Endoscopic suturing – i.e., Endocinch (this Endoscopic suturing – i.e., Endocinch (this leads to partial thickness plication)leads to partial thickness plication)
Full thickness plication – i.e., NDOFull thickness plication – i.e., NDO Radiofrequency ablation – i.e., StrettaRadiofrequency ablation – i.e., Stretta Injection therapy with augmentation of LES Injection therapy with augmentation of LES
– i.e., Enteryx– i.e., Enteryx Bulking procedures with augmentation of Bulking procedures with augmentation of
LES – i.e., GatekeeperLES – i.e., Gatekeeper

BARD EndoCinchBARD EndoCinch
Suction of tissue Suction of tissue just beneath z-linejust beneath z-line
Needle with Needle with pre-loaded pre-loaded suture advancedsuture advanced
Cinching/cutting Cinching/cutting catheter catheter advanced to advanced to tissuetissue
Final appearance Final appearance of plication in of plication in cardiacardia

NDO Plicator™NDO Plicator™
Plicator and gastroscope Plicator and gastroscope retroflexed retroflexed
Arms opened, tissue Arms opened, tissue retractor advancedretractor advanced
Gastric wall retracted, Gastric wall retracted, arms closed.arms closed.
Single, pre-tied implant Single, pre-tied implant deployed.deployed.
Full-thickness plication Full-thickness plication completedcompleted
11 22 33
44 55

Antegrade techniqueAntegrade techniqueBalloon inflationBalloon inflation
Needle deploymentNeedle deployment1 cm above z-line1 cm above z-line

Injection at the Z-LineInjection at the Z-Line

Gatekeeper™ SystemGatekeeper™ System
Stabilize site
ExpansionDeliver prosthesis
Create pocket Access pocket

MAINTENANCE THERAPY OF GERDMAINTENANCE THERAPY OF GERDOmeprazole vs surgeryOmeprazole vs surgery
0102030405060708090
100
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5 5
Years
% in
rem
issi
on
Surgery (N=122)
Omeprazole (N=133)
(Lundel et al: J Am Col Surg, 192:172, 2001)

0
2
4
6
8
10
Sy
mp
tom
Sc
ore
Sy
mp
tom
Sc
ore
So et al. So et al. SurgerySurgery. 1998;124:28-32.. 1998;124:28-32.
Typical Symptoms Typical Symptoms (n=115)(n=115)
Improvement 6.2 points
Atypical Symptoms Atypical Symptoms (n=35)(n=35)
Improvement 4.4 points
Atypical Sx Atypical Sx ImprovementImprovement
• Overall 58% of patientsOverall 58% of patients
– Pulmonary 48%Pulmonary 48%
– Atypical chest pain Atypical chest pain 58%58%
– Pharyngo/Pharyngo/laryngeal 76%laryngeal 76%
Outcomes of Atypical GERD Outcomes of Atypical GERD Symptoms Treated by LNFSymptoms Treated by LNFPreoperative Postoperative

Esophageal Chest PainEsophageal Chest Pain
GERD relatedGERD related
Motility relatedMotility related
Esophageal hyperalgesiaEsophageal hyperalgesia

Esophageal HyperalgesiaEsophageal Hyperalgesia
““Irritable esophagus”Irritable esophagus”
Abnormal nociceptionAbnormal nociception
Lower threshold for painLower threshold for pain

Esophageal HyperalgesiaEsophageal Hyperalgesia
Noxious stimulus in esophagusNoxious stimulus in esophagus
Decrease in nociceptor thresholdDecrease in nociceptor threshold
Disorder of CNS nociceptive Disorder of CNS nociceptive pathwaypathway

Chest Pain - ImipramineChest Pain - Imipramine
50 mg nightly for 3 wks50 mg nightly for 3 wks 52% reduction in chest pain episodes52% reduction in chest pain episodes Suggested visceral analgesic effectSuggested visceral analgesic effect
Cannon R, et al. N Engl J Med 1994; 330:1411-7Cannon R, et al. N Engl J Med 1994; 330:1411-7
15 healthy male volunteers15 healthy male volunteers Balloon inflation volume at pain threshold Balloon inflation volume at pain threshold
higher on imipraminehigher on imipraminePeghini PL, et al. Gut 1998; 42:807-13Peghini PL, et al. Gut 1998; 42:807-13

NCCP Non-GERD NCCP Non-GERD Esophageal TherapiesEsophageal Therapies
Calcium channel blockersCalcium channel blockers AnticholinergicsAnticholinergics NitratesNitrates BotoxBotox Antidepressants (Imipramine, Trazodone)Antidepressants (Imipramine, Trazodone) OctreotideOctreotide BougienageBougienage 5 HT5 HT33 antagonists antagonists

Initial Perception Threshold (S1) Before and 40 Initial Perception Threshold (S1) Before and 40 Minutes after Octreotide InjectionMinutes after Octreotide Injection
BaseBase 40 min40 min00
1010
2020
3030
>30>30
CC
CC
pp < 0.02 < 0.02
Johnson BT, et al Am J Gastroenterol 1999; 94:65-70Johnson BT, et al Am J Gastroenterol 1999; 94:65-70

Maximally Tolerated Pain Threshold (S2) Before and 40 Maximally Tolerated Pain Threshold (S2) Before and 40 Minutes after Octreotide InjectionMinutes after Octreotide Injection
BaseBase 40 min40 min00
1010
2020
3030
>30>30
CC
CC
Johnson BT, et al Am J Gastroenterol 1999; 94:65-70Johnson BT, et al Am J Gastroenterol 1999; 94:65-70

Overlap Syndrome of Altered Pain Overlap Syndrome of Altered Pain SensitivitySensitivity

Approach to the NCCP PatientApproach to the NCCP Patient
Take a historyTake a history Exclude coronary / cardiac diseaseExclude coronary / cardiac disease Check for musculoskeletal diseaseCheck for musculoskeletal disease Look for GERDLook for GERD Check for dysmotilityCheck for dysmotility Consider esophageal hyperalgesiaConsider esophageal hyperalgesia Collaborative managementCollaborative management