View Full Screen - respiratory-care-sleep-medicine...
37
Our digital editions give you two unique ways to view content. The “Full Screen” option makes it easy to flip through and read each spread while the “Fit to Screen” option gives you the ability to scan thumbnails of multiple pages at once, run content searches and more. VIEW FULL SCREEN Click on the “View Full Screen” button to enlarge the digital edition to full size. All of your controls will be shown at the bottom of the page. Bottom Left • Print Page: Allows you to select specific pages or print the entire digital edition. • Fit to Window: Returns you to your original view with the navigation bar on the left. • Table of Contents: Automatically takes you to the issue’s table of contents. Bottom Right • Magnifying Glasses: Enable you to zoom in or out. • Arrows: Take you to the previous page or the next page. • Go to Page: Prompts you to enter the number of the page you want to view. • Subscribe: Takes you to a secure site where you can sign up for your FREE subscription. FIT TO WINDOW In this view, the “Fit to Window” button will be replaced with the “View Full Screen” button. You’ll also have a navigation bar on the left side of the screen. Left Navigation Bar • Pages: Features a thumbnail of every page. Click on one of the thumbnails to go directly to that page. • Bookmarks: Includes important pages that have been bookmarked. Click on one of the bookmarks to go directly to that page. • Search: Allows you to enter a word or phrase and search the digital edition for it. • How To: Offers supplementary documents with helpful tips and information. INTERACTIVE FEATURES • Enlargement Features: Look for this magnifying glass logo attached to photos and figures. Click and hold the mouse down to enlarge for easier reading. • End-of-article Extras: Look for the "black box" after articles that will refer you to related content on the Executive Insight web site . • Ads and Advertiser Index: Click on any advertisement or any company listed in our comprehensive advertiser index to visit their website. • Table of Contents: Click on any listing in the table of contents to be take directly to the article.
-
Upload
nguyendung -
Category
Documents
-
view
217 -
download
3
Transcript of View Full Screen - respiratory-care-sleep-medicine...
Our digital editions give you two unique ways to view content. The “Full Screen” option makes it easy to flip through and read each spread while the “Fit to Screen” option gives you the ability to scan thumbnails of multiple pages at once, run content searches and more.
View Full ScreenClick on the “View Full Screen” button to enlarge the digital edition to full size. All of your controls will be shown at the bottom of the page.Bottom Left• Print Page: Allows you to select specific pages or print the entire digital edition.• Fit to Window: Returns you to your original view with the navigation bar on the left.• Table of Contents: Automatically takes you to the issue’s table of contents.
Bottom Right• Magnifying Glasses: Enable you to zoom in or out.• Arrows: Take you to the previous page or the next page.• Go to Page: Prompts you to enter the number of the page you want to view.• Subscribe: Takes you to a secure site where you can sign up for your FREE subscription.
Fit to windowIn this view, the “Fit to Window” button will be replaced with the “View Full Screen” button. You’ll also have a navigation bar on the left side of the screen.
Left Navigation Bar
• Pages: Features a thumbnail of every page. Click on one of the thumbnails to go directly to that page.
• Bookmarks: Includes important pages that have been bookmarked. Click on one of the bookmarks to go directly to that page.
• Search: Allows you to enter a word or phrase and search the digital edition for it.
• How To: Offers supplementary documents with helpful tips and information.
interactiVe FeatureS• Enlargement Features: Look for this magnifying glass logo attached to photos
and figures. Click and hold the mouse down to enlarge for easier reading.
• End-of-article Extras: Look for the "black box" after articles that will refer you to related content on the Executive Insight web site .
• Ads and Advertiser Index: Click on any advertisement or any company listed in our comprehensive advertiser index to visit their website.
• Table of Contents: Click on any listing in the table of contents to be take directly to the article.

1ADVANCE for Healthcare Careers

909 N. Kellogg St. · Kennewick, WA 99336(800) 245-3001 · (509) 735-6481 ph · (509) 783-6503 fx
www.cadwell.com · [email protected]
Advancing medicaltechnology to help you, help others. Join us on:
© 2012 Cadwell. All rights reserved.
Cadwell is revolutionizing the process of collecting Ambulatory EEG and PSG recordings outside of the laboratory with the addition of our NEW Q-Video® Mobile™ solution. Capture digital video and waveform
data in transit, in the home or in the workplace.
Go Anywhere. Scan the QR code or browse to
www.cadwell.com/qvm for more information or to request contact from a representative.
The information contained in this advertisement is subject to change without notice.
Go Anywhere
contact from a rept contact from a
NOWSHIPPING!
2 ADVANCE for Healthcare Careers
50 Alliance Blvd., Barrie, ON., Canada L4M 5K3 ISO 13485
1-705-726-9383 email: [email protected] www.oxyarm.com
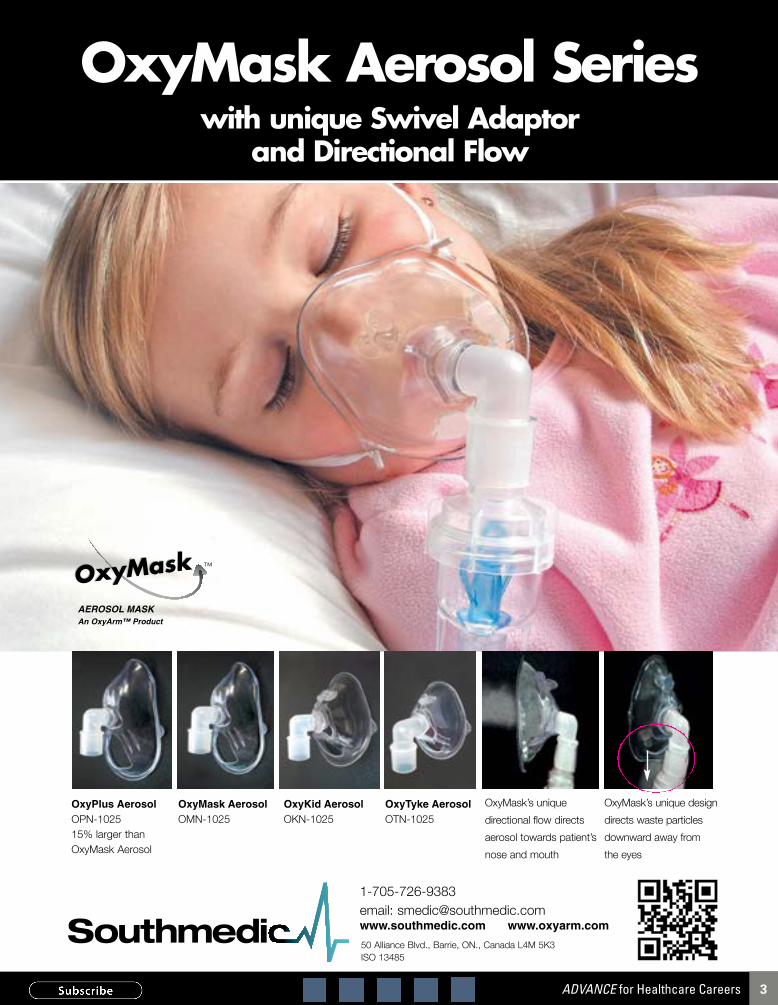
OxyMask Aerosol Serieswith unique Swivel Adaptor
and Directional Flow
™
An OxyArm™ Product
OxyMask’s unique design
directs waste particles
downward away from
the eyes
OxyMask’s unique
directional flow directs
aerosol towards patient’s
nose and mouth
OxyKid AerosolOKN-1025
OxyMask Aerosol OMN-1025
OxyPlus Aerosol OPN-102515% larger thanOxyMask Aerosol
AEROSOL MASK
OxyTyke AerosolOTN-1025
3ADVANCE for Healthcare Careers

DepartmentsNAMDRC Watch …………………… 8Physicians Roundtable ………… 10Allergies & Asthma ……………… 19Education Opportunities ………29Classified Employment …………32
proDuctsAdvertiser Index …………………… 6ADVANCE Healthcare Shop …28ADVANCE Custom Promotions … 31
■ contents
It’s time to celebrate! October is our favorite month of the year because we get two opportunities to thank our community during Sleep Technologist Appreciation Week and Respiratory Care Week. With the first celebration
drawing to a close, it is respiratory therapists’ turn to celebrate with certificates, e-cards, and games. Look for more ways to acknowledge your colleagues at http://respiratory-care-sleep-medicine.advance-web.com/Respiratory-Care-Week/default.aspx.
pharmaceutical GuideRefer to this comprehensive listing, organized by indication, of commonly used respiratory and sleep drugs. Visit advanceweb.com and click “Products & Services Resources” under the Specialty menu, beginning Oct. 18.
Historical case study: andrew JacksonFrom the time he was a 13-year-old prisoner during the Revolutionary War until he died at age 78, Andrew Jackson, war hero, statesman and seventh U.S.
president (1829-1837) endured a seemingly unending series of pulmo-nary illness and injury. Discover how modern medicine could have changed his outcome, beginning Nov. 2.
partnering With a Dental sleep providerWorking as a team with sleep centers, appropriately trained dentists can help improve outcomes for patients with sleep apnea. Discover how to find a dental sleep partner who follows the rigorous standards developed by the American Academy of Dental Sleep Medicine. Click on “Sleep Medicine” under the “Specialty” menu at advanceweb.com/respiratory.
www.advanceweb.com/respiratory
PUBLISHER - Ann Wiest Kielinski; GENERAL MANAGER - W.M. “Woody” Kielinski; Chief Information Officer - Bob Mozenter; EDITORIAL - editor: Judi Biederman senior associate editor: Kristen Ziegler; Web manager: Jennifer Montone; DESIGN - Vice president, Director of creative services: Sue Basile; Design Director: Walt Saylor; multimedia Director: Todd Gerber; art Director: Doris Mohr; senior Graphic artist: Aaron Roshong; ADvERTISING - Director of marketing services: Christina Allmer, art Director: Chris Wofford; EvENTS - public relations Director: Maria Senior; Job Fair manager: Laura Smith; events product manager: Mike Connor; ADMINISTRATION - Vice president, Director of Human resources: Jaci Nicely; Information & Business systems Director: Ken Nicely; circulation manager: Maryann Kurkowski; Billing manager: Christine Marvel; subscriber services manager: Vikram Khambatta; MEDIA & MAR-kETING OPPORTUNITIES: Vice president, media sales: Amy Turnquist; Display Advertising - corporate sales manager: Kevin Miller; national account executive: Hilary Druker; account executive: Andrea O’Brien; Education Opportunities - sales manager: Ed Zeto; Healthcare Facility Advertising - Group manager: Mark Murphy; senior account executives: Steve McCafferty; account executives: Chip Meiers, Denni Morris, Kim Reiner; CUSTOM PROMOTIONS - sales manager: Mike Kerr; senior account executives: Noel Lopez, Sue Borjeson-Romano; sales associates: Kristen Erskine, Danielle Lasorda, Gina Willett
■ onLIne contents
tHIs montH’s HIGHLIGHts
Free WeBInars
sleep Whisperers: Desensitization for pediatric nIVHow can you increase non-invasive ventilation adherence in children and adolescents? Join an Oct. 15 webinar to hear about the protocol used at Children’s Hospital Colorado to desensitize pediatric patients.
Becoming copD preparedJoin Brian Carlin, MD, for a Nov. 8 webinar on developing effective strategies for the early detection, appropriate diagnosis, and correct treatment has taken on new importance.
Register for these webinars and check out educational events for the entire year at advanceweb.com/respiratory_sleep_webinars.
Respıratory Care& Sleep Medicine
advance for
Respıratory Care& Sleep Medicine
advance forseptemBer/ octoBer 2012Volume 21 / Number 5
Copyright 2012 by Merion Publications Inc. All rights reserved. Reproduction in any form is forbidden without written permission of publisher. ADVANCE for
Respiratory Care & Sleep Medicine is published 6 times a year on a bimonthly basis by Merion Publications Inc., 2900 Horizon Drive, P.O. Box 61556, King of Prussia, PA 19406-0956. Send address changes to: Circulation, Merion Publications Inc., ADVANCE for Respiratory Care & Sleep
Medicine, 2900 Horizon Drive, P.O. Box 61556, King of Prussia, PA 19406-0956.
COLORS: 268 PURPLE / 7482 GREENFONT: CENTURY GOTHIC
coVer story
20 National Respiratory Achievement Awards ADVANCE honors the nation’s best respiratory department, manager and practitioner. By Kristen Ziegler
Feature
12 Aerosolized Drug Delivery in Mechanical Ventilation Consider factors that may influence therapy in order to optimize treat-ment for critically ill patients. By Arzu Ari, PhD, RRT, PT, CPFT, FAARC
24 Dental Dynamics in OSA Treatment Physicians and dentists can work together in providing optimal care to patients with obstructive sleep apnea. By B. Gail Demko, DMD
30 Simplifying and Improving Patient Care A case study on oxygen masks shows that oxygen flow, quick assessments, and easy adjustments find favor with RTs and nurses. By Lisa Kinler, RRT
AA
RO
N R
OS
HO
NG
/iS
TO
CK
PH
OT
O/T
HIN
KS
TO
CK
4 ADVANCE for Healthcare Careers

5ADVANCE for Healthcare Careers

Get the info you need by logging on to: www.advanceweb.com/respiratoryOur searchable online Resource Directory allows you to access detailed information about the companies listed below and the products or services they offer. Submit requests for free info.
support the companies that support your profession. The companies listed below support the respiratory care and sleep professions by placing advertisements in ADVANCE for Respiratory Care & Sleep Medicine. Their support keeps our publication coming to you free of charge. Please visit these advertisers’ websites to learn more about their products or services.
■ aDVertIser InDex
Editorial Advisory BoardGerard J. Criner, MDDirector of RICU, Ventilator Rehabilitation Unit and Critical Care Services, Temple Univer-sity Hospital, Philadelphia
Michael Cutaia, MD, Chief of Pulmonary and Critical Care, New York Harbor Health Care System, New York City
Andrew DesRosiers, MS, RRT, RPSGT, Director of the Caritas Centers for Sleep Medicine, Caritas Christi Health Care, Methuen, MA
Terry DesJardins, MEd, RRTProfessor Emeritus, Parkland College, Champaign, IL
Michael J. Hewitt, RRT-NPS, RCP, FAARC, FCCM, Independent Consultant, Tampa, FL
Lana Hilling, RCPCoordinator of Lung Health Services, John Muir Health, Concord, CA
Felix Khusid, RRT-NPS, RPFTAdministrative Director for Respiratory Therapy and Pulmonary Physiology Center, New York Methodist Hospital, New York City
George W. Lantz, MPS, BS, RRT, CPFT, AE-C, FAARCClinical Manager of Respira-tory Care, EKG, and Special Diagnostics, Doctors Hospital, Augusta, GA
Vernon R. Pertelle, MBA, RRT
Vice President of Clinical Operations, Catholic Health Initatives, Denville, NJ
Michael McPeck, BS, RRT, FAARC, Executive Director of Respiratory Care Services, Long Beach Memorial Medical Center/Miller Children’s Hospital, Long Beach, CA
Thomas F. Plaut, MD, FAAPPresident, Pedipress Publishers, Amherst, MA
Alphonso A. Quinones, DHA(C), MA, CHE, RRT-NPS, RPSGT, RPFT, CCT, AE-CDirector of Respiratory Therapy, North Shore University Hospital, Manhasset, NY
John A. Sestito, BA, RRTAssociate Executive Direc-tor, Clinical Practices of the University of Pennsylvania, Department of Neonatol-ogy and Newborn Services, Philadelphia
Helen Sorenson, MA, RRT, FAARC, Associate Professor, Department of Respiratory Care, UT Health Science Center, San Antonio, TX
Jeffrey L. Tarnow, RRT, RCPAdult Clinical Coordinator of Respiratory Care Services, Clinical Research Coordinator Department of Anesthesiology, University of California, San Francisco
Kimberly Trotter, MA, RPSGTPractice Manager, UCSF Sleep Disorders Center, Pulmonary Function Lab at Mount Zion, San Francisco
Editorial ConsultantsGeorge G. Burton, MD, FCCP, FAARC, Medical Director, Sleep Disorders Center Kettering Medical Center Kettering, OH
Allen Goldberg, MD, MBA, Master FCCP, Past-president American College of Chest Physicians, Chicago
Industry Advisory BoardJohn Ancy, MA, RRTSenior Clinical Consultant Instrumentation Laboratory
Bill Antilla, RPSGTSenior Product ManagerCadwell Laboratories
David BakerPresident and CEOEmbla
Richard A. Bonato, PhDPresident and CEOBRAEBON Medical Corp.
Krystanne BorgenManager, Marketing CommunicationsnSpire Health Inc.
Steve Chaucer, RRTNational Sales Manager Hamilton Medical Inc.
Edwin Coombs, MA, RRTAssociate Director of MarketingRespiratory Care SystemsDraeger Medical
Terry deBruyn, RRTSales Manager for Specialty MarketsNonin Medical Inc.
Louis Fuentes, RRTClinical Marketing SpecialistMaquet Inc.
Jeff KuzniaDirector, Business DevelopmentCompumedics Limited
Natalie Morin, RPSGTPresident and CEOSleep Strategies Inc.
Peggy Powers, RRTClinical Product SpecialistFisher & Paykel Healthcare
Mark Rizk, RPSGTBusiness Unit Manager, Sleep Products Nihon Kohden America
Judy Tietsort, RN, RRT, FAARCCEO, Respiratory Management Consultants
Stan Van GentVice President for Global Product Marketing for Ventilation and AirwayCovidien
Michael Waldman, BBAMarketing Product ManagerPARI Respiratory Equipment Inc.
■ aDVIsory BoarDs
Looking for a new job? now you can get job postings on Facebook and twitter! Follow us at twitter.com/AdvanceRTJobs and facebook.com/AdvanceRespCare to search for respiratory care and sleep jobs.
❏ ADVANCE Healthcare Shop www.advancehealthcareshop.com 28
❏ ADVANCE Custom Promotions www.advancecustompromotions.com 31
❏ Airway Management Inc. www.tapintosleep.com 25
❏ Braebon Medical Corp. www.braebon.com 27
❏ Cadwell Laboratories Inc. www.cadwell.com 2
❏ Cleveland Medical Devices Inc. www.clevemedsleepview.com 13
❏ Compumedics USA Inc. www.compumedics.com 5
❏ Fisher and Paykel Healthcare www.fphcare.com 11
❏ GE Healthcare Systems www.gehealthare.com/respiratorycare 23
❏ Hill-Rom Services Inc. www.hill-rom.com 15-18, 36
❏ Independence University www.independence.edu 29
❏ Instrumentation Industries www.iiimedical.com 10
❏ MAQUET www.maquetusa.com 21
❏ Med Way www.ssbinc.com/medway 29
❏ Meditrack Products www.doser.com 10
❏ Micro Direct www.micro-direct.com 26
❏ Mid-Atlantic School of Sleep Medicine www.schoolofsleepmedicine.com 30
❏ nSpire Health Inc. www.nspirehealth.com /connected 9
❏ Respiratory Delivery Systems www.rdsusa.com 19
❏ Southmedic Inc. www.southmedic.com 3
❏ The Compliance Team www.thecomplianceteam.org 7
❏ Ventus Medical Inc. www.proventtherapy.com/hcp 35
DON’T LET YOUR SUBSCRIPTION
EXPIRE!There are many reasons to renew your subscription to ADVANCE.
Here are three of them.
1. FREE: Magazines, e-newsletters, websites, events, career advice
2. FLEXIBLE: Print or digital subscriptions, in-person or virtual events, breaking news
or archived articles
3. FAST: Call or renew online
SUBSCRIBE OR RENEW TODAY. Call 800-355-1088 (M-F, 8am-6pm ET)
Visit advanceweb.com/General/Subscriptions.aspxThank you for taking the time to renew your FREE subscription.
NOT SURE WHEN YOUR SUBSCRIPTION WILL EXPIRE?
Check the mailing label on the front of this magazine to fi nd
your expiration date.
6 ADVANCE for Healthcare Careers
Accreditation simplified.
p The first customizable sleep center accreditation from a Medicare deemed (DMEPOS) accreditation organization to focus on day-to-day business operations in addition to sleep study protocols that includes a complete organizational review and scoring — providing a single-source solution to your accreditation needs.
p Web-based satisfaction surveys for documenting Patient Outcomes and Benchmarking to peers. Our dramatically simplified accreditation process for sleep centers is operations-driven and focused on what matters most to patients — Safety-Honesty-Caring®.
p Industry leading plain language quality standards and expert mentors guide sleep professionals through implementation of the program while covering all aspects of your business.
Here’s just a few of our value-added features:
215.654.9110 | [email protected] | www.TheComplianceTeam.org
The Compliance Team has been leading the healthcare accreditation simplification movement since 1998. Our Exemplary Provider™ accreditation programs for sleep centers and DMEPOS promote healthcare delivery excellence through the implementation of sustainable quality improvement processes that are not difficult, time consuming, or costly to realize.
Healthcare accreditation organization.
7ADVANCE for Healthcare Careers

8 ADVANCE FOR RESPIRATORy CARE & SLEEP MEDICINE september/october 2012 www.advanceweb.com/respiratory
In AprIl 2013, the National Association for Medical Direction of Respiratory Care (NAMDRC), in cooperation with the American Thoracic Society (ATS), American College of Chest Physicians (ACCP), American Association for Respiratory Care (AARC), COPD Foundation and the National Home Oxygen Patients Association (NHOPA), will convene the Pulmonary Medicine Health Policy Summit in Washington, D.C. The goal of the summit is to address pulmonary medicine issues that lend themselves to regu-latory and/or legislative solutions. A detailed strategic roadmap will be developed and shared broadly within the pulmonary medicine community.
The issues to be addressed have been vetted by the respective societies and will involve several hours of discussion from experts, including members of Congress and their staffs, represen-tatives of regulatory agencies and nationally recognized experts in the respective specific issues. These initial discussions are open to physicians, allied health professionals, patients, policy experts and representatives of industry.
Discussion topics will include:Performance measures for pulmonary medicine: The societies agree that pulmonary medicine is not moving forward as swiftly as other segments of the medical community and that this slower pace might lead to other entities, such as the American Medical Association or the National Quality Forum, developing performance measures without direct, coordinated input from the pulmonary medicine community. By itself, this situation may not be too problematic, but as the health-care delivery system shifts away from the traditional fee-for-service model to one sig-nificantly more focused on quality measures and payment tied to identifiable outcomes, it is critical that the pulmonary medicine com-munity immerse itself in these broad
initiatives. As we look forward to the likelihood of COPD hospital readmissions as a quality measure, it is incumbent upon pulmonary medicine to take an active role in planning for its own future.
COPD as a public health issue: When comparisons are made to the impact of COPD on the economy compared to other chronic diseases such as diabetes or AIDS, most would agree that research to address COPD, the third leading cause of death in the United States, is woefully inadequate.
However, integral to any discussion of COPD research is actual management of the disease. There is a problematic lag time from the onset of symptoms to the diagnosis of COPD. With an estimated 12 million undi-agnosed patients, management of COPD is a public health issue that does not lend itself to easily recognized or implemented solutions by the public or private sectors.
Telemedicine for pulmonary-related diseases: The broad issue of telemedicine is regarded as part of larger solutions to rising healthcare costs and access to healthcare ser-vices. It is the view of the societies that pul-monary medicine needs to focus on tele-medicine applications unique to pulmonary medicine, crossing a wide spectrum of settings including the critical care unit, nursing home and home. The growing issue of readmissions creates significant pressure to develop home monitoring strategies for pulmonary-related health issues, and patient compliance with in-home treatment plans is integral to the discussion. It is critical that the pulmonary community move this facet of medicine forward with aggressive and direct initiatives.
Documentation/EHR: The pulmonary community must deal with documentation issues that have surfaced across various clini-cal settings, including the hospital inpatient, hospital outpatient and home care settings. For example, documentation requirements
imposed on physicians ordering oxygen, CPAP, and nebulized drugs have raised serious access concerns. While some solutions, such as broad implementation of an electronic health record, might alleviate problems with the corollary audits tied to apparent lack of documentation, pulmonary issues warrant specific attention.
Oxygen payment reform: Medicare expenditures for long-term oxygen therapy account for the largest single item under the durable medical equipment benefit. The current payment methodology is more than 25 years old and has not kept up with new technologies, some of which have been available for more than a decade. The current payment system awards the greatest payment for the cheapest devices (stationary concentrators) and the lowest payment for newer, standard-of-care, portable devices. This can lead to problematic access issues as providers find it difficult to shift their inventories of large cylinders to more clinically appropriate systems.
Improving this situation is complicated by the realities of competitive bidding and a structure that requires providers to bid on payment for specific codes. Any change to payment formulas would unquestionably be chaotic to that program, but serious questions surrounding access and clinical appropriate-ness of device selection are driven by the current payment dichotomy.
For more information and to register for the Pulmonary Medicine Health Policy Summit, call (703) 752-4359 or visit www.namdrc.org. ■
Phil Porte is executive director of the National Association for Medical Direction of Respiratory Care (NAMDRC).
national SummitExperts from across the country will meet to discuss strategic regulatory and legislative approaches for pulmonary health issues.
■ namDrc WatcH By Phil Porte
This column is a joint venture of ADVANCE and NAMDRC. For information, write to NAMDRC, 8618 West-wood Center Dr., Suite 210, Vienna, VA 22182, visit their website at www.namdrc.org, or
call the staff at (703) 752-4359, by fax at (703) 752-4360, or by email at [email protected].
8 ADVANCE for Healthcare Careers
HIS/EMR
PFT LabOrders / ADT
Testing
PFT LabWorkflow
Optimization
Review StationReportsAttachmentsDigital Signatures
Remote ClinicSpirometry Shared Database
Connected PFT EnterpriseThe
Now, with nSightTM
software from nSpire Health, you can share your Pulmonary Function Testing with the Enterprise...
Your mother always told you to share.
Learn how your PFT system can process PFT orders from billing, centralize configuration & test data from remote offices, review & sign electronically, and streamline your workflow:
See us at CHEST 2012 in Atlanta, booth 1045
See us at AARC 2012 in New Orleans, booth 1316
Visit www.nspirehealth.com/connected
Call 800.574.7384
EMR/HIS connectivitynet
TM
streamlined PFT testing software rapid remote data accesswebeb
Now, with nSight software from nSpire Health, you can share yourNow with nSightTM
software from nSpire Health you can share your
Your mother always told you to share.Your mother alllways told you to shareYour mother always told you to share.Your mother always told you to share.
powered by iFlow
TM
Inspiring Respiratory Health
9ADVANCE for Healthcare Careers

When robert DemerS, bS, rrt, stumbles across an interesting case, he knows there’s one person he can call, day or night: his daughter Kristen. As a fellow respiratory therapist, she’s equally enthralled with stories of using advanced modes of ventilation and harrowing transports.
Not all respiratory therapists are lucky enough to have a relationship like Demers’. But a new social media network from the American College of Chest Physicians can give them the instant interaction with like-minded clinicians they crave.
The ACCP e-Community is a private, secure network where clinicians can connect to discuss clinical issues, create and answer polls, and share resources such as videos, photos, slideshows, and links to journal articles. They also can search for other e-Community members by institutions, specialty, or clinical interest, and subscribe to receive content alerts via email or RSS feed.
“It’s just so timely and tangible to talk about issues or procedures to see what is new or what is coming down the pike,” said Demers, former president of the American Association for Respiratory Care and a member of the e-Community.
For example, after a particularly eventful shift that had him using an intensive care unit ventilator interfaced to an e-cylinder of oxygen to apply airway pressure release ventilation to transport a patient with a failed stent in the left anterior descending coronary artery (aka the widow maker), Demers created and posted a 26-minute video about using the ventilation mode. The video started a lively discussion on the ACCP e-Community.
“It gave me a good idea of how conversant most physicians are with the mode,” said Demers, who also is the incoming chair of the ACCP’s Allied Health NetWork.
The e-Community also is hooked into the ACCP’s NetWorks, the special interest groups that focus on particular areas of chest medicine and whose members participate in the development of policies, opinions and position statements af-fecting the field. Members will be using the platform to supplement their phone calls, emails and open discussions at the annual CHEST meeting.
The ACCP e-Community is open to any ACCP member who is part of an ACCP Network, and while Demers initially had some doubts about whether it would catch on (“Like me, a lot of physicians were born long before the advent of the digital revolution,” he said), the e-Community is already flourishing. As of early October, more than 4,500 professionals have logged in to the e-Community.
To connect with the e-Community, log on to your ACCP profile and join a NetWork. You’ll receive an e-Community invitation via email within one week. ■
Kristen Ziegler can be reached at [email protected].
Instant InteractionThe new ACCP e-Community gives clinicians access to peers and the latest research
■ pHysIcIan rounDtaBLe By Kristen Ziegler
Physicians Roundtable is a joint venture of ADVANCE and the American College of Chest Physicians. For more information on ACCP activities and offerings, contact Megan Schagrin, CAE, CFRE, at (847) 498-8314. For membership information, call Suzanne Sletto at (847) 498-8359, or write to ACCP, 3300 Dundee Road, Northbrook, IL 60062-2348. You also can reach the ACCP online at www.chestnet.org or email [email protected].
Counter for MDI Inhalers
The DOSER is a lightweight electronic counter that easily attaches tothe top of an MDI. It automatically counts down each time an inhalationis taken. The remaining number of doses in the canister are displayedon the LCD screen. Dose history is displayed on screen and a warning
sound is given when only 20 doses remain in the canister.Call Free: 1-800-863-9633
MediTrack Products, 448 Turnpike St., Ste. 1-B, S. Easton, MA 02375
WWW.DOSER.COM
DOSER byMediTrack Products
No More Guesswork
Ideal Product for Keeping Track of theMedicine in your Inhaler
& Common Canister ProtocolUsed by Over 400 Hospitals and Asthma
Organizations !
InhalationsRemaining
History
10 ADVANCE for Healthcare Careers

Designed to Perform – in Tune with You
The F&P Eson is designed to perform in tune with you and your needs. The F&P Eson’s three key components, the RollFit™ Seal, ErgoFit Headgear and Easy Frame work in harmony and have been designed to deliver the comfort, seal and easy use that Fisher & Paykel Healthcare masks are known for. This compact nasal mask is packed with technological innovations orchestrated to provide effective CPAP therapy.
For more information please call 1800 446 3908 or visit www.fphcare.com
Nasal Mask
Experience the F&P Eson nasal mask for:
• Easy Fit• Easy Comfort• Easy Clean
11ADVANCE for Healthcare Careers
AeroSol therApy is a common practice in mechanically ventilated patients who suffer from dyspnea and bronchoconstriction. The effective-ness of aerosol therapy depends on several factors such as aerosol device, drug, ventilator parameters, and circuit.1-4 Clinicians without the necessary knowledge and experience about these factors may not be able provide effective aerosol therapy in ventilator-dependent patients. Therefore, it is important to understand all the factors influencing aerosol therapy during mechanical ventilation in order to optimize aerosol drug delivery in critically ill patients.
aerosol Device InfluencesThe types of aerosol devices, their placement in the ventilator circuit, and administration technique of aerosol therapy affect drug delivery in ventilator-dependent patients. There are two types of aerosol devices used in mechanical ventilation—nebulizer and pressurized metered-dose inhalers (pMDI)— and aerosol therapy can be administered through jet, mesh, or ultrasonic nebulizers. Not only the type of nebulizer, but also different batches of the same brand impact aerosol deposition.5-7 For instance, mesh and ultrasonic nebulizers have smaller residual volumes compared to jet nebulizers; therefore, they are more efficient than jet nebulizers. 2,4,8,9,10,11 Also, they operate with electricity, unlike jet nebulizers which require compressed air or oxygen to generate aerosols.12
The placement of an aerosol device in the ventilator circuit impacts aerosol deposition during mechan-ical ventilation. A 2010 study reported that the deposition efficiencies of the pMDI, ultrasonic and mesh nebulizers are best when they are placed 15 cm away from the “Y” adapter, while placement of the jet nebulizer prior to the humidifier improves aerosol drug delivery during mechanical ventilation.10,11 When the jet nebulizer is placed further away from the endotracheal tube, continuous aerosol output from the jet nebulizer charges the ventilator circuit's inspiratory limb between inspirations and improves drug output delivered with each breath.10,11
The administration technique of aerosols also inf luences aerosol drug delivery to mechanically ventilated patients. For instance, jet nebulizers may be connected to a ventilator with the intermittent nebulization function, which operates the nebulizer only in inspiration and
minimizes aerosol loss during expiration. Studies showed that intermit-tent nebulization increases aerosol drug delivery more than continuous nebulization during mechanical ventilation.13,14 Another example is offered by pMDI. When the actuation of pMDI is synchronized with the beginning of inspiration, aerosol drug delivery is maximized.15 Using a chamber-shaped spacer with the pMDI increases the efficiency of aerosol therapy up to sixfold compared to elbow adapter or unidirec-tional inline spacer.16 Also, it is very important to shake and prime the pMDI before the treatment, especially prior to first use and when it has not been used for more than 24 hours. Otherwise, the drug in the pMDI formulations may separate from propellants and cause a reduction in aerosol deposition up to 35 percent.17
Drug InfluencesUsing bronchodilators in ventilator-dependent patients is a widespread practice. While bronchodilators improve respiratory mechanics of mechanically ventilated patients with COPD, use of inhaled cortico-steroids (ICS) and their appropriate doses have not been determined for patients on mechanical ventilators. 18-20 Also, experience with broncho-
dilator and ICS combination therapy is limited, and the cost of such therapies would be high—especially when higher doses are needed.
Ventilator parameter InfluencesVentilator parameters such as mode, tidal volume, inspiratory time, flow rate, and trigger sensitivity (bias flow) affect aerosol drug delivery in mechanical ventilation. For example, the ef-ficiency of aerosol therapy in mechanically ventilated patients
varies with the modes of ventilation. Aerosol delivery through the nebulizer is lower in pressure-controlled ventilation than in
volume-controlled ventilation that is used for the treatment of critically ill patients with low compliance and low resis-
tance.21 Also, spontaneous modes such as continuous positive airway pressure (CPAP) increase aerosol
delivery up to 30 percent compared to controlled breaths of equivalent tidal volume.22
It is important to set the tidal volume larger than the volume of ventilator tubing and
artificial airway in order to increase the efficiency of aerosol therapy during me-
chanical ventilation. Although setting the tidal volume greater than 500 mL in adults improves aerosol drug deliv-
ery, clinicians also should note that tidal volumes greater than 8-10 mL/kg can
Aerosolized Drug Delivery in mechanical VentilationConsider factors that may influence therapy in order to optimize treatment for critically ill patients.
■ VentILatIon toDay By Arzu Ari, PhD, RRT, PT, CPFT, FAARC
12 ADVANCE for Healthcare Careers
SleepView®
Monitor + Web PortalEasy to usewith new all-inclusive rental option
1•877•CLEVEMED (1•877•253•8363 )www.C levemedSleepv iew.com
Expanding the reach of your sleep services today and tomorrow
Smallest, lightest home sleep monitor utilizing
traditional sleep lab methodology. Meets AASM
guidelines to assess sleep disordered breathing.
Type III, 8-channels
• Heart rate
• Pulse oximetry
• Respiratory airflow
• RIP respiratory effort
• Snore
• Body position
• Thermal airflow
• Actigraphy
Acquire good data with Sensor Check to ensure
proper data collection during testing. Save
time with Smart Check to validate quality of
the recorded sleep study before SleepView® is
returned to the provider.
SleepView™Web Portal is HIPAA compliant and
allows seamless, secure access to patient’s raw
sleep data for scoring and interpretation.
Rental option detailsOne price for three months of home sleep testing:Home Sleep Monitor + Starter Kit Unlimited: Sleep Study Kits + Web Portal access
13ADVANCE for Healthcare Careers

■ VentILatIon toDay
CELEBRATE SLEEP’SFINEST
GAIN RECOGNITION FROM FELLOW PROFESSIONALS AND WIN A CASH PRIZE:
BEST SLEEP TECH: $250
BEST SLEEP MANAGER: $250
BEST SLEEP DEPARTMENT: $500
ENTER ONLINEVisit www.advanceweb.com/respiratory and click
on the National Sleep Achievement Awards ribbon icon
to nominate a tech, manager or department.
SPONSORED BY
Winners will also receive a keepsake plaque to
commemorate their achievements. Plus, ADVANCE for
Respiratory Care & Sleep Medicine will recognize them in
a special section of the magazine and on the website.
If you nominate someone who wins, we’ll send you a
$25 gift certifi cate to the ADVANCE Healthcare Shop!
It’s time to fi nd out who is among sleep’s elite
practitioners. Nominate yourself or someone you
know for the 2013 National Sleep Achievement
Awards Competition from ADVANCE for
Respiratory Care & Sleep Medicine.
ENTRY DEADLINE: FEBRUARY 15, 2013
on the Web Discover the best administration technique for aerosolized drug delivery by jet nebulizer, mesh nebulizer, and pMDI. Click “References & Charts” under the “Resources” menu at advanceweb.com/respiratory.
be detrimental to the lungs and should not be used to increase aerosol deposition in mechanically ventilated patients. 22-24
The duration of inspiratory time (Ti) affects the nebulizer's efficiency as it generates aerosol over time. Longer Ti will help nebulizers have a cumulative effect in optimizing aerosol delivery as opposed to the pMDI, which is not influenced by Ti due to its short aerosol generation time.22 It is also known that high inspiratory flow rates increase turbulent flow leading to inertial impaction of aerosol particles and decrease aerosol de-position during mechanical ventilation. Reducing the peak inspiratory flow rate to 40 to 50 L/min, as long as it is tolerated by patients, will improve aerosol drug delivery in mechanically ventilated adults.22,25
While aerosol delivery with the pMDI is not influenced by the trigger sensitivity (bias flow), the nebulizer is affected by the flow-trigger that dilutes the aerosol and increases the washout of the aerosol into the expira-tory limb between breaths.22 A 2010 study found that increased bias flow decreases the amount of aerosol deposition during mechanical ventilation. The authors also recommended using lower bias flow ≤ 2 lpm in order to improve aerosol drug delivery to mechanically ventilated patients.11
circuit InfluencesThe circuit-related factors include artificial airways, density of inhaled gas, heat and humidity. Artificial airways such as endotracheal tube (ETT) and tracheostomy tube (TT) are used in mechanical ventilation and have a great influence on aerosol deposition. For example, aerosol therapy through ETT is less efficient than TT because TT is shorter than ETT and creates less of a barrier than ETT for aerosol delivery during mechanical ventilation. 26,27 Also, aerosol delivery reduces as the inner diameter of ETT decreases. 28
The density of inhaled gas also influences aerosol drug delivery to critically ill patients. For instance, heliox has low density that creates persistent laminar flow in the airways, decreases particle-impaction losses caused by airflow turbulence and increases aerosol deposition.29-32 However, heliox should not be used to power the nebulizer as it is not effective in aerosolizing the drug. Also, flow rate with heliox should be increased by two folds to improve aerosol delivery during mechanical ventilation.
Heat and moisture exchangers (HMEs) and heated humidifiers are the two types of humidification systems used during mechanical ventilation. Several studies reported that heat and humidity of inhaled gas decrease aerosol deposi-tion by 40 percent due to hygroscopic growth of aerosols in a heated and hu-midified environment.22,33-35 However, bypassing the humidifier is not an option for aerosol therapy during mechanical ventilation because breaking the circuit and waiting for several minutes for the circuit to dry is not desirable.2
In summary, many factors affect aerosol drug delivery in mechanical ventilation. Understanding the impact of all these factors and utilizing the optimum technique are essential in optimizing aerosol drug delivery to ventilator supported patients. ■
View a list of references at advanceweb.com/respiratory.
Arzu Ari, PhD, RRT, PT, CPFT, FAARC, is associate professor, division of respiratory therapy at Georgia State University in Atlanta.
14 ADVANCE for Healthcare Careers
ill-Rom’s participation in respiratory care has a long history. As one of the leading medical sup-pliers of hospital beds and stretchers, Hill-Rom’s background in pulmonary care started at the
bedside with bed surfaces that included rotation therapy to prevent and treat pulmonary complications. Eventually,Hill-Rom acquired Advanced Respiratory, Inc. (ARI) and created a division solely dedicated to the pulmonary market and pulmonary outcomes—Hill-Rom Respiratory Care.
Hill-Rom Respiratory Care supports two innovative products—The Vest® Airway Clearance System and The MetaNeb® System. “As the respiratory care eld has changed,” explains Chad Boerst, vice president and general manager (global) of Hill-Rom Respiratory Care, “the im-portance of pulmonary care has continued to advance over time.” As the industry changes, products like The Vest® System and The MetaNeb® System continue to address issues surrounding airway clearance. As Boerst explains, healthcare has seen an increase in multidisciplinary care teams that focus on the patient’s needs as a whole. A
patient’s pulmonologist, nutritionist and primary care pro-vider must work together to nd a solution.
THE VEST® AIRWAY CLEARANCE SYSTEM
New to the market in 1988, The Vest® System has been in Hill-Rom’s portfolio since the company acquired ARI in 2003. The Vest® System is a medical device for children and adults. The therapy is called High Frequency Chest Wall Oscillation (HFCWO), which creates mini-coughs that dislodge mucus from the bronchial walls, increase mobilization and move secretions toward central airways.
Initially used on Cystic Fibrosis (CF) patients, The Vest®
System now is prescribed for many other respiratory dis-eases and conditions in the acute care setting as well as in the home setting. Now in its fth generation, The Vest®
System quietly provides the most air ow of any HFCWO product on the market today. Prescribed by more than 19,000 physicians, The Vest® System enables therapy com-pliance and positive outcomes.
THE METANEB® SYSTEM
Hill-Rom Respiratory Care’s most recent addition is The MetaNeb® System. A therapeutic device for all ages, The MetaNeb® System off ers three therapies in one device: lung expansion, secretion clearance and aerosol delivery. More impressively, all three therapies can be administered during a single 10-minute treatment. As with The Vest® System (which off ers single patient use garments for the acute care arena), The MetaNeb® System employs a single-patient-use circuit to address cross contamination concerns.
Currently used only in the acute care setting, TheMetaNeb® System uses a systematic approach to enhancing secretion mobilization and resolving or preventing patchy atelectasis. Patients who may bene t include those with asthma, chronic bronchitis and chronic obstructive pulmo-nary disease (COPD), as well as surgical patients requiring
BREATHING EASY THE VEST® AIRWAY CLEARANCE SYSTEM AND THE METANEB® SYSTEM ARE IMPROVING LIVES.
ADVANCE FOR RESPIRATORY CARE & SLEEP MEDICINE | SEPT/OCT 2012
ADVERTORIAL
THE VEST® AIRWAY CLEARANCE SYSTEM: SAFE, EASY TO USE AND EFFECTIVE; AVAILABLE IN THE ACUTE AND HOME CARE SETTINGS.
15ADVANCE for Healthcare Careers
post-operative airway management. Boerst explains that there was a gap in their product line, which The MetaNeb®
System lled.
FUTURE OF AIRWAY CLEARANCE
As healthcare changes, the focus is on readmission reduc-tions, limiting length of stay and improving patient out-comes. The Vest® System and The MetaNeb® System are products designed to support these initiatives. “Our focus is to enhance outcomes for our patients and their caregivers,” says Boerst. “As healthcare changes, there’s only going to be an increased focus on improved outcomes. This is the core of what we do and what we will do in the future.” These products have become a standard part of airway clearance pro-tocols in hospitals throughout the country. All stakeholders—the patients, physi-cians and respiratory therapists—see the fundamental value in these products.
FORSYTH MEDICAL CENTER
According to the Centers for Disease Control and Prevention (CDC), COPD caused an estimated 126,005 deaths in the United States in people older than 25 years in 2005, an 8 percent increase from 2000.
At Forsyth Medical Center, a 900-plus-bed facility, in Winston-Salem, N.C., this statistic is not surprising.With a 46-bed pulmonary unit, For-syth treats individuals with varying pulmonary complications, but COPD
is the most prevalent disease. Forsyth’s pulmonary pa-tient pro le is an older adult battling respiratory com-plications from poor air quality and tobacco use. Typ-ically, pulmonary issues are compounded by existing complications. “Anyone who is not mobile is always a challenge,” explains John Wilson, respiratory clinicalcoordinator at Forsyth. “You take those types of patients and add COPD, bronchitis or pneumonia, and it will mag-nify the challenge.”
To help reduce intensive care unit (ICU) readmissions, Forsyth relies on The Vest® System and The MetaNeb®
System to move secretions and reduce infections. However,readmission reductions are diffi cult to credit to a particular therapy, and if a patient’s pulmonary system is severely compromised they are going to be in the hospital longer, which can result in additional pulmonary issues, explains Wilson.
Wilson was rst introduced to The Vest® System as a student at Wake ForestBaptist Medical Center as the staff was using the The Vest® System on their CF patients. In his current role, Wilson is involved with vendor selection, so his early exposure to the product left a positive impression. Initially, Forsythstarted with older vest models, and now the medical center has nine of The Vest® Systems and eight of TheMetaNeb® Systems.
At Forsyth, any time a physicianorders anything respiratory related,
the patient receives a consult with a respiratory therapist. During the consult, the therapist reviews the patient’s chart, conducts an interview, and completes a physical assessment with the patient. Then the therapist devel-ops a treatment plan based on protocols approved by the medical executive committee. As healthcare changes, the system demands more action with less support – more tri-age, explains Wilson. However, Hill-Rom’s products sup-port this change. “I don’t think one therapy or product is the magic bullet,” says Wilson, “but I think both of these products have given us good tools in our tool box. In fact, they have given us higher-caliber tools.”
And because every patient is diff erent, Wilson and his staff work to nd the right therapy the rst time around. “If you have a patient who follows commands, TheMetaNeb® System works well. If you have a patient who is lethargic or confused, The Vest® System is a good product for them,” says Wilson. Finding the right product is key, as it helps with length of stay (LOS) and readmissions.Currently, LOS at Forsyth is about 4.8 days, looking at all ICU patients. Wilson would love to see an average three-day stay; even a one-day decrease in LOS would savesigni cant money over the course of a year.
MEDICAL CITY DALLAS HOSPITAL
As the Pediatric Respiratory Care Manager at Medical City Dallas Hospital in Dallas, Texas, Steve Acton knows the im-portance of effi cient airway clearance in his pediatric patients.
With a robust pulmonary division, Medical City has been using The Vest® System and The MetaNeb® System for many years. The hospital’s pediatric pulmonary unit takes in many respiratory issues, including CF, pneumonia, bronchiolitis and respiratory syncytial virus (RSV). Medical City also sup-ports a cranial facial program, and many of those children have issues with airway clearance.
To reduce the risk of cross contamination, Medical City has 10 of The Vest® Systems and 10 of The MetaNeb®
Systems designated to speci c hospital rooms to avoidunneeded exposure from room-to-room transfers. In his 11 years at Medical City, Acton believes Hill-Rom prod-ucts reduced pulmonary complications and helped reduce readmission rates.
As healthcare changes, deploying resources eff ectively
and effi ciently is an ongoing challenge. Hill-Rom’s products help to address this issue. “When you do a treatment with The MetaNeb® System, you are doing two concrete thingsinstead of one,” he explains. “The MetaNeb® System deliversa bronchodilator and also helps with secretion clearance at the same time.” Staff members value the product’s ability to deliver multiple therapies in a single device.
As for The Vest® System, the product was amazing tech-nology when it was introduced; it is even more impressive today. “I think both products are going to continue to grow. These technologies have helped to improve the quality of life of our young patients,” he says.
With young patients, hospitals need therapies and treat-ments that produce results and make patients feel comfortable. Acton says that kids respond very well to treatments, even if they have to use two products in the same session. “Often-times, we do a treatment with The MetaNeb® System and The Vest® System in the same session. It helps clear the pneumonia or RSV in these children by mobilizing secretions.”
HOAG MEMORIAL PRESBYTERIAN HOSPITAL
Celebrating 60 years in 2012, Hoag Memorial Presbyterian Hospital, a 579-bed facility, has been a cornerstone of the Newport Beach, Calif., community. As a community-based, not-for-pro t hospital, Hoag is expanding; it added a sec-ond campus in Irvine, Calif., in 2010. In addition, Hoag and St. Joseph Health System formed an affi liation to create a stronger healthcare alliance in Southern California.
Like many other hospitals and healthcare systems throughout the country, Hoag’s Respiratory Care Depart-ment impacts all departments. As Director of Hoag’s Respi-ratory Care Department, Kristin Vercnocke, BS, RRT, knows that “respiratory touches everyone.” She is involved in car-diology, neurology, emergency room, neonatal, Pulmonary Rehabilitation, Pulmonary Function Testing and infection prevention initiatives. In addition, Vercnocke serves on the Readmission Reduction team for pneumonia.
Hoag’s patient pro le varies, but individuals older than 70 with multiple comorbidities and hospital visits in a calendar year use the most resources. Most often, these patients lack social and family support, as well as pallia-tive care planning. Hoag also treats many chronic COPDpatients, who struggle with rebound issues and create
SEPT/OCT 2012 | ADVANCE FOR RESPIRATORY CARE & SLEEP MEDICINE ADVANCE FOR RESPIRATORY CARE & SLEEP MEDICINE | SEPT/OCT 2012
ADVERTORIAL ADVERTORIAL
“Our focus is to enhance outcomes for our patients and their caregivers. As healthcare changes, there’s only going to be an increased focus on improved outcomes. This is the core ofwhat we do, and what we will do in the future.”
- Chad Boerst Vice President and General Manager (Global), Hill-Rom Respiratory Care
THE METANEB® SYSTEM:EASY TO USE, THREE THERAPIES IN ONE DEVICE;AVAILABLE IN THE ACUTE CARE SETTING.
16 ADVANCE for Healthcare Careers

post-operative airway management. Boerst explains that there was a gap in their product line, which The MetaNeb®
System lled.
FUTURE OF AIRWAY CLEARANCE
As healthcare changes, the focus is on readmission reduc-tions, limiting length of stay and improving patient out-comes. The Vest® System and The MetaNeb® System are products designed to support these initiatives. “Our focus is to enhance outcomes for our patients and their caregivers,” says Boerst. “As healthcare changes, there’s only going to be an increased focus on improved outcomes. This is the core of what we do and what we will do in the future.” These products have become a standard part of airway clearance pro-tocols in hospitals throughout the country. All stakeholders—the patients, physi-cians and respiratory therapists—see the fundamental value in these products.
FORSYTH MEDICAL CENTER
According to the Centers for Disease Control and Prevention (CDC), COPD caused an estimated 126,005 deaths in the United States in people older than 25 years in 2005, an 8 percent increase from 2000.
At Forsyth Medical Center, a 900-plus-bed facility, in Winston-Salem, N.C., this statistic is not surprising.With a 46-bed pulmonary unit, For-syth treats individuals with varying pulmonary complications, but COPD
is the most prevalent disease. Forsyth’s pulmonary pa-tient pro le is an older adult battling respiratory com-plications from poor air quality and tobacco use. Typ-ically, pulmonary issues are compounded by existing complications. “Anyone who is not mobile is always a challenge,” explains John Wilson, respiratory clinicalcoordinator at Forsyth. “You take those types of patients and add COPD, bronchitis or pneumonia, and it will mag-nify the challenge.”
To help reduce intensive care unit (ICU) readmissions, Forsyth relies on The Vest® System and The MetaNeb®
System to move secretions and reduce infections. However,readmission reductions are diffi cult to credit to a particular therapy, and if a patient’s pulmonary system is severely compromised they are going to be in the hospital longer, which can result in additional pulmonary issues, explains Wilson.
Wilson was rst introduced to The Vest® System as a student at Wake ForestBaptist Medical Center as the staff was using the The Vest® System on their CF patients. In his current role, Wilson is involved with vendor selection, so his early exposure to the product left a positive impression. Initially, Forsythstarted with older vest models, and now the medical center has nine of The Vest® Systems and eight of TheMetaNeb® Systems.
At Forsyth, any time a physicianorders anything respiratory related,
the patient receives a consult with a respiratory therapist. During the consult, the therapist reviews the patient’s chart, conducts an interview, and completes a physical assessment with the patient. Then the therapist devel-ops a treatment plan based on protocols approved by the medical executive committee. As healthcare changes, the system demands more action with less support – more tri-age, explains Wilson. However, Hill-Rom’s products sup-port this change. “I don’t think one therapy or product is the magic bullet,” says Wilson, “but I think both of these products have given us good tools in our tool box. In fact, they have given us higher-caliber tools.”
And because every patient is diff erent, Wilson and his staff work to nd the right therapy the rst time around. “If you have a patient who follows commands, TheMetaNeb® System works well. If you have a patient who is lethargic or confused, The Vest® System is a good product for them,” says Wilson. Finding the right product is key, as it helps with length of stay (LOS) and readmissions.Currently, LOS at Forsyth is about 4.8 days, looking at all ICU patients. Wilson would love to see an average three-day stay; even a one-day decrease in LOS would savesigni cant money over the course of a year.
MEDICAL CITY DALLAS HOSPITAL
As the Pediatric Respiratory Care Manager at Medical City Dallas Hospital in Dallas, Texas, Steve Acton knows the im-portance of effi cient airway clearance in his pediatric patients.
With a robust pulmonary division, Medical City has been using The Vest® System and The MetaNeb® System for many years. The hospital’s pediatric pulmonary unit takes in many respiratory issues, including CF, pneumonia, bronchiolitis and respiratory syncytial virus (RSV). Medical City also sup-ports a cranial facial program, and many of those children have issues with airway clearance.
To reduce the risk of cross contamination, Medical City has 10 of The Vest® Systems and 10 of The MetaNeb®
Systems designated to speci c hospital rooms to avoidunneeded exposure from room-to-room transfers. In his 11 years at Medical City, Acton believes Hill-Rom prod-ucts reduced pulmonary complications and helped reduce readmission rates.
As healthcare changes, deploying resources eff ectively
and effi ciently is an ongoing challenge. Hill-Rom’s products help to address this issue. “When you do a treatment with The MetaNeb® System, you are doing two concrete thingsinstead of one,” he explains. “The MetaNeb® System deliversa bronchodilator and also helps with secretion clearance at the same time.” Staff members value the product’s ability to deliver multiple therapies in a single device.
As for The Vest® System, the product was amazing tech-nology when it was introduced; it is even more impressive today. “I think both products are going to continue to grow. These technologies have helped to improve the quality of life of our young patients,” he says.
With young patients, hospitals need therapies and treat-ments that produce results and make patients feel comfortable. Acton says that kids respond very well to treatments, even if they have to use two products in the same session. “Often-times, we do a treatment with The MetaNeb® System and The Vest® System in the same session. It helps clear the pneumonia or RSV in these children by mobilizing secretions.”
HOAG MEMORIAL PRESBYTERIAN HOSPITAL
Celebrating 60 years in 2012, Hoag Memorial Presbyterian Hospital, a 579-bed facility, has been a cornerstone of the Newport Beach, Calif., community. As a community-based, not-for-pro t hospital, Hoag is expanding; it added a sec-ond campus in Irvine, Calif., in 2010. In addition, Hoag and St. Joseph Health System formed an affi liation to create a stronger healthcare alliance in Southern California.
Like many other hospitals and healthcare systems throughout the country, Hoag’s Respiratory Care Depart-ment impacts all departments. As Director of Hoag’s Respi-ratory Care Department, Kristin Vercnocke, BS, RRT, knows that “respiratory touches everyone.” She is involved in car-diology, neurology, emergency room, neonatal, Pulmonary Rehabilitation, Pulmonary Function Testing and infection prevention initiatives. In addition, Vercnocke serves on the Readmission Reduction team for pneumonia.
Hoag’s patient pro le varies, but individuals older than 70 with multiple comorbidities and hospital visits in a calendar year use the most resources. Most often, these patients lack social and family support, as well as pallia-tive care planning. Hoag also treats many chronic COPDpatients, who struggle with rebound issues and create
SEPT/OCT 2012 | ADVANCE FOR RESPIRATORY CARE & SLEEP MEDICINE ADVANCE FOR RESPIRATORY CARE & SLEEP MEDICINE | SEPT/OCT 2012
ADVERTORIAL ADVERTORIAL
“Our focus is to enhance outcomes for our patients and their caregivers. As healthcare changes, there’s only going to be an increased focus on improved outcomes. This is the core ofwhat we do, and what we will do in the future.”
- Chad Boerst Vice President and General Manager (Global), Hill-Rom Respiratory Care
THE METANEB® SYSTEM:EASY TO USE, THREE THERAPIES IN ONE DEVICE;AVAILABLE IN THE ACUTE CARE SETTING.
17ADVANCE for Healthcare Careers

high costs for the organization. “We can treat the symp-toms,” says Vercnocke, “but what is the quality of life? We as Respiratory Therapists see how this patient de-mographic is draining healthcare system resources on so many levels.” Overall, Vercnocke estimates 50 percent of patients remain in the hospital longer than projected due to pulmonary complications.
For more than 25 years, Hill-Rom has had a strong pres-ence in Hoag’s Respiratory Care Department. Currently,Hoag utilizes 10 of The Vest® Systems and 13 of TheMetaNeb® Systems. The products off er aggressive/non-in-vasive therapy that can be used in critical to non-critical care settings, and patients “feel” the diff erence, so there is improved compliance,” explains Vercnocke.
When Hoag decided to adopt The Vest® System, the enthusiasm grew quickly among the staff . “The Vest®
System is excellent because it is not position dependent, and it’s easy to place on the patient,” says Vercnocke. She describes The Vest® System as a “kinder, gentler” therapy that is eff ective. The Vest® System is a versatile therapy; the bene ts are tangible for an 80-year-old fragile womanor a young, 300-pound man. Vercnocke anticipates health-care changes will move care from the hospital to the home setting, so a product like The Vest® System will be anessential part of recovery and healthcare maintenance.
As for The MetaNeb® System, Hoag was one of the rst facilities in Orange County, Calif., to trial it on patients. A success from the beginning, Hoag’s Clinical EducationSupervisor, Daryl Weber, RRT-NPS, created The MetaNeb®
System Recruitment Airway Clearance (RAC) protocol that was later shared with Hill-Rom. In fact, when Hoag launched The MetaNeb® System, it underestimated how popular it would be with therapists and physicians. “We have never experienced a product launch with such global adoption—we ran out of circuits for The MetaNeb® Sys-tem on day two, organization wide,” Vercnocke says.
MARICOPA INTEGRATED HEALTH SYSTEM
As the cardiopulmonary supervisor and educator at Mar-icopa Integrated Health System (MIHS) and Arizona Burn Center in Phoenix, Ariz., Jo-el Detzel, RRT, educates her staff and hospital physicians on various respiratory ther-apies. She also is expected to be an expert in inhalation
burn injuries and the neonatal ICU, pediatric ICU and adult/pediatric trauma emergency.
At the Burn Center, The MetaNeb® System is the most-used Hill-Rom product. With ve units, The MetaNeb®
System supports the facility’s infection control policy. Every patient is in isolation, so The MetaNeb® System’s single-patient-use circuit and the fact that the unit doesn’t touch the patient contribute to reducing the risk of cross contamination.
“The MetaNeb® System is very popular in our facil-ity,” says Detzel. “What’s nice about it is that you canadjust your settings—you can give your pediatric patients a break from the actual percussion.” In addition to thesecretion capabilities of The MetaNeb® System, Detzel also feels it’s a good tool as a preventative type of medicine.
Since infection is a major concern with burn patients, the goal is to keep them off the ventilator or limit the num-ber of days on the ventilator. With burn patients, a patient is more susceptible to infection if they have to go back to the operating room. If patients can spend two days before surgery on The MetaNeb® System, it optimizes their pre- and post-surgical experience.
“There are three people who really like The MetaNeb®
System: the patient, the physician and the therapist,”explains Detzel.
SUCCESS THROUGH ACTION
As healthcare changes and costs increase, products likeHill-Rom’s The Vest® System and The MetaNeb® System will help manage a hospital’s bottom line. ICU costs are increas-ing, and it is important to reduce LOS and readmission.
“[We] believe the eld of respiratory care will continue to seek solutions that bring true value to our healthcare system by reducing length of stays, lowering readmission rates and improving patient outcomes,” says Boerst. ■
Hill-Rom Respiratory CarePhone: 800-426-4224 or 651-490-1468
www.thevest.com | www.metaneb.com | www.hill-rom.com
SEPT/OCT 2012 | ADVANCE FOR RESPIRATORY CARE & SLEEP MEDICINE
ADVERTORIAL
18 ADVANCE for Healthcare Careers

ASthmA hAS been on the rise, but so has the ability to control it with better medications, technology and patient education. Today, for properly guided asthma patients, visits to the emergency room should be fewer than ever before. However, that is not the case—primarily because of a fervent lack of “adherence” on the part of asthma patients.
Although asthma may be considered part of the “COPD umbrella” of respira-tory diseases, patients often forget that it bears the distinction of being nearly always reversible and highly preventable. Additionally, it is a disorder that spares some people for significant periods of time, occasionally without any aggressive management or therapeutic adherence at all, leading patients to believe it will “disappear” if they wish hard enough. But therein lays asthma’s real danger: Wishful thinking leads to neglect, which can be disastrous.
Some people have varying levels of asthma symptoms daily while others are completely normal until they are exposed to their specific physical and psycho-logical triggers. Therefore, the absence of preventive measures in between episodes has become a marked concern in the big picture. The patient with chronic asthma who is unaware and/or uncooperative is just another asthma episode waiting to happen, usually under the worst of circumstances. To paraphrase the often-quoted Murphy’s Law, asthma is likely to exacerbate at the most improbable moment where the least amount of help is available.
Steve Dolan, RRT, offers an interesting point of view on the causation and prevention of asthma episodes because, in addition to being a skilled, highly experienced respiratory therapist, he is asthmatic himself. According to him, adherence is all about consistent control of triggers through avoidance, short- and long-term prescription medications and preventive self-care. He says, in many cases, the real problem is patients’ lack of self-discipline when they’re feeling good; this is when they’re likely not to use their medications as prescribed while exposing themselves to known triggers. They get slap-happy, allowing the triggers like dust mites, seasonal cold, cockroach parts, pet dander, mold, air fresheners and allergic responses to cause inflammation and bronchocon-striction, necessitating emergency action far in excess of what would be needed under a regimen of proper adherence.
Some patients may take their medication but don’t follow instructions, creat-ing another kind of adherence problem. “Using an inhaler without a spacer substantially reduces effectiveness because a good portion of the medication is completely wasted,” Dolan says. He feels that true adherence is not only getting the patient to act on their list of do’s and don’ts, but to perform the do’s with maximum efficiency. It is imperative to ensure that a dose is a true dose and not just the act of squeezing off a compromised shot of medicine, he says. “I tell my patients to always use a spacer and then show them exactly how it is done. The difference is huge.”
Dolan’s comments offer a good example of the role clinicians must play in educating and gaining the trust of asthma patients. In short, we can promote adherence by:• Understanding the positive power of good patient-clinician relationship; • Promoting an in-depth understanding of asthma, its treatment and
prevention;• Determining a patient’s true attitude and perception of the disease and
treatment; and• Teaching patients to take a daily active part in asthma management. These four principles are the keys for clinicians to treat and manage asthma,
but our knowledge of them is not enough to solve the problem of patient adherence. It has been estimated that adherence could be grossly improved in more than two-thirds of chronic asthma cases, so we must be vigilant in continuously reminding patients of preventive measures and prophylactic care. The likelihood of increased long-term clinical success may be a matter of clinicians participating in prevention in the most aggressive manner that skill and time allows. ■
Daniel Fardella, RRT, PhD, has been a writer and filmmaker in addition to practicing as a respiratory therapist.
Improving AdherenceClinicians must be diligent in educating asthma patients
■ aLLerGy anD astHma By Daniel Fardella, RRT, PhD
Respiratory Delivery Systems, Inc.Phone 978-970-1947 • Fax: 978-970-1948
Aerosol Spacer andChamber for MDIsFor use with Metered-Dose Inhalers
Call toreceive
FreeSamples
Mention our ad in Advance Newsmagazines.
®
NEW
For free samples
Respiratory Delivery Systems, Inc. in Chelmsford, MA develops, manufactures and supplies the smallest spacer and chamber devices available for use with metered-dose inhaler products. The Microspacer® and Microchamber® devices are signi cantly less expensive, convenient to use and clean, latex free, dishwasher safe. Performs as well as the larger and much more expensive devices. Compatible with CFC and HFA
(Also available for Medicaid patients)
metered-dose inhaler formulations.
19ADVANCE for Healthcare Careers

AA
RO
N R
OS
HO
NG
/iS
TO
CK
PH
OT
O/T
HIN
KS
TO
CK
■ coVer story
BestDepartment: cincinnati children’s Hospital medical center in ohio
“Our goal is to be the best at getting patients better,” said Thomas J. Cahill, BS, RCP, RRT-NPS, interim director of the respiratory care division at Cincinnati Children’s Hospital Medical Center. And between its specialty prac-titioner positions, push for education and shared governance structure, it’s clear that the department is well on its way.
It all starts with an innovative staffing model that hires respiratory therapists directly into areas such as the emergency department, post-acute
care, cystic fibrosis center, and transport team. “Our big advantage of being matrixed (is) the doctors, residents and nursing staff know who you are and trust your skills,” explained Jerry Edens, MEd, RRT-NPS, clinical program manager. Specialty positions exist to acknowledge experts and to provide staff with resources in airway clear-ance, asthma management and research. Another group of therapists, called the respiratory resource unit, acts as the “chess master,” identifying when one department experiences an influx in patients and/or patient acuity and sending reinforcements to help handle the load.
RTs gain expertise through an extensive educational system. Therapists can earn continu-ing education hours monthly through a grand rounds program that features national speakers and hospital-based experts. A cohort program with a local university allows staff to attend classes on the hospital campus that count toward a bachelor’s degree in health sciences. The program is paid for up front by the hospital for for three years. Tuition
reimbursement and assistance programs help cover the cost of the electives required to graduate, bachelor’s degree programs at other institutions, and classes for therapists pursing a master’s degree.
“Most managers undertake a year-long leadership program focused on the basics of leadership, management and business,” said Kie Shelley, manager of the transport team. Some elect to receive one-on-one coaching from the human resources department as well.
Staff also can take an active role in leading the division through a shared governance model. They can pose a problem to the professional inquiry council to be researched. If the literature supports a change, the information is sent to a practice council and education council to enact the change and train staff. “It gives everyone in the hospital the ability to have their voice heard,” said Phil Stutler, RRT, a member of the transport team.
The shared governance model also is present hospital-wide, giving respiratory therapists a seat at the table with members from every other dis-cipline in the hospital and helping to foster a sense of teamwork and profound respect. “That’s one thing that makes us outshine any other place,” said Shannon Brannon of the neonatal intensive care unit. “You feel that you are not just part of the hospital and the respiratory department, you become part of the medical staff of doctors, fellows and specialists.”
respiratory’s Golden HeroesBy Kristen Ziegler
as tHe natIon cheered the united states bringing home 104 gold medals in the 2012 summer olympics, ADVANCE considered a throng of entries vying for just three golden trophies awarded in our 12th annual national respiratory achievement awards. How could we choose top honors with so many highly qualified entries? read on to see what made these winners stand out as the “Best in respiratory.”
Kristen Ziegler can be reached at [email protected].
national respiratory achievement awards
HonorableMentions: Leonard J. chabert medical center, houma, la. st. Luke’s episcopal Hospital, houston, texasmercy Hospital – Joplin, in missouri
20 ADVANCE for Healthcare Careers

SERVOlution is a trademark of MAQUET Critical Care AB.
AT AARC 2012, VISIT MAQUET BOOTH #417 www.maquetusa.com
Join the SERVOlution™
MAQUET is committed to providing therapeutic options for disease-specific entities that help you improve patient
outcomes. SERVOlution is our new innovative approach to mechanical ventilation that provides you with comprehen-
sive, goal-oriented therapeutic packages for a patient’s course of treatment in the ICU.
The new SERVO with SERVOlution.
■■ Relieve—help reduce work of breathing
■■ Synchronize—improve patient ventilator interaction and patient comfort
■■ Protect—reduce lung stress and help maintain muscle conditioning
■■ Baby—help protect infants with improved synchrony and NIV support
Explore how the new SERVO with SERVOlution can help you liberate your patients from mechanical ventilation.
Scan to Learn More
21ADVANCE for Healthcare Careers

■ coVer story
BestManager: amanda mcGarrigle, rrt, rrt-nps, rpFt, manager, Bronchoscopy, pulmonary Function Lab, sleep center, and pIcc team, medical university of south carolina in charleston
When Amanda McGarrigle, RRT, RRT-NPS, RPFT,
first joined the management team at the Medical
University of South Carolina in Charleston, there
were some grumbles about her relatively tender
age. But when staff saw the 27-year-old’s gusto
for managing four departments, com-
pleting graduate studies in healthcare
administration and volunteering regu-
larly, any doubts were quashed.
A year later, pulmonary function
technologist Christopher Kling, RRT,
RPFT tells ADVANCE that we “definite-
ly made the right decision” by naming
her this year’s Best Manager. “She not only leads
by example at work but with her business or on-
goings outside of the hospital,” said Kling. “you
can tell she’s in it, she really loves her job.”
Since taking over the department, she’s cross-
trained staff in areas such as pulmonary func-
tion testing, bronchoscopy and pulmonary re-
habilitation so that they can help out in times of
high census.
McGarrigle also was the driving force behind
creating a shared governance structure that
gives RTs input on practice and policies, proto-
col development and community service and
events — and in making sure that busy RTs were
able to attend the meetings. Conference rooms
in each of the campuses’ three hospitals are
set up to broadcast the meetings and
therapists also can call in from home.
“I think getting staff involvement in
policies is really important, because
they are the ones who it affects,” Mc-
Garrigle said.
On her own time, McGarrigle
petitioned the mayor of Charleston
to sign a proclamation recognizing Respiratory
Care Week 2011 and was recognized by Ameri-
can Lung Association for organizing the team
with the most participants in the Fight For Air
Walk last fall. She’s just finished working with
the Cystic Fibrosis Foundation on a summer-
long campaign that raised nearly $60,000 for
disease research.
Our judges also were impressed with all she’s
done in her short time as an RT, calling her a
“rising star in the profession.”
“She demonstrates how passion, motivation
and perseverance can take you far,” explained
Brooke yeager, RRT, who nominated McGarrigle
for the honor. “She sets an example that every-
one in our profession, new and even not so new,
can look up to.”
BestPractitioner: Len picha, rrt, cpFt, Lead therapist, pulmonary rehabilitation, charleston area medical center, W.Va.
No one would blame Len Picha, RRT, CPFT, if he wanted to slow down after 39 years as a respiratory therapist. “Instead (he) is ramping up speed to tackle new and difficult topics all to benefit the individual patient and the longevity, viability and capacity of the respiratory thera-pist,” said Cynthia Keely, manager of the West Virginia Asthma Education and Prevention Program, who nominated him for this award.
For three years, Picha has worked as lead coordinator of the West Virginia Charleston Asthma Management Program for Seniors,
dedicating his time to educating and enabling older adults to control their asthma. He has developed low-literacy education materials that use pictures with brief descriptions to explain
spacers and peak flow meters. “Seniors with lung disease, I just
have a heart for those folks,” said Picha. “They just seem to be so needy, and the little things that I can teach them and show them, they just seem so grate-ful.”
Take, for example, the patient who couldn’t take his two middle-school-
aged daughters swimming because he needed supplemental oxygen. Picha worked with him to build muscle tone and trained him in breathing techniques until he could go without oxygen long enough to take them swimming. “It’s the little things like that, when I can just see the joy in their eyes. It’s a matter of giving a little bit of their life back to them.”
Picha also made it his mission to train physicians and nurses in the county’s four regional rural health clinics about the importance of obtaining regular spirometry readings from asthmatic pa-tients after learning that only 3 percent of asthma patients had a reading on record.
As a lead therapist in the pulmonary rehabilita-
tion program at Charleston Area Medical Center in West Virginia, Picha worked with nurses and respiratory therapists to develop a pulmonary handbook that staff can use to help patients un-derstand chronic obstructive pulmonary disease, asthma, pneumonia, bronchitis, and emphysema. Nurses trigger a respiratory consult by asking whether patients ever have had any of those dis-eases. While data for the whole year hasn’t yet been analyzed, it appears so far as if patients who undergo the program have fewer readmissions over the following six months than those who don’t.
But like any respiratory hero, Picha is quick to share credit for the results. “I am a brain-stormer; I throw ideas out,” he said, claiming that it’s his team of skilled co-workers who polish those ideas into respiratory gold.
HonorableMentions: David orloff Bs, rrt, rpsGt, rst, Associate Director-Sleep Services, Sleep for life-Somerset medical Center, hillsborough, n.J.
stanley John, Bs, rt, rrt-nps, cpFt, cpc, Department manager, respiratory therapy, north Shore University hospital, manhasset, n.y.
About the Contest:Judges for the 2012 competition were: mary Lou Guy, rrt, mBa, cHt, and Joe Hylton, Bsrt, rrt-nps, cpFt, ncemt-B, Faarc.
the following sponsor congratulates all the winners:
HonorableMentions: Brooke yeager, Bs, rrt, Cardiopulmonary rehabilitation, medical University of South Carolina in Charleston
theresa James, crt, respiratory Care, hSC pediatric Center, Washington DC
GE Healthcare
Breathe easy.Sleep well.
At GE Healthcare we’re working to make sure patients with respiratory and sleep disorders don’t have to struggle for air or wrestle to get a good night’s rest. That’s why we offer homecare solutions for a variety of patients from high clinical dependency to lower care needs. Our range of homecare respiratory products can help you to improve patient outcomes and enhance their independence, comfort and quality of life.
Our sleep disorder solutions include the iSleep™ family, a range of CPAP’s to meet the needs of patients with obstructive sleep apnea. Our home care ventilatory solutions include the Vivo™ family and iVent™ 101: a collection of ventilators to match the respiratory requirements of your patients.
Explore our respiratory offerings tailored to a wide range of patient needs at: www.gehealthcare.com/respiratorycare
22 ADVANCE for Healthcare Careers
GE Healthcare
Breathe easy.Sleep well.
At GE Healthcare we’re working to make sure patients with respiratory and sleep disorders don’t have to struggle for air or wrestle to get a good night’s rest. That’s why we offer homecare solutions for a variety of patients from high clinical dependency to lower care needs. Our range of homecare respiratory products can help you to improve patient outcomes and enhance their independence, comfort and quality of life.
Our sleep disorder solutions include the iSleep™ family, a range of CPAP’s to meet the needs of patients with obstructive sleep apnea. Our home care ventilatory solutions include the Vivo™ family and iVent™ 101: a collection of ventilators to match the respiratory requirements of your patients.
Explore our respiratory offerings tailored to a wide range of patient needs at: www.gehealthcare.com/respiratorycare
23ADVANCE for Healthcare Careers
the Sleep meDICIne profession is undergoing a dramatic evolution as oral appliance therapy emerges as a key treatment for obstructive sleep apnea. As a result, the role dentists can play in helping sleep apnea patients continues to increase.
Here’s one barometer that reflects this trend: By 1989, there were only 11 articles in medical and dental literature about oral appliance therapy for the treatment of OSA. In just the past year, 43 English-language articles were published on the topic, covering key issues that included understanding the mechanics of oral appliance therapy, learning possible side effects and quantifying the physiologic improvement of patients who use oral appliance therapy to treat their obstructive sleep apnea.1
Years ago, the articles published consisted of single-case presentations or presentation of data on fewer than 20 subjects.2 There were few con-trolled studies and minimal use of placebo therapies. Today’s studies are robust, featuring retrospective studies of 500-900 patients, randomized controlled trials and placebo therapies to determine effectiveness of mandibular advance-ment.3-5 Another key change is that, in the past, this literature was published only in dental jour-nals and virtually unavailable to physicians. Now the majority of literature is in the medical realm.
Despite this recent increase in understanding oral appliance therapy, continuous positive airway pressure (CPAP) remains the standard of care for OSA. What has led to the predominance of CPAP therapy, which became available in 1981, just one year before the first publication of literature on oral appliance therapy?6,7
traditions and perceptions There are several explanations for today’s treatment environment. One relates to the initial education process. Years ago, all dentists were trained in a medical school setting. After taking basic courses like pathophysiology, pharmacology and gross anatomy with their medical peers, they would then go off to learn the skills required of a practicing dentist. This led to isolation of both
groups as physicians became immersed in their hospital rotations while dentists learned “tooth by tooth” in a dental environment.
In addition, the majority of practitioners in each field opened solo practices and ministered to patients in their neighborhoods. Hospitals handled secondary and tertiary care patients referred from the primary care solo practitioner. More recently, medicine has been reshaped into large group practices that can handle the com-plicated medical problems and incorporate the vast medical literature written annually. Physicians also have a long history of researching various therapies and working as a team to treat patients with complicated medical problems.
Dentists, on the other hand, continued to maintain small, localized offices, remaining isolated from other practitioners. Some dentists would join study groups, their state societies and national society to maintain a close peer group and keep up with changes in the various aspects of dentistry. Dentists were not used to engaging physicians or their peers when it came to treat-ing the typical patient, let alone those with medical problems. While dentists in specialties such as periodontics or oral surgery had much more understanding of the need to communicate with a patient’s medical providers, this was not the norm for a group of professionals who were predominantly general practitioners.
Based on these cultural dynamics, physicians went to their peers in other disciplines when help was needed to treat OSA. They were not in the habit of seeking help from a dentist nor did they actually understand how a dentist could help treat patients with obstructive sleep apnea.
However, a mutual meeting of the minds can break down these barriers and create a strong camaraderie between physicians and dentists treating obstructive sleep apnea. Physicians need to understand that dentists offer a therapy that will round out their armamentarium in provid-ing optimal care to their patients with obstructive sleep apnea. Dentists need to understand that communication with physicians about diagnosis
and medical comorbidities—as well as urging the patient to return to his sleep physician for follow-up testing—is a basic requirement in helping to provide this optimal medical care.
compelling research Helping to drive the adoption of oral appliance therapy today is the wealth of research now avail-able that illustrates how it is a very effective clini-cal treatment for mild to moderate OSA and also has been impressively successful in treating some patients with severe obstructive sleep apnea.8-10 Physicians understand that it is outside their scope of practice to fabricate a custom-fitted oral appli-ance and that custom-fitted appliances are much more effective and much more comfortable than the “boil and bite” (prefabricated) appliances available to medical providers.11 Therefore, when a study of more than 56.8% of unselected patients at Walter Reed Medical Center were returned to an apnea-hypopnea index (AHI) of less than five with oral appliance therapy (confirming similar conclusions published in 2009), it underscored how oral appliance therapy often can equal CPAP in effectiveness and may offer a higher patient compliance than CPAP.12-14
In addition, oral appliance therapy has been shown to be similar to CPAP in reduction of both nocturnal and diurnal blood pressure, de-creased excessive daytime sleepiness, increased quality of life measures, decreased snoring and improvement in neurobehavioral function.15-18
remaining challengesThe inability to predict which patient will be returned to an AHI below five does present problems.19 Yet, multiple studies looking at monitoring techniques such as remotely con-trolled mandibular advancement appliances that can be titrated during polysomnography, actual patient titration of oral appliance therapy and use of sequential home sleep testing (HST) are helping to provide understanding of patient characteristics that correlate with total control of OSA when using oral appliance therapy.20,22
It must be noted, however, that an even more significant number of patients can be brought below an AHI of 10 or 15, regardless of the severity of their disease.23 Compliance with oral appliance therapy has been shown, using patient diaries validated by covert monitoring, to be as high as 75% of patients using the appliance all night seven nights a week.24,25 Certainly, objective compliance monitoring is much easier to accomplish when the compliance monitor is in a CPAP machine rather than inside an oral
■ oraL appLIance tHerapy
Dental Dynamics in oSA treatmentPhysicians and dentists can work together.
by b. Gail Demko, DmD
24 ADVANCE for Healthcare Careers
866.264.7667
TAP IntoSleeP .com
As effective as CPAP in most patients.
TAP® devices are made in the U.S.A.
1. Hoekema, A., B. Stegenga, et al. Obstructive sleep apnea therapy. In: Journal of Dental Research, 2008 87(9): 882-887.
2. Holley AB, Lettieri CJ, Shah AA. efficacy of an Adjustable Oral Appliance and Comparison to Continuous Positive Airway Pressure for the Treatment of Obstructive Sleep Apnea Syndrome. In: chest DoI 10.1378/chest.10-2851, June 2, 2011
1, 2
The TAP® 3 Elite.You wouldn’t prescribe a CPAP that only goes to 10 cmH2O, so why settle for inferior oral appliances?
Unlike cPAP devices which all go to 20 cmH2o, oral appliances differ in their ability to treat Sleep Disordered Breathing. only the tAP has been shown in many independent peer review studies to treat the full range of sleep apnea from mild to moderate to severe. As disease progresses and symptoms re-occur, your patients can easily adjust their tAP with the key.
ReASOnS TO PReSCRibe The TAP® 3 eliTe:
• Patient-adjustable in-mouth With the KeY
• ends unnecessarY adjustment aPPointments
• Patient PlaYs active role in theraPY
• indePendent clinical studies (over 32)
• adjustable in the sleeP lab for tItRAtIon
25ADVANCE for Healthcare Careers
■ oraL appLIance tHerapy
cavity, though multiple studies using covert compli-ance monitoring in oral appliance therapy are underway in both Canada and Europe.
Yet another challenge in the use of oral appliance therapy is the current structure of medical insur-ance companies; some have bylaws that do not allow non-physicians/non-surgeons to become in-network providers. They also have bylaws that prevent direct payment to out-of-network provid-ers. This often means that patients are required to pay out-of-pocket to dentists who treat obstruc-tive sleep apnea with an oral appliance and then wait for some level of reimbursement from their medical insurance company. To this end, physi-cians understand that CPAP, while often being more onerous to use, may be a patient’s only fi-nancial option. While these constraints are chang-ing, it will be some time before patients have equal access to all scientifically relevant therapies.
Even anecdotal perceptions must be overcome. Physicians often are not able to see the patients who return to the dental office day after day happy, symptom-free and enthralled with their oral appli-
ance. They have heard only the complaints of patients who return to CPAP therapy after a negative expe-rience with an oral appliance. Conversely, some dentists have the belief that there is no patient suc-cessfully using CPAP. Each view is equally invalid.
Many studies now are looking at the long-term effectiveness of oral appliance therapy. Data show that patients with an oral device for more than five years remain effectively treated.26 Oral appli-ances have side effects and so does CPAP; in fact recent literature shows that both modalities of treatment move teeth. Oral appliances do not cause temporomandibular joint pain when prop-erly fitted and properly adjusted. A recent study showed that patients using oral appliance therapy long term had an overall decrease in TMJ com-plaints while patients using CPAP had an overall increase in TMJ complaints.27
same team, same pageArmed with this additional knowledge, and backed by evidenced-based research, we are witnessing increased teamwork between physi-
cians and dentists to optimally treat patients with OSA. We’re confident this will continue to rise. Dentists can provide oral appliances not only as standalone therapies, but also used with CPAP to prevent mouth leaks and open the oral airway enough to allow reduction of effective CPAP pressures by 2-5 cm H2O.28 Many of the oral appliances can support struts to hold CPAP masks and nasal pillows—without the need for any head straps. This minimizes mask leaks that occur when the patient turns his head and straps move the mask.
Custom-fitted CPAP masks are another therapy dentists can offer. Patients with abnormal facial anatomy, hemimaxillectomies or unusual nasal structure would benefit significantly from the mask being fabricated using a mold of their face. There is even a device that delivers CPAP through a custom-fitted oral appliance, resulting in laminar airflow to the oropharynx, which is Food and Drug Administration-accepted for the treatment of severe OSA only. The options that
Micro I, The New GenerationMicro I, The New GenerationMicro I, The New Generation Low Cost Precision Pocket SpirometerLow Cost Precision Pocket SpirometerLow Cost Precision Pocket Spirometer
Measures FEV1, FVC, PEF, FEF25-75, FEV6, FEV1/FVC, FEV1/FEV6, FEF25, FEF75 Choice of four indices can be displayed Choice of predicted values Variation from norm as percentage or z-score Confirming diagnostic interpretation Post bronchodilator comparison Optional NLHEP mode PC software for unit configuration Maneuver quality checks Quick test mode 2-Year parts and labor warranty Model number: MS10
Micro Direct, Inc. 803 Webster St., Lewiston, ME 800-588-3381 Fax 207-786-7280 Email [email protected]
Call 1-800-588-3381 today! visit www.micro-direct.com
Continued on 30
26 ADVANCE for Healthcare Careers

27ADVANCE for Healthcare Careers

'Tis the Season to Celebrate Your Friends & CoworkersVisit us online to see our entire selection of products for Sleep Techs & Respiratory Professionals
��
�
#06386 #02758
�
Respiratory Care Professionals
RSFIF122
Use promo code
Not valid on Littmann stethoscopes,Ultrascope (#11840), Oximeter
(#13221), Cherokee WorkWear, affi liate-specifi c merchandise or items ending in $.97 cents. Valid
now through 12/02/12.
SAVE 15%
� Metal Carabiner PenBlack ink. #04542 $3.49
� Ceramic Mug*15 oz. Personalize It! #15349 $9.99
�
�
�
� Men's & Women's Tees#26849 Men's / Navy, Charcoal or Black.#26848 Women's / Black, Navy or Raspberry.$16.99 S-XL; $19.99 2XL Women's S-2XL only.
� Lapel Pins1" x 1". $4.99 ea.
� Car Magnet4". #26570$3.99
Sleep Technologist� Ceramic Mug*15 oz. Personalize It! #26199$9.99
� Poster18" x 24". #26150 $16.99
� Men's & Women's Full-Zip HoodiesEmbroider It! #26241 Women's / Baby Blue, Deep Heather or Navy.$42.99 S-XL; $45.99 2XL#26677 Men's / Deep Heather, Navy or Olive.$46.99 S-XL; $49.99 2XL
� Embroidered Messenger Bag*16" x 111⁄2" 4 3⁄4". Personalize It! #15110$27.99
� Carabiner Pen PackBlack Ink. 5-pack. #25235$8.99
� Car Magnet4". #26514$3.99
advancehealthcareshop.com1-877-405-9978
Catalog Code: RS-1242APrices and offers valid through 12/10/12
Connect with us at facebook.com/ShopAdvance
Share What You Love with Pinterest
Follow us on Twitter.com/ShopAdvance
Add us to your circle on Google+
Connect with us!
��g
by Blue,
2XL
2XL
0
Pack235
Personalize
$3.99
New!
New!
�
�
* Additional charge for personalization or embroidery.
�
New!
�
❄❄ ❄❄ ❄❄ ❅
❅❅❅ ❅
❅
❅
5-Pack
RS-1242 A.indd 1 10/4/12 9:46 AM
28 ADVANCE for Healthcare Careers

www.advanceweb.com/respiratory september/october 2012 ADVANCE FOR RESPIRATORy CARE & SLEEP MEDICINE 29
■ E
DU
CA
TIO
N O
PP
OR
TU
NIT
IES
Choose the Proven WayUpgrade to RRT or Earn Your Degree, Online 24/7!
You could advance your career and increase your earning potential in a fast, flexible way.
Proven online healthcare degree programs put you in control — you can complete your coursework anytime, anywhere. Our online student services make your studies available to you 24 hours a day, 7 days a week.
The only ASRT distance education program accredited by the Commission on Accreditation for Respiratory Care (CoARC)
The leader in RT distance education for over 30 years
Employer Reimbursement Accepted Call for more details
Approved for GI Bill/VA Education benefits
Associate’s Degrees:Allied Health
BusinessRespiratory Therapy
Bachelor’s Degrees:BusinessNursing*
Respiratory Therapy
Master’s Degrees:Business AdministrationNursing Administration*
Healthcare AdministrationPublic Health
Health Services-Health Promotion*RN Required
NOW OFFERING
BSRC Program in
Advanced Clinical
Practice
Financial Aid Now Availablefor Qualified Students
888-814-1893For more information about our graduation rates, the median debt of students who completed the program and other important information, please visit our website at www.independence.edu/student-information.
Bioterrorism AgentsSleep Disorders
Respiratory Medications and many more!!
Available 24 hours a day Complete course and post-test online
Print your certifi cate immediately Courses also offered as home study
Online RespiratoryCE Courses
Bioterrorism AgentsSleep Disorders
Respiratory Medications and many more!!
AARC - Approved
Great for last minute CEs.
www.ssbinc.com/medwayor call 1-800-301-5262
CHECK YOUR MAILING LABEL TO SEE IF YOU NEED TO RENEW YOUR FREE SUBSCRIPTION TO ADVANCE!
TIME MAY BE RUNNING OUT!
RS Cal 10_15.indd 1 10/11/12 5:07:01 PM
29ADVANCE for Healthcare Careers

■ E
DU
CA
TIO
N O
PP
OR
TU
NIT
IES
If you are considering a career as a sleep technician,this course can provide you with all the necessary training!
If you are a physician interested in the field of sleep,we can provide you with entry level training.
Our next 10 day Course begins:November 5, 2012
Call or log on today for details.1.856.793.0318 ext. 156
plus
Comprehensive10 Day Polysomnographic
Training Courses
2 Day Scoring Workshops& RPSGT Review Workshops.
www.schoolofsleepmedicine.com
Visit us on the web for our full line of courses andworkshops: www.schoolofsleepmedicine.comSPACE IS LIMITED SO REGISTER EARLY.
Discounts available on groups of 3 or more.
FIND YOUR SEASONAL STYLE!
SET THE SCENE WITH
Discover our selection of season-friendly favorites at advancehealthcareshop.com
FREE SHIPPING!
RS Cal 10_15.indd 2 10/11/12 5:07:19 PM
a well-trained dentist can bring to a busy sleep practice are myriad.
Looking ForwardDentists are aware that CPAP is the standard of care. Our goal is to optimize therapy whether oral appliance therapy is a stand-alone therapy or part of combinational therapy. Working as a team with sleep physicians, dentists can help patients accept therapy, improve medical out-comes and increase compliance regardless of treatment choice. And these are goals we all embrace. ■
Visit the resources section of www.advanceweb.com/respiratory to view references.
B. Gail Demko, DMD, is president of the American Academy of Dental Sleep Medicine and is certified by the American Board of Dental Sleep Medicine. She serves as the expert advisor to the Food and Drug Administration in the field of oral appliance therapy for the treatment of obstructive sleep apnea. Her practice, Sleep Apnea Dentists of New England, is located in Weston, MA.
Continued From 30
oral appliance therapy
St. tAmmAny pArISh Hospita l in Covington, La. was introduced to OxyMask approximately five years ago by our specialty respiratory distributor. We always are looking for new technology and innovation that will allow our therapists and nurses to provide better care to patients in a cost-effective manner. When I saw the OxyMask, I immediately was impressed by its simple and safe design and the fact that one mask could deliver a full range of flows to meet a patient’s oxygen requirement.
We initiated a trial of the OxyMask with several of our patients who already were on mask oxygen. The patients immediately com-mented that they didn’t feel so claustrophobic with this mask. Nurses loved that they could understand what their patients were saying. They also appreciated that patients could take sips of water through the straw without taking the mask off and having their oxygen saturation fall. It was very easy for our physicians, nurses, and therapists to adjust the flow of oxygen to achieve the desired saturation. The ability to adjust oxygen levels using a single mask by adjusting the flow was a logical extension of our oxygen protocol for nasal cannulas. The physicians would order a desired SaO2, and then the therapist would assess the patient and use the appropriate device.
The OxyMask had a large impact on our post-anesthesia care unit (PACU), where nurses are responsible for setting up oxygen for their patients. The nurses frequently used to find themselves having to try up to three different devices to either increase or reduce the amount of oxygen the patient was receiving. With the switch to OxyMask, they now use one device for the patient and simply adjust the flow to achieve the ordered or desired oxygen level. Not only was patient care improved and nursing care simplified, we also saved money by reduc-ing the number of masks that were used in the PACU area.
St. Tammany Parish Hospital has been a strong advocate of protocols. Our oxygen
therapy protocol coupled with a respiratory therapist’s assessment of a patient’s requirement allows us to determine whether the patient will be placed on a nasal cannula or the OxyMask. Simple cannulas, OxyMask, and high-flow heated/humidified cannulas meet the needs of the bulk of our patient population. We have kept a few non-rebreathing masks in inventory, but we find that if OxyMask doesn’t meet the patient’s need, then they probably are going to need a high-flow heated/humidified cannula, CPAP or NIV.
Our therapists also love the OxyTrach. It allows simple and safe transport of patients who have a tracheotomy. Therapists don’t have to waste time searching for and putting together a system for those patients.
In my experience, the two major improvements in oxygen therapy have been the high-flow heated/humidified nasal cannula and the OxyMask. These two devices literally have eliminated the need for any other oxygen mask at our facility. It is easy for us to order, stock, and use the reduced number of items.
By using OxyMask products, our patients’ needs are met in a comfortable and safe manner. We never have to worry about a flow inadver-tently being set too low on a conventional mask and causing rebreathing of CO2. Nursing can communicate easily with patients without inter-rupting their oxygen therapy. Our therapists can assess and apply the required oxygen device and flow quickly and efficiently. We are very happy that we have chosen OxyMask as our on ly ox ygen ma sk for pa t i ent s a t St. Tammany Parish Hospital. ■
Lisa Kinler, RRT, is depart-ment head of Respiratory Services at St. Tammany Parish Hospital, a 235-bed, full-service acute care facility i n C o v i n g t o n , L a . OxyMask™and OxyTrach™ are registered trademarks of Southmedic.
■ case stuDy: oxyGen masKs
Improving patient CareAdjustable oxygen flow, quick assessments, and easy adjustments find favor with RTs and nurses.
30 ADVANCE for Healthcare Careers

Make the Season Memorable
1-877-776-6680advancecustompromotions.com
FESTIVE PROMOTIONS Delight patients and staff with these holiday-themed giveaways.
TOKENS OF APPRECIATION Say thanks with these seasonal favorites.
MEMORABLE GIFTS Recognize outstanding contributions with these luxurious gifts.
Reward staff, empower patients and celebrate the season with unique custom gifts and giveaways from ADVANCE. When you add your imprint to any of our
dozens of holiday products, you’ll be sure to celebrate the season in style.
NEED MORE PRODUCT IDEAS? CALL 1-877-776-6680 TO SPEAK WITH A CONSULTANT OR VISIT ADVANCECUSTOMPROMOTIONS.COM.
Candy Cane Key TagIMPRINT ON BACK
Holiday Cookie Cutter
Holiday Crayons Santa ClausStress RelieverIMPRINT ON BACK
Silver Snowflake Ornament
Mug Gift Set“Season’s Greeting” Card
IMPRINT ON INSIDE
Holiday Candle Set
Wave Art Glass Award Berlino Picture Frame
Spa Set in a BoxStainless Steel Mug Gift Set
169935_Holiday_Print.indd 1 9/28/12 10:11 AM
31ADVANCE for Healthcare Careers

32 ADVANCE FOR RESPIRATORY CARE & SLEEP MEDICINE October 2012 www.advanceweb.com/respiratory
C
AR
EE
R O
PP
OR
TU
NIT
IES New York
MIDDLE ATLANTIC
If you’re interested in exploring possibilities for career growth, consider New York Methodist Hospital. We’ve been a strong and stable presence in our community for more than 125 years, delivering service excellence in a friendly, positive and dynamic environment.
NEONATAL RESPIRATORY THERAPIST Full Time, Part-Time & Per-Diem Due to our continuous expansion, we have a Per Diem, 12-hour Shift position available. Must have very extensive NICU Critical Care experience.
Our Respiratory Therapy Department provides: • Protocols/Guidelines directed ventilatory
support/weaning • HFOV, HFPV, HFOPV • INO administration therapy
• High flow heliox therapy • Intubations • Point of care ABG analysis
You will provide: • The ability to utilize state-of-the-art equipment and provide expert care to the patients
Newly upgraded pay scale (includes experience, specialty credentials and shift differentials) and an excellent compensation package. To learn more about why New York Methodist Hospital is the borough’s most desirable hospital for employees as well as patients, or to apply, visit: www.nym.org/careers
We are an equal opportunity employer
EXPLORE YOUR FUTURE WWW.NYM.ORG/CAREERS
Get more out of your healthcare career in Brooklyn's Park Slope.
IS BETTER ATOPPORTUNITY
NEW YORK HARBOR HEALTHCARE SYSTEM
“START THE CAREER
OF A LIFETIME”
Registered Respiratory TherapistBrooklyn, NY
If you’re looking for a professional atmosphere where team work is present and quality care isthe name of the game, then the Department of Veterans Affairs New York Harbor Healthcare Systemis for you.
Successful candidate will be involved with Ventilator Management, Intubations, Arterial Blood GasAnalysis, Pulmonary Function Testing, Student Teaching, Patient Education, BCLS & ACLSinstruction available. State of the art equipment. Registered Applicants preferred.
Some of our benefits include: 10% shift differential, Sat & Sun Premium Pay, Excellent Salary &Benefits with a Great Retirement Plan.
Applicant MAY be eligible to apply for and participate in the Education Debt Reduction Program(EDRP). This program assists the employee in reducing their outstanding student loan(s).
Please send resumes to: [email protected]
The VA is an EOE M/V/F/H. U.S. Citizenship required.
CALL 800.355.1088
TIME TO RENEW YOUR FREE SUBSCRIPTION
LOOKING FOR A LOW-COST MAILER?CALL 800-355-5627 FOR ADVANCE REPRINTS!
1 Middle Atlantic . . . . . . . . . . . . . . . . p. 32 2 Lower South Atlantic. . . . . . . . . . . . .p. 33 3 Upper South Atlantic . . . . . . . . . . . . .p. 33 4 West South Central . . . . . . . . . . . . . .p. 34 5 Mountain . . . . . . . . . . . . . . . . . . . . . .p. 34 6 Southwest . . . . . . . . . . . . . . . . . . . . .p. 34 7 Pacific . . . . . . . . . . . . . . . . . . . . . . . .p. 34
Career Opportunities
FREE ADVANCE JOB FAIR & CAREER EVENTS
IN YOUR AREAWWW.ADVANCEWEB.COM/JOBFAIRS
RS 10.15.12REC.indd 32 10/11/12 7:04:12 PM
32 ADVANCE for Healthcare Careers

www.advanceweb.com/respiratory October 2012 ADVANCE FOR RESPIRATORY CARE & SLEEP MEDICINE 33
Florida, Virginia C
AR
EE
R O
PP
OR
TU
NIT
IES
UPPER SOUTH ATLANTIC
LOWER SOUTH ATLANTIC
Bon Secours Virginia Health System is seeking highly skilled professionals for our specially designed ground Critical Care Transport Team. Delivering world class care, our team is specialized in both adult and pediatric critical care, including cardiac (intra-aortic balloon pump & LVAD patients), NICU, PICU, and maternal fetal medicine. Ongoing training is provided including OR intubation rotations along with scenarios in our state-of-the-art high defi nition simulation labs. If you are a Respiratory Therapist, trained in NICU/PICU, interested in growing or expanding your career in ground transport, consider joining our team and deliver good help when it matters most. To learn more about our opportunities, competitive wages, and benefi ts packages, apply online at:
www.bonsecours.com or call (757) 213-7986 to speak with our recruiter today!
&&& hhourrss &&bbyy tthheeiirr siidde
After all tthhe advanced pprrocceeduurress
ff
cccccccchhhhhhheeeeccckkkkkk ooooooonnnnnn tttthhhhhhem when yyyyyyyyyyooouuuuuuurrrr ssssssssshhhhhhhhhhiiiiiiiffffffft is overyyyyyyyyyyyooooouuuuuuuurrr sssssssshhhiifft is over.
EOE
BLAKE MEDICAL CENTER, BRANDON REGIONAL HOSPITAL, CENTRAL FLORIDA REGIONAL HOSPITAL, DOCTORS HOSPITAL OF
SARASOTA, EDWARD WHITE HOSPITAL, ENGLEWOOD COMMUNITY HOSPITAL, FAWCETT MEMORIAL HOSPITAL, LARGO MEDICAL
CENTER, MEDICAL CENTER OF TRINITY, NORTHSIDE HOSPITAL, OAK HILL HOSPITAL, OSCEOLA REGIONAL MEDICAL CENTER,
REGIONAL MEDICAL CENTER BAYONET POINT, SOUTH BAY HOSPITAL, ST. PETERSBURG GENERAL HOSPITAL
TOGETHER, PERFORMING AT A HIGHER STANDARD™
HOSPITALSSTRONG
you’re devoted to caring.CAREGIVER
You’re not just a
We are on a journey to reach new heights in service excellence for our patients, their families and the communities we serve. We believe the path to success is by empowering and supporting our people — our caregivers who are committed to excellence and devoted to caring. When you go out of your way to help someone find their way, you know exactly what we mean.
To explore Seasonal Contract Opportunities, visit MoreSeasonalCareers.com
To learn about other opportunities available, visit MoreCareerChoices.com
Follow us on facebook.com/HCAWestFloridaCareers
Connect with us: linkedin.com/company/hca-west-florida
Follow us on our blog: recruitingatHCAwest.com
Visit Our Exciting Respiratory ForumsChat with your peers on myriad topics. Stop by our bustling online network at www.advanceweb.com/respiratory and click on the “community” tab.
JOB OPENINGS – SENT DIRECTLY TO YOUR E-MAILSIGN UP TODAY AT WWW.ADVANCEWEB.COM
RS 10.15.12REC.indd 33 10/11/12 7:04:14 PM
33ADVANCE for Healthcare Careers

34 ADVANCE FOR RESPIRATORY CARE & SLEEP MEDICINE October 2012 www.advanceweb.com/respiratory
C
AR
EE
R O
PP
OR
TU
NIT
IES Texas, Montana, New Mexico, California
MOUNTAIN
PACIFIC
SOUTHWESTWEST SOUTH CENTRAL
Come work with us in Silver City, New Mexico
near the Gila National Forest!
POSITION CURRENTLY AVAILABLE
POLYSOMNOGRAPHICTECHNICIAN
•RPSGT
•New Mexico License
APPLY ONLINE www.grmc.orgHuman Resources Contact
(575) 538-4076
Employment is contingent upon successful completion of pre-employment
drug and alcohol testing. GRMC is an Equal Opportunity Employer
Now hiring experienced NICU, Respiratory Therapists for
immediate assignments in Central Valley and Greater Los Angeles.
Per Diem/13 week Travel assignments. Top pay and benefi ts.
E-mail resume [email protected]
Livingston HealthCare, located in Livingston Montana, is a unique group of healthcare professionals providing services to the residents of Park County and surrounding communities. Included in those services are a 25-bed hospital (CAH), a multi-specialty physician practice, home care, hospice care, rehab, a sleep center and much more. Livingston HealthCare is accepting applications for the position of Registered Respiratory Therapist: Full time position with benefits. Pre-employment drug testing required. If you enjoy fly fishing, skiing and hiking, or if you just love the outdoors and are looking for a balance of lifestyle and career, complete application at www.livingstonhealthcare.org. For additional information call 406-823-6471.
Livingston HealthCare is an Equal Opportunity Employer.
Registered Respiratory Therapist
We’re looking for red-hot talent this winter!
Seasonal Plan in Central Texas
Not just a living. A way of life. Austin, Texas.
Adult & Pedi Registered Respiratory Therapists
Come work at Seton Healthcare Family. With 11 innovative hospitals throughout Central Texas, our Seasonal Plan will make your career sizzle!
13-26 week contract starts as early as October 2012 & runs through March 2013
Premium pay rates
Friendly staff, mild winters & no state income tax
Tell your friends, too!
Now is the best time to earn a little extra cash for the holidays. We have limited openings, so visit www.Seton.Seasonal-Careers.net today to find out more and sign up for a recruiter to contact you! EOE/AA/M/F/D/V
facebook.com/SetonCareers
@SetonCareers
CE DirectoryOur brand new directory will assist you in locating sources to obtain various forms of continuing education credits and advanced degrees. Visit www.advanceweb.com/respiratory.
Follow Us on Twitter Sign up to receive our “tweets” about new online content and links to stories elsewhere on the web. You’ll always know the latest health care informa-tion and what the ADVANCE editors are doing today. Visit http://twitter.com/advancerespcare.
FIND THOUSANDS OF JOBS ONWWW.ADVANCEWEB.COM
RS 10.15.12REC.indd 34 10/11/12 7:04:18 PM
34 ADVANCE for Healthcare Careers

Amazingly simple, advanced treatment for the entire OSA patient spectrum
Provent® Sleep Apnea Therapy successfully treats mild, moderate and severe OSA patients. Because Provent is well tolerated with excellent compliance, more OSA patients get on treatment and stay treated.
• Demonstrated efficacy across all patient severities
• Clinically proven in multiple studies
• Treated OSA patients have significantly lower risk of comorbidities
© 2012 Ventus Medical, Inc. Provent, Ventus Medical and the V logo are registered trademarks or trademarks of Ventus Medical, Inc., in the U.S. and other countries. The Provent device is covered by U.S. Patent Numbers 7,506,649, 7,735,492, 7,735,491, 7,856,979 and other pending U.S. and foreign patents. MSM0404-01_A
Therapy that sticks.
ProventTherapy.com / HCP1-888-SLP-WELL (1-888-757-9355)
Get more of your patients on treatment
Proven option for all OSA patients
12-VTM-058 Provent Full Page Ad for Advance_v1.indd 1 7/30/12 4:19 PM
35ADVANCE for Healthcare Careers
Clear the Way for Better OutcomesEvery day, around the world, we enhance outcomes for our patients and their caregivers.
To order today, call 800-426-4224, option #3, or contact your local sales representative.
The MetaNeb® SystemAvailable for Acute Care
The MetaNeb® System is indicated for lung expansion therapy, the mobilization of secretions, and the treatment and prevention of pulmonary atelectasis. The system is very simple and easy to use.
The Vest® Airway Clearance System, Model 105 (Home Care) is distributed by Advanced Respiratory, Inc. a Hill-Rom Company
The Vest® Airway Clearance System, Model 205 (Acute Care/Long-term Care) is distributed by Hill-Rom
MetaNeb® is a registered trademark of Comedica, Inc.
© 2012 Hill-Rom Services, Inc. ALL RIGHTS RESERVED
The Vest® Airway Clearance SystemAvailable for Home Care and Acute Care
The Vest® Airway Clearance System provides safe, easy-to-use and effective therapy that can eliminate the need for patient repositioning and reduce the time spent delivering therapy.
36 ADVANCE for Healthcare Careers