VESTIBULAR SYSTEM - smbs.buffalo.edu · From Principles of Neural Science by Kandel, Schwartz, and...
6
1 VESTIBULAR SYSTEM Objectives: • Understand the functions of the vestibular system: What is it? How do you stimulate it? What are the consequences of stimulation? • Describe the vestibular apparatus, the 2 vestibular organs, and their unique sensory receptors • Describe the 1st and 2nd order neurons in vestibular pathways • Describe the pathways mediating vestibular perception and reflexes • Understand the importance of vestibular tests for clinical assessment • Describe: 1) acoustic neuroma and its the symptoms 2) benign paroxysmal positional vertigo 1. Case Description: A 70 year-old woman complains of severe episodes of dizziness over the past month. She reports the following symptoms: • When she awakens in the morning and rolls over in bed, she feels like the room is spinning around her. This usually lasts only about 20 sec, but sometimes it is accompanied by nausea and a few times she has vomited. She also says that sometimes she has a brief period of dizziness when she stands or when she shakes her head to answer “No”. Last week when this happened, she fell and hurt her shoulder. When you question her, she remarks that her hearing has not changed and she has no ringing in her ears. Questions: 1. What does she mean by dizziness? 2. What is relationship between: spinning room, nausea/vomiting, falling, hearing, ringing in ears? 3. What causes this condition? 2. Function – Vestibular Sensation •Vestibular sensation provides information to the CNS about movement and position of the head in space. The purpose of this information is: • Conscious perception of head movement and position • Reflexive control of: • Posture and balance – by adjusting body muscles • Head Position – keep head upright on shoulders • Eye-head coordination – keep eyes fixed on visual targets (vestibulo-ocular reflex) • Autonomic Centers in brainstem •Principally a REFLEXIVE system with a conscious pathway of lesser importance. 3. Vestibular Receptors •Inner ear (labyrinth) is made up of bony and membranous portions. •Membranous labyrinth is filled with endolymph secreted by specialized areas of the epithelium; perilymph fills the space between the membranous labyrinth and bone. From Principles of Neural Science by Kandel, Schwartz, and Jessell, Appleton 1991 Deficits cause: Vertigo Falling Tilting Nystagmus Nausea, vomiting
Transcript of VESTIBULAR SYSTEM - smbs.buffalo.edu · From Principles of Neural Science by Kandel, Schwartz, and...
1
VESTIBULAR SYSTEM Objectives:
• Understand the functions of the vestibular system: What is it? How do you stimulate it? What are the consequences of stimulation?
• Describe the vestibular apparatus, the 2 vestibular organs, and their unique sensory receptors • Describe the 1st and 2nd order neurons in vestibular pathways • Describe the pathways mediating vestibular perception and reflexes • Understand the importance of vestibular tests for clinical assessment • Describe: 1) acoustic neuroma and its the symptoms 2) benign paroxysmal positional vertigo
1. Case Description: A 70 year-old woman complains of severe episodes of dizziness over the past month. She reports the following symptoms:
• When she awakens in the morning and rolls over in bed, she feels like the room is spinning around her. This usually lasts only about 20 sec, but sometimes it is accompanied by nausea and a few times she has vomited. She also says that sometimes she has a brief period of dizziness when she stands or when she shakes her head to answer “No”. Last week when this happened, she fell and hurt her shoulder. When you question her, she remarks that her hearing has not changed and she has no ringing in her ears. Questions: 1. What does she mean by dizziness? 2. What is relationship between: spinning room, nausea/vomiting, falling, hearing, ringing in ears? 3. What causes this condition?
2. Function – Vestibular Sensation
•Vestibular sensation provides information to the CNS about movement and position of the head in space. The purpose of this information is: • Conscious perception of head movement and position • Reflexive control of:
• Posture and balance – by adjusting body muscles • Head Position – keep head upright on shoulders • Eye-head coordination – keep eyes fixed on visual targets (vestibulo-ocular reflex) • Autonomic Centers in brainstem
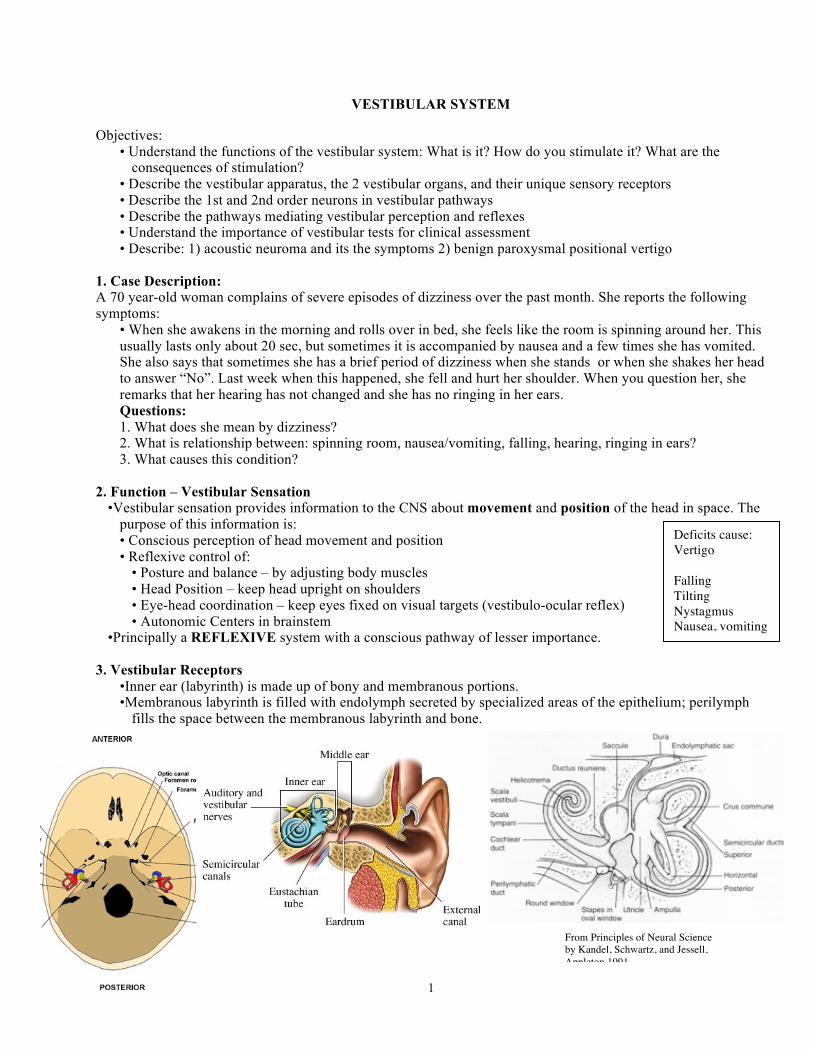
•Principally a REFLEXIVE system with a conscious pathway of lesser importance. 3. Vestibular Receptors
•Inner ear (labyrinth) is made up of bony and membranous portions. •Membranous labyrinth is filled with endolymph secreted by specialized areas of the epithelium; perilymph
fills the space between the membranous labyrinth and bone.
From Principles of Neural Science by Kandel, Schwartz, and Jessell, Appleton 1991
Deficits cause: Vertigo Falling Tilting Nystagmus Nausea, vomiting
2
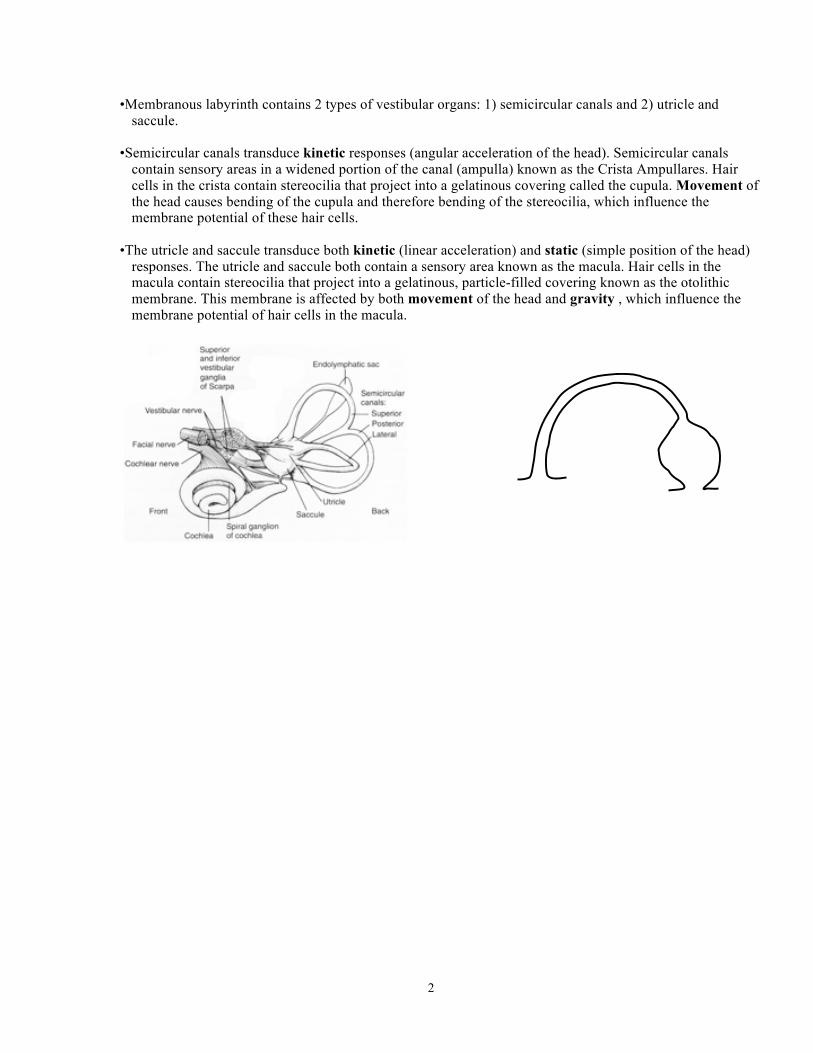
•Membranous labyrinth contains 2 types of vestibular organs: 1) semicircular canals and 2) utricle and saccule.
•Semicircular canals transduce kinetic responses (angular acceleration of the head). Semicircular canals
contain sensory areas in a widened portion of the canal (ampulla) known as the Crista Ampullares. Hair cells in the crista contain stereocilia that project into a gelatinous covering called the cupula. Movement of the head causes bending of the cupula and therefore bending of the stereocilia, which influence the membrane potential of these hair cells.
•The utricle and saccule transduce both kinetic (linear acceleration) and static (simple position of the head)
responses. The utricle and saccule both contain a sensory area known as the macula. Hair cells in the macula contain stereocilia that project into a gelatinous, particle-filled covering known as the otolithic membrane. This membrane is affected by both movement of the head and gravity , which influence the membrane potential of hair cells in the macula.

3
3. Hair Cells • Innervated by afferent and efferent fibers of cranial nerve VIII. • At their apical ends contain a single, long kinocilium followed by 50-60 stereocilia of decreasing length
resulting in a polarized morphology Þ Bending of hair bundle toward or away from kinocilium results in either depolarization or hyperpolarization of hair cell.
• Hair cells are surrounded by supporting cells 4. First Order Neurons (Vestibular Ganglion)
•Cell Bodies in Vestibular Ganglion (Scarpa’s Ganglion) •Bipolar neurons •Peripheral process contacts hair cells in macula and crista •Central process travels in vestibular division of CN VIII to enter
brainstem at cerebellopontine angle. • axons synapse on vestibular nuclei in brainstem AND
cerebellum (via the inferior cerebellar peduncle).
5. Vestibular Nuclei (second order neurons) •4 components: inferior, medial, lateral, and superior •Located laterally in the floor of the 4th ventricle; they extend from pons (level
of abducens nucleus) to medulla. Lesions in this area of brainstem cause vestibular symptoms.
•Project to: cerebellum, nuclei of III, IV, VI, and spinal motoneurons. •Vestibular nuclei act together with the cerebellum. They communicate via axons that travel in the inferior cerebellar peduncle.
6. Central Pathways
A. Conscious information: Vestibular Nuclei ----® VPL ---® Parieto-temporal cortex (near postcentral gyrus)
• Pathway details are unknown. • Vestibular lesions cause vertigo (perceived motion in the absence of real
movement). • Control of Balance
The vestibular system participates with the visual and tactile sensory systems to create our perception of motion and spatial orientation. Disorders in any of these systems can cause unsteadiness (eg: visual system- have you been to an IMAX movie?). Normal vestibular function is required to maintain balance because vertigo has an over-riding effect on balance. The visual system is used for external reference to the horizon and proprioception provides information about body orientation. Visual information can Assuming normal vestibular function, the Romberg test assesses normal proprioception when the eyes are closed.
From Principles of Neural Science by Kandel, Schwartz, and Jessell, Appleton 1991

4
B. Reflexive Control: 1) Posture and Balance
• axons from lateral vestibular nucleus travel ipsilaterally in LVST to spinal motoneurons throughhout all cord levels; provide tonic excitation to extensor muscles to counter gravity and maintain upright posture. Lesions cause falling to same side.
2) Head Position • axons from medial vestibular nucleus travel bilaterally in MVST to cervical
motor neurons innervating neck muscles; acts to maintain upright head position, which aids visual discrimination. Lesions cause head tilt or oscillation (titubation).
3) Coordinates Eye-Head Movement by Vestibulo-ocular reflex • maintains a visual target on the fovea during head roation by
moving the eyes in the opposite direction. •axons from vestibular nuc. travel bilaterally in MLF to synapse on
nuclei of VI, IV, and III to adjust eyes in all 3 planes of head movement.
• Lesions cause nystagmus ( 4) Autonomic centers for Vomiting in medulla and pons
•2 areas involved in nausea and vomiting and communicate with vestibular nuclei: A. Chemoreceptor Trigger Zone (CTZ) in rostral medulla (caudal end of 4th ventricle). This area lacks
blood brain barrier and senses chemical stimuli (drugs, toxins) in blood and CSF. B. Vomiting Center in lateral Reticular Formation of medulla.
• Vestibular lesion cause nausea/vomiting.
Tract Origin Destination Function Lat Vestibulospinal t Lat Vestibular Nuc Spinal Motor System Posture, Balance Med Vestibulospinal t Med Vestibular Nuc Cervical motor sys
controlling neck muscles Upright Head posture
MLF All Vestibular Nuc CN Nuc III, IV, VI Eye-head coordination
Autonomic reflexes Vestibular Nuc Reticular Formation(CTZ) Nausea, vomiting 7. Responses Induced by Vestibular Stimulation
•Vertigo – the illusion of motion; sensation of world turning although head is stationary. •this should be distinguished from “dizziness”, a nonspecific term patient’s use to describe any of the
following; 1) vertigo, 2) feeling of faintness (typically due to decreased blood supply, oxygen, or glucose to the brain), 3) disequilibrium– unsteady gait (problem of motor system), 4) lightheadedness (a psychological symptom of anxiety, stress, etc.)
•Loss of Balance/Falling (towards side of lesion), past pointing •Nystagmus – rapid oscillating movements of eyes; has slow and fast components in opposite directions •Nausea, vomiting

5
8. Thinking about vestibular deficits and vestibular pathways
• Symptoms: You must be able to recognize vestibular symptoms in patients, which are a key indicator of vestibular system involvement.
• Source of symptoms: Vestibular symptoms can be caused by peripheral (vestibular apparatus or nerve) or central lesions. These 2 locations can cause symptoms with somewhat different characteristics that help to localize their source.
• For lesions in the CNS: • It is unlikely that a lesion will affect a single tract of the vestibular pathways and cause a single
symptom. However, MS can produce localized lesions in the MLF. • Vestibular symptoms in patients are more likely to be multiple (eg a combination of vertigo, loss of
balance, nausea, nystamus). In this case the likely source of the lesion is in the vestibular nuclei (or vestibular parts of the cerebellum that we will cover later).

6
Acoustic neuroma
9. Clinical Testing/Conditions • Oculocephalic Reflex (aka Doll's Eye Maneuver) for unconscious patients without neck injury.
• in a normal, conscious patient - when the head is rotated manually, the eyes usually are not fixated on a visual object so they move in the direction of rotation.
• in an unconscious patient - the vestibulo-ocular reflex dominates, so head rotation should elicit conjugate eye movements in opposite direction to head rotation if the pathways that mediate the reflex are intact.
• Caloric test – Cold/warm water in external ear; used instead of Doll’s Eye Maneuver if neck injury is suspected and tympanic membrane is intact.
• Barany chair (for conscious patients) – controlled rotation to patient to stimulate vestibular system. • CASE: On returning home from shopping, a wife finds her 59 year-old husband unconscious
on the floor. He has no pulse. After calling 911, she begins CPR. When Mr. T arrives in the ED, he is in ventricular fibrillation. Spontaneous circulation is eventually restored, but Mr. T remains comatose. After 3 days in coma, his wife asks about her husband’s condition and the probability of a good outcome. • How can we assess extent of CNS damage/function in unconscious patient
1. Somatosensory Evoked Potential Brainstem Reflexes assess functionality of pathways in brainstem. Loss of reflex indicates poor outcome; however, intact reflex does not imply cortical functionality. 2. Corneal reflex 3. Pupillary constriction reflex 4. Oculocephalic Reflex or Caloric test
•Acoustic Neuroma: a benign, slow growing tumor of schwann cells
of CN VIII within the internal auditory canal. Causes vestibular and auditory symptoms including unsteadiness, vertigo, hearing loss, and tinnitus. If large, it can involve CN V and CN VII.
10. Case Discussion:
1. What does she mean by dizziness? >vertigo 2. What is relationship between: spinning room, nausea/vomiting, falling,
hearing, ringing in ears? • spinning room, nausea/vomiting, falling are symptoms of vestibular over-stimulation. Hearing loss and ringing in ears are auditory symptoms that would indicate involvement of CN VIII.
3. What causes this condition? • Benign Paroxysmal Positional Vertigo (BPPV): a nonprogressing condition characterized by brief periods of
severe vertigo; Provoked by sudden change in head position; Causes: idiopathic/normal aging, head trauma, infection.
• Pathophysiology: otoconia become dislodged from otolithic membrane, move in endolymoph into semicircular canals and stimulate crista abnormally.
•Treatment: Otolith Repositioning Procedure (rotating head moves otoliths into vestibule); in refractory cases, surgery on semicircular canal or vestibular nerve fibers may be used.
National Center for Emergency Medicine Informatics, http://www.ncemi.org/