
Vertical Ridge Augmentation
43
Company Logo Jun chan g hun @ VERTICAL RIDGE AUGMENTATION 가가가가가가가 가가가 가가가가가가가
description
Clinical management of lost vertical bone ridge dimension
Transcript of Vertical Ridge Augmentation

CompanyLogo
Jun chang hun
@
VERTICAL RIDGE AUGMENTATION
가천의과대학교 길병원 구강악안면외과
Jun chang hun
Edentulism
Once the teeth are lost, a continuous resorptive process Results
Diminished volume and strength of residual bone Loss of facial vertical dimension Impaired masticatory function Difficulty choosing a balanced diet Speech difficulty Facial soft tissue changes Pathologic fracture possibility
Jun chang hun
SITE DEVELOPMENT
Reconstruction of deficient alveolar ridges that lacks sufficient volume, contour, or height
Ultimate surgical goal Restore function, form, and long-term stability
Surgical approach selection Type, size, and shape of the defect Surgical expertise or experience level of surgeon Intended direction of the augmentation

Jun chang hun
SITE DEVELOPMENT
Hard tissue management Ridge(socket) preservation Ridge augmentation
Vertical ridge augmentation Horizontal ridge augmentation
Soft tissue management
Jun chang hun
SITE DEVELOPMENT
Hard tissue management Ridge(socket) preservation Ridge augmentation
Vertical ridge augmentation Horizontal ridge augmentation
Soft tissue management

Jun chang hun
Defect size
Small edentulous segments (such as single tooth) Particulate autogenous bone with membrane (Fugazzotto 1997)
Large ridge reconstructions Controversial (Lang et al 1994, Chiapasco et al 1999)
Autogenous block bone Extra-oral Intra-oral
Distraction (>5mm vertical deficiency)

Jun chang hun
TMI
Bosker Transmandibular Implant (TMI) In the late 1970s Without the need for autologous bone graft Technique sensitive both surgeon & prosthodontist Significant “reversible complication” rate
22.2% (Keller et al, Int JOMI 1986;1:101) Infection, superstructure fx, mandible fx, fail to osseointegrate

Jun chang hun
Ridge augmentation methods
Bone grafting Biomaterials GBR Alveolar distraction osteogenesis
Jun chang hun
Distraction Osteogenesisfor vertical ridge augmentation
History 1992, McCarthy and coworker 1996, Block & colleager ; dog 1996, Chin & Toth ; DO & Implant
Advantage No additional surgery involving a harvesting procedure No limit to lengthening Simultaneous lengthening of surround soft tissue
Dis-advantage Long treatment period Need for suitable distractor Danger of infection
Ilizarov (1989) Preservation of blood supply at the corticotomy site
Kojimoto & coworkers (1988) Preservation of periosteum : distraction Vestibular incision rather than crestal incision
Jun chang hun
Ridge augmentation methods
Bone grafting Biomaterials GBR (Guided Bone Regeneration) Alveolar distraction osteogenesis
Jun chang hun
Titanium membrane only
Cornelini (2000) Ti-memb only, 3mm vertical ridge augmentation

Jun chang hun
Simultaneous implant placement and vertical ridge augmentation with a titanium-reinforced
membrane: A case report
Vertical ridge augmentation with titanium reinforced memb. 2nd surgery : 12 months later 3mm hard tissue augmentation 2mm dense connective tissue covered the newly formed bone
Cornelini R, Cangini F, Covani U, Andreana S (Int JOMI, 2000;15:883-888)

Jun chang hun
Ridge augmentation methods
Bone grafting Biomaterials GBR Alveolar distraction osteogenesis

Jun chang hun
Autogenous bone graft
Gold standard for bone augmentation procedures
Block bone or particulate forms Block bone - reduced osteogenic activity & slow revascularizatio
n than particulate bone marrow Extra-oral or Intra-oral donor-site
Intraoral harvested intramembraneous bone graft may have minimal resorption, enhanced revascularization, and better incorporation at the donor site
Jun chang hun
Autogenous bone graft
Advantage Osteogenic potential Block grafts that maintain form and shape Ability to correct any size or shape deformity Elimination of the possibility for an immunogenic reaction
Disadvantage 2nd surgical intervention Morbidity associated with the donor site Unpredictable bone resorption Longer recovery period Difficulty in managing soft tissue coverage Increased treatment time Increased risks

Jun chang hun
Autogenous block bone grafts
Width deficiency Veneer or saddle graft Most predictable and resistant to resorption
Vertical deficiency Onlay or saddle graft Difficult to gain and maintain, high resorption rate
Combined deficiency

Jun chang hun
Donor Sites of Autogenous Bone
Cortical Bone Mandible, Cranium
Cancellous Bone Mx. Tuberosity Inner Cancellous part
Cortico-Cancellous Bone Iliac bone

Jun chang hun
Intra-oral vs Extra-oral
Kusiak et al (1985) Intramembranous bone grafts accelerate revascularization and healing
as compared to endochondral bone grafts Cortical membranous grafts revascularize more rapidly than endochon
dral bone graft with a thicker cancellous part Zins & Whittacker (1983), Philips & Rhan (1990)
Membranous bone (such as mandible) undergoes less resorption than endochondral bone (such as iliac crest)
Intraoral harvested intramembraneous bone grafts Minimal resorption Enhanced revascularization Better incorporation at the donor site

Jun chang hun
Iliac bone
Jun chang hun
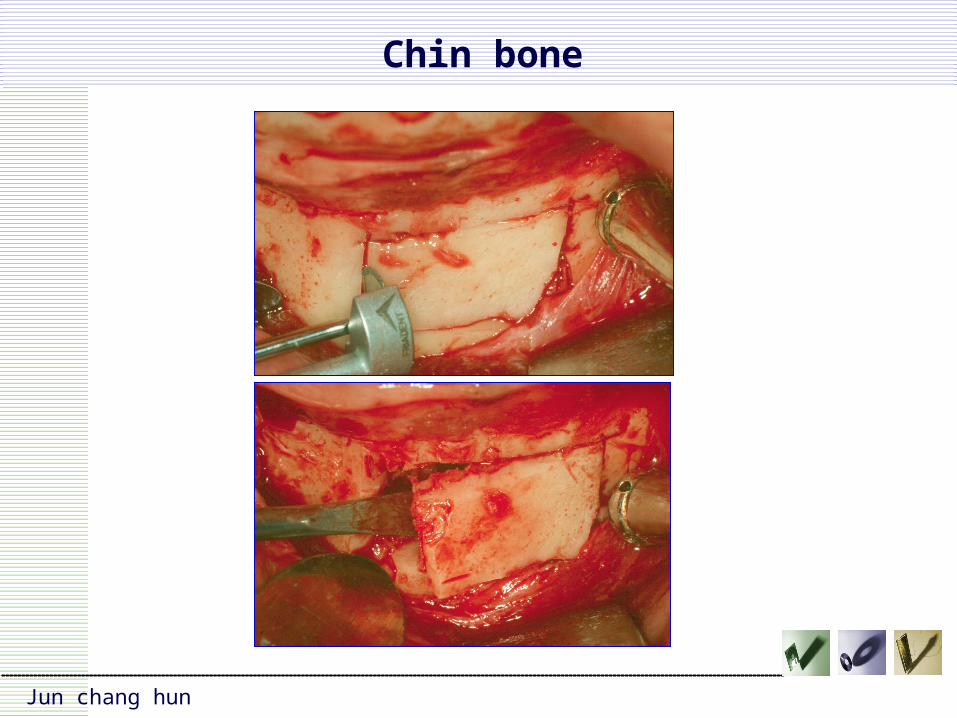
Chin bone

Jun chang hun
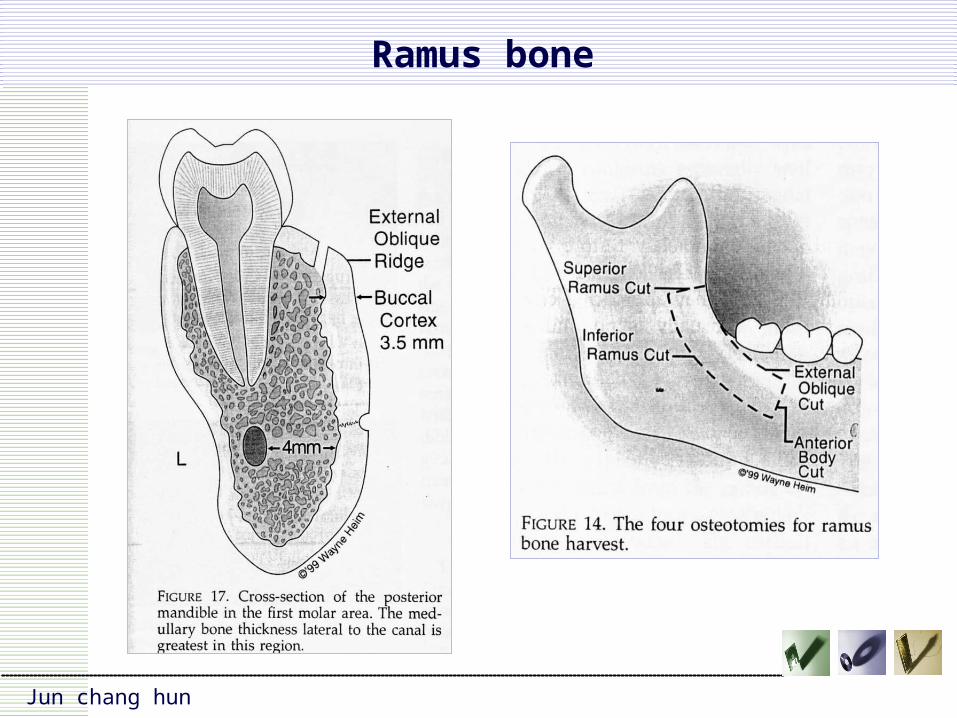
Ramus bone
Jun chang hun
Ramus bone
Jun chang hun
Chin vs Ramus
Complication (chin vs ramus) Less cosmetic concern Less wound dehiscence No gingival recession Less sensory disturbance Less discomfort complain Trismus & edema (medication)

Jun chang hun
Parameter Symphysis Ramus
Surgical access Good Fair to good
Cosmetic concern High Low
Graft shape Thick rectangular Thinner rectangular veneer
Graft Size >1cm3 <1cm3
Graft Morphology Corticocancellous Cortical
Graft Resorption Minimal Minimal
Healed Bone Quality Type 2>type 1 Type1>Type2
Post-OP pain/edema
Moderate Minimal to moderate
Teeth Common(temporary) Uncommon
Nerve damage Common(temporary)Uncommon
Incision dehiscence Occasional(Vestibular) Uncommon
Chin vs Ramus
Jun chang hun
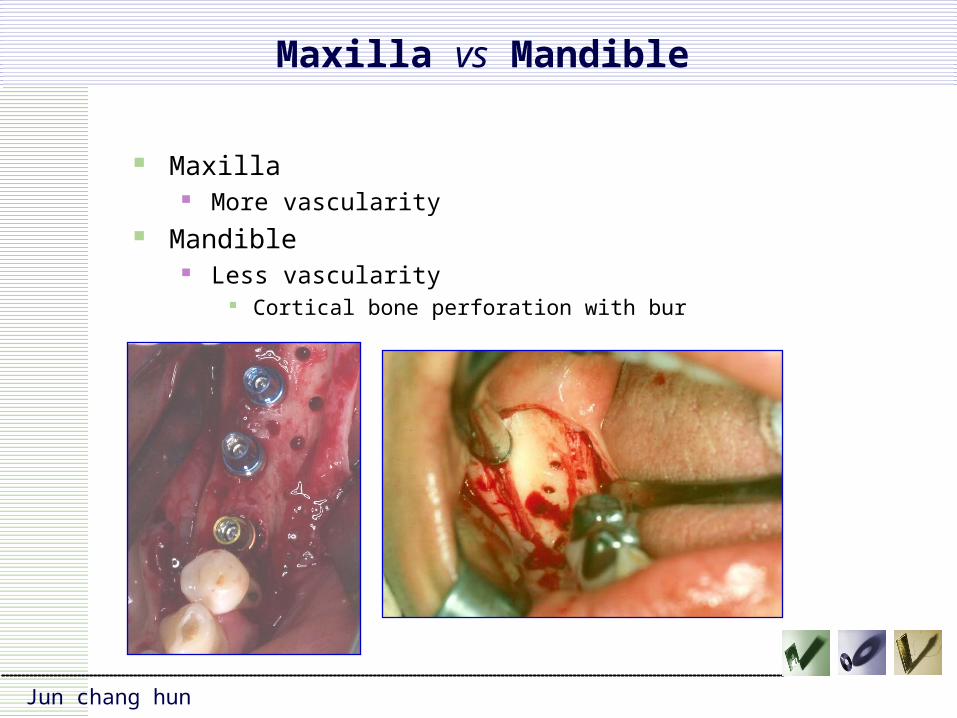
Maxilla vs Mandible
Maxilla More vascularity
Mandible Less vascularity
Cortical bone perforation with bur

Jun chang hun
Critical Success Factors
Stability of grafting materials Condition of recipient sites No infections Resistance to resorptions Soft tissue coverage

Jun chang hun
Stability of grafting materials
Bony irregularity contouring Graft fixation
Block bone : at least 2 fixation screws for immobilization

Jun chang hun
Condition of recipient sites
Inlay graft (3~4 wall defect) More favorable
Onlay graft (1~2 wall defect) More prone to resorption

Jun chang hun
Infection
Disrupt the process and halts the growth of new bone
Rupture of the soft tissue closure Block graft exposure
Exposure time (2002, proussaefs) Late exposure : no clinical & histologic sign of pathosis or necrosis Early exposure : partial or total necrosis
Fixation screw infection Adjacent teeth(structure) pathologic conditions

Jun chang hun
Resistance to resorption
Immobilization Satisfactory to restore mandibular volume
In function the grafted bone underwent rapid resorption Onlay graft
Use membranous bone & graft stability (Philips & Rhan 1990)
Cortical bone Use of membrane Adequate implant placement timing

Jun chang hun
Soft tissue coverage
Crestal incision with releasing incisions Lingual flap
Mesially at least 3 teeth include Raise extending beyond mylohyoid muscle
Tension-free suture Mattress suture : contact over 3mm Soft tissue graft
Free graft : FGG, CT Pedicle graft : palatal or labial

Jun chang hun
Controversy
1 stage surgery (bone graft & implant placement) Single surgical intervention Potentially reduced healing time
2 stage surgery Prosthetically better implant placement Superior esthetics

Jun chang hun
1 stage surgery
1 stage surgery (bone graft & implantation) Long-term implant survival rates : 25~100% Implant position & angulation are critical factors Implant survival alone does not predict successful restoration of occlu
sion
Verhoeven et al 1997 Carr & Laney 1987 Marx & Morales 1988

Jun chang hun
Advantage of delayed implantation
Reducing the infection rate & graft failure rate Proper angulation & more precise positioning
After 5 years of masticatory functional loading Onlay grafting & simultaneous implantation in maxilla
Success rate : 51~83% Secondary implantation
Schliephake et al (1997, JOMS) 20% higher success rate

Jun chang hun

Jun chang hun
Resorption rate
Proussaefs, Lozada et al (2002) Block graft with Bio-oss : 16.34 %, 17.58 %
Cordaro et al (2002) Block bone : Mn 41.5%, Mx 43.5% (mean 42%)
Wang and colleagues (1976) : onlay bone graft During the first 3 years : 14%~100%
Bell et al (2002) Iliac crest block bone : 33%

Jun chang hun
The use of ramus autogenous block grafts for vertical alveolar ridge augmentation and implant placement: A pilot study
Ramus block autograft for vertical alveolar ridge augmentation Ramus block bone, Fixation screws, Periphery : Bio-Oss 4~8 months later : HA implant (Steri-Oss)
Results Radiographic
6.12 mm (1 month) 5.12 mm (4~6 months) : 16.34 % Laboratory volumetric
0.91 mL (1 month) 0.75 mL (6 months) : 17.58 % Peripheral pariculate bone (Bio-Oss)
Bone (34.33%), fibrous tissue (42.17%), residual Bio-Oss particle (23.50%) Discussion
Early exposure appeared to compromised the results, while late exposure did not affect the vitality of the block autografts
Proussaefs P, Lozada J, Kleinman A, Rohrer M (Int JOMI 2002;17:238-248)

Jun chang hun
Clinical results of alveolar ridge augmentation with mandibular block bone grafts in partially edentulous patients prior to implant placement
15 partially edentuous patients Ramus & symphysis block bone Fixed with titanium screw After 6 months screw remove, implant placed 12 months later implant supported fixed bridges
Mean reduction rate Lateral : 23.5% Vertical : 42 % Mandibular site more resorption rate than maxillary sites
GroupsNo. of aug. sites
Lateral aug. at bone grafting
Lateral aug. at implant placement
% reduction of lateral aug.
Vertical aug. at bone grafting
Vertical aug. at implant placement
% reduction of vertical aug.
Group 1 & 2 18 6.5+0.33 5.0+0.23 23.5% 3.4+0.66 2.2+0.66 42%
Group 1 : Mx 10 6.5+0.6 5.2+0.4 20% 4.75+1.5 2.75+1.5 41.5%
Group 2 : Mn 8 6.5+0.37 4.75+0.12 27.5% 2.4+0.2 1.4+0.2 43.5%
Cordaro L, Amade DS, Cordaro M (Clin oral impl res, 2002;13:103-111)

Jun chang hun
Staged reconstruction of the severely atrophic mandible with autogenous bone graft and endosteal implants
Materials and Methods Vertical mandibular height <7mm (atrophic mandible) Iliac crest bone graft to the mandible via an extraoral approach After 4~6 months, implantation
Results Mean pre-op bone height : 9mm (midline), 5mm (body) Before implantation (4~6months) vertical bone loss : 33% After implantation (24 months)
Non-implant supported region bone loss 11% per year Implant-supported region bone loss negligible
Conclusions (improve success rates) Prosthetically sound implant positioning Provide an affordable reconstructive option Staged reconstruction
Bell RB, Blakey GH, White RP, Hillebrand DG, Molina A (JOMS, 2002;60:1135-1141)

Jun chang hun
Complications of grafting in the atrophic edentulous or partially edentulous jaw
Intraoperative complications Bone
Insufficent donor material Over-reduction Inadequate fixation
Soft tissue Perforation Inability to mobile
Teeth Root damage
Other anatomy Sinus : membrane tear Nerve injury
Postoperative complications Gerneral
Infection Bone
Excessive resorption(early exposure, loss of graft)
Inadequate bone for implant Soft tissue
Hematoma Flap retraction Flap necrosis Color or tissue-type mismatch Loss of papilla Shallowing of vestibule
Teeth External root resorption
Other anatomy Sinusities Nasal bleeding Oroantral fistula
Bahat O, Fontanesi RV Int JPRD 21:487-495 2001

CompanyLogo
Jun chang hun
@
CASE REPORT
LINK
Jun chang hun
Conclusions
Autogenous block bone graft (chin or ramus) 5~7mm gaining About 30% resorption rate
Staging the grafting and implant procedure

Jun chang hun
Primary stability (+) Exposed threads can be covered with autogenous bone associated
with a membrane Jovanovic et al (1992), Jovanovic & Buser (1994), Giovannolli & Ren
ouard (1995), Antoun et al (1996) Primary stability (-)
Ridge augmentation should be performed before implantation


















![Continuous advancements in the field of implant …implants, vertical ridge augmentation and lifting the si-nus membrane to increase the available length for im-plant placement [4].](https://static.fdocuments.us/doc/165x107/5f09fcd87e708231d4297801/continuous-advancements-in-the-field-of-implant-implants-vertical-ridge-augmentation.jpg)