Version Type of Date Description of change change… · V06 Review Apr 19 V06.1 Update Jul 19...
37
Document Title Trust Standard for the Assessment and Management of Physical Health Reference Number CNTW(C)29 Lead Officer Group Nurse Director – Safer Care – Anne Moore Author(s) (name and designation) Group Medical Director – Dr Jonathan Richardson Ratified by Business Delivery Group Date ratified April 2019 Implementation Date April 2019 Date of full implementation April 2019 Review Date April 2022 Version number V06.1 Review and Amendment Log Version Type of change Date Description of change V06 Review Apr 19 V06.1 Update Jul 19 Inclusion of body mapping V06.2 Update Nov 19 Governance Changes This policy supersedes the following document which must now be destroyed: Reference No: Title CNTW(C)29 – V06 Trust Standard for Physical Assessment and Examination Policy
Transcript of Version Type of Date Description of change change… · V06 Review Apr 19 V06.1 Update Jul 19...

Document Title Trust Standard for the Assessment and Management of
Physical Health
Reference Number CNTW(C)29
Lead Officer Group Nurse Director – Safer Care – Anne Moore
Author(s) (name and designation)
Group Medical Director – Dr Jonathan Richardson
Ratified by Business Delivery Group
Date ratified April 2019
Implementation Date April 2019
Date of full implementation
April 2019
Review Date April 2022
Version number V06.1
Review and Amendment
Log
Version Type of change
Date Description of change
V06 Review Apr 19
V06.1 Update Jul 19 Inclusion of body mapping
V06.2 Update Nov 19 Governance Changes
This policy supersedes the following document which must now be destroyed:
Reference No: Title
CNTW(C)29 – V06 Trust Standard for Physical Assessment and Examination Policy

CNTW(C)29
1 Cumbria Northumberland, Tyne and Wear NHS Foundation Trust CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.2-Nov 19
Trust Standard for the Assessment and Management of Physical Health
Section Contents Page No:
1 Introduction 1
2 Purpose 1
3 Duties and Responsibilities 2
4 Procedure for physical examination – inpatient services 4
5 Physical health review following admission 6
6 Physical interventions 6
7 Healthcare of service users who are in-patient for over one year
7
8 The deteriorating patient 7
9 Recommended equipment for in-patient psychiatric units 8
10 Physical healthcare of service users treated in the community
8
11 Completion of core physical health monitoring record 12
12 Medication recording 16
13 Diagnosis ICD10 16
14 Procedure and minimum standards – children and adolescent services
17
15 Training 17
16 Identification of Stakeholders 18
17 Equality and Diversity 18
18 Implementation 18
19 Abbreviations 19
20 Monitoring compliance 19
21 Fraud, bribery and corruption 19
22 Fair blame 20
23 Associated documentation 20
24 References 21
Standard Appendices
A Equality Impact Assessment Tool 22
B Communication and Training Needs Information 24
C Monitoring Tool 26
D Policy Notification Record Sheet - click here

CNTW(C)29
2 Cumbria Northumberland, Tyne and Wear NHS Foundation Trust CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.2-Nov 19
Appendices – listed with the policy
Appendix No:
Description
1 Physical Health Monitoring Guidance
2 Guidance for ECG monitoring
3 Body Mapping Adult
4 Body Mapping Child
Practice Guidance Notes– Listed separate to policy
PGN No: Description
AMPH-PGN-01 Venous Thromboembolism: Reducing the Risk PGN
AMPH-PGN-02 Enteral Feeding Overview PGN
AMPH-PGN-02.1 PEG Feeding PGN
AMPH-PGN-02.2 NG Feeding PGN
AMPH-PGN-03 National Early Warning Scores
AMPH-PGN-04 Urethral catheterization PGN
AMPH-PGN-05 Sepsis Assessment Tool PGN
AMPH-PGN-07 Oral Motor Device/Chewy Tube PGN
AMPH-PGN-08 Battery Ingestion Draft
Draft
AMPH-PGN-09 Lower urinary Tract Infection
AMPH-PGN-10 Intramuscular Injection (IMI)
AMPH-PGN-11 Bowel Care Management in Adults, Children and Young People

CNTW(C)29
1 Cumbria Northumberland, Tyne and Wear NHS Foundation Trust CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.2-Nov 19
1 Introduction 1.1 People with a Learning Disability or Mental Health problems are more likely than
other citizens to have significant health risks and develop major physical health problems. Once they have developed a physical illness both groups are likely to die younger. (Disability Rights Commission-Equal Treatment: Closing the Gap, 2006). Improving Health and Lives (Department of Health), Health Inequalities and People with LD in the UK 2010
1.2 It is Cumbria Northumberland, Tyne and Wear NHS Foundation Trust’s (the Trust/CNTW) intent that all service users will receive a core assessment and review of their physical health needs, and all service users admitted to hospital will receive a full physical examination. This policy describes the minimum standard of physical assessment that a service user can expect and may be supplemented by additional guidance in relation to emergent guidance, locally agreed protocol and relevant CQUIN requirements as they occur.
1.3 These standards also apply to service users admitted for routine respite care. 1.4 All service users resident in an inpatient facility for more than 12 months will
have a documented review of their physical health every 6 months, and a full physical examination every year, more frequently if clinically indicated. This review will include a documented medication review.
1.5 All assessments and interventions must be considered on a case by case basis
and should be clinically appropriate. 2 Purpose
2.1 Physical examinations and any clinical interventions will be offered in line with
the Trust’s policies, CNTW(C)05 - Consent to Examination and Treatment, and CNTW(C)34 - Mental Capacity Act. There are areas of the Trust that undertake a variety of clinical interventions. These will be supported by the Practice Guidance Notes (PGNs) index attached to this policy.
2.2 This policy guidance should be used in conjunction with the Trust’s policy CNTW(C)20 - Care Coordination and Care Programme Approach Process.
2.3 Each service area will identify how their service will meet the minimum
standards described in this policy, and address any additional needs of service users cared for within that area.
2.4 It is emphasized that these are minimum standards and some services may
require a more rigorous examination. Expert advice should be sought from specialist services when specific conditions are already established or identified in the course of assessment, for example, diabetes, coronary heart disease, asthma, chronic obstructive pulmonary disease (COPD), infections and epilepsy. In order to inform care plans, on-going treatment regimes should be regularly reviewed and documented.
2.5 Clinicians should refer to NICE guidance and guidelines, Trust and Local, North
of Tyne, (NoT) guidance – when clinically appropriate – in the assessment and

CNTW(C)29
2 Cumbria Northumberland, Tyne and Wear NHS Foundation Trust CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.2-Nov 19
management of specific clinical conditions.
2.5.1 For example, in the detection and monitoring of diabetes, hypertension, obesity and hypercholesterolaemia/lipid modification
http://www.nice.org.uk/
and Local (NoT) guidance on blood glucose monitoring, hypertension and lipid modification (‘FATS7’, Feb 2015)
http://www.northoftyneapc.nhs.uk/
3 Duties and Responsibilities 3.1 Healthcare organisations have an obligation to provide physical examination
and healthcare in collaboration with primary care and other specialists within secondary healthcare.
3.2 The Medical Director and Executive Director of Nursing and Chief
Operating Officer are required to:
Ensure that all medical and nursing staff are aware of this Policy and other policies and guidance which relate to this policy
Ensure that adequate training is given to allow medical and nursing staff to safely implement the policy
Inform Senior Mental Health management if the policy is not being implemented appropriately
3.3 Medical staff are required to:
Ensure that they are aware of the contents of this policy and supporting policies
Ensure that their professional knowledge and skills are up to date (in all spheres including physical examination) in accordance with General Medical Council (GMC) requirements
Ensure and where clinically appropriate perform physical examinations, investigations and health screening as outlined in this policy
Ensure and where appropriate complete all relevant documentation in relation to physical examination, investigations and health screening
Ensure that appropriate actions are taken for service users with abnormal findings on examination or investigation
Ensure that relevant physical health issues are communicated to other healthcare professionals, as appropriate

CNTW(C)29
3 Cumbria Northumberland, Tyne and Wear NHS Foundation Trust CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.2-Nov 19
3.4 The Ward/Team manager is required to:
Ensure that all staff are aware of this policy and other policies and guidance which relates to this policy
Ensure that recommended equipment is available
Ensure that adequate training is provided to allow staff to safely implement the guidelines
Audit the use of guidelines
Inform Senior Mental Health management if the policy is not being implemented appropriately
3.5 Registered Nursing staff are required to:
Be fully aware of the contents of this policy and supporting policies and guidance
Ensure that their physical examination skills are maintained in accordance with the Nursing and Midwifery Council (NMC) requirements
Where clinically appropriate perform and support medical staff in physical examinations, investigations and health screening as outlined in this policy
Ensure and when appropriate complete all relevant documentation in relation to physical examination, investigations and health screening
3.6 Care Coordinators
Complete all relevant documentation in relation to physical examination, investigations and health screening for service users in the community
3.7 Unqualified Nurses are required to:
Be fully aware of the contents of this policy and supporting policies and guidance
Support registered nursing staff and medical staff to implement the policy
3.8 Clinical Interventions
Each clinical intervention PGN includes full procedural guidance 3.9 These guidance notes should be used in conjunction with the following policy
documents:
CNTW(O)09 – Records Management Policy, practice guidance note, - RM-PGN-02 - Record Keeping Standards

CNTW(C)29
4 Cumbria Northumberland, Tyne and Wear NHS Foundation Trust CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.2-Nov 19
4 Procedure for physical examinations– In-Patient Services 4.1 All service users will be offered a chaperone as per the policy and this must be
documented in the physical health monitoring record.
4.2 Where, after discussion with the service user, it is agreed to delay the examination or when the service user refuses the examination, the reasons for this will be recorded by the Doctor and a date set for review. The Doctor should consider the physical health of the service user and document an initial assessment.
4.3 All service users admitted to any of the Trust’s Inpatient Services (including those for older people, people with learning disability and forensic service users) must have a full physical examination, ideally within 6 hours of admission, otherwise within 24 hours of admission, unless the service user refuses, in which case the reasons must be clearly documented in the notes, with a management plan and review date.
4.4 Children admitted to the Trust or to Children and Young Peoples In-patient
Services, will be seen by the admitting clinician within six hours. The admitting clinician will assess whether urgent physical examination is required or whether it would be more clinically appropriate to await routine examination by the designated service. This routine physical examination by the designated service should be undertaken within 1 week of admission. The outcome of this assessment will be clearly recorded. (See also Section 8 – The Deteriorating Patient). All physical examinations of a child or young person to be chaperoned
4.5 Where a service user lacks capacity to consent to examination this will be recorded, as will the Doctor’s reasons for proceeding with, or not proceeding with, physical examination, in line with Trust’s policy, CNTW(C)34 - Mental Capacity Act.
4.6 In many services it is likely that the admitting Nurse will carry out the surface examination for injuries, urine dipstick analysis, height, weight BMI evaluations, NEWS2 and other baseline physiological measurements appropriate to patient.
4.7 The physical health history, examinations, investigations and plans should be documented as follows:
On Admission
o Document current and past physical health history within the core assessment and within the Diagnosis Section of the core physical health monitoring record
o Document physical examinations, investigations and
associated interventions plan within the core physical health monitoring record
o The Trust’s validated nutrition screening tool should be completed within 48 hours of admission and repeated as indicated (at least monthly).

CNTW(C)29
5 Cumbria Northumberland, Tyne and Wear NHS Foundation Trust CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.2-Nov 19
o Smoking history, with brief advice and interventions and onward referral for support with smoking cessation, if applicable, must be documented.
o Alcohol status and brief interventions, as well as onward referral for support should also be made and any other advice including those for performance measures e.g. CQUINs.
o A full drugs screen may be needed where appropriate.
o Completion of formal risk assessments e.g. Braden / VTE or in CQUIN guidance.
Body mapping is a useful and simple way of recording injuries as an aid to later diagnosis and to support potential safeguarding. It is better to record what is actually observed than to speculate on the cause of the injuries at this stage.
If the body map is to serve as a monitoring tool for minor injuries observed over a period of weeks (or even months), a new body map should be used on each occasion. See Appendix 3 or 4. It is therefore very important to be consistent in the method of recording injuries so that comparisons can be made with earlier charts.
At the following time points:-
o Annual Physical Health Check
o CPA Review
o Medication Related Health Check
4.8 Documentation of relevant and clinically appropriate physical examination, investigations and plan should be within the core physical health monitoring record
4.9 Outside of the time points listed above, if physical examination, investigations or lifestyle review is undertaken this must be documented on the core physical health monitoring record.
4.10 Outside of the time points listed above, please note, that it is appropriate to continue to record regular blood pressure, temperature, respiration and pulse rates in the NEWS2 charts and to record regular height and weight checks in the weight form now included within the core physical health folder on RiO.
4.11 Centile charts for Children and Young People should continue to be completed as per current practice
4.12 Current care plans for physical health and seclusion will need to be completed as per current practice
4.13 Any actions stemming from a physical examination such as further
investigations or referrals to physical care specialists both internal and external

CNTW(C)29
6 Cumbria Northumberland, Tyne and Wear NHS Foundation Trust CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.2-Nov 19
will be recorded. The examining health professional will clearly state who is responsible for ensuring investigations are carried out and that the appropriate referrals are made.
4.14 A short note should be made within the electronic patient record Progress Notes
and referenced when the above documentation has been completed, as per section 7.6 of the Trust’s Policy, CNTW(O)09 Records Management, practice guidance note, RM-PGN-02 - Record Keeping Standards.
4.15 All staff undertaking a physical examination must comply with the guidance
within Trust policy, CNTW(O)48 - Uniform and dress code policy, which requires that they should be “bare below the elbow” during the procedure.
4.16 Medical, Nursing and Pharmacy staff have an important role in ensuring that
medication reconciliation is completed within 24 hours of admission (see Trust policy, CNTW(C)17 – Medicine Management, practice guidance note – UHM-PGN-02 - Prescribing of Medicines). This must also include a check of any drug allergies and appropriate documentation of such see Drug Allergy PPT)
4.17 For transfer between acute trusts and CNTW, the service within CNTW must
feel comfortable managing healthcare needs for example having update to NEWS2, investigation results, clinical plan and availability of equipment and skills for that plan implementation.
5. Physical Health Review following admission 5.1 A full physical health review should be completed ideally within 1, but certainly
within 2 weeks of admission. As clinically appropriate, this should include:
family history of premature cardiovascular disease or diabetes
personal history of, or exposure to, infectious diseases, including blood borne viruses
all current medication, side effects and allergies
details of health screening (e.g. dental care, cervical screening, breast screening, bowel screening)
nutrition screening tool to be completed within 48 hours of admission and repeated as indicated (minimum of monthly)
Clinical risk assessment tools e.g. Braden/ VTE
5.2 This information should be documented (as outlined in section 4.7) and any action should be care planned, which may include, where appropriate, Health Action Plans, which have been agreed with the service user.
6 Physical interventions 6.1 Minimum physical investigations, as clinically appropriate, should be completed
ideally within 1 week, but certainly within 2 weeks of admission. 6.2 Blood tests should be carried out as clinically indicated as a baseline, usually to
include full blood count, urea and electrolytes, liver function tests, blood glucose thyroid function tests and lipids and HbA1c. (For further information see Trust’s practice guidance note sitting with this policy, PPT-PGN-08 - Physical health

CNTW(C)29
7 Cumbria Northumberland, Tyne and Wear NHS Foundation Trust CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.2-Nov 19
monitoring of patients prescribed Antipsychotics and the Lester tool). 6.3 Electrocardiograms should be carried out on all service users as per identified
in the PGN. 6.4 Other investigations should be arranged as appropriate, and on an ongoing
basis in conjunction with the National and Trust guidelines for medication related monitoring. (See product literature at www.medicines.org.uk and also the Trust’s practice guidance note sitting with this policy, PPT-PGN-08 - Physical health monitoring of patients prescribed Antipsychotics
6.5 Urine dipstick analysis/urine drug screen – as clinically indicated. 6.6 Records should be kept in accordance with Trust’s policy, CNTW(O)09 Records
Management, practice guidance note RM-PGN-02 – Record Keeping Standards.
7 Physical health care of service users who are in-patients for over one
year 7.1 All service users resident in an inpatient facility for more than 12 months should
have a documented review of their physical health every 6 months, and a full physical examination every year, (more frequently if clinically indicated). Chronic disease monitoring (e.g. diabetes, asthma, COPD, cardiovascular disease) should be reviewed, and actions taken as required. A full medication review must also be carried out and documented (as outlined in section 4.4). Weight should be monitored monthly (or more frequently if indicated within nutrition screening too or if initiated on an antipsychotic).
7.2 Service users should have access to smoking cessation and alcohol/substance
misuse advice and support, dental care, chiropody, dietician, physiotherapy, sexual health care, and an optician. Access to these services should be offered regularly and at least every six months when the physical health review is undertaken. Action taken, or a record of services being declined, should be documented.
7.3 Service users on High Dose Antipsychotic Therapy should be reviewed, and
their monitoring carried out as per Trust policy guidelines, CNTW(C)38 – Pharmacological Therapy practice guidance note - PPT-PGN-10 - Guidelines for the Use of High Dose Antipsychotics
8 The deteriorating patient 8.1 The National Early Warning Score (NEWS2) is the recommended system for
the assessment and scoring of vital signs in patients at risk of a deteriorating clinical status (see practice guidance note – AMPH-PGN-03 - National Early Warning Score (NEWS), this tool must be used to record regular monitoring of physiological measurements. It is based on data derived from four physiological readings (systolic blood pressure, heart rate, respiration rate and body temperature) and one observation of level of consciousness. The resulting observations are compared to a normal range, to generate a single score. This

CNTW(C)29
8 Cumbria Northumberland, Tyne and Wear NHS Foundation Trust CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.2-Nov 19
is used to support staff in decision making via a flow chart detailing recommended actions and observation frequencies.
8.1.1 The PEWS tool (paediatric early warning score) is used in place of NEWS2 for
children and young people. 8.2 Staff should be cognisant of:
Resuscitation Equipment and its location
Any ‘Do Not Attempt’ resuscitation order
8.3 Further guidance please see the Trust’s CNTW(C)01 - Resuscitation Policy.
9. Recommended equipment to be available for In-patient Units and
physical health care facilities in the Community
9.1 Minimum:
Stethoscope
Sphygmomanometer
Thermometer
Digital weighing scales
Urinalysis dipsticks
Height measure
Disposable gloves
Tape measure
Phlebotomy equipment (including safer sharps)
Blood glucose monitor
Ophthalmoscope
Tendon hammer
ECG machine
9.2 For inpatient units to have access to:
Auroscope
Examination couch
Tuning fork (256Hz)
Alcomete
Oximeter
Drug testing kits and oral swabs

CNTW(C)29
9 Cumbria Northumberland, Tyne and Wear NHS Foundation Trust CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.2-Nov 19
10 Physical health care of service users treated within the community
10.1 Within Learning Disability (LD) community services, people may be referred for a specific physical health need such as Epilepsy, Health promotion and education, Dysphagia, or postural care rather than mental health with associated physical health needs. Therefore LD has a layered approach, where any patient requiring a specific intervention will have that health need assessed and treatment or intervention care planned based on referral need, and the need to ensure access to mainstream health services where possible. The GP will be asked for information regarding the referral need and date of last Directed Enhanced Service (DES) annual health check and any health actions required. LD health screening tool will be used (currently call LD health monitoring tool new on RIO)
10.2 For patients with Learning Disabilities referred for their mental health or
challenging behaviour they will have the same as patients without a learning disability seen in the community (as set out in 10.1 onwards), and will use the core physical health monitoring record in the first instance and for further health conditions related to Learning Disabilities may use LD health screening tool.
10.3 Physical health care of all service users treated in the community is a shared
responsibility between our service and GP dependant on clinical need and clinical pathway. Shared care guidance can be found here
10.4 Physical healthcare of service users in the community is dependent on clinical
need and service specification e.g. addictions services. 10.5 Prior to initial assessment if the primary care summary is not available via the
Medical Interoperability Gateway (MIG) then a GP Summary should be requested from the general practice, ideally to include the following:
Physical health diagnoses
Current Medication and allergies
The most up to date documented BP, Weight, Height and any investigations; if this exists on their system
For service users in Learning Disability services the date of the last DES annual health check and any health actions required
10.6 On Initial Assessment:
Ascertain whether the service user is registered with a GP
Facilitate registration if necessary
The service user and GP (if the MIG is not available) will be asked for relevant information in relation to long term medical conditions, physical and mental health issues, and monitoring of psychotropic or other medication (see point 10.2)
Capacity of patients should be documented prior to examination and MC1 form completed if it is a best interest decision.
Baseline clinical observations and other recommended investigations should be documented, dependant on clinical

CNTW(C)29
10 Cumbria Northumberland, Tyne and Wear NHS Foundation Trust CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.2-Nov 19
judgement prior to starting medication as per Trust Guidelines e.g. PPT-PGN-08 - Physical health monitoring of patients prescribed antipsychotics - Part of CNTW(C)38 – Trust Standard for the Management and Assessment of Physical Health.
Advice and guidance re potential side effects of medication prescribed and dependant on clinical judgement utilising Trust patient information leaflets on patient medication and or other trusted websites such as www.medicines.org.uk. / www.choiceandmedication.org/ntw
an enquiry should be made into lifestyle factors, and a discussion of these documented:
o Smoking, Alcohol and other substances
o Diet and exercise
Health screen any comorbidities associated with a service user’s mental health and or learning disability.
Completion of clinical risk assessment tool e.g. Braden / VTE
10.7 A Physical Health Plan regarding such measures should be developed as
part of the assessment plan that is communicated to the GP. 10.8 If psychotropic medication recommendations are likely to be made an
enquiry into sexual health should be included. This is to ensure that patients who maybe pregnant or of child bearing age are aware of the risks of psychotropic medication in pregnancy e.g. Valproate linked to PGN.
10.9 On Follow Up/ CPA Reviews:
Ongoing monitoring of physical health and the support required to ensure attendance at appointments within primary care
Advice and guidance about requirements for physical health care monitoring in line with Trust guidance and local shared care agreements
Reporting of abnormal examination or investigation
Documentation of who the primary prescriber is
General liaison with other services as regards any other physical health care needs
Health promotion should be considered and reviewed as clinically indicated e.g. smoking cessation, alcohol/substance misuse advice and support, weight management, healthy eating, physical activity, dental care, chiropody, dietician, physiotherapy, opticians and sexual health care, blood borne infections etc
Advice and guidance re side effects and medicines management
Document health promotion discussion, physical examinations, investigations and associated interventions plan within the core physical health monitoring record

CNTW(C)29
11 Cumbria Northumberland, Tyne and Wear NHS Foundation Trust CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.2-Nov 19
10.10 A Physical Health Interventions Plan regarding such measures should be developed and recorded in the core physical health monitoring record.
10.11 If psychotropic medication recommendations are likely to be made an enquiry
into sexual health should be included. This is to ensure that patients who maybe pregnant or of child bearing age are aware of the risks of psychotropic medication in pregnancy.
10.12 Medication and or physical treatments should have the care plan documented in the relevant section (Service Specific File>Physical Treatment) and linked to the Community care co-ordination care plan.
Consult the Pharmacological Therapy Policy CNTW(C)38 and associated Practice Guidance Notes
10.13 Medication initiations should be completed as clinically indicated and according to the relevant Trust Practice Guidance Note with care plans being sent to GP. There should be an explicit agreement on when the prescribing and monitoring responsibility is transferred to General Practice, according to relevant shared care protocols. The GP should be explicitly advised on what the on-going physical health monitoring requirements will be e.g. shared care.
10.14 We should ensure that the necessary physical health monitoring is taking place.
Access to a local laboratory results system can assist this process, and liaison with the GP to send the additional parameters is equally important. Such monitoring should be updated on the relevant physical treatment form and the core physical health monitoring record. Teams should have protocols for sharing this responsibility and systems of reminders in place}.
10.15 Community teams may be required to meet the additional monitoring
requirements for High Dose Antipsychotic Therapy, where General Practices are unlikely to agree (See the Trust’s CNTW(C)38 – Pharmacological Therapy Policy, practice guidance note, PPT-PGN-10 - Guidelines for the Use of High Dose Antipsychotics).
10.16 The need for ECG at baseline and serially needs to be considered and included as part of the care plan - Guidance for ECG monitoring in psychiatric/learning disability in-patient units can be found in Appendix 2 of this document
10.17 Abnormal or high risk results must be acted upon as clinically appropriate and
as per professional standards in terms of accountability. If actions are taken on abnormal results, there should be reduced morbidity and mortality by reducing risk factors for long-term health problems such as diabetes, cardiovascular and cerebrovascular disease in line with the Lester Tool. This will involve team efforts to consider measures to modify the potential causative factors; together with GP or specialist liaisons.
10.18 Recommended equipment as per Section 9 – Recommended equipment to be
available for In-patient Units. 11 Completion of the core physical health monitoring record

CNTW(C)29
12 Cumbria Northumberland, Tyne and Wear NHS Foundation Trust CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.2-Nov 19
11.1 It is important that all documentation about a patient’s physical health is
recorded in a single location within the patient electronic record (RiO). The core physical health monitoring record was developed to enable this.
11.2 On admission/initial assessment a summary of the patient’s physical health
must be requested from the patient’s GP/previous placement on admission. This must be recorded in the Core Physical health monitoring record screen within the patient electronic record (RiO). Please record the date the summary was requested and received.
11.3 Record the time point in the patient’s pathway (from the drop down list labelled
“Review Type”) when the form is being completed e.g.
Admission
Initial Assessment
Annual Physical Health Check
Discharge
CPA Review
Medication Related Health Check
Other – detail to be completed in free text box
11.4 In section headed Clinicians Involved and Consent
Record when a health check is due but unable to be completed (with reasons) Record whether the physical health check has been completed, partially completed or consent not given, with detail in the free text box
Record relevant details of chaperone
11.5 The section headed Patient and Carer Concerns, Expectations and Wishes is a free text field to record any issues raised by the patient or carer
11.6 In section headed Diagnosed Conditions
Please choose an option for all the conditions listed with drop down boxes as appropriate
Narrative regarding diagnosis can be recorded in the “Other Physical Health Diagnosis”
11.7 In section headed Mental Health Diagnosis
Narrative regarding diagnosis can be recorded
Note:
Additionally it is important that the diagnosis and associated ICD10 code is recorded within the diagnosis section of the patient electronic record (RiO) by

CNTW(C)29
13 Cumbria Northumberland, Tyne and Wear NHS Foundation Trust CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.2-Nov 19
all responsible clinicians; Guidance on completion of this is included in Section 13 - Diagnosis/ICD 10 coding 11.8 In section headed Lifestyle Factors:
Smoking
o Choose from drop down box of whether a “Current smoker”, “ex-smoker” or “non-smoker”
o Enter the number of cigarettes smoked per day in the “Number per day” box. Enter “0” for non-smoker / ex-smokers; leave box blank if service user refuses to answer or can’t be engaged.
Alcohol
o Choose from drop down box of whether a “current user”, “ex-user” or “non-user”
o Enter the number of units consumed per week in the “Number of units per week” box. Enter “0” for non-user / ex-user; leave box blank if service user refuses to answer or can’t be engaged.
Substance Misuse
o Choose from drop down box the appropriate option to record service users situation (if patient has not had a substance misuse problem chose Never used)
NB: Specific details of substance use should continue to be recorded in the core assessment and use of AUDIT tool for alcohol use.
Exercise
o Complete the box detailing average hours per week of exercise completed by the patient
11.9 If there are any issues relating to lifestyle that need to be addressed tick the relevant issues you can tick more than one area or tick “No further action” if there are no issues. (use the Lester Tool guidance for recommended interventions)
11.10 In the “Lifestyle discussion” box detail any information arising from
discussions with the patient e.g. health factors associated with heavy smoking etc.
11.11 In addition, any Care Plans/Interventions arising from these discussions will
also need to be recorded (e.g. exercise therapy) within the Physical Health and Wellbeing Plan free text box (see 11.17).
11.12 In section headed Examination Findings:

CNTW(C)29
14 Cumbria Northumberland, Tyne and Wear NHS Foundation Trust CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.2-Nov 19
11.12.1 General Appearance
This should be completed for all patients:
o Enter Current weight in “Weight (kg)” box. Note whether the person is pregnant or given birth in the previous 6 weeks. If it is required to monitor weight over a period of time this can be added to the “Regular weight monitoring” form
o Enter current height in “Height (m)” box
o Enter current BMI in “Body Mass Index (BMI) “ box
o Enter Waist size in “Waist circumference (cm)” box
Record if patient refuses or can’t engage at the point of assessment, and record in the Physical Health and Wellbeing Plan.
Any issues relating to the above “general appearance” issues or any other factors (e.g. skin) that are off significance please enter in the free text box
Vital Signs
o Record blood pressure and pulse rate for patient in lying, sitting and standing positions, in order to assess risks from orthostatic hypotension
o If it is required to monitor BP over a period of time this should be recorded via the NEWS2 charts and alternatively this can be added to the “TPR form” within the Physical Health Monitoring folder in Core Clinical Documents
o If required record Temperature, Respiratory rate, saturation
level O2 etc (not mandatory)
For more regular vital signs monitoring, it is appropriate to continue to record blood pressure, temperature, respiration and pulse rates in the BP and TPR forms and to record regular height and weight checks in the weight form
NB: both are now included within the core physical health folder on RiO)
11.13 Please add any relevant factors within the following free text boxes where appropriate:
Head and Neck Examination/Oral Examination/Cardiovascular Examination / Respiratory System / Gastrointestinal System / Genitourinary System / Nervous System / Musculoskeletal System. This may include details of NHS screening programmes, contraception and medication side effects.
11.14 In section headed Investigations:

CNTW(C)29
15 Cumbria Northumberland, Tyne and Wear NHS Foundation Trust CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.2-Nov 19
As a minimum for all patients the Lipids and Glucose must be recorded
o For existing diabetic patients a glycated haemoglobin (HbA1c) must be recorded. This provides a longer term measure of overall glucose control over the preceding 8-12 weeks
o Random, or fasting, blood glucose and glycated haemoglobin (HbA1c) are investigations used in the detection and management of hypoglycaemia, hyperglycaemia and diabetes. The measurements are not interchangeable, have different units of measurement and are monitored in different situations
o (Gestational Diabetes risk is not to be measured using fasting plasma glucose, random blood glucose, HbA1c, glucose challenge test or urinalysis – NICE guidelines NG3)
Other areas should be completed where required. Other documents can be added electronically if required (e.g. Body maps)
Please record the date investigation is requested and the date results are received
Please record any comments arising from the results in the comments field. For example, if a patient has abnormal results
There is the facility to add additional test types in the box below the listed tests
11.15 In section headed Assessment Scales:
Record 10 year Cardiovascular (CV) risk score if appropriate
Record Venous Thromboembolism (VTE) assessment has been completed as per PGN and repeated as clinically indicated
Braden complete as per admission and as clinically indicated. 11.16 In section headed Vaccinations
Record flu and pneumococcal vaccinations, as clinically appropriate.
(the top left of core physical health monitoring record screen gives details of the at risk categories)
Record whether there is a need for a heatwave or winter care plan
11.17 Physical Health and Wellbeing Plan
Record any Intervention Plans relating to the factors highlighted in the previous sections, using the Lester Tool recommendations as a guide in the Physical Health and Wellbeing Plan.

CNTW(C)29
16 Cumbria Northumberland, Tyne and Wear NHS Foundation Trust CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.2-Nov 19
If a Physical Health Interventions Plan is not required this should be indicated using the check box “no intervention required”
12 Medication Recording
12.1 To be completed as per Trust policy, CNTW(O)09 – Records Management, practice guidance note - RM-PGN-02 Record Keeping Standards.
The Medicines, Allergies and Sensitivities form should be completed and updated at least at the following key points:
Admission/Initial assessment
CPA review
Initiation of medication (as per PGN or locally agreed protocol for example relevant CQUIN guidance)
Changes in medication prescription (as per PGN or locally agreed protocol for example relevant CQUIN guidance)
Discharge
12.2 The ‘medicines related physical health monitoring’ box should be completed as clinically appropriate.
13 Diagnosis/ICD 10 coding 13.1 If the assessment process involves a Consultant Psychiatrist and it is possible
to agree a mental health diagnosis/confirm any mental health diagnosis provided by the GP the Consultant Psychiatrist (or other qualified member of team e.g. coding team member) should enter this as the service user’s primary diagnosis with associated ICD 10 code on the diagnosis screen of the electronic patient record (RiO) and then add any secondary diagnoses including physical health conditions.
13.2 If the diagnosis is unclear, then the Consultant Psychiatrist should enter a
suitable code to indicate this. We are required when we communicate to the GP to share ICD 10 codes.
13.3 At each CPA review, once the review has been entered and outcomed on the
CPA/Standard care management screen
If the service user does not have an existing diagnosis with associated ICD 10 code entered on the diagnosis screen of electronic patient record (RiO) a mental health diagnosis should be entered by the Consultant Psychiatrist as the service user’s primary diagnosis with associated ICD 10 code on the diagnosis screen of electronic patient record (RiO)
Once there is a primary diagnosis, the Consultant Psychiatrist should add any secondary diagnoses including physical health conditions

CNTW(C)29
17 Cumbria Northumberland, Tyne and Wear NHS Foundation Trust CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.2-Nov 19
If the service user has existing diagnosis(es) with associated ICD 10 code entered on the diagnosis screen of electronic patient record (RiO) the Consultant Psychiatrist will either need to confirm the service user’s primary diagnosis with associated ICD 10 code or enter and confirm any new diagnosis(es) with associated ICD 10 code and confirm/any add any secondary diagnoses including physical health conditions
If the diagnosis is unclear, then use code Z004 – Psychiatric Examination to indicate this. We are required when we communicate to the GP to share ICD 10 codes
14 Procedure and Minimum Standards – Children and Adolescent Services 14.1 Children admitted to the Trust or to Children and Young People Specialist
Service (CYPSS) will be seen by the admitting clinician within six hours. The admitting clinician will assess whether urgent physical examination is required or whether it would be more clinically appropriate to await routine examination by the contracted GP service at the next available opportunity. The outcome of this assessment will be clearly recorded.
14.2 On those rare occasions where young people are admitted to adult mental
health facilities they will be offered a physical examination as per the Trust standards.
15 Training 15.1 The Trust’s expectation is that healthcare staff will keep their physical health
examination skills up to date in accordance with their respective codes of conduct.
15.2 The aims of the training would be:
Understanding the links between serious mental illness and physical health
Providing support and advice to clients in the following areas: healthy eating, weight management, exercise, smoking, alcohol and illicit drug use, and general health and wellbeing
Identifying and managing side effects of medication, including use of validated rating scales e.g. LUNSER’S, GASS, High Dose Antipsychotic Therapy monitoring.
Being aware of the role of primary care services in physical health monitoring
To be competent in clinical skills
15.3 All staff would be expected to utilise health promotion opportunities, such as smoking cessation and signposting to healthy lifestyle resources when working with service users. Staff who have had additional training would be expected to champion and promote those skills in their clinical areas and teams.

CNTW(C)29
18 Cumbria Northumberland, Tyne and Wear NHS Foundation Trust CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.2-Nov 19
15.4 Levels of training are identified in the training needs analysis and are included within the Training Guide which can be accessed via this link:
http://nww1.ntw.nhs.uk/services/index.php?id=3796&p=2780
16 Identification of Stakeholders 16.1 This is an existing policy which has been reviewed, with additional/changed
content that relates to operational and/or clinical practice and was therefore circulated to those listed below for a four week consultation period:
North Locality Care Group
Central Locality Care Group
South Locality Care Group
Cumbria Locality care Group
Corporate Decision Team
Business Delivery Group
Safer Care Group
Communications, Finance, IM&T
Commissioning and Quality Assurance
Workforce and Organisational Development
NTW Solutions
Local Negotiating Committee
Medical Directorate
Staff Side
Internal Audit
17 Equality and Diversity 17.1 In conjunction with the Trust’s Equality and Diversity Officer this policy has
undergone an Equality and Diversity Impact Assessment which has taken into account all human rights in relation to disability, ethnicity, age and gender. The Trust undertakes to improve the working experience of staff and to ensure everyone is treated in a fair and consistent manner.
18 Implementation 18.1 Implementation of this policy will be immediate. It will be monitored by the
Physical Health Group which is a sub group of Trust’s Quality and Performance Group and if at any stage there is an indication that the target date cannot be met for the initial and any subsequent versions then the Physical Health and Wellbeing Group will consider the implementation of an action plan.
19 Abbreviations
CC Care Coordinator
CYPS Children and Young People Services
GMC General Medical Council
GP General Practitioner

CNTW(C)29
19 Cumbria Northumberland, Tyne and Wear NHS Foundation Trust CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.2-Nov 19
IPC Infection, Prevention and Control
NMC Nursing, Midwifery Council
PGN Practice Guidance Note
CQUIN Commissioning for Quality and Innovation
NEWS2 National Early Warning Score
MIG Medical Interoperability Gateway
DES Directed Enhanced Service 20 Monitoring Compliance 20.1 This policy will be audited through a programme of clinical audit of health
records, carried out at least annually within every care group and is applicable to the electronic and integrated records used by all disciplines and be organised through the Physical Health and Wellbeing Group and demonstrate robust implementation of the audit cycle. The audit standards will be as a minimum as set out in Appendix C, Monitoring Tool.
20.3 Audit results will be provided to Associate Directors who will be responsible for
producing an action plan which must be implemented. Audit outcomes and associated action plans will be received Care Group Quality and Performance group to who will monitor the implementation of the action plans and for assurance by the Physical Health and Wellbeing Group.
20.5 It is important that the policy develops to continually improve the standards expected by service users and carers, changes in organisational policy, legislation and recognised good practice. It will be the responsibility of the Trust and associated partners, to ensure that this happens. This policy will be reviewed three years after date of issue. The review will incorporate service users supported in community settings and user group specific operational procedures, including recording documentation.
21 Fraud, Bribery and Corruption 21.1 In accordance with the Trust’s CNTW(O)23 - Fraud, Bribery and Corruption
Policy, all suspected cases of fraud and corruption should be reported immediately to the Trust’s Local Counter Fraud Specialist or to the Executive Director of Finance.
22 Fair Blame 22.1 The Trust is committed to developing an open learning culture. It has endorsed
the view that, wherever possible, disciplinary action will not be taken against members of staff who report near misses and adverse incidents, although there may be clearly defined occasions where disciplinary action will be taken.
23 Associated Documentation
CNTW(C)01 - Resuscitation Policy
CNTW(C)02 - Rapid Tranquilisation Policy

CNTW(C)29
20 Cumbria Northumberland, Tyne and Wear NHS Foundation Trust CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.2-Nov 19
CNTW(C)05 - Consent to Examination and Treatment Policy
CNTW(C)10 – Seclusion Policy
CNTW(C)18 - Tissue Viability Policy
CNTW(C)16 – Positive and Safe, Management of Violence and Aggression Policy
CNTW(C)17 - Medicine Management (including non-med prescribing) Policy
o UHM-PGN-02 - Prescribing of Medicines
CNTW(C)19 - Observational Policy
CNTW(C)20 - Care Coordination/CPA Policy
CNTW(C)23 - Infection, Prevention and Control Policy and PGNs
CNTW(C)26 - Dysphagia Policy
CNTW(C)29 - Trust standard for the assessment and management of physical health policy
o AMPH-PGN-03 - National Early Warning Score (NEWS)
o PPT-PGN-08 - Physical health monitoring required for patients on antipsychotics
CNTW(C)34 - Mental Capacity Act Policy
o MCA-PGN-02 – Advance decision to refuse treatment and advance statements
CNTW(C)35 - Phlebotomy Policy
CNTW(C)38 - Pharmacological Therapy Policy – Practice Guidance Note(s)
o PPT-PGN-05 – Safe Prescribing of Clozapine
o PPT-PGN-10 - Guidelines for the Use of High Dose Antipsychotics
o PPT-PGN-19 – Safer Lithium Therapy
CNTW(C)40 - Dignity in Care Policy
CNTW(C)48 – CC/CPA Children and Young People Policy
CNTW(C)49 - Care of the Dying Policy

CNTW(C)29
21 Cumbria Northumberland, Tyne and Wear NHS Foundation Trust CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.2-Nov 19
CNTW(C)51 - Electroconvulsive Therapy Policy
CNTW(O)01 - Development/Management of Procedural Documents Policy
CNTW(O)09 - Records Management Policy; Practice Guidance Note
o RM-PGN-02 – Record Keeping Standards
CNTW(O)23 – Fraud, Bribery and Corruption Policy
CNTW(O)27 - Nutrition Policy
CNTW(O)48 - Uniform and dress code policy
CNTW(C)21 - Medical Devices Policy
CET-PGN-01 - Chaperone Guidance
Lester Tool
24 References
Disability Rights Commission-Equal Treatment ‘Closing the Gap, 2006

CNTW(C)29
22 Cumbria Northumberland, Tyne and Wear NHS Foundation Trust CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.2-Nov 19
Appendix A
Equality Analysis Screening Toolkit
Names of Individuals involved in Review
Date of Initial Screening
Review Date Service Area / Locality
Chris Rowlands April 19 April 22 Trust wide
Policy to be analysed Is this policy new or existing?
CNTW(C)29 Trust standard for the assessment and management of physical health – V06
Existing
What are the intended outcomes of this work? Include outline of objectives and function aims
People with a Learning Disability or Mental Health problems are more likely than other citizens to have significant health risks and develop major physical health problems. Once they have developed a physical illness both groups are likely to die younger. (Disability Rights Commission-Equal Treatment: Closing the Gap, 2006). Improving Health and Lives (Department of Health), Health Inequalities and People with LD in the UK 2010 It is Cumbria Northumberland, Tyne and Wear NHS Foundation Trust’s (the Trust/CNTW) intent that all service users will receive a core assessment and review of their physical health needs, and all service users admitted to hospital will receive a full physical examination. This policy describes the minimum standard of physical assessment that a service user can expect and may be supplemented by additional guidance in relation to relevant CQUIN requirements as they occur.
Who will be affected? e.g. staff, service users, carers, wider public etc
Service Users
Protected Characteristics under the Equality Act 2010. The following characteristics have protection under the Act and therefore require further analysis of the potential impact that the policy may have upon them
Disability Addresses health positively in a holistic manner, in keeping with the findings of the DRC report and NHS England
Sex NA
Race NA
Age NA
Gender reassignment
(including transgender)
NA
Sexual orientation. NA
Religion or belief NA
Marriage and Civil Partnership
NA
Pregnancy and maternity
NA
Carers NA

CNTW(C)29
23 Cumbria Northumberland, Tyne and Wear NHS Foundation Trust CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.2-Nov 19
Other identified groups NA
How have you engaged stakeholders in gathering evidence or testing the evidence available?
Through standard policy process
How have you engaged stakeholders in testing the policy or programme proposals?
Through review of the policy process
For each engagement activity, please state who was involved, how and when they were engaged, and the key outputs:
Policy consultation group
Summary of Analysis Considering the evidence and engagement activity you listed above, please summarise the impact of your work. Consider whether the evidence shows potential for differential impact, if so state whether adverse or positive and for which groups. How you will mitigate any negative impacts. How you will include certain protected groups in services or expand their participation in public life.
No negative impact Some evidence to suggest that the policy will help reduce health inequalities for Disabled People.
Now consider and detail below how the proposals impact on elimination of discrimination, harassment and victimisation, advance the equality of opportunity and promote good relations between groups. Where there is evidence, address each protected characteristic
Eliminate discrimination, harassment and victimisation
Provision improves access to physical healthcare for disabled people
Advance equality of opportunity Provides better access to basic healthcare requirements
Promote good relations between groups Bridging the gap between physical and mental health will have a positive effect
What is the overall impact?
Positive
Addressing the impact on equalities Adherence to the policy and others associated with it.
From the outcome of this Screening, have negative impacts been identified for any protected characteristics as defined by the Equality Act 2010?
If yes, has a Full Impact Assessment been recommended? If not, why not? No – Policy clearly positive and in line with requirements.
Manager’s signature: Chris Rowlands Date: April 2019

CNTW(C)29
24 Cumbria Northumberland, Tyne and Wear NHS Foundation Trust CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.2-Nov 19
Appendix B
Communication and Training Check list for policies
Key Questions for the accountable committees designing, reviewing or agreeing a new Trust policy
Is this a new policy with new training requirements or a change to an existing policy?
Changes to existing policy
If it is a change to an existing policy are there changes to the existing model of training delivery? If yes specify below.
NO
Are the awareness/training needs required to deliver the changes by law, national or local standards or best practice?
Please give specific evidence that identifies the training need, e.g. National Guidance, CQC, NHS Resolutions etc.
Please identify the risks if training does not occur.
Please specify which staff groups need to undertake this awareness/training. Please be specific. It may well be the case that certain groups will require different levels e.g. staff group A requires awareness and staff group B requires training.
Medical, nursing, nursing assistants, pharmacists and pharmacy technicians, care co-ordinators.
Is there a staff group that should be prioritised for this training / awareness?
All clinical staff should be aware of this policy and have an understanding of their individual responsibilities
Please outline how the training will be delivered. Include who will deliver it and by what method. The following may be useful to consider: Team brief/e bulletin of summary Management cascade Newsletter/leaflets/payslip attachment Focus groups for those concerned Local Induction Training Awareness sessions for those affected by the new policy Local demonstrations of techniques/equipment with reference documentation Staff Handbook Summary for easy reference Taught Session E Learning
The policy should be circulated via normal methods of distribution and appropriate professional forums
Please identify a link person who will liaise with the training department to arrange details for the Trust Training Prospectus, Administration needs etc.
Dr Jonathan Richardson

CNTW(C)29
25 Cumbria Northumberland, Tyne and Wear NHS Foundation Trust CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.2-Nov 19
Appendix B – continued
Training Needs Analysis
Staff / Professional Group Type of Training Duration of Training
Frequency of Training
Should any advice be required, please contact: - 0191 245 6777 (internal 56777- Option 1)

CNTW(C)29
26 Cumbria Northumberland, Tyne and Wear NHS Foundation Trust CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.2-Nov 19
Appendix C
Monitoring Tool Statement
The Trust is working towards effective clinical governance and governance systems. To demonstrate effective care delivery and compliance, policy authors are required to include how monitoring of this policy is linked to auditable standards/key performance indicators will be undertaken using this framework.
CNTW(C)29 - Trust Standard for Physical Assessment and Examination Policy - Monitoring Framework
Auditable Standard/Key Performance Indicators
Frequency/Method/Person Responsible
Where results and any associate Action Plan will be reported to implemented and monitored; (this will usually be via the relevant Governance Group).
1 To demonstrate effective care delivery and compliance, policy authors are required to include how monitoring of this policy will be undertaken using this framework. Authors should consider auditable standards within the policy and whether there are existing performance indicators that can be used to support the monitoring process e.g. where adherence to requirements are set out and measured through the metrics in contracts, quality standards or CQUIN.
Review of a selection of clinical records via the Quality team targets; physical health report.
Annually
Associate Directors
Group Quality and Performance Committees
Physical Health and Wellbeing Group
The Author(s) of each policy is required to complete this monitoring template and ensure that these results are taken to the appropriate Quality and Performance Governance Group in line with the frequency set out

CNTW(C)29
Cumbria Northumberland, Tyne and Wear NHS Foundation Trust Appendix 1- Guidance on Use of Core Physical Health Monitoring Record CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.1-May 19
Appendix 1
Guidance for the Use of the Core Physical Health Monitoring Record These guidance notes should be used in conjunction with the following policies:
CNTW(O)09 – Records Management Policy practice guidance note, MR-PGN-02 - Record Keeping Standards
CNTW(C)29 – Trust Standard for the Assessment and Management of Physical Health
Completion of the Core Physical Health Monitoring Record
To link the record to the appropriate community referral or inpatient admission
To record whether the summary care record has been obtained from the patient’s GP/previous placement on admission
To record the time point in the patient’s pathway when the form is being completed i.e.
o Admission
o Initial Assessment
o Annual Physical Health Check
o Discharge
o CPA Review
o Medication Related Health Check
Outside of the time points listed above, please note, that it is appropriate to continue to record regular blood pressure, temperature, respiration and pulse rates in the BP and TPR forms and to record regular height and weight checks in the weight form now included within the core physical health folder on RiO. Centile charts for Children and Young People should continue to be completed as per current practice
The core assessment should be used to record appropriate physical health information and also details of alcohol and drug use - this information should continue to be completed along with the core physical health monitoring record
Clinicians Involved and Consent
To record relevant details of chaperone
To record when a health check is due but unable to be completed (with reasons)
Patient and Carer Concerns, Expectations and Wishes
A free text field to record any issues raised by the patient or carer

CNTW(C)29
Cumbria Northumberland, Tyne and Wear NHS Foundation Trust Appendix 1- Guidance on Use of Core Physical Health Monitoring Record CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.1-May 19
Diagnosed Conditions
To record whether the patient has any diagnosed physical health conditions e.g. diabetes or epilepsy and also include mental health diagnosis information
Lifestyle Factors
To record smoking, alcohol, substance misuse, exercise and diet plus any relevant information arising from discussions with the patient in the free text box at the bottom of this section. In addition, any Care Plans/Interventions arising from these discussions will also need to be recorded within the Physical Health Plan free text box (see below)
NB: specific details of alcohol and substance use should continue to be recorded in the core assessment Examination Findings
To record weight, height and BMI plus discussions regarding the patient’s BMI or weight, if applicable
To record waist circumference, if appropriate/relevant
To record any issues arising in relation to skin
Vital Signs
To record blood pressure and pulse rate
To record other vital signs such as temperature, if appropriate or required
For more regular vital signs monitoring, it is appropriate to continue to record blood pressure, temperature, respiration and pulse rates in the BP & TPR forms and to record regular height and weight checks in the weight form (NB: both are now included within the core physical health folder on RiO)
Head and Neck Examination / Oral Examination / Cardiovascular Examination / Respiratory System / Gastrointestinal System / Genitourinary System / Nervous System / Musculoskeletal System
To record any relevant information associated with the above factors
Investigations
To record date investigation is requested and the date results are received
To record any comments arising from the results. For example, if a patient has abnormal results, this should be noted in the comments field
There is a link to uploaded documents
There is the facility to add additional test types in the box below the listed tests
Associated Documents link could be used to upload documents in relation to Physical Health eg. body maps

CNTW(C)29
Cumbria Northumberland, Tyne and Wear NHS Foundation Trust Appendix 1- Guidance on Use of Core Physical Health Monitoring Record CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – V06.1-May 19
Assessment Scales
To record 10 year Cardiovascular (CV) risk score, if clinically appropriate, within your team
To record venous Thromboembolism (VTE) assessment, as clinically appropriate
Vaccinations
To record flu and pneumococcal vaccinations, as clinically appropriate Physical Health Plan
Record any Physical Health Plans, as appropriate. You need to indicate the factors covered within the plan using the check boxes provided. For example, if smoking cessation is documented within the free text box as part of the Physical Health Plan, please indicate by ticking the smoking check box
Medication
Medication side effects monitoring forms should be recorded in the medication documentation (e.g. Lunsers, GASS)
Medication should continue to be recorded using existing medication forms, as per PGN-MR-02 Record Keeping Standards

CNTW(C) 29
Appendix 2
Cumbria Northumberland, Tyne and Wear NHS Foundation Trust Appendix 2- Guidance for ECG Monitoring CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – Nov 19
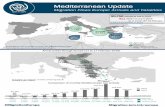
Guidance for ECG monitoring in psychiatric/learning disability in-patient units
Patients with severe mental illness may be at increased risk of cardiovascular disease. This document is intended to provide guidance for considering which patients should be offered ECG monitoring. It is not intended to replace sound clinical judgement
Any ECG’s performed should be reviewed by a medic at the earliest opportunity, within a 24 hour period and sent for cardiology opinion if required
ECG may not be required if: ECG at admission if: Serial ECG monitoring if:
Young patient (under 35 yrs)
No history of CVD or arrhythmias
No established CV risk factors
No significant family history of CVD
Not receiving treatment with a potentially cardio-toxic drug
No significant medical co-morbidity
Patients aged over 35 years
History of CVD or arrhythmias
Presence of CVD risk factors
Significant family history of CVD
Receiving treatment with a potentially cardio-toxic drug
May need parenteral medication (e.g. for rapid tranquillisation) Significant medical co-morbidity
Abnormalities on baseline ECG
Prolonged QTc interval
New onset symptoms suggestive of arrhythmia or other CVD
Commencing treatment with a potentially cardio-toxic drug
Electrolyte abnormalities
Drugs which may prolong the QT interval and predispose to arrhythmias
Psychotropic drugs Antiarrhythmic drugs Immunosuppressant drugs Chlorpromazine Type 1A (e.g. Quinidine) Tacrolimus Droperidol Type 1C (e.g Flecainide) Haloperidol Type 3 (e.g. Amiodarone) Antidiuretic hormone Pimozide Vasopressin Sertindole Anti-histamines Ziprasidone Hydroxyzine Others Loratadine Adenosine Amitryptiline Mizolastine Papaverine Clomipramine Cocaine Desipramine Antimicrobial drugs Methadone Nortryptiline Clarithromycin Citalopram Clindamycin Lithium Erythromycin Chloral hydrate Ketokonazole Pentamidine Quinine NB: This list is not exhaustive
Factors which may predispose to arrhythmias
Electrolyte abnormalities Cardiac disease Hypokalaemia Congenital LQTC Hypomagnesaemia IHD Hypocalcaemia DCM HOCM Drugs LV dysfunction See table opposite Myocarditis Hypertension CNS disorders Bradycardia Intracranial haemorrhage SA or AV block Stroke ECG parameters Systemic diseases Prolonged QT Liver disease Abnormal T wave Renal disease Abnormal U wave Hypothyroidism BBB Vent. Ectopics

Cumbria Northumberland, Tyne and Wear NHS Foundation Trust Appendix 2- Guidance for ECG Monitoring CNTW(C)29 - Trust Standard for Assessment and Management of Physical Health – Nov 19
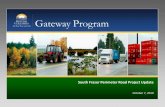
Appendix 3-Body Mapping (Adults)
Name: RiO number:
Date: Time completed?
Web based incident number (where applicable)
Reason for mapping? (circle as appropriate)
Fall / admission / transfer / self-harm / accident / assault / PMVA / pre-discharge
Other? (Please specify)
Name / designation of person completing body map form:
Number each anatomical site, on page two complete description and ensure full clinical
description is placed on RiO

Site Brief description of site and issue (full description on RiO)
1
2
3
4
5
Body mapping is a useful and simple way of recording injuries as an aid to later diagnosis and to support potential safeguarding. It is better to record what is actually observed than to speculate on the cause of the injuries at this stage.
If the body map is to serve as a monitoring tool for minor injuries observed over a period of weeks (or even months), a new body map should be used on each occasion. It is therefore very important to be consistent in the method of recording injuries so that comparisons can be made with earlier charts. Where several different staff may be completing the monitoring forms, managers should ensure they understand what is required of them.
The following points should be covered:
The individual’s dignity and respect should be maintained during any examination.
Please ensure that you seek consent from the adult prior to carrying out any examination. If the person lacks capacity to consent to an examination, please follow the principles of the Mental Capacity Act 2005 and ensure that the decision is made in the person’s best interests and is the less restrictive option.
If consent can be obtained then visual referencing using photographs will help future review of improvement or deterioration. Staff should use the consent form located in the CNTW(O)45 Visual Imaging and Audio Recording Policy
Accurately date and reference any chart used to ensure it relates to the correct client (date, time, Rio or NHS number) body maps and wound assessment guide is located in (TV-PGN-04 - Wound Assessment - Appendix 1)
Describe any marks, swelling, lacerations or other injuries carefully (cuts, bruises scratches) using the wound assessment TIME acronym will aid this – tissue, infection/inflammation, moisture and edge.
Describe the colour (brown/yellow/blue), size and shape of any bruises and indicate their location on the body chart; also describe any pattern if there are several bruises close together. When measuring use a tape measure – there is one in every wound care dressing pack.
Where indicated completion of a web based incident form and or safeguarding report should be completed
in-line with Trust policy.
Briefly list any relevant circumstances witnessed, such as anger or aggression by the individual at risk or by anyone in contact with the person at risk.
Also record any explanations of injuries given immediately by the vulnerable adult/child and any other witnesses.
Ensure that for each chart completed the date and time of examination are clearly entered along with the
name of the person completing the chart.
* Scan and upload completed form to Rio *

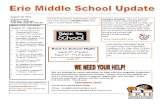
Appendix 4-Body Mapping (Child)
Name: RiO number:
Date: Time completed?
Web based incident number (where applicable)
Reason for mapping? (circle as appropriate)
Fall / admission / transfer / self-harm / accident / assault / PMVA / pre-discharge
Other? (Please specify)
Name / designation of person completing body map form:
Number each anatomical site, on page two complete description and ensure full clinical
description is placed on RiO

Site Brief description of site and issue (full description on RiO)
1
2
3
4
5
Body mapping is a useful and simple way of recording injuries as an aid to later diagnosis and to support potential safeguarding. It is better to record what is actually observed than to speculate on the cause of the injuries at this stage.
If the body map is to serve as a monitoring tool for minor injuries observed over a period of weeks (or even months), a new body map should be used on each occasion. It is therefore very important to be consistent in the method of recording injuries so that comparisons can be made with earlier charts. Where several different staff may be completing the monitoring forms, managers should ensure they understand what is required of them.
The following points should be covered:
The individual’s dignity and respect should be maintained during any examination.
Please ensure that you seek consent from the adult prior to carrying out any examination. If the person lacks capacity to consent to an examination, please follow the principles of the Mental Capacity Act 2005 and ensure that the decision is made in the person’s best interests and is the less restrictive option.
If consent can be obtained then visual referencing using photographs will help future review of improvement or deterioration. Staff should use the consent form located in the CNTW(O)45 Visual Imaging and Audio Recording Policy
Accurately date and reference any chart used to ensure it relates to the correct client (date, time, Rio or NHS number) body maps and wound assessment guide is located in (TV-PGN-04 - Wound Assessment - Appendix 1)
Describe any marks, swelling, lacerations or other injuries carefully (cuts, bruises scratches) using the wound assessment TIME acronym will aid this – tissue, infection/inflammation, moisture and edge.
Describe the colour (brown/yellow/blue), size and shape of any bruises and indicate their location on the body chart; also describe any pattern if there are several bruises close together. When measuring use a tape measure – there is one in every wound care dressing pack.
Where indicated completion of a web based incident form and or safeguarding report should be
completed in-line with Trust policy.
Briefly list any relevant circumstances witnessed, such as anger or aggression by the individual at risk or by anyone in contact with the person at risk.
Also record any explanations of injuries given immediately by the vulnerable adult/child and any other witnesses.
Ensure that for each chart completed the date and time of examination are clearly entered along with the
name of the person completing the chart.
* Scan and upload completed form to Rio *