Venous Thromboembolism Prevention - King's Thrombosis...
48
Venous Thromboembolism Prevention A Guide for Delivering the CQUIN Goal
Transcript of Venous Thromboembolism Prevention - King's Thrombosis...

Venous Thromboembolism PreventionA Guide for Delivering the CQUIN Goal

Editors:Dr Roopen Arya BMBCh MA PhD FRCP FRCPath
Director, King’s Thrombosis CentreLead for the National VTE Exemplar Centre Initiative
London Director of Thrombosis
Professor Beverley Hunt FRCP FRCPath MDProfessor of Thrombosis & Haemostasis, King’s College, London
Consultant, Guy’s & St Thomas’ NHS Foundation Trust Medical Director, Lifeblood: The Thrombosis Charity (Health charity of the year 2010)
Published by:
Project Editor: Aidan McManus PhD (MMRx Consulting)Designer: Raz O’Connor (www.auralmassage.com)

Foreword . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Professor Sir Bruce Keogh
Preface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Dr Roopen Arya
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Professor Beverley Hunt
VTE prevention in the quality framework . . . . . . . . . . . . 8
- Introduction- The CQUIN framework, VTE goal and quality indicator for VTE prevention
- NICE clinical guideline 92
- The ‘NHS Standard Contract for Acute Services’ and VTE prevention
- NICE Quality Standard
- CQUIN and VTE prevention beyond 2011
Essential first steps to achieve the CQUIN goal . . . . . . . 12
- Understand the denominator for the VTE CQUIN goal
- What constitutes a day case?
- Numerator of the CQUIN goal
- Pregnancy and VTE prevention
- Engage with your PCT/Commissioners
- An SHA-wide programme of work
- Institutional support and prioritisation of VTE prevention
- Identify a lead physician, form a multidisciplinary team and develop an action plan
- Identify what success will look like
Introduce protocols that standardise VTE risk assessment and prophylaxis provision . . . . . . . . . . . . . . 16
- Local modifications of the risk assessment tool- Paper-based risk assessment tools
- Electronic risk assessment
- A national electronic risk assessment tool
Embedding VTE prevention protocols into patient care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
- Develop a Trust-wide VTE prevention policy- VTE protocols are the base for layered interventions
- Designing reliability into the VTE protocol
- Drug chart integration of VTE risk assessment and prophylaxis provision
- Quality improvement schemes - clinical support staff
- System prompts and ‘hard stops’ for VTE prevention
- Commissioning for VTE prevention
Ensuring reliable data collection and performance tracking . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
- Collecting the numerator of the CQUIN goal
- VTE prophylaxis audit
- VTE prophylaxis performance dashboards
- Balancing measures
- Root cause analysis of hospital-acquired VTE
- Clinical coding and VTE
- National benchmarking: estimates of hospital-acquired VTE
Ensuring educational programmes are created to support the protocols . . . . . . . . . . . . . . . . . . . . . . . . . 26
- Ongoing professional training and education
- Grand rounds
- Leadership walk-rounds
- Educational evenings and competitions
- Engaging the patient
Prevention of VTE: delivering this key patient safety priority . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
Dr. William H. Geerts
Resource Centre
Development timeline of the National VenousThromboembolism Prevention Programme in England . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
National venous thromboembolism risk assessment tool . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
Modified national venous thromboembolism riskassessment tool . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
WHO surgical safety checklist . . . . . . . . . . . . . . . . . . . 36
VTE prevention at King’s College Hospital . . . . . . . . . . 38
The VTE Exemplar Centre Network . . . . . . . . . . . . . . . 40
London’s Quality Observatory portal . . . . . . . . . . . . . . 41
Map of Medicine and venous thromboembolism pathways . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42
e-Learning venous thromboembolism . . . . . . . . . . . . . 43
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
1
Veno
us Throm
boem
bolism Preve
ntion A
Guide
for D
elivering the CQUIN
Goa
l
Contents

2
The National Venous
Thromboembolism Prevention
Programme in England
Venous thromboembolism (VTE) is
a terrible condition which strikes
rapidly and often silently to cause
death or long term problems such
as swollen limbs, varicose veins or
festering limb ulcers. While there
exists a range of estimates as to the
burden of VTE, everyone agrees that
it causes many thousands of deaths
in hospitals in England each year.
Many of these are avoidable, all
cause untold heartache.
Last year at the National Conference
on VTE Prevention, I was asked by
two Royal Medical College
presidents why, given that the
problem had been known about
for three decades, the Government
would not mandate treatment to
prevent VTE in our hospitals. I was
struck by the sad irony that leaders
of the medical profession were
asking the Government to enforce
good clinical practice. It seemed to
me that the key to resolving this
problem was to change professional
and organisational attitudes. The
first requires aggressive leadership
from clinical Royal Colleges and the
latter requires system wide carrots
and sticks that acknowledge the
devolved nature of the modern NHS
and reinforces the importance of
decisions being locally-owned and
clinically driven.
So the SHA Medical Directors and I
forged common cause between the
Academy of Medical Royal Colleges,
the Royal College of Nursing and
the NHS leadership to make tackling
VTE a top clinical priority for 2010.
The deal was the DH would put
levers in the system; the Royal
Colleges would provide professional
clinical leadership.
So, through the NHS leadership
team, we have introduced a range
of measures to prevent VTE in
hospitals. These measures build on
the former Chief Medical Officer’s
work to raise awareness of this issue
in the NHS since 2005.
We are now in an aggressive
implementation phase, which
started with the inclusion of VTE
prevention in the NHS Operating
Framework for 2010-11, which
states explicitly that professional
leadership in the area of VTE
prevention will be provided by the
Academy of Medical Royal Colleges.
This represents a unique partnership
between the Royal Colleges and
NHS management in improving
patient safety. The implementation
phase for VTE prevention aims to
ensure that all adult patients
admitted to hospital are risk-
assessed for VTE and, where
appropriate, receive the right
prevention (thromboprophylaxis).
To support this, the National
Institute for Health and Clinical
Excellence (NICE) published the new
clinical guideline 92, ‘Venous
ForewordProfessor Sir Bruce Keogh
I warmly welcome this guide that has been created in partnership between King’s Thrombosis
Centre, VTE Exemplar Centres and Lifeblood. It is both timely, as we introduce a number of
system changes designed to encourage and enable the NHS to save more lives from this terrible
condition, and critical, in order to highlight the urgency of our collective healthcare response.

thromboembolism - reducing the
risk’, in January 2010 and will be
publishing a follow-up Quality
Standard which will define good
practice in this arena in June / July
2010. A national tool for risk
assessment based on the NICE
guidelines has been developed.
A financial incentive for
organisations to focus on VTE
prevention has been introduced
through the Commissioning for
Quality and Innovation Payment
Framework (CQUIN) for 2010-11.
A proportion of CQUIN payments
to acute providers will be
conditional on risk assessing at
least 90% of patients admitted to
hospital. From 1 June 2010,
providers have been required to
report the proportion of admitted
patients who have been risk
assessed. As well as ensuring
uptake of risk assessment
procedures, this will also support
VTE prevention by providing a
national picture so that further
work can be targeted appropriately.
The commissioning arrangements
for VTE prevention have been
strengthened in the national
contracting process for 2010/11.
Acute service providers will be
required to report to their lead
commissioner through monthly
audits of the percentage of patients
receiving appropriate prophylaxis
after risk assessment using the
national tool. A root cause analysis
of all confirmed cases of hospital-
acquired VTE will also be required
from every acute provider. This
approach has proven to be of
particular importance in reducing
rates of MRSA.
The Academy of Medical Royal
Colleges and Royal College of
Nursing are supporting this work by
producing speciality-specific
guidance where needed, ensuring
that their Fellows and Members are
aware of the importance of VTE
prevention and encouraging
participation in audit of VTE
prevention practice.
I have appointed Dr Anita Thomas
OBE as National Clinical Lead on
VTE, and she will report to me on
progress of this implementation
strategy.
To be successful this attack on VTE
needs to be owned by everyone
involved in the NHS, but driven by
those who are experts in the field.
This is why I am so pleased to see a
guide such as this which represents
the joint endeavour of enthusiastic
Clinicians and experts in VTE.
Professor Sir Bruce Keogh has
been NHS Medical Director since
November 2007 and is responsible
for the Clinical Policy and Strategy,
Healthcare Quality and Medicines,
Pharmacy and Industry Divisions
within the Department of Health.
He oversees the work of NICE, the
National Patient Safety Agency
and Medical Education England.
3
Veno
us Throm
boem
bolism Preve
ntion A
Guide
for D
elivering the CQUIN
Goa
l
NHS Medical Director

4
The development of the National
VTE Prevention Programme over
the last five years was prompted
initially by the recommendations
of the Health Select Committee
Report on the Prevention of VTE
in Hospitalised Patients in 2005
and was made manifest by the
recommendations of the Chief
Medical Officer’s VTE expert group
in April 2007, which sought to
address the issue of reducing
avoidable death, long-term
disability and chronic ill health
from VTE in hospitalised patients.
The programme focuses on risk
assessment, as this is the trigger
for the VTE prevention pathway.
Thinking about the risks of VTE
and bleeding in each patient will
increase thromboprophylaxis rates
and improve outcomes by ensuring
appropriate prophylaxis.
The implementation phase of the
programme includes a new
mandatory data collection, which
began on 1 June 2010, to allow
reporting and monitoring of VTE
risk assessment nationally. This
monthly census through UNIFY has
financial and logistical implications
for our Trusts. A national goal on
VTE risk assessment was included
within acute provider CQUIN
schemes for 2010-11 to support
the work on VTE prevention,
linking payment to at least 90% of
adult patients being risk-assessed
for VTE on admission to hospital.
Although most Trusts already have
risk assessment procedures in
place, the CQUIN goal requires
that the risk assessment and
exclusion criteria described in the
National risk assessment tool are
employed in full, with no
exceptions or opt-outs agreed by
the Department of Health to the
policy of assessing VTE risk in all
patients on admission. A ‘cohort
approach’ to risk assessment using
the National VTE risk assessment
tool may be considered locally for
certain patients. This approach
allows Medical Directors (local and
SHA) to make a clinical decision
regarding a group of patients
admitted for the same procedure
who are felt to have a similar risk
PrefaceDr Roopen Arya
Prevention of venous thromboembolism (VTE) has been identified as the most important
safety practice in our hospitals. There is increasing awareness of the burden of disease due to
VTE and most hospitals already have thrombosis committees and guidelines for
thromboprophylaxis. This is the moment when systems, procedures and the culture within our
hospitals must change to ensure delivery of the National VTE Prevention Programme in
England. The measures that have been introduced, including the new national mandatory
data collection of VTE risk assessment linked to a national CQUIN goal, the implementation of
NICE guideline 92, and the recent publication of the NICE VTE quality standard, reflect the
recognition of VTE prevention as a top clinical priority for the NHS by the National Quality
Board, the NHS Management Board, and the Academy of Medical Royal Colleges. The National
VTE Exemplar Centre Network continues to play a key role at this juncture by bridging
national strategy and local implementation and disseminating best practice across the NHS.

5
Veno
us Throm
boem
bolism Preve
ntion A
Guide
for D
elivering the CQUIN
Goa
l
profile and are assessed as a group
as being at no risk of VTE. Medical
Directors are asked to take
responsibility for compliance and
SHA Medical Directors in quality
assurance of this national
approach. There are significant
organisational challenges for Trusts
to ensure that all patients within
the denominator of the CQUIN
goal are risk assessed, and
logistical challenges to ensure that
the risk assessment data are
collected accurately.
Undoubtedly, this implementation
phase is a major challenge for all of
us in the year ahead. But I think this
is one of the best opportunities that
we have as clinicians to
demonstrate our collective
leadership and to help guide the
NHS in a way that’s good for
patients and help shape its future.
With this in mind, King’s
Thrombosis Centre, in conjunction
with Lifeblood and then NHS
London, arranged two workshops
to facilitate exchange of ideas and
sharing of resources to address the
challenges around delivery of the
CQUIN goal and other aspects of
the National VTE Prevention
Programme. This resource book
hopes to capture many of the
excellent suggestions made at the
workshops and I wish to thank all
the participants who gave openly
of their time, materials, intellect
and energy.
The content of this guide also
leans heavily on the work being
undertaken within the VTE
Exemplar Centre Network. There
are now sixteen VTE Exemplar
Centres, spanning the length and
breadth of the country and
incorporating diverse models of
healthcare within the NHS. These
include acute hospital Trusts (from
200 to 2000 beds), North
Lancashire Teaching PCT and the
South West SHA forming an
enlightened network of centres of
excellence in VTE care. Under this
‘kite-mark’ for good practice in
VTE care, Exemplar Centres share
examples of good practice such as
clinical best practice and
educational and audit material,
provide advice regarding VTE care,
receive visitors and collaborate on
clinical research into VTE. We hope
to have captured many of the
innovative VTE prevention practices
being developed within the
Exemplar Centre Network in this
guide. The Exemplar Centre
website, hosted by the King’s
Thrombosis Centre, provides easy
access to these materials, with each
Exemplar Centre equipped with a
resource page for download of
protocols and other materials.
We should feel justifiably proud of
the National VTE Prevention
Programme, which is identified by
Professor Bill Geerts in this guide as
perhaps the most comprehensive
of any healthcare system in the
world. There is now a unique
opportunity for the NHS to move
forward using a standardised VTE
risk assessment tool, linked to NICE
guidance on thromboprophylaxis
and underpinned by a robust
quality framework. It will be a
considerable achievement when
VTE prevention is fully integrated
into NHS systems and will be
hugely beneficial to our patients.
London, 14 June 2010
Director, King’s Thrombosis CentreLead, National VTE Exemplar CentreInitiativeLondon Director of Thrombosis

6
Anecdotal evidence suggests that
VTE prevention is not being
delivered effectively on the ground
due to perceived difficulties in
delivering the CQUIN goal. For this
reason, Lifeblood and the VTE
Exemplar Centre Network hosted a
national workshop on 26th April
2010 at BMA House in London,
inviting Chairs of Thrombosis
Committees to feedback their
experiences in attempting to deliver
the CQUIN goal, and to share
examples of how some of these
difficulties have been overcome.
The workshop was oversubscribed.
We were pushed to capacity with
over 60 Trusts represented – and
many more kept on the waiting list
and requesting feedback following
the event. The workshop made it
resoundingly clear that Trusts up
and down the country are facing
similar practical barriers to
implementing best practice.
However, it was an extremely
productive exercise, allowing us
to listen to and learn from Trusts
that have managed to come up
with innovative and often
simple methods of overcoming
these barriers.
This Guide forms the output of that
workshop. It brings together the
key challenges and suggested
solutions, which we hope will
together enable those responsible
for overseeing or implementing
VTE prevention on the wards, to
deliver the CQUIN goal. We would
like to thank everybody who
attended the workshop and thus
contributed to this Guide (see
picture). We strongly believe that
shared learning of best practice
can ensure Trusts are able to meet
the VTE CQUIN goal, and in so
doing, deliver the real life saving
intervention that VTE prevention
so clearly provides.
On 8th June 2010, as this guide
went to Press, the new Secretary of
State for Health, Rt Hon Andrew
Lansley MP, reiterated the new
coalition-government’s desire to
“involve patients more in the care
they receive, to remove central
targets and to create an NHS
focussed on patient outcomes”.
Such a focus on outcomes,
specifically on the decision not to
reimburse secondary care providers
for patients readmitted within 30
days, has huge relevance for Trusts
with sub-optimal systems for
preventing VTE in their patients.
IntroductionProfessor Beverley Hunt
Clinicians across England will rightfully support the Department of Health’s recognition that
hospital-acquired venous thromboembolism (VTE) prevention be made a clinical priority for
the NHS for 2010, by making it a national goal in the Commissioning for Quality and
Innovation (CQUIN) payment scheme for hospitals. Incentivising hospitals to put evidence-
based steps in place to ensure all patients are assessed for their risk of hospital-acquired
clots will enable those at-risk patients to receive the life-saving preventative measures they
need. At the same time, NICE has estimated this is highly cost-effective and will save NHS
money by reducing the need to treat acute VTE and the long-term effects of those who
survive their clot.

7
Veno
us Throm
boem
bolism Preve
ntion A
Guide
for D
elivering the CQUIN
Goa
l
Whilst the majority of centralised
targets may become yesterday’s
news, the long-term priority of
preventing hospital-acquired VTE
will not. The requirement to
perform mandatory VTE risk
assessment and prescribe
appropriate thromboprophylaxis
will continue, as the Secretary of
State’s assertion that ‘high levels of
infection, VTE, emergency
readmissions, falls, and pressure
sores all lead to suffering and cost’,
is undoubtedly correct. Ultimately
good care is safe care and in these
times of fiscal prudence, we are
assured that the NHS will continue
more than ever to eliminate unsafe
care which costs more, in lives and
in cash.
Therefore, efforts made to
undertake effective clinical audit
now, so as to achieve the CQUIN
VTE target, will pay dividends in
both the future prevention of VTE
and for the future monitoring of
each Trust's reimbursement linked
clinical outcomes.
Professor of Thrombosis & Haemostasis,King’s College, London
Consultant, Guy’s & St Thomas’ NHSFoundation Trust
Medical Director, Lifeblood: TheThrombosis Charity (Health charity of the year 2010).
Access the website at: www.thrombosis-charity.org.uk
Attendees at the VTECQUIN goal workshop,BMA House, 26 April 2010.
8
The National VTE Prevention Programmein England is in place and is perhaps themost comprehensive of any healthcaresystem. The implementation phase beganin early 2010 and aims to ensure that alladult patients admitted to hospital arerisk-assessed for VTE and receiveappropriate thromboprophylaxis. Thisprogress has been made possible by thesteadfast commitment of many partnersand stakeholders, who have worked withthe Chief Medical Officer and NHSMedical Director on this patient safetyinitiative. The Academy of Royal Collegesis providing professional leadership andthe National Exemplar Network is helpingto promote and deliver best practice.System levers such as the CQUIN goal arein place1, NICE quality standards are indevelopment2 and the NHS LitigationAuthority are piloting a risk managementstandard on VTE in 2010/11 (criterion4.11)3. VTE now lies at the centre of ourquality framework.
The CQUIN framework, VTE goal andquality indicator for VTE prevention
High Quality Care for All included acommitment to make a proportion ofproviders’ income conditional on qualityand innovation4, through theCommissioning for Quality and Innovation(CQUIN) payment framework. Theframework, launched in April 2009, aimsto support the vision set out in High
Quality Care for All of an NHS wherequality is the organising principle and ispart of the commissioner-providerdiscussion everywhere.
The Department of Health (DH) guidanceon using the CQUIN payment frameworkwas recently supplemented by anaddendum, which outlines developmentsto the framework for 2010/111. Inconjunction with the NHS OperatingFramework for 2010/115 and the nationalstandard contracts for acute, ambulance,community, mental health and learningdisability services6, these contracts requirecommissioners to make 1.5% of contractvalue available for providers to earn if theyachieve locally agreed quality improvementand innovation goals. CQUIN payments areconditional on the provider achieving theCQUIN goals set out within the contract.For cash flow purposes, the defaultposition in 2010/11 contracts is that 50%of the financial value of the scheme is paidto the provider in advance in monthlyinstalments, with reconciliation againstperformance at least at months 3, 6, and 9as well as at year end.
CQUIN schemes for acute providers (allproviders of NHS funded care deliveringrelevant acute services under the NHSStandard Contracts for acute hospitals orcommunity services, including FoundationTrusts, NHS Trusts and independent sectorproviders) in 2010/11 must include two
nationally defined goals, which relate toreducing the impact of VTE and improvingresponsiveness to personal needs ofpatients. These goals each have a specifiedindicator and in total are linked to arounda fifth of the value of schemes (0.3% ofprovider income). Specifically, the VTEnational goal for acute CQUIN schemes in2010/11 is to ‘reduce avoidable death,disability and chronic ill health from VTE’.The quality indicator that will be measuredto show achievement of the national goalis the percentage of all adult inpatientswho have had a VTE risk assessment onadmission to hospital, using the nationalrisk assessment tool. CQUIN payment willbe dependent on achieving at least 90%of admissions risk assessed.
The new mandated VTE risk assessmentdata collection (ROCR/OR/0276/FT6/000MAND) will be via UNIFY, and the firstmandatory monthly return will report onpatients admitted in June 2010 and mustbe submitted no later than 28 July 2010.Trusts may submit data before this time ona voluntary basis relating to admissions inApril and May 2010 and a return must besubmitted each month. The requirementwas delayed from April 2010 in order togive providers time to develop or modifylocal systems to enable reporting viaUNIFY. Detailed guidance on the datacollection is available in draft form on theUNIFY system currently. It should beemphasised that the requirement is for a
Venous thromboembolism preventionin the quality framework
At this point, the NHS in England is in the unique position internationally of having a national
risk assessment tool for venous thromboembolism (VTE) in hospitals together with
comprehensive national clinical guidance for appropriate thromboprophylaxis. The inclusion
of a goal on VTE prevention within all acute CQUIN schemes in 2010/11 helps commissioners to
ensure that these national best practice resources on VTE are effectively used for the benefit of
patients at local level. There is a strong feeling in the NHS that this is the key point to move
forward on VTE prevention with respect to patient safety and quality of care.

monthly census through UNIFY, ratherthan a snapshot audit and that all patientsmust undergo risk assessment.
NICE clinical guideline 92
NICE published its clinical guidance(clinical guideline 92) on reducing the riskof VTE for adults admitted to hospital asinpatients (including those admitted for
day-case procedures) in January 20107.This guidance updates and replaces NICE’sprevious guidance produced in April 2007(clinical guideline 46)8. Thiscomprehensive guidance offers specificcare pathways for all patients and providesspecific criteria for assessing the risks ofboth VTE and bleeding across the range ofpatient groups. The recommendations forreducing the risk of VTE include
pharmacological and mechanicalmethods. The guideline recommends thatrisk of bleeding and VTE are reassessedwithin 24 hours of admission andwhenever the clinical situation changes.Other recommendations include ensuringthat the methods of VTE prophylaxisemployed are suitable, that VTEprophylaxis is being used correctly andthat hospitals should identify adverseevents resulting from VTE prophylaxis.
The ‘NHS Standard Contract for AcuteServices’ and VTE prevention
The national contracting process stipulatesthat providers are expected to ensure thatpatients receive appropriate prophylaxisfor VTE based on national guidanceaccording to their risk assessment, andalso to carry out root cause analysis on allconfirmed inpatient cases of VTE. Morespecifically, from April 2010 the contractrequires Trusts to:
(1) Report to their lead commissioner onlocal audits of the percentage ofpatients risk-assessed for VTE whoreceive the appropriate prophylaxis,both the risk assessment and theprophylaxis being based on nationalguidance. (Where appropriateprophylaxis is used but is not based onnational guidance, the reasons for thisclinical decision will need to be fullydocumented.)
(2) Undertake and report to their leadcommissioner on root cause analysis ofall confirmed cases of hospital-acquiredPE and DVT (including those arisingfrom a current stay or new eventsarising where there is a history ofadmission to hospital within the lastthree months, but not includingpatients admitted to hospital with aconfirmed VTE with no history of anadmission to hospital within the lastthree months).
9
Veno
us Throm
boem
bolism Preve
ntion A
Guide
for D
elivering the CQUIN
Goa
l
UNIFY
UNIFY2 is the main online data collection portal used by the NHS to collect and shareperformance information, aggregate data and statutory returns.
Data collection form: The upload template for data collection will be made availablethrough the Non-DCT collections area of UNIFY2. The ‘control panel’ will allow the userto specify which provider they are from, for which month they are reporting, and alsonotifies the user of any validation errors which must be accounted for before uploadingto UNIFY2.
Submission:Data on VTE risk assessment should be uploaded onto UNIFY2 and signedoff no later than 20 working days after the month end e.g. information relating to June2010 must be submitted no later than 28 July 2010.
Sign off policy: Data collection can be signed off at provider level. Commissioners orStrategic Health Authorities (SHAs) are not required to sign off this collection.
Revisions policy: Revisions before the cut off date for submission of data will beallowed, and can be made as many times as necessary. These revisions can be submittedin the normal way through UNIFY2. As stated above, this cut off date will be 20 workingdays after the month end. Revisions after the cut off date can also be made, but thesemust be done in liaison with DH colleagues.
Fig 1DVT presenting as a swollen leg; hospital-acquired VTE can be asymptomatic, hence the term ‘silent killer’.
Image courtesy of James Heilman, MD on Wikipedia.

10
NICE quality standard
As a result of High Quality Care for All,NICE was tasked with developingindependent standards clarifying whathigh quality care looks like in relation tothe three dimensions of quality, namelyclinical effectiveness, patient safety andpatient experience4. This work is a keypart of making quality the organisingprinciple of the NHS. NICE qualitystandards will act as a final distillation ofclinical best practice, derived from thebest available evidence from NICEguidance or other sources accredited byNHS Evidence to provide a set of specificconcise quality statements andassociated measures that act as markersof high quality, cost effective patient careacross a pathway or clinical area; arederived from the best available evidence;and are produced collaboratively with theNHS and social care professionals, alongwith their partners and service users.
The primary purpose of NICE qualitystandards is to bring clarity to matters ofquality by providing patients and thepublic, health and social careprofessionals, commissioners and service providers with definitions of high quality care and provide a cleardescription of what a high quality servicewould look like, enabling organisationsto aspire and progress to improve qualityand achieve excellence. They areintended to support benchmarking ofcurrent performance against evidencebased measures of best practice and toidentify priorities for improvement.
The scope of the quality standard for VTEprevention is the reduction in risk of VTEin adults admitted as hospital inpatientsor formally admitted to a hospital bed forday-case procedures2.
Pregnant women and women up to 6weeks post partum are also specificallycovered.
1. All patients, on admission, receive anassessment of VTE and bleeding riskusing the clinical risk assessmentcriteria described in the national tool.
2. Patients/carers are offered verbal andwritten information on VTE preventionas part of the admission process.
3. Patients provided with anti-embolismstockings have them fitted andmonitored in accordance with NICE guidance.
4. Patients are re-assessed within 24hours of admission for risk of VTE and bleeding.
5. Patients assessed to be at risk of VTEare offered VTE prophylaxis inaccordance with NICE guidance.
6. Patients/carers are offered verbal andwritten information on VTE preventionas part of the discharge process.
7. Patients are offered extended (posthospital) VTE prophylaxis inaccordance with NICE guidance.
CQUIN and VTE prevention beyond 2011
CQUIN monies are non-recurrent toproviders, as they are conditional uponquality improvement goals which areagreed annually. CQUIN payments areseparate from tariff and non-tariffcontract income. It is understood that theGovernment is currently working toinclude VTE risk assessment within thestandard acute contract to ensure thelegacy of the national VTE programmecontinues if the data collection goal is notrenewed in 2011. This is in line with theDH’s 5 year strategy ‘NHS 2010–2015:from good to great. Preventative, people-centred, productive’, whichmade eliminating avoidable cases of VTEone of a number of safety challenges tobe met over the next five years9.
Fig 3NICE clinical guideline 92 was publishedin January 2010. National CQUIN goalfor VTE was specified in an addendum
to original CQUIN policy guidance.
Fig 2VTE prevention care pathwayfor all hospital admissions(NICE clinical guideline 92).
Patient admitted to hospital
Assess VTE risk.
Assess bleeding risk.
Balance risks of VTE and bleeding.
Offer VTE prophylaxis if appropriate. Do not offerpharmacological VTE prophylaxis if patient has any risk factorfor bleeding and risk of bleeding outweighs risk of VTE.
Reassess risks of VTE and bleeding within 24 hours ofadmission and whenever clinical situation changes.

11
Veno
us Throm
boem
bolism Preve
ntion A
Guide
for D
elivering the CQUIN
Goa
l
Patients who are at risk of VTE
Medical patients Surgical patients and patients with traumaIf mobility significantly reduced for If total anaesthetic + surgical time > 90 minutes or≥ 3 days or If surgery involves pelvis or lower limb and totalIf expected to have ongoing reduced anaesthetic + surgical time > 60 minutes ormobility relative to normal state plus any If acute surgical admission with inflammatory orVTE risk factor. intra-abdominal condition or
If expected to have significant reduction in mobility orIf any VTE risk factor present.
VTE risk factors1
Active cancer or cancer treatmentAge > 60 yearsCritical care admissionDehydrationKnown thrombophiliasObesity (BMI > 30 kg/m2)One or more significant medical comorbidities (for example: heart disease; metabolic, endocrine orrespiratory pathologies; acute infectious diseases; inflammatory conditions)Personal history or first-degree relative with a history of VTEUse of HRTUse of oestrogen-containing contraceptive therapyVaricose veins with phlebitis
1 For women who are pregnant or have given birth within the previous 6 weeks see page 23.
Patients who are at risk of bleeding
All patients who have any of the following.Active bleedingAcquired bleeding disorders (such as acute liver failure)Concurrent use of anticoagulants known to increase the risk of bleeding (such as warfarin with INR > 2)Lumbar puncture/epidural/spinal anaesthesia within the previous 4 hours or expected within the next12 hoursAcute strokeThrombocytopenia (platelets < 75 x 109/l)Uncontrolled systolic hypertension (≥ 230/120 mmHg)Untreated inherited bleeding disorders (such as haemophilia or von Willebrand’s disease)
A
Does risk of VTE outweigh riskof bleeding?
Has patient beenadmitted for stroke?
Is pharmacological VTEprophylaxis contraindicated?
See page 13.
Offer pharmacological VTEprophylaxis with any one of:
fondaparinuxLMWH5
UFH6.
Continue until patient no longerat increased risk of VTE.
Consider offering mechanicalVTE prophylaxis with any one of:
anti-embolism stockings(thigh or knee length)foot impulse devicesintermittent pneumaticcompression devices (thighor knee length).
Reassess risks of bleeding and VTEwithin 24 hours of admission andwhenever clinical situation changes.
Yes No
Yes No
Yes No
General medical patients
Fig 5Care pathway for general medicalpatients (NICE clinical guideline 92).
Fig 4Assessing risks of VTE and bleeding(NICE clinical guideline 92).

12
Understand the denominator for the VTE CQUIN goal
Commissioners and provider need tocomplete the template within thecontract, including time periods on whichperformance is assessed, and ensure aclear understanding of the numerator and denominator and data collectionarrangements and timings. Figure 6(right) shows the aspect of the uploadtemplate that will require providers toenter the information specified – foundon the tab ‘Frontsheet’. Aspects (i) and (ii)are entered by providers, but (iii) isautomatically calculated from items (i)and (ii) and cannot be overwritten.
The DH has confirmed that thedenominator specified for the CQUINcensus is the number of adults admittedas inpatients10. This specifically includesday cases (including regular day caseattendees), maternity cases, andtransfers, both elective and non-electiveadmissions. There are no exceptions inprinciple to the policy of all adult patientsreceiving a risk assessment for VTE on
admission (ordinary and day cases). It is not the intention to replace anenthusiastic consensus on riskassessment, which is based on theperception that this something worthdoing for the good of patients, with abureaucracy that irritates and alienateshealth care professionals required to
deliver the care. This data collection onVTE risk assessment is intended to embed VTE risk assessment across theNHS and will be critical in evaluating theimpact of the National VTE PreventionProgramme on improving healthoutcomes for patients.
Essential first steps to achieve theCQUIN goal
The number of adult inpatients(ordinary admission and day care)
admitted in the month who have beenrisk assessed for VTE using the National
Tool on admission to hospital.
Month Actual
i 0
ii 0
iii 0%
Total number of adult inpatients(ordinary admission and day care)
admitted in the month.
Percentage of adult inpatients admittedin the month assessed for risk of VTE
on admission.
VTE Risk Assessments on Admission to Hospital
Trusts must employ the correct denominator for the VTE CQUIN goal quality indicator, which is
the total number of adult inpatients (hospital admission will be as defined by your PCT and will
include day cases and transfers). For the numerator (number of adult inpatients risk assessed),
a ‘cohort approach’ to certain risk assessment in some patient groups may be permissible;
these must be agreed with the Trust Medical Director in advance. Any patient regarded as part
of a cohort is deemed to have been risk assessed, not exempted from risk assessment. In order
to achieve the CQUIN goal, Trust Chief Executives should engage with NHS commissioners and
agree a local package of VTE prevention initiatives to support the national programme and
review these in the context of an SHA-wide programme of work. Institutional support and
prioritisation of VTE prevention are essential to ensure the necessary VTE metrics are delivered.
Next steps to ensure delivery of the CQUIN goal include identifying a lead physician, forming a
multidisciplinary team to lead the change and identifying what success will look like.
Fig 6Data collection form for Non DCT collection.

13
Venous Throm
boem
bolism Prevention A Guide for Delivering the CQUIN Goal
What constitutes a day case?
For the purposes of data collection onVTE risk assessment, the definition of anadmission is subject to local admissionspolicies and local arrangements foradmission criteria. The UNIFY collectioncovers all those patients who, under localdefinitions, have been admitted tohospital, either for a day case procedureor as an ordinary admission. This datacollection is a census of all patients – it is not considered appropriate to usesampling methodologies to produceestimates.
The definition of a Day Case admissioncan be found within the description of theNHS Data Model and Dictionary attributePatient Classification:
“A patient admitted electively during thecourse of a day with the intention ofreceiving care who does not require theuse of a hospital bed overnight and whoreturns home as scheduled. If this originalintention is not fulfilled and the patientstays overnight, such a patient should becounted as an ordinary admission.”
For patients who make daily ward visits,such as those allowed to go home everynight and attend the next day for the nextcourse of treatment, for examplechemotherapy, the activity is recorded as aseries of admissions, with the Patient
Classification recorded as National Code03 Regular Day Admission, defined by theNHS Data Model and Dictionary as:“A patient admitted electively during theday, as part of a planned series of regularadmissions for an on-going regime ofbroadly similar treatment and who isdischarged the same day. If the intentionis not fulfilled and one of these admissionsshould involve a stay of at least 24 hours,such an admission should be classified asan ordinary admission. The series ofregular admissions ends when the patientno longer requires frequent admissions.”
Numerator of the CQUIN goal
The numerator of the CQUIN goal is thenumber of adult inpatients (ordinaryadmission and day care) admitted in themonth who have been risk assessed forVTE using the National Tool on admissionto hospital.
A ‘cohort approach’ to risk assessmentusing the National VTE risk assessmenttool may be considered locally for certainpatients undergoing procedures wherethat cohort of patients share similarcharacteristics and are not at risk of VTEaccording to the NICE guidance11,12. Thisapproach to risk assessment can only beused when the Trust Medical Director issatisfied that, when using the NationalVTE risk assessment tool in conjunctionwith the NICE guidelines, the cohort
would always be regarded as not at risk of VTE, or no pharmacological ormechanical prophylaxis would beappropriate regardless of the risk factors.Any such local protocols must be agreedwith the Trust or hospital MedicalDirector, and included within local VTEgovernance policy and audits. SHAMedical Directors will be involved in theassurance of this approach. Any patientregarded as part of a cohort is deemed tohave been risk assessed, not exemptedfrom risk assessment.
The Trust/hospital Medical Directors areresponsible for signing off that the VTErisk assessment being used at a local levelis fully compliant with the National VTErisk assessment tool and that all riskfactors have been taken into account.SHA Medical Directors have providedguidance on which cases might besuitable for a cohort approach. Examplesof day case procedure groups that havebeen assessed as being at low risk of VTEusing the National VTE risk assessmenttool/NICE guidance include haemodialysisand cataract surgery (specificallyophthalmological procedures with localanaesthetic/ regional/sedation and notfull general anaesthetic).
Pregnancy and VTE prevention
VTE is a major source of maternalmortality and morbidity in pregnancy and many of these events are potentiallypreventable through identification of riskand appropriate prophylaxis. The RoyalCollege of Obstetricians andGynaecologists has a set of guidelinesentitled Thrombosis and Embolismduring Pregnancy and the Puerperium,Reducing the Risk (Green-top 37), whichare widely employed in clinical practice.The NICE guideline includes pregnancyand the puerperium as risk factors andthe Green-top guideline was consideredduring the NICE guideline development;
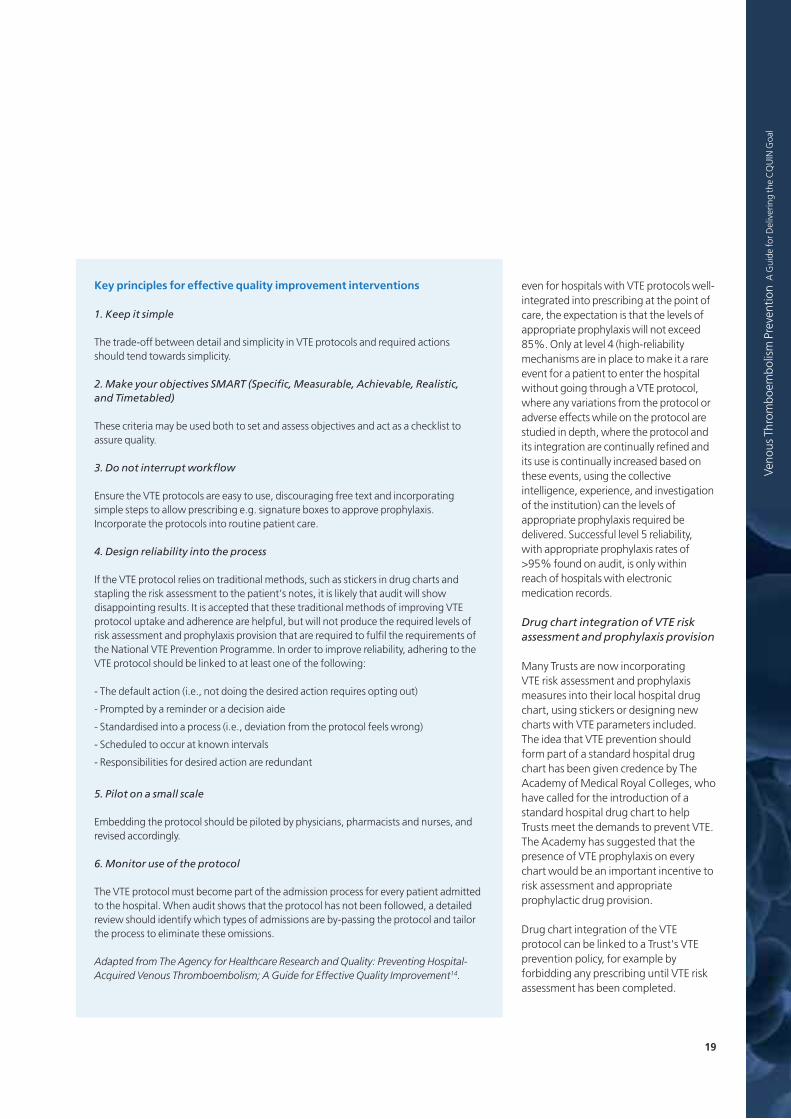
Case study
The East of England (EoE) SHA commissioning framework requires that contracts forservices should ‘ensure that all patients (inpatient and day-case patients) receiveevidence-based VTE risk assessment on admission and if their clinical status changes,that appropriate thromboprophylaxis is administered to reflect the risk profile from the risk assessment.’ EOE PCT operational plans have been scrutinised by the SHAto ensure that the key delivery components for VTE are included in sufficient detail i.e.services commissioned in line with new NICE guidance and subject to the nationalCQUIN goal.

14
it is the intention that the Green-topguideline is consistent with the clinicalpractice recommendations included inthe NICE guideline.
Recommendations for risk assessment ofpregnant women as part of the CQUINgoal are not different; women admittedto hospital are to undergo a riskassessment and these figures to formpart of the census.
Engage with your PCT/Commissioners
In England, PCTs are the local NHScommissioners. They consult and workcollaboratively with a variety of partnerswithin and outside the NHS, but areultimately accountable for commissioningdecisions, the budget, and health, well-being and clinical outcomes. They have tobe able to publish a credible account ofeffectiveness, efficiency and equity. It isincumbent upon commissioners toensure that the services they commissionassess all patients for risk of VTE using anassessment tool complying with the mostrecent NICE and DH guidance and thatthose services comply with NICE guidanceon the prescription of VTE prophylaxisand in the near future with the NICEquality standard for VTE prevention.
The CQUIN framework remains a nationalframework for locally agreed schemes,and it is incumbent on commissioners andproviders to discuss and agree how totranslate these national goals into actionat local level. Many Trusts, particularlythose without an electronic riskassessment tool and reliant on paper, willfind it difficult to put in place the necessaryprocesses to ensure compliance with the90% threshold for risk assessment by June1st. Therefore, the recommendation is tobegin a constructive engagement withcommissioners immediately, focusing onthe entire package of VTE preventioninitiatives being undertaken within the Trust.
Effective engagement by PCTs and Trustsis critical in agreeing the regionalmeasures, which will include not just thegoal of VTE risk assessment alone, butalso the fulfilment of the NHS StandardContract obligation to audit appropriateprophylaxis and undertake root cause
analysis of all cases of hospital-acquiredVTE. For many Trusts, agreement hasalready been made with localcommissioners to deliver the package ofVTE prevention initiatives in a slightlyextended timetable, looking at completecompliance by Q3 or Q4 of 2010. Clearly,identifying cases of hospital-acquiredVTE, performing root-cause analysis, andfeeding back the results into the clinicalrisk management framework of Trustswill require significant culture change.Introducing the risk assessment goal is atrigger for this, and is at the top of thispathway; but gradually, over the nextfew months, layering additionalinterventions such as thromboprophylaxisaudit and in-hospital VTE education willbe required to make this wholeprogramme of VTE prevention a success.
An SHA-wide programme of work
Determine how Trusts in your local SHAare interacting and assess the value ofdeveloping an SHA-wide programme forVTE prevention. Integrating local effortsinto a single SHA-wide vision for VTEprevention and the identification of acommon vision helps resource sharing,aides operational implementation andsharing of best practice.
Institutional support andprioritisation of VTE prevention
In March, the Chief Medical Officer andthe NHS Medical Director issued a ‘DearColleague’ letter to ask that the ChiefExecutives of all acute providers (whohave not already done so) ensure theintroduction of procedures to supportthe forthcoming mandatory datacollection relating to VTE risk assessmentby 1 June 2010, and for all MedicalDirectors to ensure by that time that any
risk assessment templates used locallyhave the same clinical risk assessmentcriteria as are summarised in the revisedNational VTE risk assessment tool10.Although the communications in Marchand April from the Chief Medical Officer,the NHS Medical Director and theAcademy of Medical Royal Colleges willhave ensured that all Trusts are aware ofthe requirements of the National VTEPrevention Programme, many will still bedeveloping programmes to addressachieving these VTE preventionimprovements. Institutional support andprioritisation for the initiative, expressedin terms of policy, a meaningfulinvestment in time, equipment,personnel, and informatics, and a sharingof institutional improvement experienceand resources to support any projectneeds, are vital to ensure success. Simplesteps of updating Trust policy to reflectthe VTE goal, for example by forbiddingprescribing until a VTE risk assessmenthas been documented, offer credenceand priority to VTE prevention.
Identify a lead physician, form amultidisciplinary team and developan action plan
Awareness of VTE prevention has neverbeen higher and all medical staff will havebeen contacted by their Royal Collegeregarding the National VTE PreventionProgramme13. Engaging senior Trust staff,including medical directors andconsultants and then nominating clinicalarea leads to take responsibility for VTEprevention is essential.
Identifying an appropriate clinical leadwith management responsibility isvaluable. Most hospitals will have in placea multi-disciplinary thrombosis committeethat can drive the process and ensure
Case study
At Chelsea and Westminster Hospital NHS Foundation Trust, the senior managementsupported VTE prevention by seeking the support of the Executive Clinical GovernanceCommittee and specifying the reduction of hospital-acquired pulmonary embolism as aquality indicator in the Trust.
At King’s College Hospital NHS Foundation Trust, VTE metrics will be incorporated as ‘keyperformance indicators’ in the Trust Clinical Scorecard. Senior management supports theintegration of VTE risk assessment as a mandatory field for electronic clerking.

15
Veno
us Throm
boem
bolism Preve
ntion A
Guide
for D
elivering the CQUIN
Goa
l
changes required across the organisationare delivered. It is important to engageother clinical area leads to ensure actionacross the whole trust. Well-tried projectmanagement techniques offer a valuableframework to begin the process and willinclude a formal action plan withlandmark achievements and a detailedtimeline for delivery. The thrombosiscommittee should develop and drive asystematic approach towards improvingthe VTE metrics, and these metrics shouldbe embedded into performanceindicators in the Trust.
Identify what success will look like
It is important to identify in your Trust,and in your region or SHA, what successwill look like. In a broad sense, it isessential to develop a systems-basedapproach to the prevention of VTE inhospitalised patients to ensure success.This requires a professional workforceaware of the VTE risk, system-driven riskassessment and prophylaxis provisionand evaluation of outcome.
The Federal Agency for Healthcare,Research and Quality in the United Stateslooked at 79 different safety interventionsincluding infection control, and identifiedVTE prevention to be the most effective.
They have sought to define an ideal VTEprotocol and offered this view: it shouldbe applicable across all the patients inscope such that it is definite in itsauthority and also modifications can bemade after feedback. It should be easy to access and use, and it should link each level of risk to an evidence-basedchoice for prevention and also listcontraindications to prophylaxis andprovide suitable alternatives14. The National VTE risk assessment tool,linked to the NICE guidelines complieswith all these elements and the challenge is delivering this ideal protocolin our hospitals. Introducing thisprotocol, ensuring VTE risk assessmentand delivering the National VTEPrevention Programme will requirechange in almost all Trusts. The followingelements are essential in supporting thechange required to achieve the VTEprevention goals:
- Prioritisation and support for VTEprevention by Trust management
- Introduction of protocols thatstandardise VTE risk assessment andprophylaxis provision
- Embedding VTE prevention protocolsinto patient care
- Ensuring reliable data collection andperformance tracking
- Ensuring educational programmes are created to support the protocols
Royal College instructions to all members
In April, the Academy of Medical RoyalColleges instructed all Colleges andFaculties with Fellows and Membersinvolved in direct patient care to:
1. Bring to the attention of all theirFellows and Members theimportance of risk assessment andappropriate prophylaxis for venousthromboembolism in all patientsadmitted to hospital. This includesthe assessment of risk in primary careat the time of referral to hospital.
2. Emphasise that all Fellows andMembers should ensure that theirclinical unit has systems in place toensure all patients are assessed forVTE prophylaxis and that the reasonsfor the resulting decision aredocumented and appropriatetherapy given. This may be achievedthrough modifying drug charts, forexample.
3. Ensure Fellows and Membersparticipate in regular audit of thepercentage of patients risk-assessedfor VTE. In some specialties this issuitable for becoming a mandatorystandard for revalidation.
4. Produce specialty-specific guidancewhere needed.
5. Continue emphasis of theimportance of VTE in undergraduateand postgraduate curricula andtraining programmes, and promotionthrough various e-learning initiatives.
Fig 7Defining success in VTE prevention
(Dr Anita Thomas, National Clinical Lead for VTE).
Case study
The EoE VTE project is an SHA-wide initiative. The VTE project was initiated in 2009 under the ‘Towards the best, together’ vision and meeting the sixth pledge in Improving Lives; Saving Lives: “We will make our health service the safest inEngland.” The EoE VTE project is leading the way for the region to implement bestpractice and provide health professionals with the skills to implement thesemeasures. The objectives of the project are:
- To reduce the incidence of hospital-acquired VTE in all EoE hospitals by 50%
- To develop systems, processes and audit for VTE prevention in secondary care
- To include VTE measures in the commissioning framework for all secondary care
- To develop and implement a process measure tracking mechanism and specimencontract schedule for inclusion in 2010/11 contracts
- To provide training and education to all health professionals on the preventionand treatment of VTE.
The EoE VTE project is shown in more detail on page 21 of this book.
Patient admitted to hospital
Evaluation of outcome
Professional workforce aware of VTE risk
Organisation and system support for riskassessment and appropriate prophylaxis
Individual patient risk assessed for VTE
Appropriate preventative strategy implemented

16
In September 2008, the Chief MedicalOfficer released the National VTE riskassessment template. Authored by theVTE Implementation Working Group inconsultation with the main stakeholdersin VTE, this was a useful evidence-basedtool to raise awareness and guide the riskassessment process. With the publicationof NICE clinical guideline 92 in January20107, the National tool was updated byDH in collaboration with NICE andimportantly included a single tick optionfor mobile medical patients to completethe risk assessment. It is the informationin this tool that sets out the criteria forVTE risk assessment that the DH expectsall Trusts to employ as part of themandatory data collection on riskassessment. The National VTE riskassessment tool is reproduced in full inthe resource section of this book.
Local modifications of the riskassessment tool
It is expected that Trusts will modify theirlocal risk assessment process to ensure this basic data set is incorporated into theirlocal documentation and systems, eitherpaper-based or electronic, and it is theseelements that must be completed to ensurethe CQUIN quality indicator is achieved. Toensure compliance with the NICE VTEquality standard, the document shouldinclude risk assessment on admission andre-assessment within 24 hours of admissionfor risk of VTE and bleeding. Many Trustshave created a unified risk assessment andprophylaxis provision tool, incorporatingNICE-compliant thromboprophylaxisrecommendations into a single document.
Paper-based risk assessment tools
The addition of patient identifiers,signature lines and additional columns tofacilitate easy addition of locally-requiredinformation can tailor the risk assessmenttool to local needs. Examples of modifiedpaper-based risk assessment tools areprovided in the resources section.
Electronic risk assessment
In the long term the answer to thechallenges of achieving documented riskassessment for all patients lies in anelectronic system. An example of theimpact that an electronic risk assessmentapproach can have is shown below. TheLondon Clinic, one of the National VTEExemplar Centres, introduced anelectronic system for risk assessment inQ2 2007; the risk assessment rates wentfrom about 30% to around 90% withinone year. The further advantage ofelectronic risk assessment is the enablingof simple audit of the patient numbers.
A National electronic risk assessment tool
At the national level, the Clinical SafetyTeam at NHS Connecting for Health iscontinuing to work on the developmentof electronic solutions to VTE riskassessment for hospitalised patients15.Work to develop a prototype VTE riskassessment tool is ongoing. A prototypetool was piloted at three NHS secondarycare locations. The pilot work is aimed attesting the utility of a VTE risk assessmentchecklist on mobile and hand-held digital equipment.
Last year, NHS Connecting for Healthidentified the long-term vision of astrategic end-to-end solution throughoutthe patient’s journey from primary care tosecondary care15. From the moment a GPreferral is sent via Choose and Bookinformation on the patient’s VTE riskcould be included and extracted by thehospital PAS. This might then populatethe VTE risk template and encourage riskassessment on admission. Throughout apatient’s hospital stay, staff would beassisted by a combination of VTEguidance, decision support embedded inthe PAS and electronic bed board displayand alerts. Medication record, dischargesummaries and VTE history could beautomatically populated from VTE clinicalinformation held in the patient record.Any assessments conducted during theirinpatient treatment could be sent back totheir GP. While this remains the goal,many Trusts are pressing ahead with localelectronic solutions to ensure the CQUINgoal of 90% risk assessment is achieved.
Introduce protocols that standardise VTErisk assessment and prophylaxis provision
Modifying the National risk assessment tool to local needs and linking VTE risk assessment
with NICE-compliant prophylaxis provision are common steps to ensure effective
thromboprophylaxis delivery. In the long term the answer to the challenges of achieving
documented risk assessment for all patients lies in an electronic system.
Fig 8Impact of electronic risk assessment on risk
assessment rates at the London Clinic .
100
80
60
40
20
0Q1 07 Q2 07 Q3 07 Q4 07 Q1 08 Q2 08

17
Veno
us Throm
boem
bolism Preve
ntion A
Guide
for D
elivering the CQUIN
Goa
l
Hospital no:
Surname:
First name:
DOB:
Case study
Modifying the National VTE risk assessment tool
The National risk assessment tool was modified at King’s College Hospital to integratethe elements of risk assessment with patient identification details, clinician responsibilityincluding signature, and a link from the VTE risk category to the local (NICE-compliant)guidelines for thromboprophylaxis. There is a general view that a separate riskassessment for obstetric patients is important. At King’s College Hospital, a unique riskassessment for obstetric patients is employed, incorporating essential elements of theDH risk assessment tool and the Green top guidelines (see resources section).
Completing risk assessment quickly in mobile medical admissions/short-stayobstetric cases
For medical patient admissions, only those judged to have a projected three days ofimmobility are at risk of VTE. A simple tick in the mobility box for a medical patient NOTexpected to have significantly reduced mobility relative to normal state completes therisk assessment. Frequently, pregnant women are admitted for several hours only andwould not be anticipated to be immobile for an extended period. It may be possible toagree a 'cohort' definition for risk assessment in such cases.
Fig 9Modified risk assessment tool at King’s College Hospital.
Fig 10Hospitalised medical patients are at risk of VTE if
expected to be immobile for 3 days or more.
Eliminate the need to retypethe risk assessment tool
Converting the National riskassessment tool from PDF toMicrosoft Word is simple. WithAdobe® Reader software, you canconvert a PDF document to a textfile and then edit directly. This willhelp you repurpose the existingtext and graphics for your localVTE risk assessment template.
Simply open the PDF, right-click onthe document, select copy andpaste into a word document. TheDH VTE risk assessment tool isavailable for download as a word document at http://www.kingsthrombosiscentre.org.uk
RISK ASSESSMENT FOR VENOUS THROMBOEMBOLISM (VTE)
Mobility – all patients (tick one box)
Tick Tick Tick
Surgical patient Medical patient expected to have ongoing reduced mobility relative to normal state
Medical patient NOT expected to have significantly reduced mobility relative to normal state
Assess for thrombosis and bleeding risk below Risk assessment now complete
Thrombosis risk
Patient related Tick Admission related Tick
Active cancer or cancer treatment Significantly reduced mobility for 3 days or more
Age > 60 Hip or knee replacement
Dehydration Hip fracture
Known thrombophilias Total anaesthetic + surgical time > 90 minutes
Obesity (BMI >30 kg/m2) Surgery involving pelvis or lower limb with a total anaesthetic + surgical time > 60 minutes
One or more significant medical comorbidities (eg heart disease;metabolic,endocrine or respiratory pathologies;acute infectious diseases; inflammatory conditions)
Acute surgical admission with inflammatory or intra-abdominal condition
Personal history or first-degree relative with a history of VTE
Critical care admission
Use of hormone replacement therapy Surgery with significant reduction in mobility
Use of oestrogen-containing contraceptive therapy
Varicose veins with phlebitis
Pregnancy or < 6 weeks post partum (see NICE guidance for specific risk factors)
Bleeding risk
Patient related Tick Admission related Tick
Active bleeding Neurosurgery, spinal surgery or eye surgery
Acquired bleeding disorders (such as acute liver failure) Other procedure with high bleeding risk
Concurrent use of anticoagulants known to increase the risk of bleeding (such as warfarin with INR >2)
Lumbar puncture/epidural/spinal anaesthesia expected within the next 12 hours
Acute stroke Lumbar puncture/epidural/spinal anaesthesia within the previous 4 hours
Thrombocytopaenia (platelets< 75x109/l)
Uncontrolled systolic hypertension (230/120 mmHg or higher)
Untreated inherited bleeding disorders (such as haemophilia and von Willebrand’s disease)
© Crown copyright 2010 301292 1p March 10

18
Develop a Trust-wide VTE prevention policy
First steps include forming a Trust-wideVTE prevention policy. There is greatvalue in piloting such a policy, seekingmultidisciplinary feedback and redraftingprotocols to perfect the policy. The policyshould be reviewed by all services andspecialties. Ensure widespreadagreement with the individual businessunits or directorates involved, e.g.emergency care, medicine, surgery.
VTE protocols are the base forlayered interventions
It is vital that VTE prevention protocols areproperly integrated into the clinicalworkflow and for most hospitals, thisremains a significant challenge. Ideal VTEprotocols that link the DH risk assessmenttool with NICE-compliant prophylaxisoptions and contraindications are theessential base for layered interventions,such as education and audit.
Small steps are important – ensure VTEprophylaxis guidance is available andeasily accessible to all healthcareprofessionals and present on all wardsand that the guidance is incorporated into protocols and within patient group
directions – but for most Trusts, this willnot be sufficient to ensure delivery of theVTE metrics required. VTE preventionprotocols are more likely to fail if keyprinciples for effective qualityimprovement are not followed. Theseprinciples have been identified by TheAgency for Healthcare Research andQuality (AHRQ) in the United States (seeinformation box)14.
Designing reliability into the VTE protocol
Estimates of the proportion of patientslikely to receive prophylaxis have beenmade in the United States, and a‘hierarchy of reliability’ has beencalculated based on the extent ofhospitals’ actions to implement a VTEprevention protocol (see figure 11). Thesefindings are valuable and suggest that
Embedding VTE prevention protocolsinto patient care
It is vital that VTE prevention protocols are properly integrated into the clinical workflow.
Ideal VTE protocols that link the National risk assessment tool with NICE-compliant prophylaxis
options and contraindications are the essential base for layered interventions, such as
education and audit. If the VTE protocol relies on traditional methods, such as stickers in drug
charts and stapling the risk assessment to the patient’s notes, it is likely that audit will show
disappointing results. VTE prevention protocols are more likely to fail if key principles for
effective quality improvement are not followed. Success requires quality improvement schemes
beyond protocol integration; developing roles for clinical support personnel and building in
system prompts and hard stops will help embed prevention strategies into routine patient care.
Predicted prophylaxis rate (%)Integration of VTE protocolLevel
1 No VTE protocol 40
2Decision support exists but not linked to
prescribing or prompts exist within prescribing but no decision support at hand
50
3 Protocol well-integrated into prescribing at point of care
65-85
4Protocol enhanced by other quality
improvement schemes and implementing high-reliability strategies
80-90
5 Oversights identified and addressed in real time
>95
Adapted from The Agency for Healthcare Research and Quality: Preventing Hospital-Acquired Venous Thromboembolism; A Guide for Effective Quality Improvement14. Fig 11
Hierarchy of reliability based on actionsto embed VTE prevention protocols.
19
Veno
us Throm
boem
bolism Preve
ntion A
Guide
for D
elivering the CQUIN
Goa
l
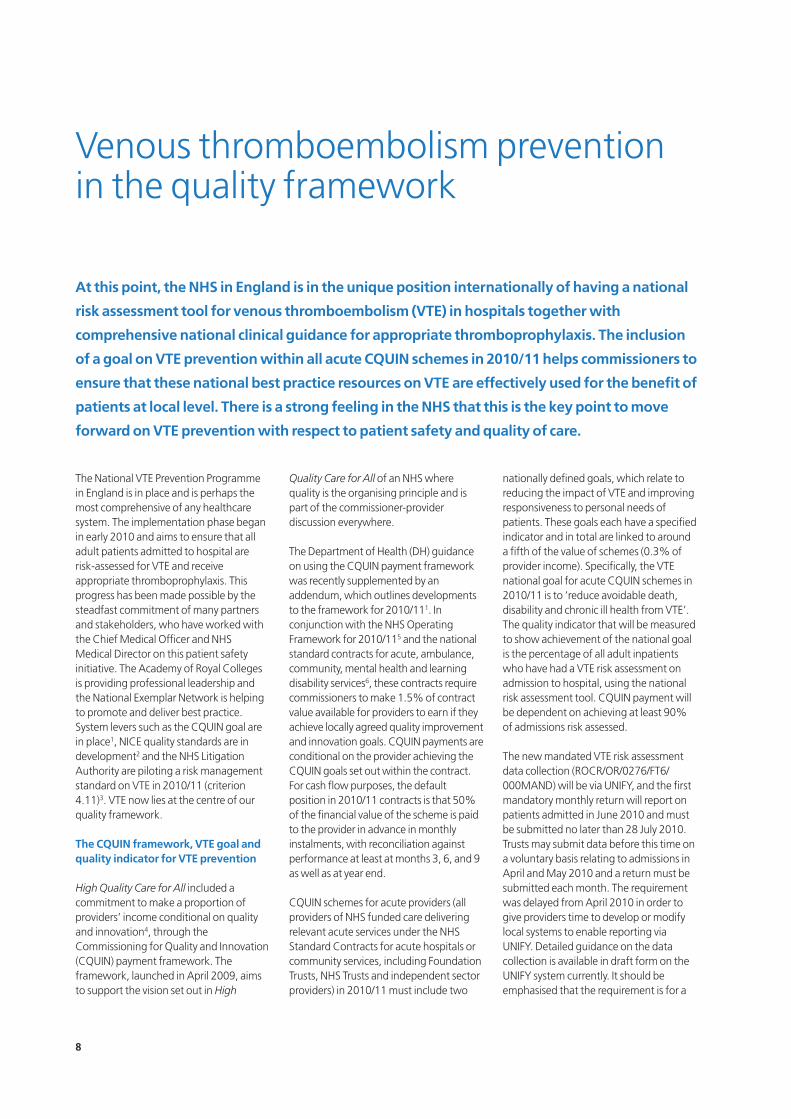
even for hospitals with VTE protocols well-integrated into prescribing at the point ofcare, the expectation is that the levels ofappropriate prophylaxis will not exceed85%. Only at level 4 (high-reliabilitymechanisms are in place to make it a rareevent for a patient to enter the hospitalwithout going through a VTE protocol,where any variations from the protocol oradverse effects while on the protocol arestudied in depth, where the protocol andits integration are continually refined andits use is continually increased based onthese events, using the collectiveintelligence, experience, and investigationof the institution) can the levels ofappropriate prophylaxis required bedelivered. Successful level 5 reliability, with appropriate prophylaxis rates of>95% found on audit, is only within reach of hospitals with electronicmedication records.
Drug chart integration of VTE riskassessment and prophylaxis provision
Many Trusts are now incorporating VTE risk assessment and prophylaxismeasures into their local hospital drugchart, using stickers or designing newcharts with VTE parameters included. The idea that VTE prevention shouldform part of a standard hospital drugchart has been given credence by TheAcademy of Medical Royal Colleges, whohave called for the introduction of astandard hospital drug chart to helpTrusts meet the demands to prevent VTE.The Academy has suggested that thepresence of VTE prophylaxis on everychart would be an important incentive torisk assessment and appropriateprophylactic drug provision.
Drug chart integration of the VTEprotocol can be linked to a Trust's VTEprevention policy, for example byforbidding any prescribing until VTE riskassessment has been completed.
Key principles for effective quality improvement interventions
1. Keep it simple
The trade-off between detail and simplicity in VTE protocols and required actions should tend towards simplicity.
2. Make your objectives SMART (Specific, Measurable, Achievable, Realistic, and Timetabled)
These criteria may be used both to set and assess objectives and act as a checklist toassure quality.
3. Do not interrupt workflow
Ensure the VTE protocols are easy to use, discouraging free text and incorporatingsimple steps to allow prescribing e.g. signature boxes to approve prophylaxis.Incorporate the protocols into routine patient care.
4. Design reliability into the process
If the VTE protocol relies on traditional methods, such as stickers in drug charts andstapling the risk assessment to the patient’s notes, it is likely that audit will showdisappointing results. It is accepted that these traditional methods of improving VTEprotocol uptake and adherence are helpful, but will not produce the required levels ofrisk assessment and prophylaxis provision that are required to fulfil the requirements ofthe National VTE Prevention Programme. In order to improve reliability, adhering to theVTE protocol should be linked to at least one of the following:
- The default action (i.e., not doing the desired action requires opting out)
- Prompted by a reminder or a decision aide
- Standardised into a process (i.e., deviation from the protocol feels wrong)
- Scheduled to occur at known intervals
- Responsibilities for desired action are redundant
5. Pilot on a small scale
Embedding the protocol should be piloted by physicians, pharmacists and nurses, and revised accordingly.
6. Monitor use of the protocol
The VTE protocol must become part of the admission process for every patient admittedto the hospital. When audit shows that the protocol has not been followed, a detailedreview should identify which types of admissions are by-passing the protocol and tailorthe process to eliminate these omissions.
Adapted from The Agency for Healthcare Research and Quality: Preventing Hospital-Acquired Venous Thromboembolism; A Guide for Effective Quality Improvement14.

20
Quality improvement schemes -clinical support staff
At the King’s Thrombosis Centre, nurseshave been in the front line of the VTEprevention initiative. The major qualityinitiatives have been the development ofa nursing care plan to ensure a systematicapproach to VTE prevention and thedevelopment of clinical nurse specialists,a consultant nurse role and the creationof VTE Link Nurses, who have takenownership of the process on the wardsand are embedding VTE prevention intoroutine patient care.
The Coagulation Link Nurse role wasestablished to work with the ThrombosisTeam to promote evidence-basedpractice and embed VTE preventionprotocols throughout the Trust. The roleof the Link Nurse is to act as a resource intheir clinical area and to liaise with theThrombosis Team. The Link Nurse role isto improve the quality of care, educationof staff and patients and improvecommunication between the ward andthe service. Each Link Nurse is providedwith a badge to identify them to theirteam and patients. The nurse agrees totake on the responsibilities of the role,which are defined as:
- To liaise between their clinical area andthe specified team
- To liaise with the nurse in charge of theclinical area with regard to the
implementation of team policies andprocedures
- To participate in teaching staffappropriate aspects of care relating tothe specified area
- To act as a visible resource for both staffand patients
- To commit to attend Link Nursemeetings monthly and undertake anyeducation required
System prompts and ‘hard stops’ forVTE prevention
Electronic patient record systems allowfor simple reminder boxes to appear toinfluence physician behaviour, to allowoversights to be identified and addressedin real time. These allow the introductionof hard stops, blocking prescribing untilthe VTE risk assessment has beenrecorded, and in cases of patients at risk,using electronic prompts to consider
prescribing of prophylaxis and to blockfurther prescribing until the prophylaxisquestion is addressed.
Linking VTE risk assessment to routineblood test requests is another route toimprove integration. For example,doctors can be prompted to completethe VTE risk assessment on admissionand 24 hours after admission and thecompletion of risk assessment linkedwith requests for routine bloods, toensure that the VTE risk assessment iscompleted on time.
Commissioning for VTE prevention
The CQUIN goal and the providercontracts for 2010 present profoundopportunities to improve quality andpatient safety by embodying the keyissues and standards with respect to VTEprevention in a formally agreed and
Case studies
At the Whittington Hospital, a 5-hospital collaboration on a new drug chart has resulted inthe addition of thromboprophylaxis risk stratification on the front page and theintroduction of a prescribing section specifically for thromboprophylaxis on the 3rd page.
At the HomertonHospital, pre-printedstickers with differentdoses of low-molecular-weightheparin andcompressionstockings are availableas additions to thecurrent drug chart. A new drug chart has
been developed and will be deployed shortly with the different forms of VTE prophylaxisalready pre-prescribed, with a signature only required to initiate treatment. There isongoing development of electronic prescribing to help fulfil the VTE prevention goals.
Fig 12 Modified drug chart incorporating VTE at the Whittington Hospital.
Fig 13 Developing a nurse consultant role for thrombosis has
been successful at King’s College Hospital.
Fig 14 Electronic prompts to consider prescribing of prophylaxis
can act as hard stops to ensure protocol compliance.

documented national preventionprogramme. All Trusts must now reportto their lead commissioner on local auditsof the percentage of patients risk-assessed for VTE who receive theappropriate prophylaxis, and undertakeroot cause analysis of all confirmed casesof hospital-acquired PE and DVT(including those arising from a currentstay or new events arising where there isa history of admission to hospital withinthe last three months). In this context,
commissioning for VTE preventionrequires a whole-system approach.EoE NHS has developed an SHA-wideVTE view, with world classcommissioning and stakeholderengagement key components of thevision. The project was initiated in 2009under the ‘Towards the best, together’vision and meeting the sixth pledge inImproving Lives; Saving Lives: “We willmake our health service the safest inEngland.” The project is leading the way
for the region to implement best practiceand provide health professionals with theskills to implement these measures.
Understanding the idiosyncrasies of thelocal health economy within the nationaland international context, utilising awide variety of skills and influences andbringing a range of stakeholders onboard are all necessary to ensure all Trustsmove to at least level 4 integration of VTEprotocols into patient care.
21
Veno
us Throm
boem
bolism Preve
ntion A
Guide
for D
elivering the CQUIN
Goa
lNational DataLocal information
MediaAffiliates
Current pathwaysNew drugs
Stand aloneLink to other initiatives
Evaluation of initiativesNew opportunities
AuditTrajectories
Root Cause AnalysesMedicines Management
CliniciansPatientsCarers
CitizensNHS Boards
CliniciansPatientsCarersTrust Boards & ManagersPractice Based Commissioners
Contracts
Practice Based CommissioningMap of Medicine
Primary Care
Secondary CarePatient
NPSABMA Learning
Risk AssessmentDischarge arrangementsFollow up arrangements
PROMsProject Management
Needs Assessment
Quality Improvement
R&D
Governance
Marketing
SUSHospitals’own
PRMISQoFReferral Data
CommissioningVTE
Education
Information
Existing Exemplars: Colchester Hospital, James Paget
Tertiary education engagement - VTE in undergraduate courses
Nurse Led-Doctor Complete systemLook Back Programme, Primary - Secondary care
Application of CQUIN to trusts, QIPP, Clinical Governance, CQC
Compliance/Quality/Clinical Governance(Operational - Performance Management)
World Class Commissioning
Education & Training
ExemplarTrusts
NHSEast of
England
Systems, Improvement, Best Practice
Communications & StakeholderEngagement
Awareness campaigns - Stop the Clot campaign 2010, Stakeholder engagement events,Third party/Charity engagement, Patient/carer involvement and experience
World Class Commissioning, commissioning framework, NHS Operating framework 2010/11
Other health professionals e.g. pharmacists
Future EoE Exemplar sites
Working towards application for exemplar status
University of HertfordshireVTE education courses
Regional best practice, E-risk assessment tool, Gateway system, drug charts
Trust reporting to SHA, Audits, NICE Guidance
PCT-CQUIN,Quality accounts
Networking eventsfor acute trusts, PCTS
Fig 16 The East of England NHS has developeda VTE package to work towards.
Fig 15 Mind map issues to consider whencommissioning for VTE prevention.

22
Collecting the numerator of theCQUIN goal
The general goal of VTE risk assessmentfor all patients has now been transformedinto a metric-specific aim statement, withthe process measure defined as 90% riskassessment of all in-patients. Simple auditis not sufficient to ensure this metric isdelivered, as continuous census of the VTEgoal is necessary to fulfil the CQUINtarget. This represents a difficult challengeto Trusts – ensuring reliable data collectionis a key issue that must be addressed inevery Trust. While the total hospitaladmissions will be available centrally inthe Trust (denominator), the challengeremains collating the patient riskassessment data (numerator) from many disparate sources.
Electronic records greatly simplify theprocess of establishing the numerator. In Trusts with electronic patient records,VTE risk assessment can be integrated intothe record and the census conductedthrough retrospective data retrieval (seecase study). In Trusts with website accesson the ward, or using paper-based riskassessment, development of a web-basedrisk assessment tool greatly simplifies thedata collation. Risk assessments can beconducted online, or completed on a hardcopy template and entered online by dataentry clerks later, with the websitedatabase allowing upload directly toUNIFY. Such a system is in development at Colchester Hospital.
For hospitals that operate electronicdischarge systems, the addition of a tickbox on the summary to indicate that VTErisk assessment has been completed maysimplify the process of tracking risk
assessment, and in addition offer anopportunity to work towards NICEcompliance with regard to extendedthromboprophylaxis. Making aspects ofthe discharge summary compulsory, such
Ensuring reliable data collection andperformance tracking
Ensuring reliable data collection is a key issue that must be addressed in every Trust. For
CQUIN, the total hospital admissions will be available centrally in the Trust (denominator),
but the challenge will be collating the numerator from many disparate sources. Electronic
approaches, using electronic patient records or web-based databases can greatly simplify the
process. Appropriate prophylaxis and root cause analysis audits are required now; in the near
future, audits to fulfil the requirements of the NICE quality standard for VTE will be sought.
Case study
Colchester Hospital University NHS Foundation Trust was designated as a National VTEExemplar Centre in 2009. Among the measures taken by the Trust, one of the mostexciting and innovative is the development of an online risk assessment tool to identifypatients at risk of VTE, which also offers guidance on the steps that should be taken tominimise the risk and includes a database which will directly upload risk assessmentdata onto UNIFY. This new tool is being developed for the EoE SHA through their VTEPrevention Steering Committee. The new tool will be trialled from June and has thefollowing functions:
- Risk assess for all inpatient scenarioscompliant with the DH riskassessment tool
- Record the hospital and date of riskassessment
- Record bleeding risks,contraindications to pharmacologicaland mechanical VTE prophylaxis
- Calculate VTE risk of patient
- Recommend VTE prophylaxis forpatient with care pathways foreducation
- Printout the risk assessment form with all details on one A4 page for attachment todrug chart for doctors' signature, prescription, delivery of prophylaxis and audit
- Record on a central secure database for each Hospital/Trust each risk assessment onadmission, at 24 hrs, and after 48hrs, and also anti-embolism stockings fitted andpatient information leaflets provided to patients
- Production of monthly data for UNIFY
Fig 17 Web-based risk assessment and auditsite developed by Colchester Hospital.

23
Veno
us Throm
boem
bolism Preve
ntion A
Guide
for D
elivering the CQUIN
Goa
l
as the record of VTE risk assessment, andforcing completion of that section beforedischarge, will contribute to accuratemeasurement of the risk assessmentmetric. The addition of details of out-of-hospital thromboprophylaxis will support improvements in the transition of care to GPs.
VTE prophylaxis audit
Although data for the CQUIN indicatorwill be gathered via monthly UNIFY data collection, the evidence aroundappropriate prophylaxis and root causeanalysis of VTE will be from clinical audit.Clinical audit of VTE prevention is now acompulsory aspect of the NHS standardcontract and local audits of VTEprevention measures, in particularappropriate prophylaxis, are required. By early July 2010, the NICE qualitystandard for VTE will be published andthis will introduce further auditrequirements, including reassessment ofrisk after 24 hours and the provision ofpatient information on VTE prevention.
The NICE guidelines provide an audittemplate as part of the audit support
tools for monitoring local practice, whichcan be accessed on the NICE website.NICE recommends using the whole toolor cutting and pasting the relevant partsinto a local audit template. Data may berequired from a range of sources,including policy documents and patientrecords. Suggestions for data sources areindicated on the tools, but most datashould be available from patient records.
VTE prophylaxis performance dashboards
Performance tracking throughdashboards is a commonly usedmanagement tool to gauge performanceand progress toward agreed goals andare particularly suitable to inform Trustsof their performance on VTE preventionmetrics. Using monthly reports, thehighest performing units can beidentified and praised, and those failingto achieve agreed goals identified clearlyto the rest of the Trust. This can contributeto overcoming lack of awareness andapathy issues. Identifying those units notachieving the required goals allows adetailed analysis in those particular unitsof the reasons for the failing, such as a
Case study
At Guy’s and St Thomas’ NHSFoundation Trust, five Electronic PatientRecord (EPR)-based VTE risk assessmenttools have been developed to facilitatedocumentation of patient-specific VTErisk assessment and retrospectiveretrieval for audit purposes. These arefor medical, stroke, surgical,orthopaedic and obstetric patientgroups. These EPR tools have beenadapted from the National VTE riskassessment tool.
The VTE risk assessment tool includes aclinical summary of the Trust’sthromboprophylaxis guidelines and amandatory field for documenting theoutcome of the VTE risk assessment.The outcome of the VTE risk assessmentincludes whether mechanical orpharmacological thromboprophylaxis is indicated and prescribed and if so,which pharmacological agent /mechanical method ofthromboprophylaxis is chosen.
The tools also record cases whenthromboprophylaxis is not indicated atthe time of the VTE risk assessment andthe reason why. This includes patientson treatment doses of heparin/oralanticoagulant therapy at the time of theVTE risk assessment and for whomthromboprophylaxis is contra-indicated.
Fig 18 Electronic Patient Record (EPR)-based VTE risk
assessment at Guy’s and St Thomas’ Trust.
Case studies
At the Whittington Hospital, continuous re-audit findings are published in the formof a performance dashboard. The audits have revealed problems amongst doctorsand nurses regarding clear lines of responsibility regarding VTE prevention, and thishas resulted in a plan to create work-flow diagrams to show where responsibilitylies during a patient’s journey through the hospital.
At King’s College Hospital, audit objectives that were appropriate and wouldproduce meaningful results were identified with the Trust Clinical Auditdepartment. Junior doctors joined link nurses and the Thrombosis Team to conductaudits. Data collection sheets were designed and spreadsheets used to collate thedata. Juniors accompanied more experienced auditors and places on the Universityof Hertfordshire Thromboprophylaxis course were secured for VTE Link Nurses toimprove their audit skills. Relevant wards and clinicians were made aware thatregular audits on VTE prevention metrics were being performed. The results werefed back to the relevant stakeholders and recorded on the Trust Clinical Scorecard.

24
lack of clarity regarding responsibility torisk assess, or unusual patient journeysthrough the hospital system resulting inopportunities to risk assess and prescribeprophylaxis being missed.
Balancing measures
An important consideration after majorsystem changes is the monitoring ofunintended consequences. It isimportant side-effects of the increase inprophylaxis provisions are also monitoredand formally audited. This is especiallythe case for bleeding episodes. TheExemplar Centre Network has initiated apilot study to monitor anticoagulant-related adverse events.
Root cause analysis of hospital-acquired VTE
Undertaking root cause analysis of everycase of hospital-acquired VTE (patientswho have had VTE relating tohospitalisation, including those whoseclot was first discovered during thecourse of hospitalisation and in the threemonths subsequent to discharge) is amajor challenge, which requires firstlycapturing the cases, undertaking theanalysis, notifying the stakeholders andfeeding the learning back into the Trustquality management framework.
A local process should be developed toensure that all cases of VTE that couldpotentially be regarded as hospitalacquired are identified. It should benoted that in cases of recenthospitalisation in a different Trust, theroot cause analysis should be conductedin the Trust in which the patient presentswith VTE.
Clinical coding and VTE
The ICD-10 coding system is nationallyand internationally recognised and playsan important role in hospitaladministrative data, but does not alloweasy identification of VTE. The diagnosiscodes that identify patients with VTEinclude: I26.0–I26.9, O88.2 for PE andI80.1–I80.9, I82.1, I82.8, I82.9, O22.3,O22.9, and O87.1 for DVT. In the UnitedStates, the AHRQ have launched qualitymeasurement, quality improvement, andpay-for-performance initiatives that
require identification of patients withacute VTE using a set of specific ICD-9-CM codes in hospital discharge records16.In England, DH are exploring aggregationof existing ICD codes for VTE into threegroups – acute VTE, chronic VTE andhospital-acquired VTE – to improve theutility of coding in the evaluation of theNational VTE Prevention Programme.
Use of ICD-10 codes to track cases of VTE should be discussed and agreedbeforehand within your Trust. It isimportant to realise that Trust clinicalcoders code for morbidity purposes.Mortality coding via death certificates is performed by the Office of NationalStatistics. Coding accuracy is critical toallow proper identification of VTE; threelevels of coding must be followed:
1. Individual codes - each clinicalstatement of diagnosis must have thecorrect code assignment
2. Totality of codes - all codes necessarymust be used to give an accurateclinical picture of the patient’s stay in hospital
3. Sequencing of codes - organised in aspecific sequence which follows therules and conventions of theclassification
National benchmarking: estimates ofhospital-acquired VTE
There are limited data on estimates ofhospital-acquired VTE in England andWales at present. Although it is widelyaccepted from post-mortem data thatVTE causes many thousands ofpotentially preventable deaths, it is achallenge to more precisely define theoverall burden of hospital-acquired VTE. In the United States, screening ICD codesfor VTE in residents from the Worcestermetropolitan area revealed that 36.8%
of outpatients presenting with VTE hadbeen hospitalised in the preceding 3months, half for medical reasons and half to undergo surgery during thehospitalisation17. These general numbers – somewhere between a thirdand a half of VTE events being linked tohospitalisation and medical reasons asimportant as surgical reasons – are widely accepted.
Systematic prevention of VTE is a keypriority for the EoE Clinical ProgrammeBoard on Patient Safety. To calculate thepotential for preventing VTE, an extract ofHospital Episode Statistics data for 2007–09 was analysed and the National VTE riskassessment model applied. This analysisshowed 2235 VTE admissions in theregion each year, and 385,000 admissionsof high-risk patients. On average, 5.8(range: 4.2 to 7.8) per 1000 at-riskpatients were diagnosed with VTE inhospital or within eight weeks followingadmission. This is in line with recentepidemiological studies, but variesconsiderably by hospital (see figure 20).Using estimates that 40% of at-riskpatients receive appropriate prophylaxisand that prophylaxis reduces VTE risk by50%, VTE occurs in EoE at a rate of 7.25per 1000 high risk patients not receivingprophylaxis, and at 3.63 per 1000 high riskpatients receiving prophylaxis. Increasingprophylaxis rates to 80% would preventup to 560 VTE events each year.
North Lancashire Teaching Primary CareTrust reviewed the same period 2007–09and found 3185 patients admitted with a primary diagnosis of VTE. Of these,around half had stayed in the hospital inthe previous 90 days. The VERITY registryreviewed 1919 patients with confirmedVTE and found that around a fifth did notseem to have an obvious risk for VTE.These figures suggest that in a largeteaching Trust like Lancashire, there are
Case study
The clinical statement ‘Deep vein thrombosis in pregnancy’ would be coded as Index entry:Thrombosis - pregnancy- - deep-vein O22.3
O22.3 Deep phlebothrombosis in pregnancy
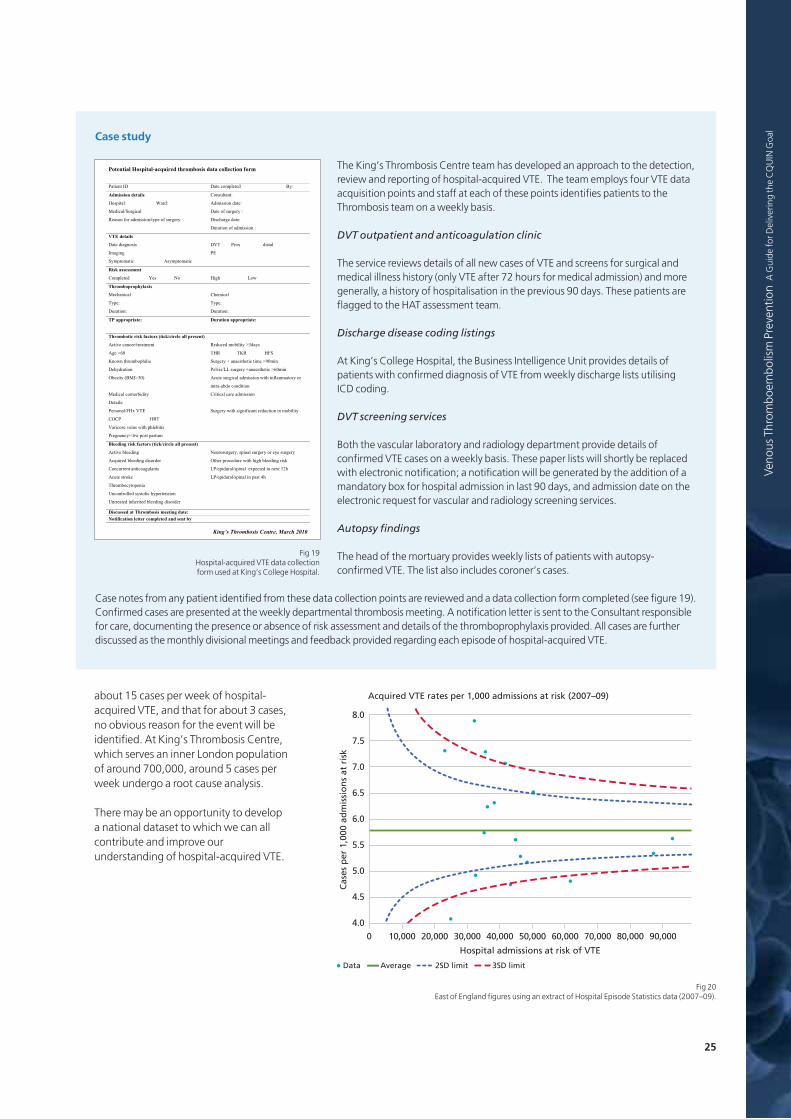
25
Veno
us Throm
boem
bolism Preve
ntion A
Guide
for D
elivering the CQUIN
Goa
l
about 15 cases per week of hospital-acquired VTE, and that for about 3 cases,no obvious reason for the event will beidentified. At King’s Thrombosis Centre,which serves an inner London populationof around 700,000, around 5 cases perweek undergo a root cause analysis.
There may be an opportunity to developa national dataset to which we can allcontribute and improve ourunderstanding of hospital-acquired VTE.
Case study
The King’s Thrombosis Centre team has developed an approach to the detection,review and reporting of hospital-acquired VTE. The team employs four VTE dataacquisition points and staff at each of these points identifies patients to theThrombosis team on a weekly basis.
DVT outpatient and anticoagulation clinic
The service reviews details of all new cases of VTE and screens for surgical andmedical illness history (only VTE after 72 hours for medical admission) and moregenerally, a history of hospitalisation in the previous 90 days. These patients areflagged to the HAT assessment team.
Discharge disease coding listings
At King’s College Hospital, the Business Intelligence Unit provides details ofpatients with confirmed diagnosis of VTE from weekly discharge lists utilising ICD coding.
DVT screening services
Both the vascular laboratory and radiology department provide details ofconfirmed VTE cases on a weekly basis. These paper lists will shortly be replacedwith electronic notification; a notification will be generated by the addition of amandatory box for hospital admission in last 90 days, and admission date on theelectronic request for vascular and radiology screening services.
Autopsy findings
The head of the mortuary provides weekly lists of patients with autopsy-confirmed VTE. The list also includes coroner’s cases.
Case notes from any patient identified from these data collection points are reviewed and a data collection form completed (see figure 19).Confirmed cases are presented at the weekly departmental thrombosis meeting. A notification letter is sent to the Consultant responsiblefor care, documenting the presence or absence of risk assessment and details of the thromboprophylaxis provided. All cases are furtherdiscussed as the monthly divisional meetings and feedback provided regarding each episode of hospital-acquired VTE.
Potential Hospital-acquired thrombosis data collection form
King’s Thrombosis Centre, March 2010
Patient ID Date completed By:
Admission details
Hospital: Ward:
Medical/Surgical
Reason for admission/type of surgery
Consultant:
Admission date:
Date of surgery :
Discharge date:
Duration of admission :
VTE details
Date diagnosis
Imaging
Symptomatic Asymptomatic
DVT Prox distal
PE
Risk assessment
Completed Yes No High Low
Thromboprophylaxis
Mechanical
Type:
Duration:
Chemical
Type:
Duration:
TP appropriate: Duration appropriate:
Thrombotic risk factors (tick/circle all present)
syad3> ytilibom decudeR tnemtaert/recnac evitcA
Age >60 THR TKR HFS
m09> emit citehtseana + yregruS ailihpobmorht nwonK in
nim06> citehtseana+ yregrus LL/sivleP noitardyheD
lfni htiw noissimda lacigrus etucA )03>IMB( ytisebO ammatory or
intra-abdo condition
Medical comorbidity
Details:
Critical care admission
noitcuder tnacifingis htiw yregruS ETV xHF/lanosreP in mobility
TRH PCOC
Varicose veins with phlebitis
Pregnancy/<6w post partum
Bleeding risk factors (tick/circle all present)
eye ro yregrus lanips ,yregrusorueN gnideelb evitcA surgery
Acquired bleeding disorder Other procedure with high bleeding risk
cepxe lanips/larudipe/PL stnalugaocitna tnerrucnoC ted in next 12h
h4 tsap ni lanips/larudipe/PL ekorts etucA
ainepotycobmorhT
Uncontrolled systolic hypertension
Untreated inherited bleeding disorder
Discussed at Thrombosis meeting date: Notification letter completed and sent by
Fig 19 Hospital-acquired VTE data collectionform used at King’s College Hospital.
Hospital admissions at risk of VTE
0 10,000 20,000 30,000 40,000 50,000 60,000 70,000 80,000 90,000
8.0
7.5
7.0
6.5
6.0
5.5
5.0
4.5
4.0
Acquired VTE rates per 1,000 admissions at risk (2007–09)
Cas
es p
er 1
,000
ad
mis
sio
ns
at r
isk
Data Average 2SD limit 3SD limit
Fig 20 East of England figures using an extract of Hospital Episode Statistics data (2007–09).

26
Ongoing professional training and education
All clinical staff should receivetraining on the Trust’s policy on VTEprevention; this should bemandatory, and monitored by theappropriate body in the Trust. Acommon complaint is the difficultyengaging with junior medical staff in the VTE dialogue. Introducing F1 and F2teaching sessions on VTE and buildingVTE prevention into the inductionprocess are valuable steps to consider.The e-VTE course developed by e-Learning for Healthcare through theDH will be extended to include a shorterinduction-orientated module on VTEprevention and Trusts are consideringmaking this a compulsory component ofthe induction training.
Many Trusts have created simple, colour-coded pocket guides on the preventionand treatment of VTE for easy referencefor healthcare professionals, and areparticularly suitable for junior doctors touse as referral guides. Internalcommunication channels should beutilised to ensure ongoing exchange ofideas and feedback.
Grand rounds
Grand rounds afford an idealenvironment to provide an integratedreview of the VTE prevention process,from evidence, Government policy
through to localprevention polices. These events areparticularly suitable to emphasise thechanging environment of VTEprevention, including the introduction ofthe CQUIN goal, the NICE guidelines andthe national approach top prevention.
Leadership walk-rounds
Another approach, successfullyemployed at Portsmouth Hospital andKing's College Hospital, is the use ofweekly patient safety leadership walk-rounds; the presence of senior trust staffensures that frontline staff are aware oftheir organisation’s commitment to VTE
prevention and afford an excellent and informal method for leaders to exchangeviews with front-line staff about VTEissues in the organisation and show theirsupport for staff-reported suggestionsfor improvement. Such events, linked todaily safety briefings on the ward, ensurethe culture of VTE prevention becomesfirmly embedded.
Ensuring educational programmes arecreated to support the protocols
Multidisciplinary ward rounds, leadership walk-rounds, and grand rounds tied to education
programmes backed by quality educational materials lie at the heart of ensuring the policies
and practices to support VTE prevention are supported. Furthermore, engaging with
patients and offering verbal and written information on VTE prevention, which itself is part
of the NICE quality standard, is required to ensure VTE prevention is addressed on both sides
of the doctor-patient relationship.
Fig 21VTE prevention leaflet atKing’s College Hospital.

27
Veno
us Throm
boem
bolism Preve
ntion A
Guide
for D
elivering the CQUIN
Goa
l
Educational evenings and competitions
Educational events directed towards thekey Trust personnel driving VTEprevention such as nurses, junior doctorsand pharmacists, are important to ensurea sense of camaraderie and team work.Asking the attendees to create andpresent materials, for example posters onVTE prevention and awarding prizes,ensures engagement and self-education.
Engaging the patient
Patient education about VTE forms a keypart of the NICE VTE quality statements.These suggest that patients/carers areoffered verbal and written information onVTE prevention at time of admission anddischarge. Most centres have developedpatient information leaflets and encouragethe nursing staff to discreetly counselpatients found to be at risk of VTE, therecommendations for prevention measuresand the signs and symptoms to watch for.
St George's Healthcare NHS Trust will use a modified risk assessment tool thatincludes a patient information leaflet. Themodified tool includes a signature sectionfor prescribers indicating that riskassessment has been completed, allowsmultiple instances of risk assessment to berecorded and provides a patientinformation leaflet, which is perforatedand can be detached to give to the patient.
Northwest London Hospitals NHS Trust isplanning to adapt the ‘Lifeblood’thrombosis charity’s patient informationleaflet and to make this available on allwards, outpatient areas and pharmacy.The ‘Lifeblood’ patient informationleaflet is available to download at:http://www.thrombosis-charity.org.uk/cms/images/stories/File/ leaflets/Preventing_a_blood_clot_when_in_hospital.pdf
Case study
Colchester Hospital University NHS Foundation Trust was awarded “exemplarcentre” status in 2009. E-learning for VTE is an integral part of the overall VTEprevention approach taken at the Trust.
Among the measures being taken by the Trust are:
- Development of a protocol in conjunction with its consultants and pharmacystaff in line with NICE guidance and the DH recommendations
- An e-learning tool for doctors and nurses who treat hospital inpatients
- Development of an online risk assessment tool to identify patients at risk of VTEand which also offers guidance on the steps that should be taken to minimise it
- The use of the Trust's clinical audit department to evaluate and report back onthe work to prevent VTE.
The ‘Nurse-Led-Doctors-Complete’ VTE risk assessment system was developed aspart of a new programme set up to tackle the difficulties of achieving goodcompliance levels in VTE prophylaxis. It is part of a programme that includes newTrust-wide VTE protocols, eVTE learning, pre-printed drug chart stickers, onlinerisk assessment, and audication (rolling audit with immediate educationalfeedback and emailed league tables for specialities and wards).
In today’s NHS, nurses are a constant presence on inpatient wards andunfortunately junior doctors are not. Hence the ‘Nurse-Led-Doctors-Complete’VTE risk assessment system allows senior nurses to maintain compliance levels ofVTE risk assessment and therefore prophylaxis. The nurses, once eVTE trained,notify junior doctors of missing risk assessments and ask them to complete the riskassessment form (online or on paper). The risk assessment forms are stapled todrug charts for ease of recognition and audit purposes. Once the risk assessmentform has been completed, thromboprophylaxis can be given by nurses, and thepatient is permitted to leave the ward for investigation or intervention.
Risk assessment and thromboprophylaxis is also checked on the pre-operativeWHO checklist and surgery cannot proceed without them. If junior doctors are notavailable and a potential delay in patient care may arise, then senior eVTE-trainednurses can risk assess, but at present doctors must still check and sign the riskassessment forms. In the future, Colchester aims to allow DVT prevention nursesand ward nurse leads for patient safety to risk assess and prescribe.
Looking to the future, audits to fulfil the requirements of the NICE quality standardfor VTE on patient information will be facilitated by the introduction of the newonline risk assessment tool. This will record on a central secure database for eachHospital/Trust each risk assessment on admission, at 24 hrs, and after 48hrs, andalso allow a record of the supply of patient information leaflets.

28
I had the privilege of delivering
the The Dr. Sol Sherry Memorial
Lecture at the International Society
on Thrombosis and Haemostasis
conference in Boston in 2009. In
that lecture, I extolled the virtues
of high-quality clinical practice
guidelines in the field of VTE
prevention.
Guidelines are helpful because
they summarise an extensive and
sometimes complex literature
and provide evidence-based
recommendations that can be
broadly applied. But I also pointed
out that even excellent guidelines
do not improve patient safety
unless incorporated into clinical
practice. At the national or system-
wide level, a number of countries
have created incentives or
legislation to induce hospitals to
implement patient safety practices
related to VTE. At that point,
England had both a national risk
assessment tool and a national
guideline, but audits continued to
show poor implementation with
low levels of risk assessment and
inconsistent thromboprophylaxis
provision. The next steps taken in
England that are outlined in this
book – a national mandatory data
collection of VTE risk assessment
linked to a specific national goal
with financial penalties for failure,
modification of hospitals’
contracts of acute care delivery to
include prophylaxis audit, and a
root cause analysis of any VTE
event related to hospitalisation –
transform the VTE prevention
agenda and it is now more
comprehensive than any such
national initiative in the world.
It is only when VTE risk assessment
and prophylaxis prescribing are
incorporated into the culture of
routine care that every
hospitalised patient will receive
thromboprophylaxis that is
appropriate to their
thromboembolic and bleeding risk.
This resource book provides
important insights into the local
approaches that are being taken in
English hospitals to deliver this most
important of safety interventions
for hospitalised patients.
Prevention of venous thromboembolism:delivering this key patient safety priority
BIOGRAPHY
Dr. William H. Geerts isProfessor of Medicine at theUniversity of Toronto in
Canada. He is also Director of theThromboembolism Program atSunnybrook Health Sciences Centre inToronto. His clinical practice isrestricted to venous thromboembolismand his research interests involve thediagnosis, treatment, and preventionof thromboembolic disease, as well asguideline implementation and qualityof care improvement.
For the past ten years, he has beenchair of the Prevention of VenousThromboembolism section of theACCP Guidelines on AntithromboticTherapy. He is currently the leader ofthe Safer Healthcare Now! initiative to improve the use ofthromboprophylaxis across Canada.Dr. Geerts chairs the sciencecommittee for the Venous DiseaseCoalition.
Both individual physicians and health care systems have responsibilities to provide
thromboprophylaxis, the highest ranked patient safety intervention for hospitalised
patients. The National VTE Prevention Programme in England delivers a framework that
ensures the NHS now has an integrated approach with financial incentives to deliver this
key patient safety priority.

Resource Centre

30
September 2008
CMO letter announcingthe publication of theNational VTE RiskAssessment Template
2008 2009
November 2008
VTE Exemplar Centreand web resource site launch
November 2008
Publication of Map of Medicine VTEprevention pathway
June 2009
National NHS VTEleadership summit
June 2009
e-VTE website
September 2008
Department of HealthNational VTE RiskAssessment Template
April 2007
National Institute for Health and ClinicalExcellence (NICE) ClinicalGuidelines - Venousthromboembolism:reducing the risk of venous thromboembolism(deep vein thrombosis and pulmonary embolism) in inpatients undergoing surgery
January 2009
WHO surgical checklist
For the developmenttimeline from 2005-07please refer to the VTEresource book, VenousThromboembolism: APatient Safety Priority
Development timeline of the NationalVenous Thromboembolism PreventionProgramme in England

31
Veno
us Throm
boem
bolism Preve
ntion A
Guide
for D
elivering the CQUIN
Goa
l
2010
June 2010
VTE Exemplar CentreNetwork increases to16 centres
June 2010
Update of Map ofMedicine VTEprevention pathway
January 2010
NICE Clinical Guideline 92 –Reducing the risk of venousthromboembolism (deepvein thrombosis andpulmonary embolism) inpatients admitted to hospital
Issue date: January 2010
NICE clinical guideline 92Developed by the National Collaborating Centre for Acute and Chronic Conditions
Venous thromboembolism: reducing the riskReducing the risk of venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to hospital
This guideline updates NICE clinical guideline 46 and replaces it
January 2010
NHS Operating Frameworkspecifies VTE prevention as anational CQUIN goal
the operating framework. for the NHS in England 2010/11
Productive • High Quality • Preventative • Innovative • Productive • High Q High Quality • Preventative • Innovative • Productive • High Quality • Prev Preventative • Innovative • Productive • High Quality • Preventative • Inno • Innovative • Productive • High Quality • Preventative • Innovative • Prod Preventative • Innovative • Productive • High Quality • Preventative • Inno igh Quality • Preventative • Innovative • Productive • High Quality • Preven Productive • High Quality • Preventative • Innovative • Productive • High Q • Innovative • Productive • High Quality • Preventative • Innovative • Prod Preventative • Innovative • Productive • High Quality • Preventative • Inno High Quality • Preventative • Innovative • Productive • High Quality • Prev Preventative • Innovative • Productive • High Quality • Preventative • Inno High Quality • Preventative • Innovative • Productive • High Quality • Prev Preventative • Innovative • Productive • High Quality • Preventative • Inno • Innovative • Productive • High Quality • Preventative • Innovative • Prod Productive • High Quality • Preventative • Innovative • Productive • High Q
March 2010
Updated National VTErisk assessment tool
RISK ASSESSMENT FOR VENOUS THROMBOEMBOLISM (VTE)
Mobility – all patients (tick one box)
Tick Tick Tick
Surgical patient Medical patient expected to have ongoing reduced mobility relative to normal state
Medical patient NOT expected to have significantly reduced mobility relative to normal state
Assess for thrombosis and bleeding risk below Risk assessment now complete
Thrombosis risk
Patient related Tick Admission related Tick
Active cancer or cancer treatment Significantly reduced mobility for 3 days or more
Age > 60 Hip or knee replacement
Dehydration Hip fracture
Known thrombophilias Total anaesthetic + surgical time > 90 minutes
Obesity (BMI >30 kg/m2) Surgery involving pelvis or lower limb with a total anaesthetic + surgical time > 60 minutes
One or more significant medical comorbidities (eg heart disease;metabolic,endocrine or respiratory pathologies;acute infectious diseases; inflammatory conditions)
Acute surgical admission with inflammatory or intra-abdominal condition
Personal history or first-degree relative with a history of VTE
Critical care admission
Use of hormone replacement therapy Surgery with significant reduction in mobility
Use of oestrogen-containing contraceptive therapy
Varicose veins with phlebitis
Pregnancy or < 6 weeks post partum (see NICE guidance for specific risk factors)
Bleeding risk
Patient related Tick Admission related Tick
Active bleeding Neurosurgery, spinal surgery or eye surgery
Acquired bleeding disorders (such as acute liver failure) Other procedure with high bleeding risk
Concurrent use of anticoagulants known to increase the risk of bleeding (such as warfarin with INR >2)
Lumbar puncture/epidural/spinal anaesthesia expected within the next 12 hours
Acute stroke Lumbar puncture/epidural/spinal anaesthesia within the previous 4 hours
Thrombocytopaenia (platelets< 75x109/l)
Uncontrolled systolic hypertension (230/120 mmHg or higher)
Untreated inherited bleeding disorders (such as haemophilia and von Willebrand’s disease)
© Crown copyright 2010 301292 1p March 10
April 2010
NHS Standard Contractrequires acute serviceproviders to audit VTEprevention and undertakeroot cause analysis
Guidance on the NHSStandard Contract forAcute Services. 2010/11
Productive • High Quality • Preventative • Innovative • Productive • High Q High Quality • Preventative • Innovative • Productive • High Quality • Prev Preventative • Innovative • Productive • High Quality • Preventative • Inno • Innovative • Productive • High Quality • Preventative • Innovative • Prod Preventative • Innovative • Productive • High Quality • Preventative • Inno • Innovative • Productive • High Quality • Preventative • Innovative • High Productive • High Quality • Preventative • Innovative • Productive • High Q • Innovative • Productive • High Quality • Preventative • Innovative • Prod Preventative • Innovative • Productive • High Quality • Preventative • Inno High Quality • Preventative • Innovative • Productive • High Quality • Prev Productive • High Quality • Preventative • Innovative • Productive • High Q
April 2010
Academy of Medical RoyalColleges Statement on VTE
June 2010
A guide for deliveringthe CQUIN goal
July 2010
NICE quality standardon VTE preventionpublished
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
IMPLEMENTATION DIRECTORATE
QUALITY STANDARDS PROGRAMME
Draft Quality Standard for Venous Thromboembolism (VTE) - prevention
Output: Draft Quality Standard Executive Summary
Scope of Quality Standard for VTE - prevention:
The reduction in risk of venous thromboembolism (VTE) in adults admitted as hospital inpatients or formally admitted to a hospital bed for day-case procedures. Pregnant women and women up to 6 weeks post partum are also specifically covered.
Policy context:
Department of Health “Venous Thromboembolism Prevention: A Patient Safety Priority” (2009).
Key development sources:
The NICE quality standard is based on a pre-publication version of the NICE Clinical Guideline, “Venous thromboembolism - reducing the of venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to hospital” (CG/Wave14/26) which has an expected publication date of January 2010, and the earlier published NICE Clinical Guideline 46, “Venous thromboembolism: reducing the risk of venous thromboembolism (deep vein thrombosis and pulmonary embolism) within in-patients undergoing surgery” (CG46 only focuses on surgical patients and is both incorporated and partially updated by the current guideline in development). The timelines for development of this quality standard were adjusted due to changes in the development schedule of the Clinical Guideline.
For the pre-publication check version of NICE Clinical Guideline “Venous thromboembolism - reducing the risk”, see http://www.nice.org.uk/guidance/index.jsp?action=folder&o=45821.This draft quality standard will be updated when the forthcoming VTE clinical guideline is published to ensure consistency.
Overview of statements:
There are a total of 7 draft quality statements being presented for consultation and field testing, each with associated quality measures. During the first Topic Expert Group (TEG) meeting, 8 of the 9 Key Priorities for Implementation (KPIs) from the draft guideline were prioritised by the TEG for development into draft quality statements. The first 4 KPIs were
June 2010
Mandatory risk assessmentdata collection linked toCQUIN goal begins
Using the Commissioning for Quality and Innovation (CQUIN) payment framework – an addendum to the 2008 policy guidance for 2010/11
This document outlines developments to the CQUIN payment framework for2010/11. It should be read as an addendum to the guidance published in December 2008 and in the context of the 2010/11 NHS Operating Framework.
Executive Summary
The CQUIN framework continues as a national framework for locally agreed quality improvement schemes.
Providers of ambulance, community, mental health and learning disability services using national contracts, like providers of acute services, now need a full CQUIN scheme to earn CQUIN money.
Commissioners must make 1.5% of contract value (or equivalent non-contract activity value) available for each provider’s CQUIN scheme.
There should be a single CQUIN scheme per provider, with specifiedexceptions only.
CQUIN goals should reflect local priorities and priority areas set out in the NHS Operating Framework.
Goals should be stretching and focussed. They must not duplicatespecific minimum expectations of providers set out in Existing Commitments, Tiers 1 & 2 Vital Signs or standard contracts.
Stronger process – a standard format will prompt clear definition ofgoals, measurement and payment.
For the acute sector, schemes can no longer reward measurement.
Acute schemes must include the two specified national goals that the NHS Operations Board has confirmed for 2010/11, on reducing the impact of Venous Thromboembolism (VTE) and improving responsiveness to personal needs of patients.
SHAs are responsible for assuring schemes and ensuring that schemes demonstrate stretch and focus.

32
RISK ASSESSMENT FOR VENOUS THROMBOEMBOLISM (VTE)
All patients should be risk assessed on admission to hospital. Patients should be reassessed within 24 hours of admission and whenever the clinical situation changes.
STEP ONE Assess all patients admitted to hospital for level of mobility (tick one box). All surgical patients, and all medical patients with significantly reduced mobility, should be considered for further risk assessment.
STEP TWO Review the patient-related factors shown on the assessment sheet against thrombosis risk, ticking each box that applies (more than one box can be ticked).
Any tick for thrombosis risk should prompt thromboprophylaxis according to NICE guidance.
The risk factors identified are not exhaustive. Clinicians may consider additional risks in individual patients and offer thromboprophylaxis as appropriate.
STEP THREE Review the patient-related factors shown against bleeding risk and tick each box that applies (more than one box can be ticked).
Any tick should prompt clinical staff to consider if bleeding risk is sufficient to preclude pharmacological intervention.
Guidance on thromboprophylaxis is available at:
National Institute for Health and Clinical Excellence (2010) Venous thromboembolism: reducing the risk of venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to hospital. NICE clinical guideline 92. London: National Institute for Health and Clinical Excellence.
http://www.nice.org.uk/guidance/CG92
This document has been authorised by the Department of Health Gateway reference no: 10278
National venous thromboembolism riskassessment toolwww.dh.gov.uk

33
Veno
us Throm
boem
bolism Preve
ntion A
Guide
for D
elivering the CQUIN
Goa
l
RISK ASSESSMENT FOR VENOUS THROMBOEMBOLISM (VTE)
Mobility – all patients (tick one box)
Tick Tick Tick
Surgical patient Medical patient expected to have ongoing reduced mobility relative to normal state
Medical patient NOT expected to have significantly reduced mobility relative to normal state
Assess for thrombosis and bleeding risk below Risk assessment now complete
Thrombosis risk
Patient related Tick Admission related Tick
Active cancer or cancer treatment Significantly reduced mobility for 3 days or more
Age > 60 Hip or knee replacement
Dehydration Hip fracture
Known thrombophilias Total anaesthetic + surgical time > 90 minutes
Obesity (BMI >30 kg/m2) Surgery involving pelvis or lower limb with a total anaesthetic + surgical time > 60 minutes
One or more significant medical comorbidities (eg heart disease;metabolic,endocrine or respiratory pathologies;acute infectious diseases; inflammatory conditions)
Acute surgical admission with inflammatory or intra-abdominal condition
Personal history or first-degree relative with a history of VTE
Critical care admission
Use of hormone replacement therapy Surgery with significant reduction in mobility
Use of oestrogen-containing contraceptive therapy
Varicose veins with phlebitis
Pregnancy or < 6 weeks post partum (see NICE guidance for specific risk factors)
Bleeding risk
Patient related Tick Admission related Tick
Active bleeding Neurosurgery, spinal surgery or eye surgery
Acquired bleeding disorders (such as acute liver failure) Other procedure with high bleeding risk
Concurrent use of anticoagulants known to increase the risk of bleeding (such as warfarin with INR >2)
Lumbar puncture/epidural/spinal anaesthesia expected within the next 12 hours
Acute stroke Lumbar puncture/epidural/spinal anaesthesia within the previous 4 hours
Thrombocytopaenia (platelets< 75x109/l)
Uncontrolled systolic hypertension (230/120 mmHg or higher)
Untreated inherited bleeding disorders (such as haemophilia and von Willebrand’s disease)
© Crown copyright 2010 301292 1p March 10
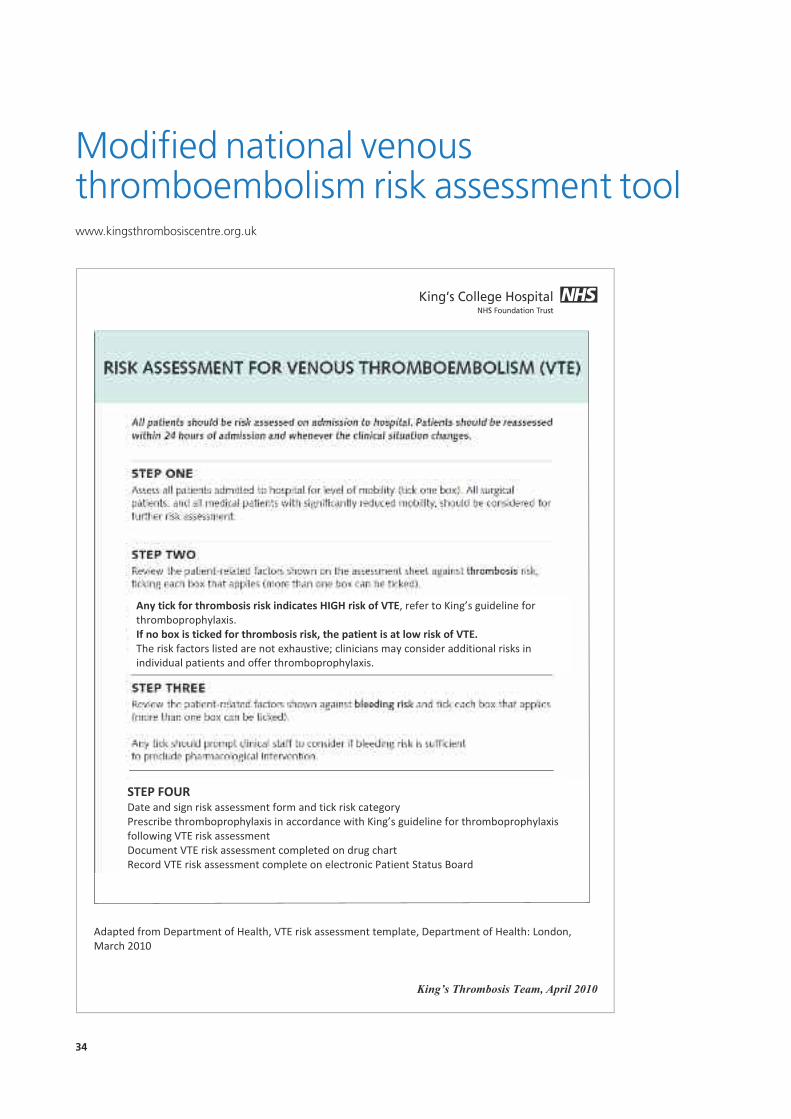
34
King’s Thrombosis Team, April 2010
Modified national venousthromboembolism risk assessment toolwww.kingsthrombosiscentre.org.uk

35
Veno
us Throm
boem
bolism Preve
ntion A
Guide
for D
elivering the CQUIN
Goa
l
Hospital no:
Surnam
e:
Firs
t nam
e:
DO
B:
Kin
g’s T
hrom
bosis
Tea
m, A
pril
2010
King’s Throm
bosis
Team
, April
2010
SURGICALPATIENTS
MEDICAL
PATIENTS
Ris
k of
VTE
R
ecom
men
ded
Prop
hyla
xis
Rec
omm
ende
d pr
ophy
laxi
s H
IGH
(w
ith lo
w ri
sk o
f bl
eedi
ng)
Enoxaparin
40 m
g daily
*
+ TE
D stoc
kings
+/- Sequ
entia
l com
pres
sion
devic
e
+
Early
mob
ilisat
ion
Enox
apar
in 4
0 m
g da
ily
+
Early
mob
ilisat
ion
HIG
H
(with
sig
nific
ant
risk
of b
leed
ing)
TE
D st
ockin
gs +
/- Se
quen
tial c
ompr
essio
n de
vice
+
Ea
rly m
obilis
atio
n
TED
stoc
kings
+/-
sequ
entia
l com
pres
sion
devic
e
+ Ea
rly m
obilis
atio
n (D
o NO
T us
e TE
D st
ockin
gs in
stro
ke p
atie
nts)
LOW
Ea
rly m
obilis
atio
n Ea
rly m
obilis
atio
n
*use
riva
roxa
ban
10m
g da
ily in
ele
ctive
hip
or k
nee
arth
ropl
asty
pos
t-ope
rativ
ely
only
Obs
tetr
ic p
atie
nts:
see
King’
s ris
k as
sess
men
t for
VTE
in p
regn
ancy
& u
p to
six
week
s po
st p
artu
m.
Neu
rosu
rgic
al p
atie
nts
Elec
tive
spin
al s
urge
ry
Cran
ial s
urge
ry p
atie
nts
(benign/malignant
tumours
, clip
ped
aneu
rysm
s, s
hunt
re
visi
ons/
inse
rtion
s, tr
ansp
heno
idal
sur
gery
, coi
led
aneu
rysm
s)
TED
stoc
kings
(+/-
Sequ
entia
l com
pres
sion
devic
e fo
r cra
nial
su
rger
y)
If ≥
ONE
pat
ient
rela
ted
risk
fact
or a
dd e
noxa
parin
40m
g da
ily
star
ting
24h
post
-ope
rativ
ely
only
Emer
genc
y sp
inal
pat
ient
s En
oxap
arin
40m
g da
ily +
TED
sto
ckin
gs
STO
P en
oxap
arin
24h
pre
oper
ative
ly, re
star
t 6h
post
-ope
rativ
ely
Maj
or h
ead
inju
ry
TED
stoc
kings
Ad
d en
oxap
arin
onl
y if
decis
ion
docu
men
ted
by re
gist
rar/c
onsu
ltant
Hi
gh b
leed
ing
risk
(SA
H, u
nsec
ured
ane
urys
m a
nd AV
Ms,
SD
H (b
oth
surg
ical
ly
and
cons
erva
tivel
y m
anag
ed),
EV
D in
situ
, DB
S in
serti
on)
TED
stoc
kings
If ≥
ONE
pat
ient
rela
ted
risk
fact
or +
/- Se
quen
tial c
ompr
essio
n de
vice
CO
NTR
AIN
DIC
ATI
ON
S En
oxap
arin
TE
Ds/
SCD
s
Tim
ing:
En
oxap
arin
sho
uld
star
t 6
hour
s po
st o
p (p
rovid
ing
haem
osta
sis s
ecur
ed)
and
then
at
6pm
dai
ly th
erea
fter.
In
addi
tion,
Eno
xapa
rin c
an b
e gi
ven
the
even
ing
prio
r to
sur
gery
(exc
ludi
ng n
euro
surg
ery,
see
abo
ve).
Mec
hani
cal
VTE
prop
hyla
xis s
houl
d be
offe
red
at a
dmiss
ion.
Ep
idur
al
Plac
emen
t or r
emov
al o
f cat
hete
r sho
uld
be d
elay
ed fo
r 12
hrs
afte
r adm
inist
ratio
n of
eno
xapa
rin.
/Spi
nal
Enox
apar
in s
houl
d no
t be
give
n so
oner
than
4 h
rs a
fter c
athe
terr
emov
al.
Ana
lges
ia
Plac
emen
t or r
emov
al o
f cat
hete
r sho
uld
be d
elay
ed fo
r 18
hrs
afte
r adm
inist
ratio
n of
riva
roxa
ban,
Ri
varo
xaba
n sh
ould
not
be
give
n so
oner
than
6 h
rs a
fter c
athe
ter r
emov
al.
Dur
atio
n:
Cont
inue
unt
il mob
ility
no lo
nger
sig
nific
antly
redu
ced.
High
risk
orth
opae
dic
patie
nts
shou
ld re
ceive
pro
phyla
xis fo
r at l
east
10
days
. Ele
ctive
kne
e re
plac
emen
t sho
uld
rece
ive 1
4 da
ys p
roph
ylaxis
. Ex
tend
ed p
roph
ylaxis
(28
days
) is
reco
mm
ende
d fo
r ele
ctive
hip
repl
acem
ent,
hip
fract
ure
and
othe
r sel
ecte
d hi
gh-
risk
gene
ral s
urge
ry p
atie
nts
e.g.
maj
or c
ance
r sur
gery
.O
besi
ty:
use
Enox
apar
in 4
0mg
twice
dai
ly if
body
wei
ght
>100
kg (o
r 60
mg
bd if
bod
y we
ight
>15
0kg)

36
WHO surgical safety checklistwww.npsa.nhs.uk/nrls

37
Veno
us Throm
boem
bolism Preve
ntion A
Guide
for D
elivering the CQUIN
Goa
l

38
VTE prevention at King’s College Hospitalwww.kingsthrombosiscentre.org.uk

39
Veno
us Throm
boem
bolism Preve
ntion A
Guide
for D
elivering the CQUIN
Goa
l
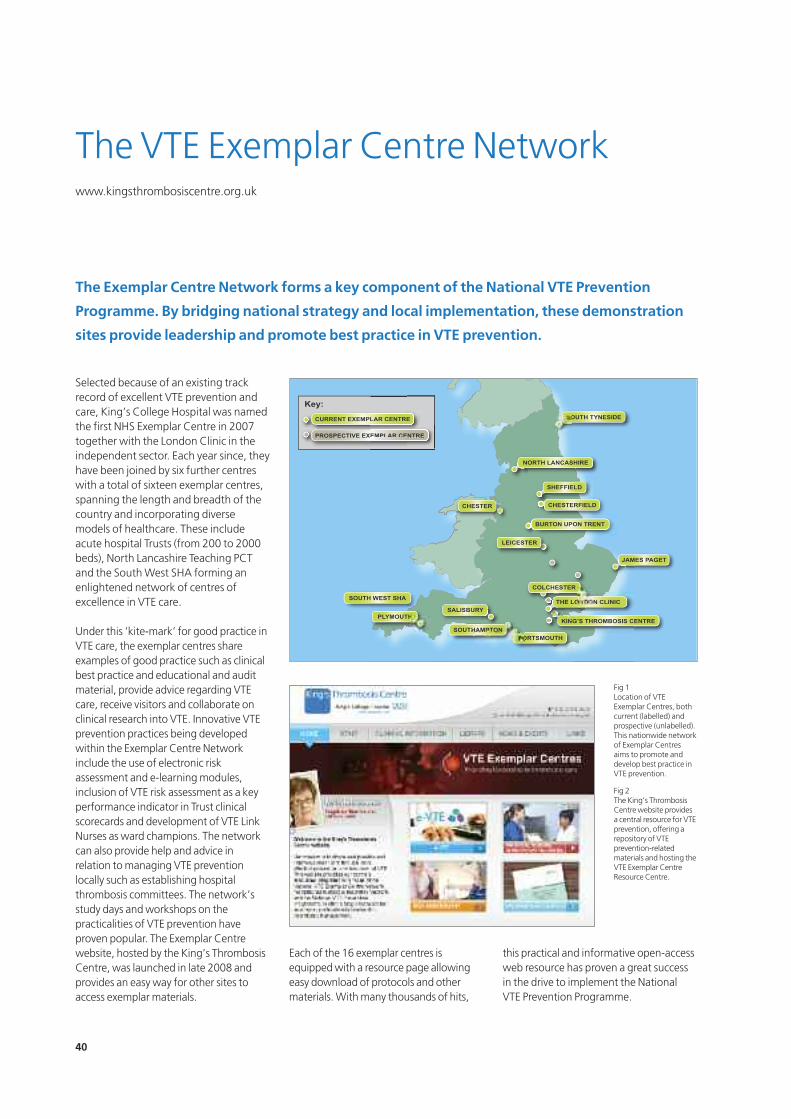
40
Selected because of an existing trackrecord of excellent VTE prevention andcare, King’s College Hospital was namedthe first NHS Exemplar Centre in 2007together with the London Clinic in theindependent sector. Each year since, theyhave been joined by six further centreswith a total of sixteen exemplar centres,spanning the length and breadth of thecountry and incorporating diversemodels of healthcare. These includeacute hospital Trusts (from 200 to 2000beds), North Lancashire Teaching PCTand the South West SHA forming anenlightened network of centres ofexcellence in VTE care.
Under this ‘kite-mark’ for good practice inVTE care, the exemplar centres shareexamples of good practice such as clinicalbest practice and educational and auditmaterial, provide advice regarding VTEcare, receive visitors and collaborate onclinical research into VTE. Innovative VTEprevention practices being developedwithin the Exemplar Centre Networkinclude the use of electronic riskassessment and e-learning modules,inclusion of VTE risk assessment as a keyperformance indicator in Trust clinicalscorecards and development of VTE LinkNurses as ward champions. The networkcan also provide help and advice inrelation to managing VTE preventionlocally such as establishing hospitalthrombosis committees. The network’sstudy days and workshops on thepracticalities of VTE prevention haveproven popular. The Exemplar Centrewebsite, hosted by the King’s ThrombosisCentre, was launched in late 2008 andprovides an easy way for other sites toaccess exemplar materials.
Each of the 16 exemplar centres isequipped with a resource page allowingeasy download of protocols and othermaterials. With many thousands of hits,
this practical and informative open-accessweb resource has proven a great successin the drive to implement the National VTE Prevention Programme.
The VTE Exemplar Centre Networkwww.kingsthrombosiscentre.org.uk
The Exemplar Centre Network forms a key component of the National VTE Prevention
Programme. By bridging national strategy and local implementation, these demonstration
sites provide leadership and promote best practice in VTE prevention.
CURRENT EXEMPLAR CENTRE
PROSPECTIVE EXEMPLAR CENTRE
Key:
LAR CENTRE
EMPLAR CE
E
NTRE
SALISBURYPLYMOUTH
SOUTH WEST SHA
KING’S THROMBOSIS CENTRE
JAMES PAGET
SOUTH TYNESIDE
NORTH LANCASHIRE
SHEFFIELD
CHESTERFIELD
BURTON UPON TRENT
THE LONDON CLINIC
COLCHESTER
SOUTHAMPTONPORTSMOUTH
LEICESTER
CHESTER
Fig 1Location of VTEExemplar Centres, bothcurrent (labelled) andprospective (unlabelled).This nationwide networkof Exemplar Centresaims to promote anddevelop best practice inVTE prevention.
Fig 2 The King’s ThrombosisCentre website providesa central resource for VTEprevention, offering arepository of VTEprevention-relatedmaterials and hosting theVTE Exemplar CentreResource Centre.

41
Veno
us Throm
boem
bolism Preve
ntion A
Guide
for D
elivering the CQUIN
Goa
l
The primary objective is to support theNHS in London implement Professor Lord Darzi's Healthcare for London: AFramework for Action (July 2007), theimplementation of which is being takenforward by the new Sector AcuteCommissioning Units and PCTs,embedded in NHS London's five-yearIntegrated Strategic Plan (ISP). The LQOwill help facilitate the implementation ofHealthcare for London through theprovision of information that supportsthe achievement of quality in serviceprovision, value for money andmeasurable improvements incommissioning.
The NHS London CQUIN meeting in May 2010 sought to address the issue of delivering the national CQUIN goal.The meeting was addressed by The NHSMedical Director, Professor Sir BruceKeogh, who encouraged all delegates to work out the fine details arounddelivery of VTE prevention. Many ideasand working examples of VTE preventioninitiatives that will help to deliver theCQUIN goal were brought to themeeting, and this information is beingcollated and placed on the LondonQuality Observatory, so that it’s available for all.
London’s Quality Observatory portalhttp://lqo.csl.nhs.uk
London's Quality Observatory (LQO) is a new web-based information portal supporting
the NHS quality agenda for London. It will serve commissioners, clinicians and provider
organisations, offering one-stop access to robust, high quality data and information.
Fig 3The LQO site includes slides and materials from the
London CQUIN meeting (Venous thromboembolism:reducing the risk and improving care – delivering the
national CQUIN goal), which took place on 10 May 2010.
Fig 4 The NHS Medical Director, Professor Sir Bruce Keogh,
addressed the NHS London CQUIN meeting andencouraged all attendees to work out the fine details
around delivery of VTE prevention. Pre and post meetingmaterials are available on the LQO site.

42
Why a Map of Medicine?
The Map of Medicine (the Map) assistsorganisations and individuals to ensurethat they remain abreast of the everincreasing array of healthcaretechnologies and innovations acrossareas of healthcare outside their specialty domain yet pertinent to holistic patient care.
Why embed the VTE preventionpathway within the Map?
VTE prevention is relevant to everyonewithin the hospital and primary caremultidisciplinary team – however, this isjust one topic that is important to thegeneralist, so embedding the VTE riskassessment and prevention pathwaywithin the Map ensures that thegeneralist (for example, a consultant on a post-intake ward round, a GP ornew locum doctor) can typically find theinformation they require, hencedisseminating information consistently.The Map covers over 350 topics withmore added every quarter.
In addition, locally specific informationallows merging local policies and protocolswith the power of the internationalevidence base within the Map to create aflexible national, but locally controlled,clinical knowledge framework for thehealthcare system. For example, the VTEMap can be adapted to suit local choices of drugs (such as NICE-approvedanticoagulants), providing local ownership.
Updates in 2010
The VTE risk assessment pathway nowincludes general recommendations for
VTE risk assessment and bleedingassessment for all patients (includingCQUIN government targets), and specificprophylaxis recommendations forsurgical, medical, trauma, and pregnantpatients. In line with Map of Medicine'seditorial methodology, the updatedpathway includes information for patientsand carers. The pathway also links toDepartment of Health’s VTE e-learning forhealthcare, an online resource helping toraise awareness and understanding ofVTE within the medical community.
Access the VTE Map of Medicine Pathway
The Map of Medicine is available licensefree to individuals across NHS Englandand Wales. You can access the pathwayvia www.mapofmedicine.com/england
Map of Medicine and venousthromboembolism pathwayswww.mapofmedicine.com/england
The VTE risk assessment pathway on the Map of Medicine has been updated in line with the
latest clinical practice and reflects the 2010 NICE guideline and Department of Health guidance.
Fig 5Image of VTE Map of Medicine Pathway showing the
ability to link from a node in the Map to the e-LfH e-learning module.
A read-only version of the Map is available on NHSChoices at http://healthguides.mapofmedicine.com.
The professional version (which allows localisationof the content) is licensed for use by all NHS staffand GPs. To find out how to access the Map visit
www.mapofmedicine.com.
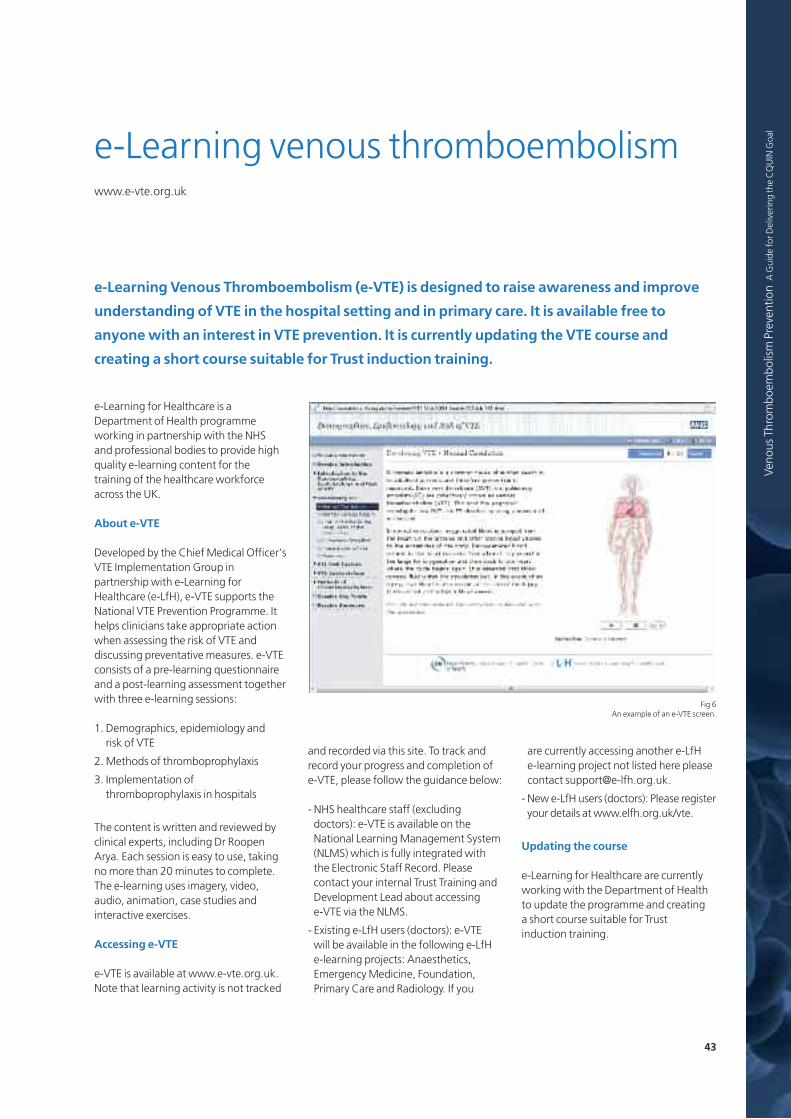
43
Veno
us Throm
boem
bolism Preve
ntion A
Guide
for D
elivering the CQUIN
Goa
l
e-Learning for Healthcare is aDepartment of Health programmeworking in partnership with the NHS and professional bodies to provide highquality e-learning content for thetraining of the healthcare workforceacross the UK.
About e-VTE
Developed by the Chief Medical Officer’sVTE Implementation Group inpartnership with e-Learning forHealthcare (e-LfH), e-VTE supports theNational VTE Prevention Programme. Ithelps clinicians take appropriate actionwhen assessing the risk of VTE anddiscussing preventative measures. e-VTEconsists of a pre-learning questionnaireand a post-learning assessment togetherwith three e-learning sessions:
1. Demographics, epidemiology and risk of VTE
2. Methods of thromboprophylaxis
3. Implementation ofthromboprophylaxis in hospitals
The content is written and reviewed byclinical experts, including Dr RoopenArya. Each session is easy to use, takingno more than 20 minutes to complete.The e-learning uses imagery, video,audio, animation, case studies andinteractive exercises.
Accessing e-VTE
e-VTE is available at www.e-vte.org.uk.Note that learning activity is not tracked
and recorded via this site. To track andrecord your progress and completion ofe-VTE, please follow the guidance below:
- NHS healthcare staff (excludingdoctors): e-VTE is available on theNational Learning Management System(NLMS) which is fully integrated withthe Electronic Staff Record. Pleasecontact your internal Trust Training andDevelopment Lead about accessing e-VTE via the NLMS.
- Existing e-LfH users (doctors): e-VTE will be available in the following e-LfHe-learning projects: Anaesthetics,Emergency Medicine, Foundation,Primary Care and Radiology. If you
are currently accessing another e-LfH e-learning project not listed here pleasecontact [email protected].
- New e-LfH users (doctors): Please registeryour details at www.elfh.org.uk/vte.
Updating the course
e-Learning for Healthcare are currentlyworking with the Department of Healthto update the programme and creating a short course suitable for Trust induction training.
e-Learning venous thromboembolismwww.e-vte.org.uk
e-Learning Venous Thromboembolism (e-VTE) is designed to raise awareness and improve
understanding of VTE in the hospital setting and in primary care. It is available free to
anyone with an interest in VTE prevention. It is currently updating the VTE course and
creating a short course suitable for Trust induction training.
Fig 6 An example of an e-VTE screen.

44
References1. Using the Commissioning for Quality and Innovation (CQUIN) payment framework (with addendum for 2010/11).
Department of Health, 2009www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_091443
2. Quality Standard for Venous Thromboembolism (VTE) – Prevention. NICE, 2010www.nice.org.uk/aboutnice/qualitystandards/vteprevention
3. NHSLA Risk Management Standards for Acute Trusts, Primary Care Trusts and Independent Sector Providers of NHS Care 2010/11. NHS Litigation Authority, 2010 www.nhsla.com/NR/rdonlyres/E974091E-036C-4D5E-A28F-229687E08461/0/201011AcuteISPCTStandardsFINAL.doc
4. High Quality Care For All. Department of Health, 2008www.dh.gov.uk/en/publicationsandstatistics/publications/publicationspolicyandguidance/DH_085825
5. The NHS operating framework for England for 2010/11. Department of Health, 2009www.dh.gov.uk/prod_consum_dh/idcplg?IdcService=SS_GET_PAGE&ssDocName=DH_091445
6. The standard NHS contracts for acute hospital, mental health, community and ambulance services and supporting guidance. Department of Health, 2010www.dh.gov.uk/prod_consum_dh/idcplg?IdcService=SS_GET_PAGE&ssDocName=DH_091451
7. Reducing the risk of venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to hospital. NICE, 2010http://guidance.nice.org.uk/CG92
8. Venous thromboembolism: reducing the risk of venous thromboembolism (deep vein thrombosis and pulmonary embolism) in inpatients undergoing surgery. NICE, 2007http://guidance.nice.org.uk/CG46
9. NHS 2010 - 2015: from good to great. Preventative, people-centred, productive. Department of Health, 2009www.dh.gov.uk/en/publicationsandstatistics/publications/publicationspolicyandguidance/dh_109876
10.Prevention of Venous Thromboembolism (VTE) in Hospitalised Patients (Dear colleague letter). Department of Health, March 2010www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_114570.pdf
11.Prevention of Venous Thromboembolism (VTE) in Hospitalised Patients (Dear colleague letter). Department of Health, May 2010www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_116320.pdf
12.Guidance Notes on VTE Data Collection. Department of Health, May 2010www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_116316
13.Academy Statement on VTE. The Academy of Medical Royal Colleges, April 2010www.aomrc.org.uk/component/content/article/38-general-news/143-academy-statement-on-vte.html
14.Maynard G, Stein J. Preventing Hospital-Acquired Venous Thromboembolism: A Guide for Effective Quality Improvement (AHRQ Publication No. 08-0075). Agency for Healthcare Research and Quality, Rockville, MD, USA, August 2008www.ahrq.gov/qual/vtguide/vtguide.pdf
15.Working to provide potential IT solutions for Venous Thromboembolism. NHS Connecting for Health - Clinical Connections, May 2009 www.connectingforhealth.nhs.uk/engagement/clinical/newsletters/connections11.pdf
16.White RH, et al. Evaluation of the predictive value of ICD-9-CM coded administrative data for venous thromboembolism in the United States. Thromb Res 2010; 126:61-7www.sciencedirect.com/science/journal/00493848
17.Spencer FA, et al. Venous thromboembolism in the outpatient setting. Arch Intern Med 2007;167:1471-5http://archinte.ama-assn.org/cgi/content/full/167/14/1471

www.kingsthrombosiscentre.org.uk
The King’s Thrombosis Centre, led by Dr Roopen Arya, forms part of theDepartment of Haematological Medicine, an Academic Clinical Unit providinghaematology laboratory and clinical services within King’s College Hospital,London. The King’s Thrombosis Centre was identified as the first NHS VTE
Exemplar Centre as part of the Chief Medical Officer's initiative to promote bestpractice in the prevention of VTE.
www.kingsthrombosiscentre.org.uk/cgi-bin/kings/exemplarcentres.pl
VTE Exemplar centres form a diverse and enlightened network of hospitals thathave an existing track record of excellence in VTE prevention and care, offerpractical support and advice to other centres by sharing their resources, and
collaborate on clinical research into VTE.
www.thrombosis-charity.org.uk
Lifeblood wishes to increase awareness of thrombosis among the public andhealth professionals and to raise research funds to improve patient care through
improved prevention and treatment of venous thromboembolic disease.