VBWG OASIS-6 The Sixth Organization to Assess Strategies in Acute Ischemic Syndromes trial.
Upload
jeffry-augustine-tylerCategory
view
219download
3
VBWG
CHARISMA
Clopidogrel for High Atherothrombotic Risk and Ischemic Stabilization, Management, and Avoidance trial
VBWG
CHARISMA: Background and hypothesis
• The combination of clopidogrel plus aspirin has been demonstrated to be superior to aspirin in the treatment of patients with ACS and after coronary stenting.
• When added to the current standard of care, does long-term treatment with clopidogrel plus aspirin provide greater vascular protection than aspirin alone in a broad population of high-risk patients?
Bhatt DL et al. Am Heart J. 2004;148:263-8.Bhatt DL et al. N Engl J Med. 2006;354:1706-17.

VBWG
*n = 166 not in either category, butincluded in overall analysis
†Coronary, cerebral, or peripheral
CHARISMA: Study design
Clopidogrel 75 mgASA 75-162 mg
n = 7802
PlaceboASA 75-162 mg
n = 7801
Symptomatic patients with coronary, cerebrovascular, or
peripheral arterial disease*n = 12,153
Follow-up until 1040 primary events
Primary end point:First occurrence of MI, stroke (any cause), CV death (including hemorrhagic)
Principal secondary end point:First occurrence of MI, stroke, CV death, hospitalization for UA, TIA, revascularization†
RandomizedDouble-blind
Bhatt DL et al. Am Heart J. 2004;148:263-8.Bhatt DL et al. N Engl J Med. 2006;354:1706-17.
Asymptomatic patients with multiple atherothrombotic
risk factors*n = 3284
N = 15,603

VBWG
CHARISMA: Baseline characteristics
Clopidogrel + ASA(n = 7802)
Placebo + ASA(n = 7801)
Age (years) Median Range
64.039.0–95.0
64.045.0–93.0
Female sex (%) 29.7 29.8
Race/ethnicity (%) White Hispanic Asian Black Other
80.49.95.03.21.5
79.910.75.03.01.4
Smoking status (%) Current Former
20.148.9
20.348.7
Bhatt DL et al. N Engl J Med. 2006;354:1706-17.

VBWG
CHARISMA: Baseline characteristics, cont’d
Clopidogrel + ASA(n = 7802)
(%)
Placebo + ASA(n = 7801)
(%)
Hypertension 73.3 73.9
Hypercholesterolemia 73.7 74.2
Diabetes 42.3 41.7
Prior MI 34.2 34.9
Prior stroke 24.9 24.3
PAD 22.6 22.7
PCI 22.4 23.1
CABG 19.5 19.9
Bhatt DL et al. N Engl J Med. 2006;354:1706-17.Other comorbidities each occurred in <15%
VBWG
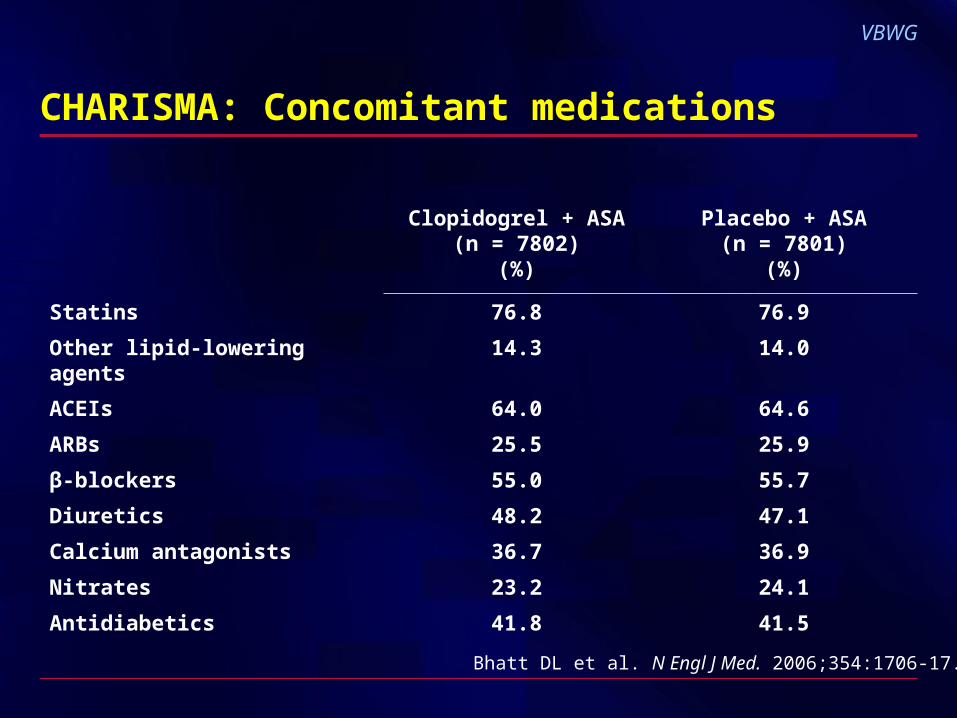
CHARISMA: Concomitant medications
Clopidogrel + ASA(n = 7802)
(%)
Placebo + ASA(n = 7801)
(%)
Statins 76.8 76.9
Other lipid-lowering agents 14.3 14.0
ACEIs 64.0 64.6
ARBs 25.5 25.9
β-blockers 55.0 55.7
Diuretics 48.2 47.1
Calcium antagonists 36.7 36.9
Nitrates 23.2 24.1
Antidiabetics 41.8 41.5
Bhatt DL et al. N Engl J Med. 2006;354:1706-17.

VBWG
CHARISMA: Treatment effect on primary end point
Bhatt DL et al. N Engl J Med. 2006;354:1706-17.
Cumulative incidence of MI, stroke, CV death; N = 15,603
7% RRRRR 0.93 (0.83–1.05)P = 0.22
Months
10
8
6
4
2
00 6 12 18 24 30
PlaceboClopidogrel
Events (%)

VBWG
CHARISMA: Treatment effect on principal secondary end point
Bhatt DL et al. N Engl J Med. 2006;354:1706-17.
Cumulative incidence of MI, stroke, CV death, hospitalization for UA,
TIA, revascularization;* N = 15,603
*Coronary, cerebral, or peripheral
20
15
10
5
00 6 12 18 24 30
Months
PlaceboClopidogrel
8% RRRRR 0.92 (0.86-0.995)P = 0.04
Events (%)
VBWG
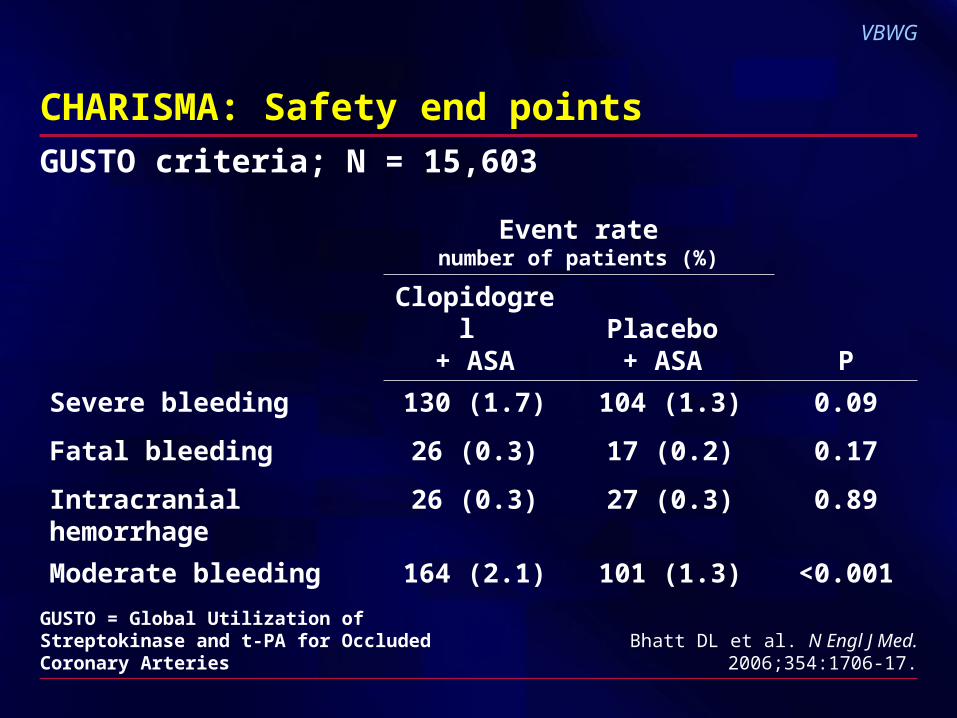
CHARISMA: Safety end points
Event ratenumber of patients (%)
Clopidogrel + ASA
Placebo + ASA P
Severe bleeding
Fatal bleeding
Intracranial hemorrhage
130 (1.7)
26 (0.3)
26 (0.3)
104 (1.3)
17 (0.2)
27 (0.3)
0.09
0.17
0.89
Moderate bleeding 164 (2.1) 101 (1.3) <0.001
Bhatt DL et al. N Engl J Med. 2006;354:1706-17.
GUSTO criteria; N = 15,603
GUSTO = Global Utilization of Streptokinase and t-PA for Occluded Coronary Arteries

VBWG
n = 3284
n = 12,153
N = 15,603
CHARISMA: Treatment effect by inclusion criteria
MI, stroke, CV death
*Multiple atherothrombotic risk factors†Documented coronary, cerebrovascular, or peripheral arterial disease
0.5 1.0 1.5Placebobetter
Clopidogrelbetter
Asymptomatic*
Symptomatic†
All patients
Hazard ratio RR (95% CI)
1.20 (0.91–1.59)
0.88 (0.77–0.998)
0.93 (0.83–1.05)
Bhatt DL et al. N Engl J Med. 2006;354:1706-17.
P = 0.20
P = 0.046
P = 0.22
VBWG
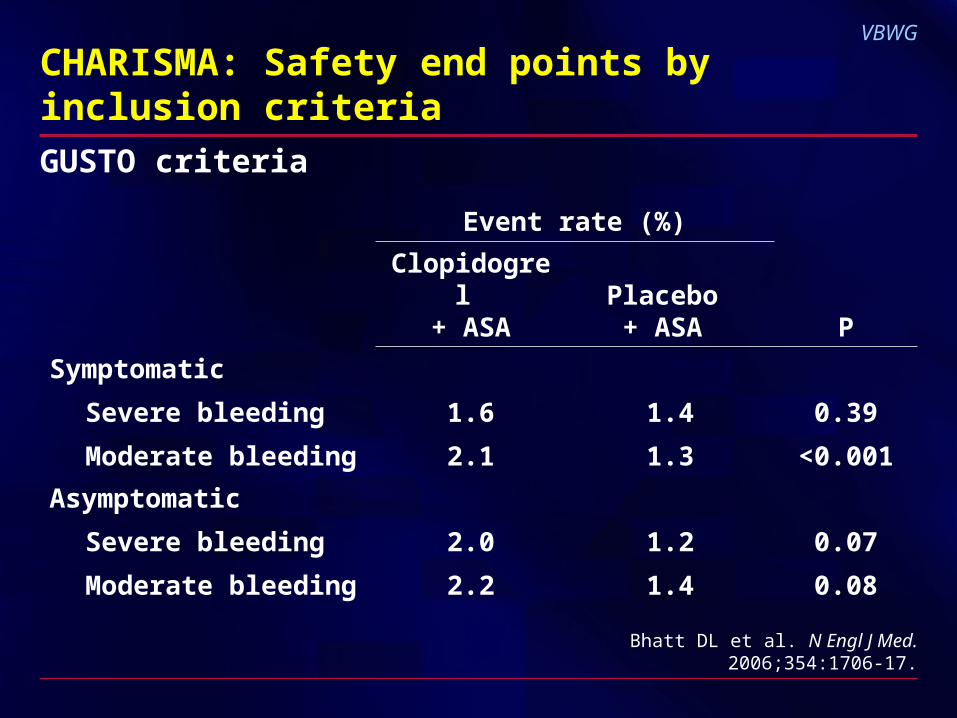
CHARISMA: Safety end points by inclusion criteria
Event rate (%)
Clopidogrel + ASA
Placebo + ASA P
Symptomatic
Severe bleeding
Moderate bleeding
1.6
2.1
1.4
1.3
0.39
<0.001
Asymptomatic
Severe bleeding
Moderate bleeding
2.0
2.2
1.2
1.4
0.07
0.08
Bhatt DL et al. N Engl J Med. 2006;354:1706-17.
GUSTO criteria

VBWG
CHARISMA: Summary
• Primary efficacy end point7% decrease in MI, stroke, CV death (nonsignificant)
• Principal secondary efficacy end point8% decrease in MI, stroke, CV death, hospitalization for UA, TIA, revascularization (significant)
• Primary safety end pointSevere bleeding was not significantly increased but a trend was noted
Bhatt DL et al. N Engl J Med. 2006;354:1706-17.

VBWG
CHARISMA: Summary, cont’d
• Symptomatic patients experienced a 12% reduction in the primary end point (significant) with no significant increase in severe bleeding
• Asymptomatic patients experienced a 20% increase in the primary end point (nonsignificant) with no significant increase in severe bleeding
• Overall, clopidogrel plus aspirin was not significantly more effective than aspirin alone in reducing the primary end point
Bhatt DL et al. N Engl J Med. 2006;354:1706-17.