Varicose veins
66
By Mahmoud Zaghloul Raslan, MD Consultant Surgeon, MGH Madina
Transcript of Varicose veins

By
Mahmoud Zaghloul Raslan, MD
Consultant Surgeon, MGH
Madina

Definition
Dilated tortuous superficial veins in
the lower limbs
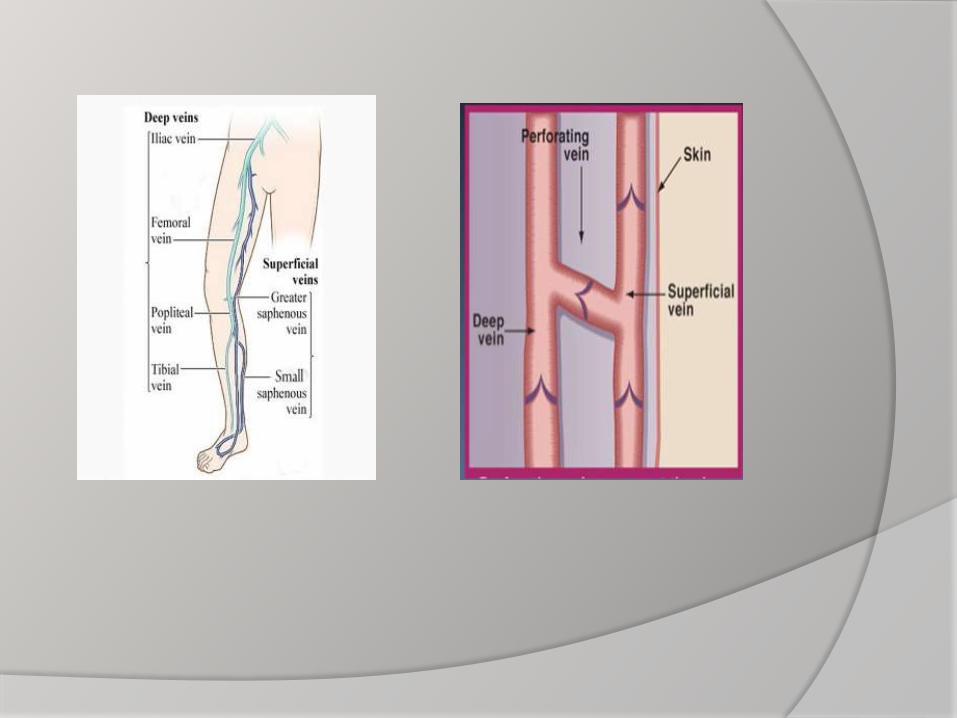
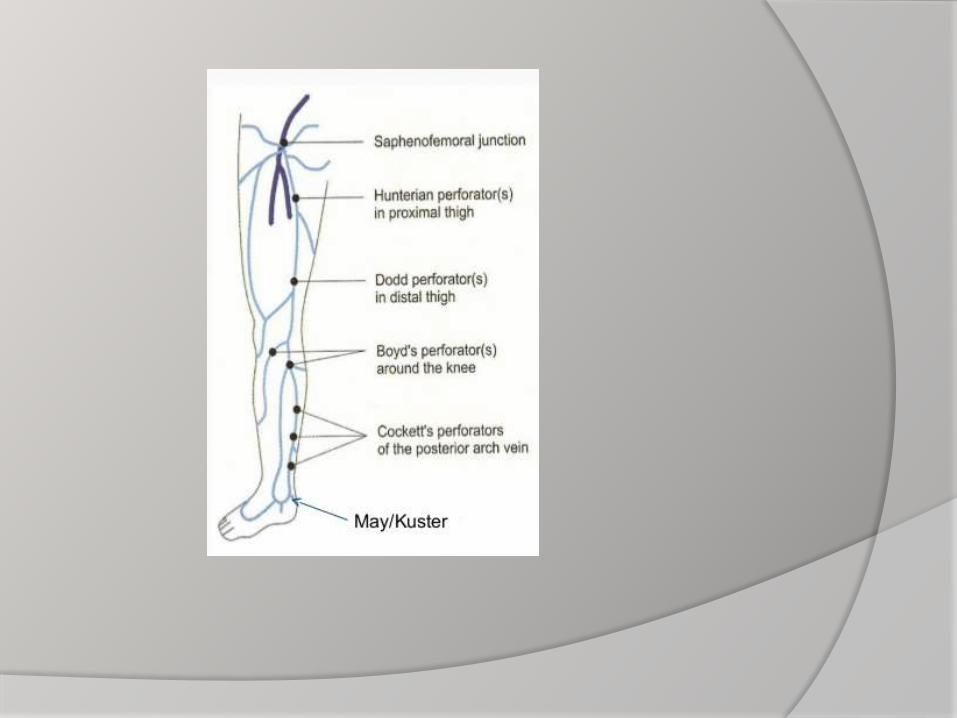
Anatomy
Venous drainage from LL is through 3 systems:
- Superficial veins:
- Long saphenous vein and tributaries
- Short saphenous vein and tributaries
- Deep veins: Ant. Tibial, post. Tibial,
peroneal, popliteal, deepF., superficial F.
and common F.
- Perforating veins: perforating deep fascia
to connect superficial with deep veins



Pathophysiology
Physiology:
_ Blood conductor:
- Muscular compression
- Negative ITP
- Calf Muscle pump
- Presence of valves

_ Blood reservoir:
- Dilatable
- Capacious
Etiology and Types
Primary VV
_ High IVP: prolonged standing,
prolonged sitting with crossed
legs, chronic straining,
_ Weakness of vein walls:
- Obesity
- Pregnancy
- Hormonal

Secondary VV:
- After previous DVT
- With pelvic tumours

Clinical Picture
Thorough history taking:
- Occupation and prolonged standing
- Throbophlebitis or DVT
- Coaguation disorders
- Diabetes
- Results of previous treatment
- Pregnancy and contraceptive pills
Symptoms:
- Pain: aching, throbbing, tingling
- Cramps, heaviness, tiredness of
legs, restless legs at night
- Of complications: Itching,
hyperpigmentation, skin ulceration
and bleeding
- Leg disfigurement



Trendlenberg test
Investigations
General:- Assess the general condition of the patient:
e.g. CBC,liver and kidney function tests
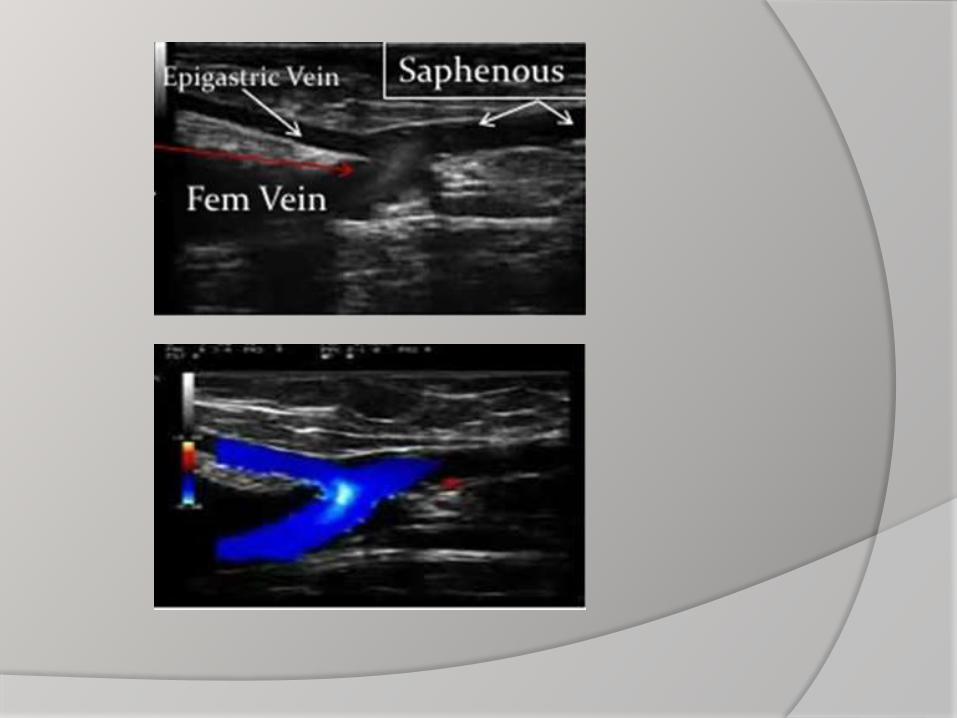
Specific: - Hand-held Doppler
- Duplex ultrasound: The best; gives both anatomical and functional diagnosis
- Others: e.g. CT venography and MRI rarely needed





Treatment

Initial conservative
treatment
(I) General measures:
Leg elevation
Excerise
(II) Compression therapy:
(III) Pharmacologic therapy:
Venoactive drugs
- Micronized purified flavonoid
MPFF e.g.Daflon
- Hydroxyethylrutoside
Rheologic agents:
- Aspirin
- Stanozolol
- pentoxifylline
- prostacyclin analogues

(IV) Skin care: Skin cleansing e.g. Dove, Olay
Emollients e.g. vaseline, cetaphil
Barrier preparations e.g. zinc oxide
cream, Vaseline
Topical corticosteroids
(V) Ulcer care Ulcer debridement
Role of systemic antibiotics
Topical agents:
- e.g. Silver sulfadiazine
- Other antiseptic agents
Ulcer dressings
- Low-adherent gauze
- Hydrogels and alginate dressing
- Silver containing dressings
Compressing dressing
Skin grafting
Others:
- Hyperbaric oxygen
- Electromagnetic therapy
- Therapeutic ultrasound
Vein ablative therapy
Indications:
- Venous hemorrhage
- Superficial thrombophlebitis
- Venous reflux associated with
symptoms
Contraindications:
- Pregnancy
- Acute superficial or deep venous
thrombosis
- Moderate to severe PAD
- Advanced generalized systemic
disease

Types of vein ablative
therapy
Chemical:
- Sclerotherpy
Mechanical:
- Surgical excision
Thermal:
- Radiofrequency ablation RFA
- Endovenous laser therapy EVLA

Sclerotherapy
Sclerosants:
_ Sodium tetradecyl sulphate
_ Sodium marrhuate
_ Polydocanol
_ Ethanolamine oleate
_ Hypertonic saline



Surgical stripping

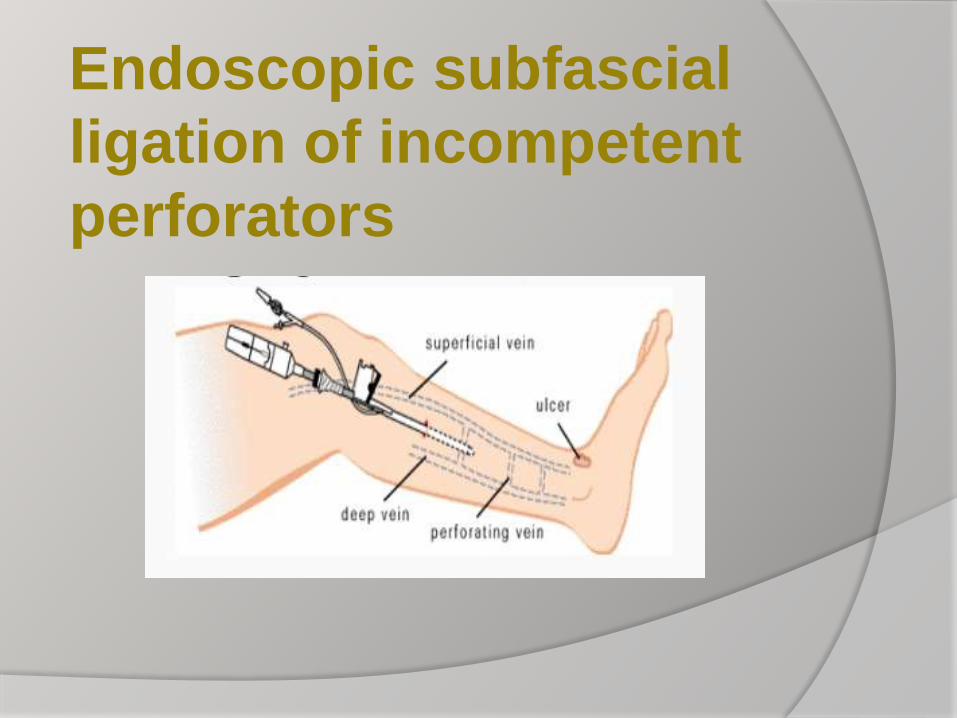
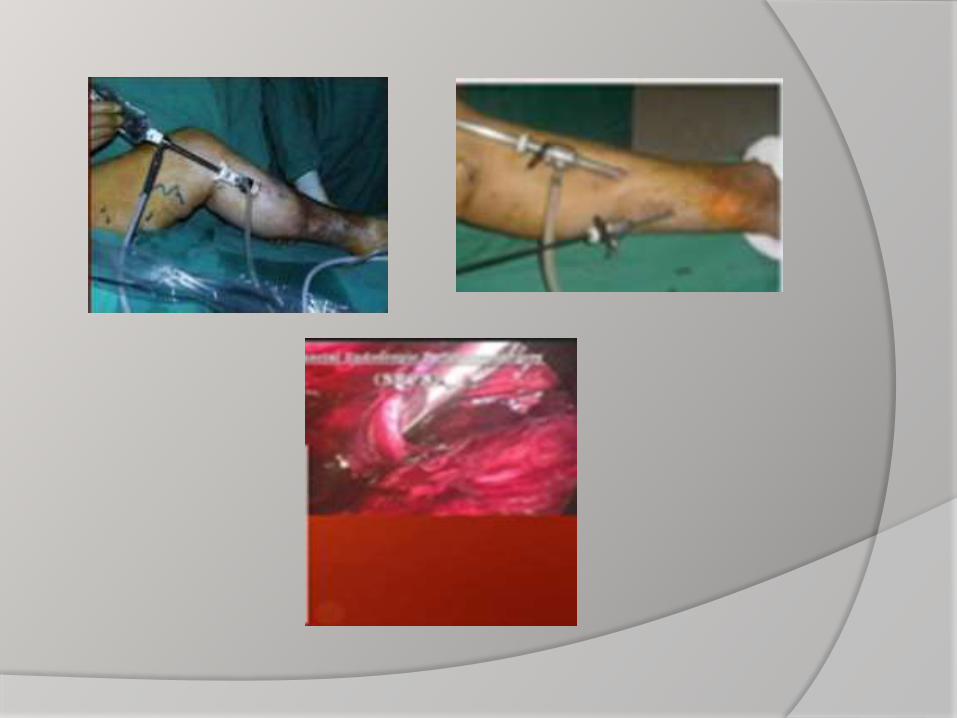
Endoscopic subfascial
ligation of incompetent
perforators
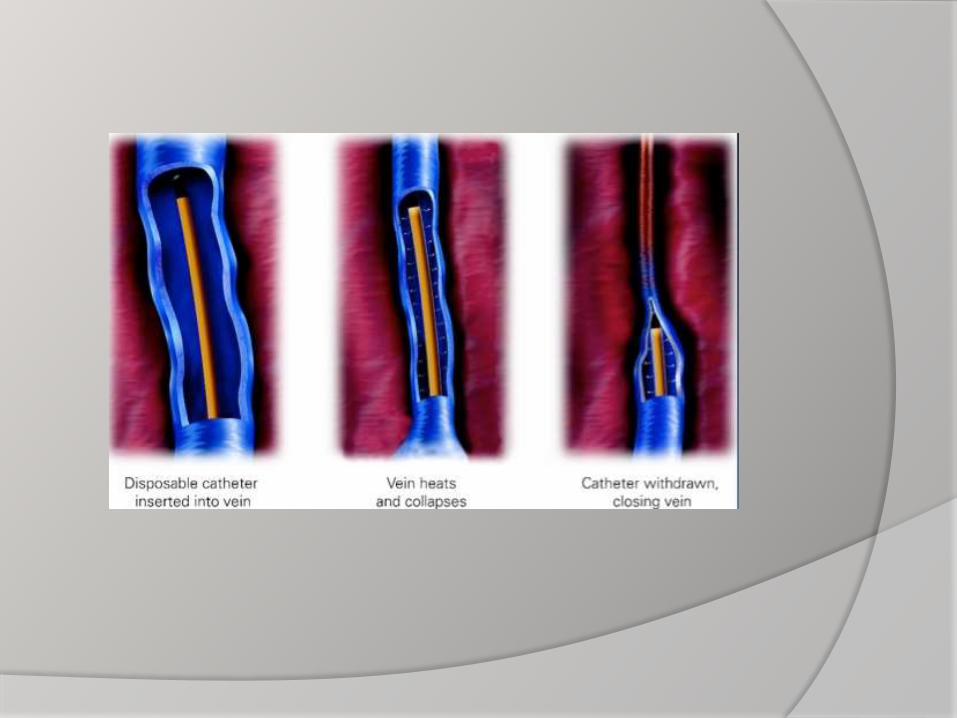
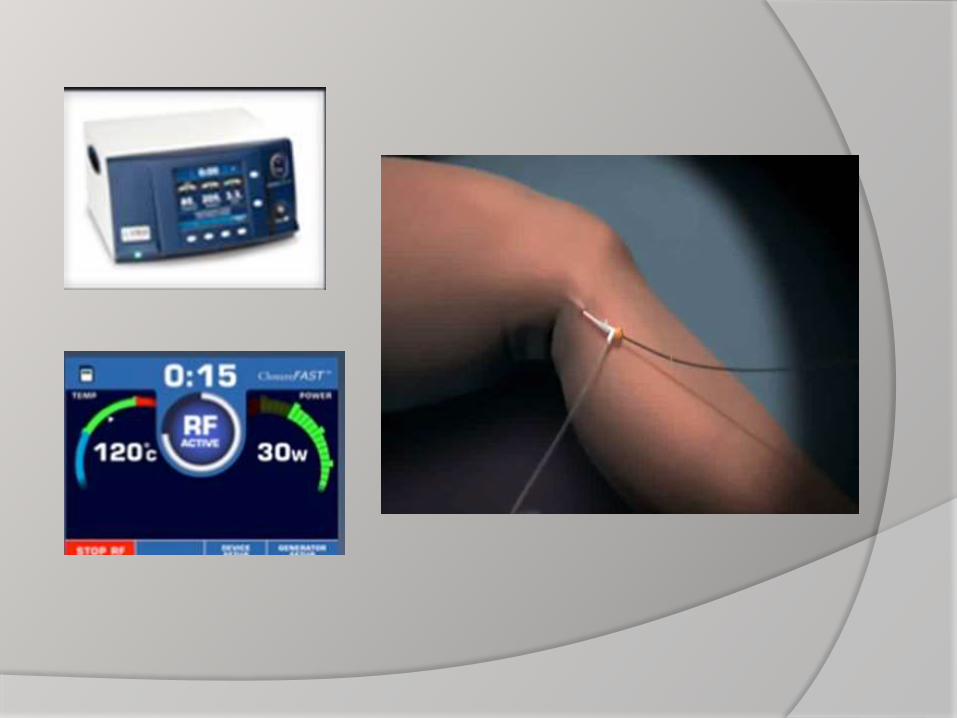
Radiofrequency ablation
therapy
By directing radiofrequency energy through a
vein, a narrow rim of tissue less than 1mm is
heated by an electrode.
The amount of heating is modulated using a
microprocessor resulting in controlled
collagen contraction, thermocoagulation and
absorption of the vein.


Endovenous laser ablation:
Initiates nonthrombotic occlusion by direct
thermal injury to vein wall causing
endothelial destruction, collagen
contraction and later fibrosis




Management by clinical category
No visible or palpable signs of
venous dis. (CEAP category 0):
- If C/O venous symptoms:
Treated conservatively
Telangiectasias and reticular veins
(CEAP category 1):
_ Asymptomatic patients with no
reflux: Treated by
- Sclerotherapy
- Laser light therapy
_ Symptomatic patients with reflux:
- Treat reflux first by surgical or
thermal ablation

Varicose veins (CEAP category 2):
_ Isolated varicosities without trunkal
reflux are treated by:
- Sclerotherapy
- Surgical excision
Depending on size, location and
number of affected veins
_ With reflux: Treated by vein ablation
Comparison of ablative therapies:
_ Recent studies reveal that minimally
invasive therapies are as effective as
surgical ablation with fewer
complications and rapid regain of daily
activities

Advanced venous disease:
_ Patients with edema, skin changes or
ulceration (CEAP categories C3, C4,
C5, C6: Treated by initial conservative
measures
_ Refractory patients to conservative
measures: Treated by ablative therapy

Summary and conclusion
Visibly dilated LL veins may indicate
underlying venous reflux, especially if
symptomatic, However, they can occur
in absence of symptoms or reflux
Duplex US is essential to identify
superficial, deep or perforator vein reflux
and R/O DVT
Patients with venous reflux and those
with complications should be referred to
venous or at least vascular specialist for
further evaluation and management
Goals of treatment are improved
symptoms and appearance
Most patients are treated by initial
conservative measures
Patients refractory to conservative
measures for 3 months with documented
reflux (>0.5 second duration) are
candidates for vein ablative therapy
Patients with telangiectasias, reticular
vein and VV with reflux should undergo
vein ablation before treating these
lesions
Telangiectasias, reticular veins and
small VV large enough to admit 27 or 30
gauge needle are treated best by
sclerotherapy with good results
Laser therapy is the only option for
telangiectasias too small to access,
allergy to sclerosants, patients afraid of
needles and after failed sclerotherapy
Endovenous ablation techniques are
preferred for saphenous and other
trunkal veins over surgical ablation
Persistent or recurrent perforators (by
duplex scan) after vein ablation are
treated by US-guided sclerotherapy or
endovenous methods
Occasionally, surgical methods may be
required for recurrent or refractory
venous ulceration