Varicella (Chickenpox) and Herpes Zoster (Shingles) Jennifer Zipprich Immunization Branch California...
52
Varicella (Chickenpox) and Herpes Zoster (Shingles) Jennifer Zipprich Immunization Branch California Department of Public Health October 17 th , 2012
Transcript of Varicella (Chickenpox) and Herpes Zoster (Shingles) Jennifer Zipprich Immunization Branch California...
Varicella (Chickenpox) and Herpes Zoster (Shingles)
Jennifer ZipprichImmunization Branch
California Department of Public HealthOctober 17th, 2012
Varicella-Zoster Virus (VZV)
• Human alpha-herpesvirus• Causes varicella (chickenpox) and herpes zoster
(shingles)• Primary VZV infection leads to chicken pox• VZV establishes latency in dorsal root ganglia
after primary infection• VZV can reactivate at a later time, causing
herpes zoster • There are 3 licensed vaccines to prevent varicella
(Varivax®, Proquad®) and herpes zoster (Zostavax®) in the US: Varivax® (licensed 1995) Proquad® (licensed 2005) Zostavax® (licensed 2006)

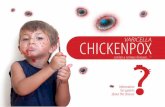
Varicella Clinical Features
• Incubation period 14-16 days (range 10-21 days)
• Mild prodrome for 1-2 days
• Rash generally appears first on head; most concentrated on trunk
• Successive crops over several days with lesions present in several stages of development
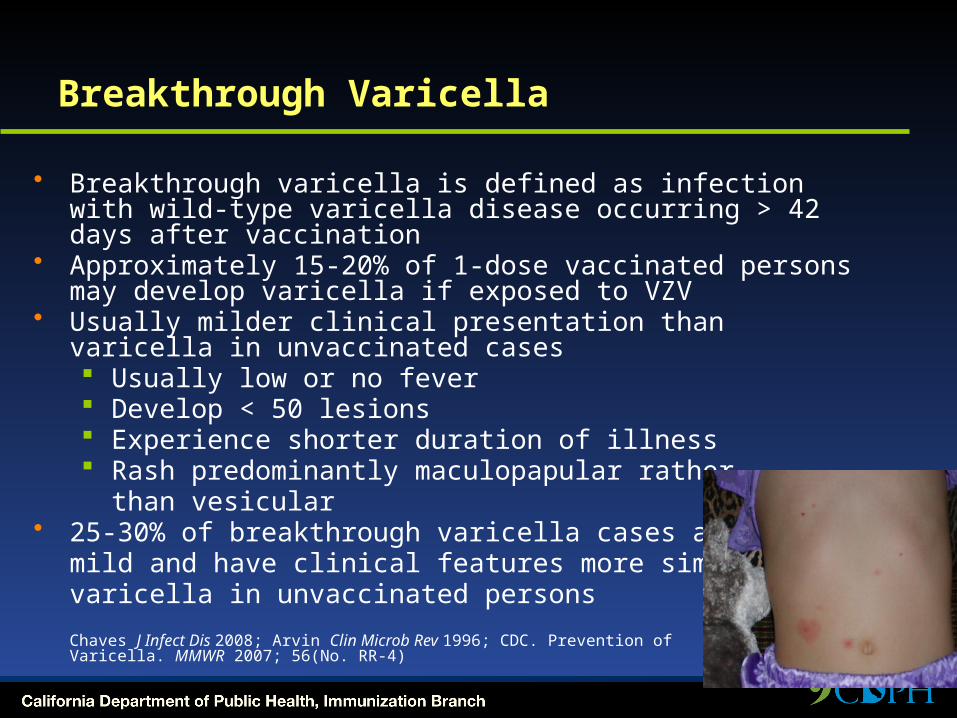
Breakthrough Varicella
• Breakthrough varicella is defined as infection with wild-type varicella disease occurring > 42 days after vaccination
• Approximately 15-20% of 1-dose vaccinated persons may develop varicella if exposed to VZV
• Usually milder clinical presentation than varicella in unvaccinated cases Usually low or no fever Develop < 50 lesions Experience shorter duration of illness Rash predominantly maculopapular rather
than vesicular• 25-30% of breakthrough varicella cases are not
mild and have clinical features more similar to varicella in unvaccinated persons
Chaves J Infect Dis 2008; Arvin Clin Microb Rev 1996; CDC. Prevention of Varicella. MMWR 2007; 56(No. RR-4)
Varicella: Complications
• Secondary bacterial infection of skin lesions• Central nervous system manifestations
(meningoencephalitis, cerebelllar ataxia)• Pneumonia (viral or bacterial)• Hepatitis, hemorrhagic complications,
thrombocytopenia, nephritis occur less frequently• Certain groups at increased risk for complications
Adults Immunocompromised persons Pregnant Women Newborns
CDC. Prevention of Varicella. MMWR 2007; 56(No. RR-4); Arvin Clin Microb Rev 19

Hemorrhagic Varicella

Varicella: Transmission
• Transmitted person to person by direct contact, inhalation of aerosols from vesicular fluid of skin lesions of acute varicella or zoster, or aerosolized respiratory tract secretions
• Period of contagiousness: 1-2 days before rash onset until all lesions crusted or disappear if maculopapular rash (typically 4-7 days)
• Varicella in unvaccinated persons is highly contagious (61-100% secondary household attack rate)
• Varicella in 1 dose-vaccinated persons half as contagious as unvaccinated cases
CDC. Prevention of Varicella. MMWR 2007; 56(No. RR-4); Arvin Clin Microb Rev 1996; Seward JAMA 2004; Vaccines, 5th edition
Herpes Zoster (Shingles)
• Following initial infection (varicella), VZV establishes permanent latent infection in dorsal root and cranial nerve ganglia
• Years to decades later VZV reactivates and spreads to skin through peripheral nerves causing pain and a unilateral vesicular rash in a dermatomal distribution
• ~1 million cases in the U.S. annually
Clinical Features of Herpes Zoster
Prodrome: headache, photophobia, malaise, fever, abnormal skin sensations and pain
Rash:• Unilateral, involving 1-3 adjacent dermatomes• Thoracic , cervical, ophthalmic involvement most
common• Initially erythematous, maculopapular• Vesicles form over several days, then crust over• Full resolution in 2-4 weeks• Occasionally, rash never develops (zoster sine
herpete)

Complications of Herpes Zoster
• Postherpetic Neuralgia (PHN) Pain ≥ 30 days occurs in 18-30% of zoster cases Mild to excruciating pain after resolution of rash Constant, intermittent, or triggered by trivial
stimuli May persist weeks, months or occasionally
years Can disrupt sleep, mood, work, and activities of
daily living and lead to social withdrawal and depression
Risk factors for PHN include age ≥ 50, severe pain before or after onset of rash, extensive rash, and trigeminal or ophthalmic distribution of rash
VZV Transmission from Zoster
• VZV can be transmitted from persons with zoster
• Risk of VZV transmission from zoster is much lower than from varicella
• Transmission is mainly through direct contact with zoster lesions, although airborne transmission has been reported in healthcare settings
• Localized zoster is only contagious after the rash erupts and until the lesions crust
• Transmission from localized zoster can be decreased by covering the lesions

Epidemiology

Varicella Disease Burden in the United States Before Introduction of Varicella Vaccine in 1995
• 4 million cases/year• 11,0000 - 13,500 hospitalizations/year• 100 - 150 deaths/year• Greatest disease burden in children
>90% cases 70% hospitalizations 50% deaths
Wharton Infect Dis Clin North Am 1996; Galil Pediatr Infect Dis J 2002; Davis Pediatrics 2004; Meyer J Infect Dis 2000; Nguyen NEMJ 2005

Varicella Immunization
• Varivax licensed in 1995• In 1995 American Academy of Pediatrics
recommended one dose of varicella vaccine for all children < 13, and for susceptible adolescents from 13-18
• In 1996 ACIP recommended vaccination for all children < 13 years of age; for susceptible adolescents and adults vaccination recommended for those at high risk of infection or complications. Vaccination of this group deemed desirable.
Pediatrics 1995;95;791. Committee on Infectious Diseases; ACIP. Prevention of Varicella. 1996.

Varicella Immunization
• One dose program estimated to save $5 for every $1 spent on vaccine when factoring in parental time lost from work and direct medical costs When medical costs were considered alone each chicken
pox case prevented would cost $2
• New Zealand – Total cost savings of $47 per child primarily driven by work-loss time averted
• Germany, Taiwan, Singapore

Varicella Immunization
• Cost-Benefit typically analyze one dose programs• Use of MMRV often not considered• Costs related to hypothetical increase in zoster
cases or increase in adult chicken pox cases not considered
• High risk groups a better target?• Number of concerns raised include: waning
immunity, potentially large pool of susceptible adults, serious complications rare
Newman. Arch Pediatr Adolesc Med 1998; Lieu. JAMA 1994; Ross. BMJ. 1995.
Varicella Active Surveillance Project (VASP)
• VASP is a CDC-funded project initiated in 1995 in Philadelphia and Los Angeles County
• Purpose of the active surveillance program To obtain population-based incidence rates for
varicella and herpes zoster diseases in a community with established high varicella vaccination coverage rates
to evaluate the impact of current and future varicella vaccination practices and policies
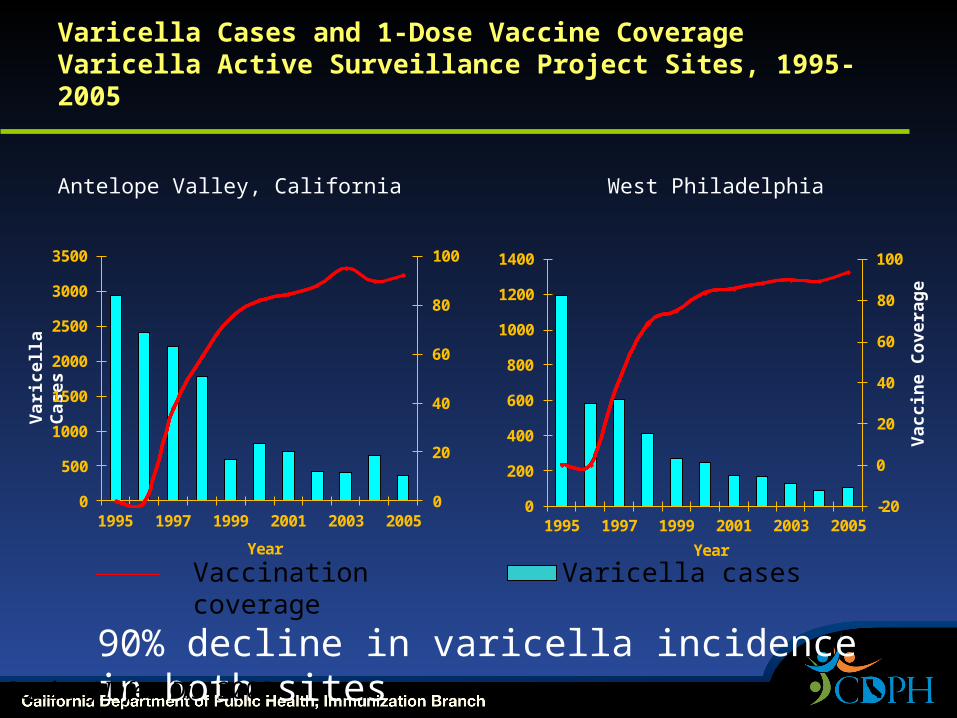
Varicella Cases and 1-Dose Vaccine CoverageVaricella Active Surveillance Project Sites, 1995-2005
Antelope Valley, California
0
20
40
60
80
100
0
500
1000
1500
2000
2500
3000
3500
1995 1997 1999 2001 2003 2005
Year
Var
icel
la C
ases
Vaccination coverage
West Philadelphia
-20
0
20
40
60
80
100
0
200
400
600
800
1000
1200
1400
1995 1997 1999 2001 2003 2005
Year
Vac
cin
e C
ove
rag
e
Varicella cases
90% decline in varicella incidence in both sitesGuris J Infect Dis 2008
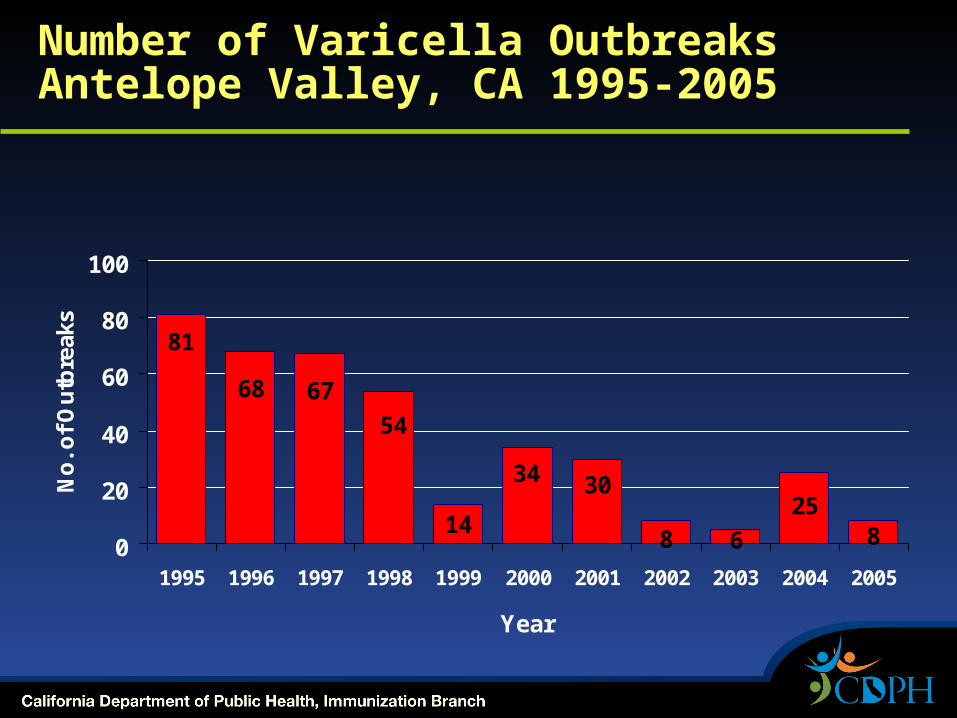
Number of Varicella OutbreaksAntelope Valley, CA 1995-2005
825
68
3034
14
54
6768
81
0
20
40
60
80
100
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
Year
No
. of
Ou
tbre
aks

Number of Varicella CasesAntelope Valley, CA 1995-2005
0
500
1000
1500
2000
2500
3000
3500
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
Year
No. of Case
s
Non-outbreak Cases Outbreak Cases

Length of Outbreaks (Days) and Age of Cases (Years)
1995-1998 2002-2005
Median Length 44.5 Days 30 Days
Median Age 6 Years 9 Years

Outbreak Cases: History of Disease or Vaccination and Disease Severity
1995-1998 2002-2005
History of prior varicella disease
6.3% 14%
Breakthrough cases 1.6% 58%
<50 Lesions 35% 45.7%
Complicated disease 9.3% 3.6%

Varicella and Measles Vaccine Coverage (1+ doses)*, Children 19-35 MonthsNational Immunization Survey, 1997-2008
26
43
58
6876
8185
88 88 89 90 91
0
10
20
30
40
50
60
70
80
90
100
Co
ve
rag
e (
%)
1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008
Year
Varicella
Measles
*National Immunization Survey (NIS), coverage available at http://www.cdc.gov/vaccines/stats-surv/default.htm#nis
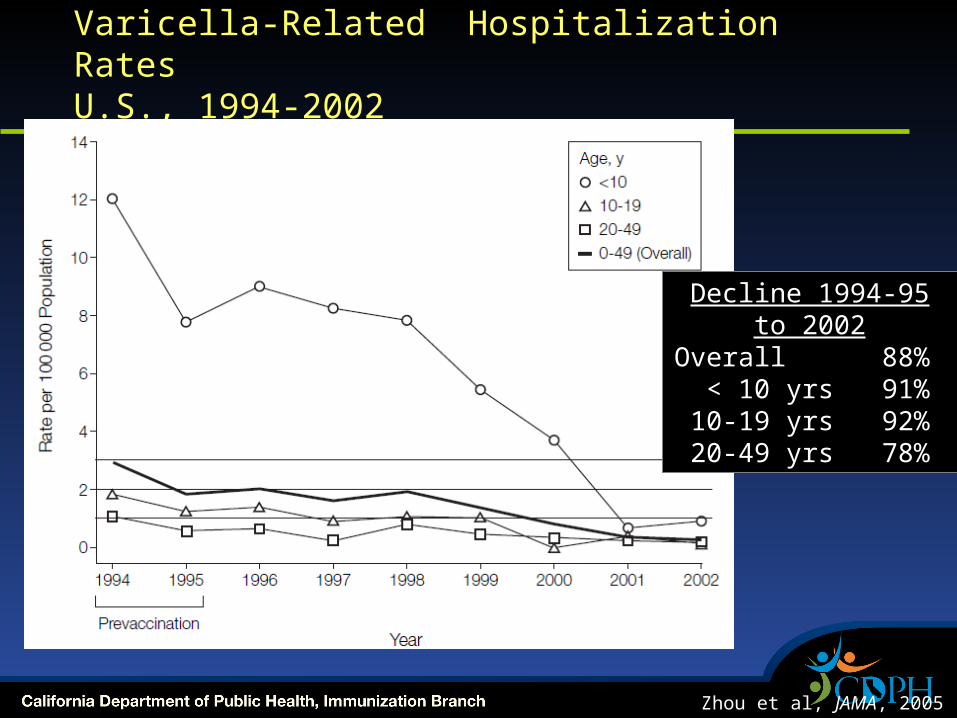
Varicella-Related Hospitalization RatesU.S., 1994-2002
Chart description of Varicella-Related Hospitalization Rates U.S. for 1994-2002. Rate per 100,000 Population. Prev-accination years of 1994, and 1995.Decline 1994-95 to 2002. Overall =88%.
<10 yrs = 91%. 10-19 yrs=92%.20-49 yrs= 78%.
Zhou et al, JAMA, 2005
Decline 1994-95 to 2002
Overall 88% < 10 yrs 91%10-19 yrs 92%20-49 yrs 78%
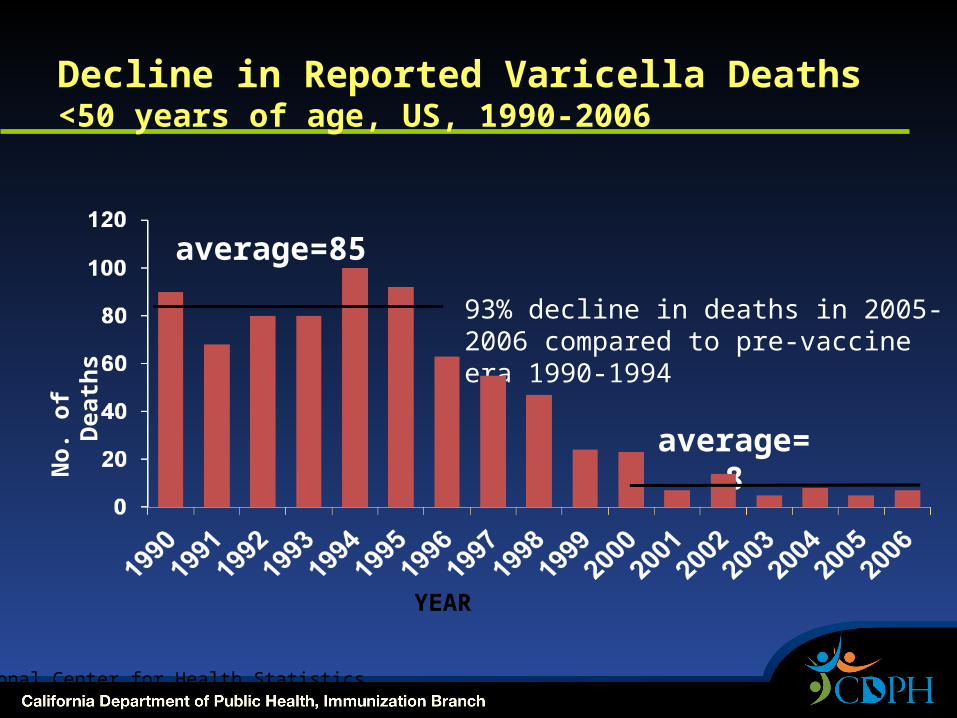
Decline in Reported Varicella Deaths <50 years of age, US, 1990-2006
No.
of
Death
s
average=85
93% decline in deaths in 2005-2006 compared to pre-vaccine era 1990-1994
average=8
YEAR
National Center for Health Statistics

Experience with 1-dose Varicella Vaccination Program
• 1-dose varicella vaccination coverage in 19-35 month-olds increased from 26% to 91% from 1997 to 2008
• Varicella disease incidence declined by 90% in two varicella active surveillance sites by 2005 as compared to 1995
• Varicella hospitalizations declined 88% during 1994-2002
• Varicella mortality rate declined 93% from 1990-1994 to 2005-2006 in persons aged <50 years
National Immunization Survey (www.cdc.gov/vaccines/stat-surv/default.htm#nis ); Guris J Infect Dis 2008; Marin Pediatrics 2008; Zhou JAMA 2005; National Center for Health Statistics

Post-licensure One-Dose Vaccine Effectiveness in US*
• 17 studies with 20 estimates Study designs: case-control, cohort (outbreaks,
other), household contact• Prevention all varicella
Median 85% (range 44% - 100%) Mean 81%
• Prevention of combined moderate and severe varicella Median 97% (range 86% - 100%) Mean
96%• Prevention of severe varicella*
Median 100% (range 97% to 100%)Mean 99%VARIVAX® Merck and Co. Inc; Seward J Infect Dis 2008

Impressive Achievements with the 1-Dose Varicella Vaccination Program But Challenges to Varicella Control Remained…
• 15-20% of children vaccinated with 1 dose remain at risk for varicella due to lack of immune response or partial protection
• Rationale for Timing of 2nd Dose of Varicella Vaccination at 4-6 Years of Age Low incidence among 1-4 year old children
Outbreaks in elementary and middle schools Similar immune response to 2nd dose with
intervals 3 months or 3-4 years after 1st dose Programmatic harmonization with MMR vaccine
and availability of MMRV vaccine

Current Varicella Vaccination Policy in the United States
Implemented routine 2-dose childhood varicella vaccination program in 2006 1st dose at age 12-15 months 2nd dose at age 4-6 years Effectiveness is 98% for
prevention of any primary varicella and 100% at prevention of severe disease
CDC. Prevention of Varicella. MMWR 2007; 56(No. RR-4)

Risk Factors for Herpes Zoster
• Increasing age• Immunosuppression
Bone marrow and solid organ transplantation Patients with hematological malignancies and
solid tumors HIV Immunosuppressive medications
• Gender: Increased risk in females • Race: Risk in African-American less than half that in
Caucasians• Trauma or surgery in affected dermatome• Early varicella (in utero, infancy): Increased risk of
pediatric zoster

Age-specific Incidence of Herpes Zoster and Postherpetic Neuralgia: U.K., 1947-1972
Hope-Simpson J R Coll Gen Pract 1975.
Varicella in California
Immunization Branch at CDPH
• Surveillance and disease reporting to CDC• Technical assistance to local health
jurisdictions• Educational materials• Laboratory testing (VRDL)

Varicella Reporting in California• Outbreaks • Hospitalizations• Deaths• HZ is not reportable
Varicella Outbreak Management• >=5 cases associated in time and place• Exclusion of cases while infectious• Provide immunization to susceptible
contacts• Provide VarzIG to high risk exposed
susceptible contacts (pregnant women)• Exclude susceptible exposed children in a
school setting?

Reported School Outbreaks in California
• Passively reported 2009: 31 outbreaks; Range 5 – 25 cases,
median 7 cases 2010: 17 outbreaks; range 5 – 55 cases,
median 7 cases 2011: 8 outbreaks; range 5 – 25 cases, median
7 cases• Many requests for technical assistance on
outbreak management are related to exclusion of exposed unvaccinated children from school
School Varicella Outbreak – October 2011
• Child in large unvaccinated family became infected with varicella (source unknown)
• All children in family and pregnant mother became infected with varicella over a five week period; mother quite ill
• Several siblings attend the same school and were the source of a school outbreak
School Varicella Outbreak
• School is K-8 with 208 students
• 66 (38%) students have PBEs
• 25 cases of varicella
• 17 (68%) of the cases have PBEs
• 2 cases had one dose of vaccine and one case had two doses
• 1 pregnant teacher exposed

California Law Granting Exclusion
• The California Health and Safety Code section 120365 states “…whenever there is good cause to believe that the person [with a personal belief exemption] has been exposed to one of the communicable diseases listed in subdivision (a) of Section 120325, that person may be temporarily excluded from the school or institution until the local health officer is satisfied that the person is no longer at risk of developing the disease.”
Pros of School Exclusion
• Theoretically may slow a varicella outbreak
• May reduce the number of infections and complications
• May decrease likelihood of varicella to spread to high-risk people
• May encourage parents to vaccinate children who would not otherwise be vaccinated
• “Proactive”
Cons of School Exclusion
• No data that exclusion is effective in slowing a varicella outbreak
• Immediate readmittance after vaccination may appear coercive
• Childcare costs for parents of excluded children could be substantial
• Long exclusion; children may suffer educationally
• School law affects cohorts of children differently
• Schools need to provide home education or risk losing attendance-based educational funds

Outbreak of rash illness in a skilled nursing facility
• 3 Residents• 4 employees• 1 visitor (husband of a resident)• Onset dates from 6/3/2012 – 6/21/2012• Ages ranged from 27 – 96 years• VZV source was suspected to be resident
with herpes zoster

Onset
Age Clinical Affiliation ResultVaricella Immune Status
6/18 40
lesions in various stages of development covering entire body and inside
mouth
Employee VZV detected IgG+ in 2008
6/19 65 Lesions; On chronic prednisone therapy
Husband of resident
VZV detected Presumed immune
based on age
6/19 40 Minimal lesions, all dry EmployeeVZV detected History of
disease
6/19 87 Typical lesions including vesicles
ResidentVZV detected
Presumed immune
based on age

Similar report in the literature
• Varicella transmission from HZ patient to 3 persons presumed immune in a long term care facility
• Secondary cases were clinically compatible with chicken pox – though mild, <100 lesions and confirmed by PCR
• Newly characterized varicella virus
Varicella Reinfection?
• Reinfection has been previously described but is rare Hall (2002) reviewed 9,947 varicella
cases and found that between 4.5% and 13.3% of cases reported a history of varicella infection
Case report on physician with prior evidence of serologic immunity
Varicella Death, 2010
• 41 yo male previously healthy• Presented with 5 days history of abdominal pain
and fever of 100.5• Presented to the ER the following day after
developing a generalized rash; discharged with acyclovir
• Developed mild delirium and difficulty breathing• Complications included encephalitis and hepatitis• Patient expired 9 days after admission

Varicella Death, 2007
• 13 month old previously healthy unvaccinated female
• Presented to ED with fever to 102 and vesicular rash; diagnosed with chicken pox
• Five days after rash onset patient became weak and unable to ambulate
• Admitted and administered IV acyclovir• Patient expired 6 days after rash onset
Questions?
Acknowledgements• Centers for Disease Control and
Prevention• Kathy Harriman• Teresa Lee• CDPH Immunization Branch
California School Immunization Law
• Immunization requirements at kindergarten entry: 4+ DTaP, 3+ polio, 2 MMR, 3 hepatitis B, 1
varicella
• Exemptions and procedure Permanent and Temporary Medical Personal Beliefs (PBE)
“shall be granted upon filing with the [school] a letter or affidavit from the pupil’s parent…that such immunization is contrary to his or her beliefs”
PBE Study – California, 2009
• Two-fold Purpose To evaluate vaccination status of kindergarten
PBEs Determine whether ‘high’ PBE schools were
different from ‘standard’ PBE schools• Method
Collected and analyzed PBE records from:a random sample of kindergartens andthe top 50 PBE kindergartens

Percent of Nonblank PBE Records Missing All Doses in Series
7.1
13.517.5
33.3
16.1
28.9 30.2
41.8
43.7
0
10
20
30
40
50
DTaP Polio Hep B MMR Var
RandomTop 50
% o
f P
BE
s
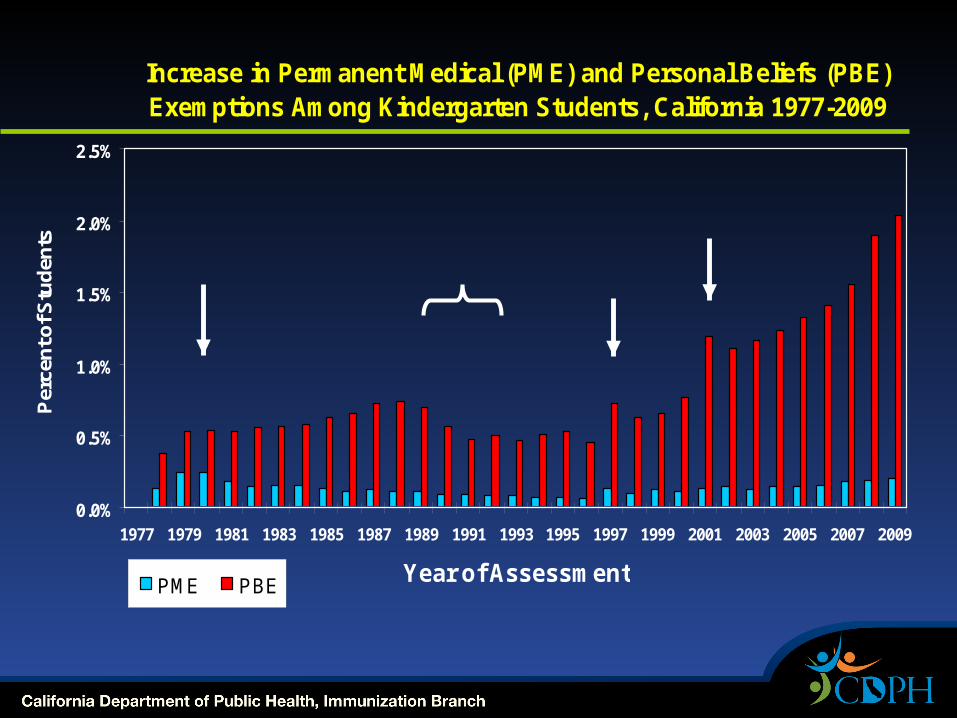
Increase in Permanent Medical (PME) and Personal Beliefs (PBE) Exemptions Among Kindergarten Students, California 1977-2009
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
1977 1979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003 2005 2007 2009
Year of Assessment
Per
cen
t of S
tud
ents
PME PBE
Measles, mumps and
rubella requirement
Hepatitis B requirement
Varicella requirementMeasles
outbreak