Valve-in-Valve Transcatheter Aortic Valve...
43
Valve-in-Valve Transcatheter Aortic Valve Implantation Michael A. Borger, MD PhD AATS Postgraduate Symposium Minneapolis, MN May 4, 2013
Transcript of Valve-in-Valve Transcatheter Aortic Valve...

Valve-in-Valve
Transcatheter Aortic Valve Implantation
Michael A. Borger, MD PhD
AATS Postgraduate Symposium
Minneapolis, MN
May 4, 2013

Disclosure
Speaking honoraria:
- Edwards Lifesciences
- St. Jude Medical
- Medtronic

Various Applications of ´Valve-in-valve´
TAVI in SAVR
TAVI in TAVI (bailout)
^ TVI in surgical MVR, PVR, TVR

Case Report
84 y.o. male with NYHA II – III:
- post-AVR 2008 (SJM Trifecta 23 mm)
- moderate AS, mod-to-severe AI
- diffuse atherosclerotic CAD
- pacemaker (DDD)
- COPD (FEV1 1.2L), former smoker
- obesity (BMI 38)
- Parkinson syndrome
- knee replacement 2010
- DVT post-knee replacement




Biological AVR (SJM Trifecta 23mm) with:
- leaflet thickening
- P max/mean 56/38mmHg
- EOA1.0 cm² (planimetry 1.1 cm²)
- mod-to-severe transvalvular AI
Case Report

Case Report
84 y.o. male with NYHA II – III:
- post-AVR 2008 (SJM Trifecta 23 mm)
- moderate AS, mod-to-severe AI
- diffuse atherosclerotic CAD
- pacemaker (DDD)
- COPD (FEV 1.4L), former smoker
- obesity (BMI 38)
- Parkinson syndrome
- knee replacement 2010
- DVT post-knee replacement
Options:
(1) Redo AVR
(2) Redo Bentall
(3) Medical management
(4) TAVR







Three Months Postop
• Good position and function of CoreValve:
– P max/mean 16/8 mm Hg,
– EOA 1.4 cm² (VTI 2.0 cm², LVOT 19 mm)
– no paravalvular leak, no AI
– EF 61%
• Improvement in symptoms (NYHA I-II)

20 30 40 50 60 70 80 90 years

VinV: from animal to FIM human
• recent trend towards bioprosthesis1
• expected durability 15-20 years2,3
• increasing life expectancy
1. AHA-Guidelines; Circulation 2006 2. Marchand; Ann Thorac Surg 2001
3. Borger; J Heart Valve Dis 2006
=> more elderly patients (comorbidities) with
degenerated bioprosthesis requiring redo procedures in
the future
- increased risk profile -

Structural Valve Degeneration
Pericardial: calcification,
impaired flexibility, stenosis
Porcine: calcification,
leaflet tear, insufficiency

V-in-V: Experimental animal studies

VinV: SAPIEN 23 in Perimount 21
first human transapical VinV 03/2007 in Leipzig (Perimount 21)

VinV: SAPIEN 23 in Perimount 21
first human transapical ViV implantation 2007 at our center
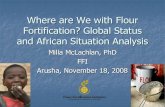
VinV: SAPIEN 26 in Hancock 25

VinV: SAPIEN 23 in Mosaic 21

VinV: SAPIEN 23 in Epic 21

Transapical V-in-V Leipzig experience

transapical V-in-V Leipzig experience
Kempfert et al., ATS 2010

VinV for degenerated aortic bioprosthesis
CE Perimount
mitral 25 mm
Edwards
SAPIEN 23 mm
Valve-in-a-Valve
(VinV)
+

Benchmark testing?
•Which valve in which valve
•Hemodynamic performance
•Measurements


Inner Diameters of Select Bioprostheses
Ferrari E EJCTS 2012;41:485-90

Valve-in-Valve Literature

Aortic V-in-V – Literature
Webb J et al. Circulation 2010

transapical V-in-V Leipzig experience

Residual gradient after
transapical aortic V-in-V (echo)
0
10
20
30
40
50
Leipzig experience
n=11
Vancoucer experience
n=10
maximal gradient
mean gradient
mmHg
Webb J et al. Circulation 2010; Kempfert et al. ARS 2010

Specific considerations
Azadani et al., ICVTS 2010

Technical considerations
Azadani et al., ICVTS 2010


Transfemoral (CoreValve) V-in-V

Transfemoral (CoreValve) V-in-V

Transfemoral (CoreValve) V-in-V

TAVI Valve-in-Valve
TAVI represents a good option for patients
with failing bioprosthetic valves
TAVI V-in-V can be achieved with low rates of
morbidity and mortality
Pre-procedure determination of optimal TAVI
valve size is crucial
TAVI V-in-V may justify lowering recommended
age for bioprosthetic AVR (at least 21 mm!)