Utility of high-resolution ultrasound for the diagnosis of dialysis-related amyloidosis
7
926 UTILITY OF HIGH-RESOLUTION ULTRASOUND FOR THE DIAGNOSIS OF DIALYSIS-RELATED AMYLOIDOSIS JONATHAN KAY, CAROL B. BENSON, SUSAN LESTER, JOSEPH M. CORSON, GERALDINE S. PINKUS, J. MICHAEL LAZARUS, and WILLIAM F. OWEN, JR. Objective. To evaluate the utility of real-time, high-resolution ultrasound of the shoulder in the diag- nosis of dialysis-related amyloidosis. Methods. We performed a case series study of 2 groups of patients seen at a referral-based clinic in a tertiary care hospital. The shoulders of 13 patients with normal renal function and of 38 patients receiving long-term hemodialysis were studied by real-time, high- resolution ultrasound. All hemodialysis patients were evaluated clinically for the presence of dialysis-related amyloidosis. Surgical specimens of joints were available for all 13 patients with normal renal function and for 17 of From the Departments of Rheumatology and Immunology, Radiology, Pathology, and Medicine, Brigham and Women’s Hos- pital, and the Departments of Medicine, Radiology, and Pathology, Harvard Medical School, Boston, Massachusetts. Supported by NIH grants AI-2253 I, AI-23401. AR-35907, AR-36308, and HL-36110, by a grant from the Peabody Foundation, and by a Postdoctoral Research grant from the Arthritis Foundation. Jonathan Kay, MD: Instructor in Medicine, Harvard Med- ical School, and Department of Rheumatology and Immunology, Brigham and Women’s Hospital; Carol B. Benson, MD: Associate Professor of Radiology, Harvard Medical School, and Department of Radiology, Brigham and Women’s Hospital; Susan Lester, MD, PhD: Clinical Fellow in Pathology, Harvard Medical School, and Department of Pathology, Brigham and Women’s Hospital; Joseph M. Corson, MD: Professor of Pathology, Harvard Medical School, and Department of Pathology, Brigham and Women’s Hospital; Geraldine S. Pinkus, MD: Associate Professor of Pathology, Har- vard Medical School, and Department of Pathology, Brigham and Women’s Hospital; J. Michael Lazarus, MD: Associate Professor of Medicine, Harvard Medical School, and Department of Medicine, Brigham and Women’s Hospital; William F. Owen, Jr., MD: Assis- tant Professor of Medicine, Harvard Medical School, and Depart- ment of Rheumatology and Immunology, Brigham and Women’s Hospital. Address reprint requests to Jonathan Kay, MD, Section of Rheumatology, Lahey Clinic Medical Center, 41 Mall Road, Burl- ington. MA 01805. Submitted for publication October 17, 1991; accepted in revised form March 2. 1992. the 38 hemdialysis patients. These specimens were eval- uated for the presence of &-microglobulin (P2m) amy- loid by Congo red and immunohistochemical staining. Results. Two ultrasonographic findings were se- lectively observed in the dialysis patients with clinical and histologic evidence of P2m amyloid in comparison with patients with normal renal function and no evi- dence of amyloid: rotator cuffs >8 mm in thickness and echogenic pads between muscle groups of the rotator cuff. The presence of at least 1 of these 2 findings corresponded to the presence of clinically and histolog- ically evident &rn amyloid with a sensitivity of 79% and a specificity of 100%. When additional patients without surgical specimens for histologic confirmation of amy- loidosis were included, the sensitivity of these 2 sono- graphic findings was 72% and the specificity was 97%. Conclusion, Real-time, high-resolution ultra- sound is a relatively sensitive and highly specific non- invasive adjunct to the clinical diagnosis of &m amyloid- osis in patients receiving long-term hemodialysis. In patients undergoing long-term dialysis, mus- culoskeletal complications may develop that manifest as an arthropathy involving the peripheral joints and/or spine (1,2). Shoulder pain and dysfunction, carpal tunnel syndrome, flexor tenosynovitis of the hands, and pain and soft tissue swelling of other large joints are often seen in patients who have had more than 5 years of dialysis (3-7). Congo red staining of involved areas of synovium and bone demonstrates amyloid deposits. Based on total amino acid content, N-terminal amino acid sequence, and immunochemi- cal determinants, &-microglobulin (&m) has been identified as the predominant component of these amyloid deposits (8,9). It has been suggested that Arthritis and Rheumatism, Vol. 35, No. 8 (August 1992)
-
Upload
jonathan-kay -
Category
Documents
-
view
212 -
download
0
Transcript of Utility of high-resolution ultrasound for the diagnosis of dialysis-related amyloidosis
926
UTILITY OF HIGH-RESOLUTION ULTRASOUND FOR THE DIAGNOSIS OF
DIALYSIS-RELATED AMYLOIDOSIS
JONATHAN KAY, CAROL B. BENSON, SUSAN LESTER, JOSEPH M. CORSON, GERALDINE S. PINKUS, J. MICHAEL LAZARUS, and WILLIAM F. OWEN, JR.
Objective. To evaluate the utility of real-time, high-resolution ultrasound of the shoulder in the diag- nosis of dialysis-related amyloidosis.
Methods. We performed a case series study of 2 groups of patients seen at a referral-based clinic in a tertiary care hospital. The shoulders of 13 patients with normal renal function and of 38 patients receiving long-term hemodialysis were studied by real-time, high- resolution ultrasound. All hemodialysis patients were evaluated clinically for the presence of dialysis-related amyloidosis. Surgical specimens of joints were available for all 13 patients with normal renal function and for 17 of
From the Departments of Rheumatology and Immunology, Radiology, Pathology, and Medicine, Brigham and Women’s Hos- pital, and the Departments of Medicine, Radiology, and Pathology, Harvard Medical School, Boston, Massachusetts.
Supported by NIH grants AI-2253 I , AI-23401. AR-35907, AR-36308, and HL-36110, by a grant from the Peabody Foundation, and by a Postdoctoral Research grant from the Arthritis Foundation.
Jonathan Kay, MD: Instructor in Medicine, Harvard Med- ical School, and Department of Rheumatology and Immunology, Brigham and Women’s Hospital; Carol B. Benson, MD: Associate Professor of Radiology, Harvard Medical School, and Department of Radiology, Brigham and Women’s Hospital; Susan Lester, MD, PhD: Clinical Fellow in Pathology, Harvard Medical School, and Department of Pathology, Brigham and Women’s Hospital; Joseph M. Corson, MD: Professor of Pathology, Harvard Medical School, and Department of Pathology, Brigham and Women’s Hospital; Geraldine S. Pinkus, MD: Associate Professor of Pathology, Har- vard Medical School, and Department of Pathology, Brigham and Women’s Hospital; J . Michael Lazarus, MD: Associate Professor of Medicine, Harvard Medical School, and Department of Medicine, Brigham and Women’s Hospital; William F. Owen, Jr., MD: Assis- tant Professor of Medicine, Harvard Medical School, and Depart- ment of Rheumatology and Immunology, Brigham and Women’s Hospital.
Address reprint requests to Jonathan Kay, MD, Section of Rheumatology, Lahey Clinic Medical Center, 41 Mall Road, Burl- ington. MA 01805.
Submitted for publication October 17, 1991; accepted in revised form March 2. 1992.
the 38 hemdialysis patients. These specimens were eval- uated for the presence of &-microglobulin (P2m) amy- loid by Congo red and immunohistochemical staining.
Results. Two ultrasonographic findings were se- lectively observed in the dialysis patients with clinical and histologic evidence of P2m amyloid in comparison with patients with normal renal function and no evi- dence of amyloid: rotator cuffs >8 mm in thickness and echogenic pads between muscle groups of the rotator cuff. The presence of at least 1 of these 2 findings corresponded to the presence of clinically and histolog- ically evident &rn amyloid with a sensitivity of 79% and a specificity of 100%. When additional patients without surgical specimens for histologic confirmation of amy- loidosis were included, the sensitivity of these 2 sono- graphic findings was 72% and the specificity was 97%.
Conclusion, Real- time, high-resolution ultra- sound is a relatively sensitive and highly specific non- invasive adjunct to the clinical diagnosis of &m amyloid- osis in patients receiving long-term hemodialysis.
In patients undergoing long-term dialysis, mus- culoskeletal complications may develop that manifest as an arthropathy involving the peripheral joints and/or spine (1,2). Shoulder pain and dysfunction, carpal tunnel syndrome, flexor tenosynovitis of the hands, and pain and soft tissue swelling of other large joints are often seen in patients who have had more than 5 years of dialysis (3-7). Congo red staining of involved areas of synovium and bone demonstrates amyloid deposits. Based on total amino acid content, N-terminal amino acid sequence, and immunochemi- cal determinants, &-microglobulin (&m) has been identified as the predominant component of these amyloid deposits (8,9). It has been suggested that
Arthritis and Rheumatism, Vol. 35, No. 8 (August 1992)

HIGH-RESOLUTION ULTRASOUND IN DIALYSIS AMYLOIDOSIS 927
amyloid composed of &m occurs mostly in the setting of long-term hemodialysis with cuprophane mem- branes (10,ll).
The diagnosis of dialysis-related amyloidosis is based on the presence of characteristic symptoms and signs in a patient who has had long-term dialysis and is confirmed by histologic evaluation of involved tissue (12). Shoulder pain occurs in as many as 95% of patients with dialysis-related amyloidosis (5) and is often the initial musculoskeletal symptom in this dis- ease (13). In pursuit of a noninvasive means of estab- lishing the diagnosis of dialysis-related amyloidosis, we evaluated the utility of real-time, high-resolution ultrasound in characterizing unique ultrasonographic abnormalities in the shoulders of patients who have undergone long-term hemodialysis.
PATIENTS AND METHODS Patients. The control group (group I) consisted of 13
patients with miscellaneous rheumatologic and orthopedic disorders but with normal renal function. All 13 had under- gone shoulder ultrasonography at the Brigham and Women’s Hospital, and all had surgical specimens from joints avail- able for histologic examination. Their musculoskeletal diag- noses were as follows: rotator cuff tear (n = 4), osteoarthritis (n = 31, impingement syndrome of the shoulder (n = 2), polymyalgia rheumatica (n = l ) , rheumatoid arthritis (n = l), avascular necrosis of the humeral head (n = I ) , and acetab- ular labrum tear (n = 1).
Shoulders of 38 long-term hemodialysis patients with shoulder pain, recruited from the hemodialysis centers affil- iated with the renal division at the Brigham and Women’s Hospital, were also studied by ultrasound. All hemodialysis patients were undergoing routine dialysis with cuprophane membranes. All hemodialysis patients were evaluated clini- cally by at least 2 of the authors (JK, JML, WFO) for the presence of dialysis-related amyloidosis. Criterion for the clinical diagnosis of dialysis-related amyloidosis was the presence of at least 2 of the following findings: flexor tenosynovitis of the hands with diminished extension of the fingers, signs or symptoms of carpal tunnel syndrome, and shoulder pain with diminished range of shoulder motion (12).
Eighteen of the dialysis patients had clinical evidence of dialysis-related amyloidosis (group 11), and the remaining 20 did not (group 111). Biopsy specimens for pathologic evaluation for the presence of pzm were available from previous orthopedic surgical procedures in 14 of the 18 patients in group I1 (group IIa) and in 3 of the 20 patients in group I11 (group IIIa).
Pathologic studies. For histologic characterization of the pathologic specimens, formalin-fixed, paraffin-embedded tissue sections were prepared from surgical specimens ob- tained from the shoulders (n = 5) , hip (n = 2), knees (n = 21, ankles (n = 2), rotator cuff (n = l), and toes (n = 1) of the patients in group I. In the 17 patients in groups IIa and IIIa, biopsy specimens for analysis for the presence of a m were
from the shoulder (n = 11, hips (n = 6), wrists (n = 7), knees (n = 2), and rotator cuff (n = 1). Surgical specimens from joints were not available for study in the remaining 4 patients with clinical evidence of dialysis-related amyloidosis (group IIb) or the remaining 17 patients who lacked clinical evi- dence of amyloidosis (group IIIb).
Tissue sections from patient groups I, IIa, and IIIa were stained with hematoxylin and eosin and Congo red (14), and immunohistochemical studies of serial sections were performed using the peroxidaseantiperoxidase technique (15). Rabbit anti-human p2m polyclonal antibody (Dako, Carpinteria, CA) at a final dilution of 1 :200 was utilized as the primary antiserum, and nonimmune rabbit antiserum was used as a control. A histologic diagnosis of &m amy- loidosis was made if characteristic amyloid deposits, dem- onstrating apple-green birefringence when Congo red- stained sections were visualized under polarized light, were present and if these deposits were immunoreactive with polyclonal rabbit anti-human a m .
None of the specimens from the 13 patients in group I had amyloid demonstrated by Congo red staining, and immunoperoxidase staining revealed only occasional endo- thelial staining. In contrast, &m amyloid deposits were present in the capsular and subsynovial tissues from all 14 patients from group IIa. Amyloid was not demonstrated by either Congo red or immunoperoxidase staining in any of the specimens from the 3 patients in group IIIa.
Ultrasonographic studies. Shoulders of all patients were evaluated, without knowledge of the patient’s clinical or histologic findings, by real-time, high-resolution ultra- sound using a 5-MHz or 7.5-MHz linear transducer (16). Anterior (region of the pectoralis muscles) to posterior (region of the teres muscles) scanning of the shoulders was performed in both transverse and longitudinal planes, and the results were recorded. On the transverse view, the thickness of the rotator cuff was measured in the region of the supraspinatus muscle, which was the point of greatest thickness. The locations and sizes of areas of altered echo- genicity were recorded.
Statistical analysis. For analysis of the sensitivity and specificity of real-time, high-resolution ultrasound of the shoulder in the diagnosis of amyloidosis, we first considered only patients who either had amyloidosis established on the basis of histologic examination of a surgical specimen (group IIa) or who had amyloidosis excluded because of the ab- sence of histologic evidence (groups I and IIIa). A positive finding on ultrasound was defined as the presence of a rotator cuff >8 mm in thickness and/or an echogenic pad of material between the muscle layers of the rotator cuff. Sensitivity was expressed as the proportion of patients with biopsy evidence of amyloidosis (group IIa) who had a positive ultrasound result. Specificity was defined as the proportion of patients who did not have amyloidosis dem- onstrated by histologic analysis (groups I and IIIa) who had a negative ultrasound result. Additional analyses of sensitiv- ity and specificity, using clinical criteria for the diagnosis of amyloidosis, were performed by including patients in groups IIb and IIIb. Univariate analyses of differences in age and duration of hemodialysis were performed using Student’s t-test (17).

KAY ET AL
Table 1. Characteristics of the patients by group
Group*
I I1 Ira Ilb 111 IIIa lI lb
No. of patients 13 18 14 4 20 3 17 Maleslfemales 419 6/12 519 113 8/12 013 819 Age, mean f SD years 62.6 f 18.4 57.8 f 11.2 57.4 -t 11.8 59.3 f 10.2 54.7 f 16.5 59.3 5 11.2 53.9 f 17.4 Duration of hemodialysis, - 14.3 2 4.0t 15.0 f 4.2 11.8 f 2.4 8.2 f 5.5t 6.7 5 7.4 10.0 f 5.3
mean f SD years ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~~~ ~~~~~~~~~
* Group 1 = patients with normal renal function (control); group I1 = hemodialysis patients with amyloidosis; group IIa = group I1 patients with clinical and histologic evidence of amyloidosis; group Ilb = group I1 patients with clinical evidence of amyloidosis but with no surgical specimens available for histologic study; group 111 = hemodialysis patients without amyloidosis; group IlIa = group Il l patients with no clinical or histologic evidence of amyloidosis; group l l lb = group 111 patients with no clinical evidence of amyloidosis but with no surgical specimens available for histologic study. t P < 0.001.
RESULTS Patient characteristics. The clinical and his-
tologic characteristics of the 3 patient groups are summarized in Table I . The mean ages were 62.6 years for the patients with normal renal function (group I) and 57.8 years and 54.7 years, respectively, for the patients with (group XI) and without (group 111) amy- loidosis (P > 0.2 for all pairwise comparisons). How- ever, the patients with amyloidosis had been receiving dialysis for a significantly longer period of time than those without amyloidosis (mean k SD 14.3 ? 4.0 years [n = 181 versus 8.2 4 5.5 years [n = 201) (P < 0.001).
Ultrasonographic findings. Six of the 13 patients with normal renal function had normal findings on ultrasound. Several sonographic abnormalities were noted in the shoulders of the remaining 7 patients in this group. These consisted of either focal or diffuse thinning of the rotator cuff to 4 3 mm (normal 4-8 mm), focal areas of increased echogenicity, and abnormal fluid collections (Table 2).
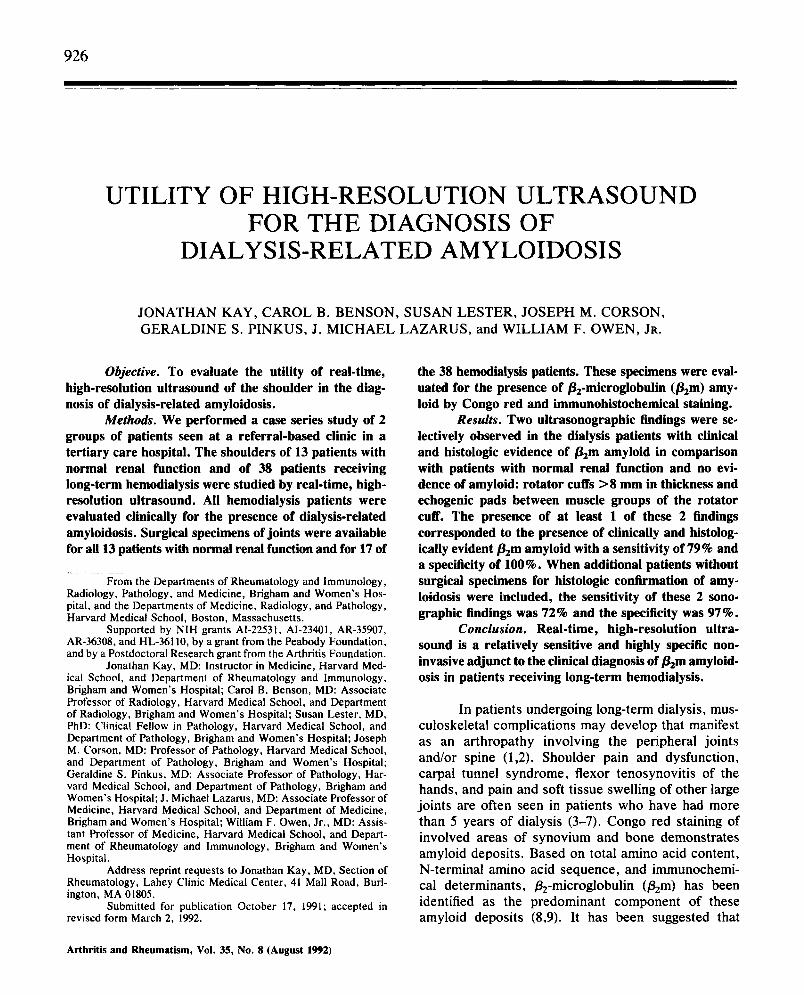
In all 14 patients with clinical and histologic evidence of amyloidosis, abnormalities were exhibited on shoulder ultrasound. The observed abnormalities were rotator cuff thickness >8 mm (Figure I), echo- genic pads of material between the muscle layers (Figure 2), focal areas of increased echogenicity within the rotator cuff, focal or diffuse thinning of the rotator cuff to 1 3 mm in thickness, irregularity of the humeral head, and abnormal fluid collections around the joint (Table 2). All 4 hemodialysis patients with dialysis- related amyloidosis by clinical diagnosis only also had abnormal results on shoulder ultrasound, including rotator cuffs >8 mm in thickness, echogenic pads,
focal areas of increased echogenicity in the rotator cuff, diffuse thinning of the rotator cuff, irregularity of the humeral head, and abnormal fluid collections around the joint (Table 2).
Two of the 3 hemodialysis patients with no clinical or histologic evidence of amyloidosis had abnormalities on shoulder ultrasound. The abnormal- ities were focal areas of increased echogenicity within the rotator cuff, diffuse thinning of the rotator cuff, irregularity of the humeral head, and abnormal fluid collections around the joint. Of the 17 hemodialysis patients without clinical evidence of dialysis-related amyloidosis in whom histologic analysis was not per- formed, sonographic abnormalities were observed in 8. These consisted of focal or diffuse thinning of the rotator cuff, irregularity of the humeral head, abnor-
Table 2. Findings on shoulder ultrasonography
Patient group (n)* Ultrasonographic
finding I (13 ) IIa (14) IIb (4) llIa (3) IIIb (17)
Normal Rotator cuff >8 mm Echogenic pad Irregular humeral head Rotator cuff >8 mm
andor echogenic pad Increased echogenicit y
in rotator cuff Focal thinning of
rotator cuff ( 5 3 mm) Diffuse thinning of
rotator cuff ( 5 3 mm) Abnormal fluid
collections
6 0 0 0 10 2 0 4 1 0 1 1 0 11 2
2 8 2
4 1 0
3 1 3
2 3 I
0
2
1
3
I
I
* Values are the number of patients.

HIGH-RESOLUTION ULTRASOUND IN DIALYSIS AMYLOIDOSIS 929
osis were broadened to include clinical features with- out histologic confirmation, the sensitivity was 13/18 (72%) and the specificity was 32/33 (97%) (Figure 3).
Subcutaneous
Humerai head A
A
B Figure 1. A, Diagram of tissue layers as imaged on transverse ultrasound of the normal shoulder. The rotator cuff tendon is a homogeneous band of tissue overlying the humeral head, deep to the deltoid muscle and subcutaneous tissue. (Reproduced, with permis- sion, from Bretzke CA, Crass JR, Craig EV, Feinberg SB: Ultra- sonography of the rotator cuff: normal and pathologic anatomy. Znvesrigative Radiology 20:311-315, 1985.) B, Transverse sonogram showing a thickened rotator cuff tendon in a patient with histologi- cally proven penarticular amyloidosis. The thickness of the rotator cuff (RC) is 12 mm (calipers). The deltoid muscle (D) is displaced by the thickened rotator cuff tendon. H = humeral head; SC = subcutaneous tissue.
ma1 fluid collections around the joint, and nonvisual- ization of the biceps. In 1 of these 8 patients, an echogenic pad was seen over the rotator cuff of 1 shoulder.
The diagnostic sensitivity and specificity of a rotator cuff >8 mm in thickness and/or the presence of an echogenic pad, in relation to histologically diag- nosed amyloidosis, were 11/14 (79%) and 16/16 (100%), respectively. When the criteria for amyloid-
B Figure 2. Echogenic pads in patients with histologically proven periarticular amyloidosis. A, Transverse oblique sonogram of the anterior rotator cuff showing 2 echogenic pads (EP) on either side of the subscapularis tendon (straight arrows) of the rotator cuffnear its insertion on the lesser tuberosity of the humeral head (H). B, Transverse sonogram showing an echogenic pad of 8 x 18 mm (calipers) between subcutaneous tissue (SC) and the rotator cuff (RC).

930 KAY ET AL
Patients with histologic di.gnos*
Positive Negative
BCmlcrogl&ilin amyldd praent (Croup 11’)
Bpnicmglobulin amyloid absent
(Groups 1. 11P)
Sensitivity - 79%
Specifidty = 100%
All patients
CIINICAL DIAGNOSIS UlrruavRo
No amyloidosis (Gmups I, 1118, I I P )
Sensitivity = 12%
Spesilidiy = 97%
Figure 3. Sensitivity and specificity of high-resolution ultrasound for the diagnosis of dialysis-related amyloidosis.
DISCUSSION Shoulder pain is common among hemodialysis
patients, most often arising from tendinitis, bursitis, rotator cuff tears, and amyloidosis. However, gout, pseudogout, infections, and hyperparathyroidism must also be considered in the differential diagnosis (18-20). Typically, the history, physical examination, and laboratory data do not permit a clear distinction among these disorders.
Real-time, high-resolution ultrasound is a sen- sitive imaging technique for evaluation of select patho- logic conditions involving the biceps, rotator cuff tendons, and subdeltoid bursa of the shoulder (16). Disorders that can be diagnosed by high-resolution ultrasound of the shoulder include rupture of the
biceps tendon, excessive fluid in the bursa, and rotator cuff tendinitis, tears, and atrophy.
High-resolution ultrasonography of the shoul- ders of hemodialysis patients with and without clinical and histologic evidence of dialysis-related amyloidosis revealed numerous abnormalities. In comparison with patients who had normal renal function (group I), 2 findings were selectively observed in the dialysis pa- tients who had clinical and histologic evidence of amyloid (group 1Ia): 71% demonstrated greatly in- creased rotator cuff thickness and 29% exhibited the presence of an echogenic pad between muscle groups. At least 1 of these findings was observed in 79% of the patients in group IIa. Analysis of the diagnostic sensi- tivity of a thickened rotator cuff and an interposed echogenic pad was extended to include hemodialysis patients who had only a clinical diagnosis of dialysis- related amyloidosis (group IIb). A thickened rotator cuff was observed in 67% of the patients with his- tologic and/or clinical evidence of amyloidosis (groups IIa and IIb combined), and an echogenic pad was observed in 28% of these patients. At least 1 of these sonographic findings was seen in 72% of the hemo- dialysis patients with amyloidosis.
In the remaining group I1 patients with clinical amyloidosis but without either of the above-described sonographic findings, rotator cuffs 5 3 mm in thick- ness, compatible with tears or atrophy, were noted. Humeral head irregularities, which were observed in hemodialysis patients with or without amyloidosis, may represent erosive changes of the humeral head resulting from inflammatory arthropathy or metabolic bone disease.
Thus, the sonographic findings of a maximal rotator cuff thickness >8 mm or the presence of a pad of echogenic material interposed between muscle lay- ers of the rotator cuff have 72-79% sensitivity in the diagnosis of amyloidosis. In contrast, these sono- graphic findings were observed in only 0-3% of the patients without amyloidosis, indicating a specificity of 97-100%. These results indicate that high-resolution ultrasound is a useful, noninvasive technique for diag- nosis of dialysis-related amyloidosis.
Dialysis-related amyloidosis typically presents with a polyarticular distribution (12). Thus, it is not surprising that sonographic abnormalities in the shoul- der are predictive of diagnostic pathologic findings in other joints. The ultrasonographic findings of in- creased echogenicity in the rotator cuff, focal or diffuse thinning of the rotator cuff to 5 3 mm, irregu- larity of the humeral heads, or abnormal fluid collec-

HIGH-RESOLUTION ULTRASOUND IN DIALYSIS AMYLOIDOSIS 93 1
tions were of little use in the diagnosis of amyloidosis in the patients studied.
The present study has potential limitations. The ultrasonographic testing was performed at a single academic medical center, and the population of dialy- sis patients may not be representative of those at other institutions. Selection bias was present because dialy- sis patients were referred for evaluation of shoulder pain. The number of patients studied was small, and the estimates of sensitivity and specificity would be more precise if the sample size were larger. Further investigations will be needed to generalize our find- ings. However, the principal results were derived using patients who did have a definitive histologic diagnosis of &m amyloidosis.
Although surgical specimens available for pathologic analysis for the presence of &m were from joints other than the shoulder or rotator cuff in 12 of the 14 patients in group IIa, the presence of &m amyloid in musculoskeletal tissue in a dialysis patient with shoulder pain suggests involvement of the shoul- der. There is, however, a slight possibility that the changes detected by ultrasonography do not represent amyloid deposits. Because of its superior imaging properties and our greater experience with visualizing pathologic conditions in the shoulder, ultrasonography was limited to this joint as a representative joint involved in dialysis-related amyloidosis. Ultrasono- graphic examination of the shoulder was performed by an ultrasonographer who was unaware of the patients' clinical or histologic evaluations. The observations were extended to those patients whose diagnosis was based on an ad hoc clinical definition with little change in either sensitivity or specificity, but we recognize that this extended observation has not been validated against a definitive standard.
Previous studies have utilized ultrasonography of the hips and knees to evaluate synovial thickness in patients undergoing long-term hemodialysis (21,22). However, the investigators did not correlate their findings with synovial histologic analyses, nor did they define levels of sensitivity or specificity. In an analo- gous manner to the present investigation, real-time, high-resolution 2-dimensional echocardiography has been utilized as a noninvasive tool for diagnosing myocardial infiltration in patients with primary amy- loidosis. Depending on the ultrasonographic criteria used, the sensitivity of this test is 6047% and the specificity is 81-100% (23), comparable with the sen- sitivity and specificity observed using ultrasound of the shoulder to diagnose dialysis-related amyloidosis. Results similar to ours were observed in a recent
investigation using conventional ultrasonography of the shoulder, but fewer patients were studied and the presence of &m amyloid deposits was not confirmed by immunohistochemical studies (24).
Based on these findings, high-resolution ultra- sound is a relatively sensitive and highly specific noninvasive method that can be used as an adjunct to clinical diagnosis of amyloidosis in patients undergo- ing long-term hemodialysis. The technique will have to be studied prospectively in larger numbers of patients to determine its capacity to detect amyloidosis both in asymptomatic individuals and individuals with early disease. It should prove to be a useful tool for assess- ing the efficacy of therapeutic interventions used to treat the &m deposition characteristic of this disorder.
ACKNOWLEDGMENTS The authors thank Dr. Jeffrey N. Katz for his helpful
comments, Sttphanie Bourdelle for excellent manuscript preparation, and the Massachusetts General Hospital and the New England Deaconess Hospital for providing paraffin blocks of some surgical specimens.
REFERENCES 1. Bardin T, Kuntz D, Zingraff J, Voisin M-C, Zelmar A,
Lansaman J: Synovial amyloidosis in patients undergo- ing long-term hemodialysis. Arthritis Rheum 28: 1052- 1058, 1985
2. Kuntz D, Naveau B, Bardin T, Drueke T, Treves R. Dry11 A: Destructive spondylarthropathy in hemodia- lyzed patients: a new syndrome. Arthritis Rheum 27: 369-375, 1984
3. Warren DJ, Otieno LS: Carpal tunnel syndrome in patients on intermittent haemodialysis. Postgrad Med J 51:450-452, 1975
4. Assenat H, Calemard E, Charra B, Laurent G, Terrat JC, Vane1 T: Htmodialyse: syndrome du canal carpien et substance amyloi'de (letter). Nouv Presse Med 9:1715, 1980
5 . Laurent G, Calemard E, Charra B: Dialysis-related amyloidosis. Kidney Int 33 (Suppl):S-32-S-34, 1988
6. Muhoz-Gbmez J, BergadB-Barado E, G6mez-Perez R, Llopart-BuisBn E, Subias-Sobrevia E, Rotts-Querol J , Solt-Arquts M: Amyloid arthropathy in patients under- going periodical haemodialysis for chronic renal failure: a new complication. Ann Rheum Dis 44:729-733, 1985
7. Durroux R, Benouaich L, Bouissou H, Mansat M, Clanet M: Ttnosynovite du canal carpien et dtp6ts amyloides chez les insuffisants rknaux chroniques htmo- dialyses (letter). Nouv Presse Med 10:45, 1981
8. Gejyo F, Yamada T, Odani S, Nakagawa Y, Arakawa M, Kunitomo T, Kataoka H, Suzuki M, Hirasawa Y, Shirahama T, Cohen AS, Schmid K: A new form of

932 KAY ET AL
amyloid protein associated with chronic hemodialysis was identified a s beta 2-microglobulin. Biochem Biophys Res Commun 129:701-706, 1985
9. Shirahama T, Skinner M, Cohen AS, Gejyo F, Arakawa M, Suzuki M, Hirasawa Y: Histochemical and immuno- histochemical characterization of amyloid associated with chronic hemodialysis as beta 2-microglobulin, Lab Invest 53:705-709, 1985
10. Vandenbroucke JM, Jadoul M, Maldague B, Huaux JP, Noel H, van Ypersele de Strihou C: Possible role of dialysis membrane characteristics in amyloid osteo- arthropathy (letter). Lancet 1:1210-1211, 1986
11. Chanard J, Lavaud S, Toupance 0, Roujouleh H, Melin 3-P: Carpal tunnel syndrome and type of dialysis mem- brane used in patients undergoing long-term hemodialy- sis (letter). Arthritis Rheum 29:1170-1171, 1986
12. Owen WF: Erosive spondyloarthropathy in a long-term chronic hemodialysis patient. Semin Dial 2:85-88, 1989
13. Chattopadhyay C, Ackrill P, Clague RB: The shoulder pain syndrome and soft-tissue abnormalities in patients on long-term haemodialysis. Br J Rheumatol 26: 181- 187, 1987
14. Puchtler H, Sweat F, Levine M: On the binding of Congo red by amyloid. J Histochem Cytochem 10:355- 364,1962
15. Pinkus GS, Said JW: Specific identification of intracel- Mar immunoglobulin in paraffin sections of multiple myeloma and macroglobulinemia using an immunoper- oxidase technique. Am J Pathol 87:47-58, 1977
16. Benson CB: Sonography of the musculoskeletal system. Rheum Clin North Am 17:487-504, 1991
17. Colton T: Statistics in Medicine. Boston, Little, Brown & Co., 1974
18. Llach F, Pederson JS: Acute joint syndrome (AJS) and maintenance hemodialysis (HD). Proc Clin Dial Trans- plant Forum 9:17-22, 1979
19. Massry SG, Bluestone R, Klinenberg JR, Coburn JW: Abnormalities of the musculoskeletal system in hemo- dialysis patients. Semin Arthritis Rheum 4:321-349, 1975
20. Wright RS, Mehls 0, Ritz E, Coburn JW: Musculoskel- etal manifestations of chronic renal failure, dialysis, and transplantation, The Kidney and Rheumatic Disease. Edited by PA Bacon, NM Hadler. London, Butter- worth, 1982
21. Laurent G, Charra B, Calemard E, Uzan M, Vane1 T, Terrat JC, Pracros JP: Mesure Bchographique de I’Cp- aississement synovial de la hanche: inttret dans I’eval- uation de I’arthropathie des dialyses. Presse Med 18: 939, 1989
22. Gielen JL, van Holsbeeck MT, Hauglustaine D, Veer- resen L, Verbeken E, Baert AL, Meens L, Vande- voorde P, Michielsen P, Coral A: Growing bone cysts in long-term hemodialysis. Skeletal Radio1 19:43-49, 1990
23. Falk RH, Plehn JF, Deering T, Schick EC Jr, Boinay P, Rubinow A, Skinner M, Cohen AS: Sensitivity and specificity of the echocardiographic features of cardiac amyloidosis. Am J Cardiol 59:41W22, 1987
24. McMahon LP, Radford J, Dawborn JK: Shoulder ultra- sound in dialysis related amyloidosis. Clin Nephrol 35~227-232, 1991