
Using Xpert to discontinue airborne isolation The ... - Shah - Use of PCR-based... · Using Xpert...
57
Using Xpert to discontinue airborne isolation – The Consensus Statement Neha Shah, MD MPH Tuberculosis Control California Department of Public Health Centers for Disease Control and Prevention NAR February 2017
Transcript of Using Xpert to discontinue airborne isolation The ... - Shah - Use of PCR-based... · Using Xpert...

Using Xpert to discontinue airborne isolation –
The Consensus Statement
Neha Shah, MD MPH
Tuberculosis Control
California Department of Public Health
Centers for Disease Control and Prevention
NAR February 2017

Disclosures
• No affiliation or financial relationship with any of the tests or companies mentioned in this presentation
• This presentation does not necessarily represent the official position of the US Centers for Disease Control and Prevention

3
guidelines

4

Removing Patients from A.I.I.
• Infectious TB disease is considered unlikely AND
EITHER
– another diagnosis explains the clinical syndrome
OR
– 3 consecutive, negative sputum smears with at least one is an early morning specimen
• For negative sputum smear results, release from A.I.I in 2 days.
5

Removing Patients from A.I.I.
• Traditionally 3 sputum smears collected early morning on 3 consecutive days
– Took a long time: average 5-7 days in isolation
– Not sensitive 50-60%
– Not specific 70-90% (depending on NTM and TB prevalence)
Abad et. al. J of Hosp Infection 2010:97; Swai et al. BMC Research Notes 2011 4(475); Cattamanchi et al. BMC Infect Dis. 2009; 9: 53.
Singhal et al. Intl J of Mycobacteriology 2015: 4 (1)

Problems with Isolation
• Limited number of A.I.I. rooms
• Systemic review showed patients in isolation tend to:
– Be seen less by HCWs
– Have an 8 fold increase in adverse effects
– Have a negative perspective of their care*
– Delay in getting the proper procedure performed
*Abad et. al. J of Hosp Infection 2010:97

8

Luetkemeyer Clin Infect Dis. 2016 May 1;62(9) 9

Luetkemeyer Clin Infect Dis. 2016 May 1;62(9) 10
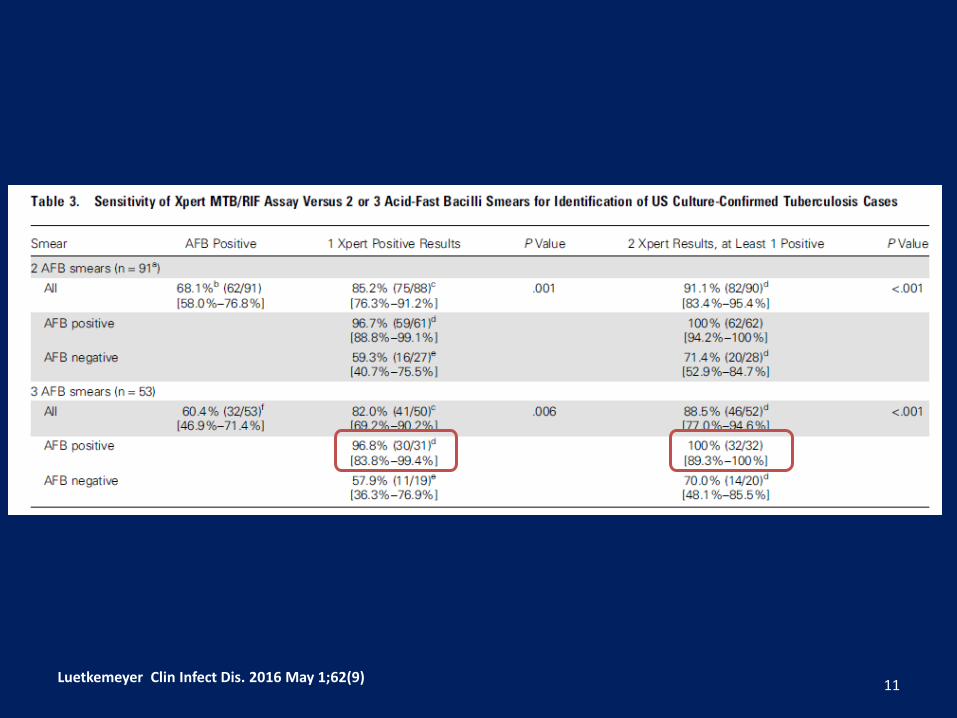
Luetkemeyer Clin Infect Dis. 2016 May 1;62(9) 11
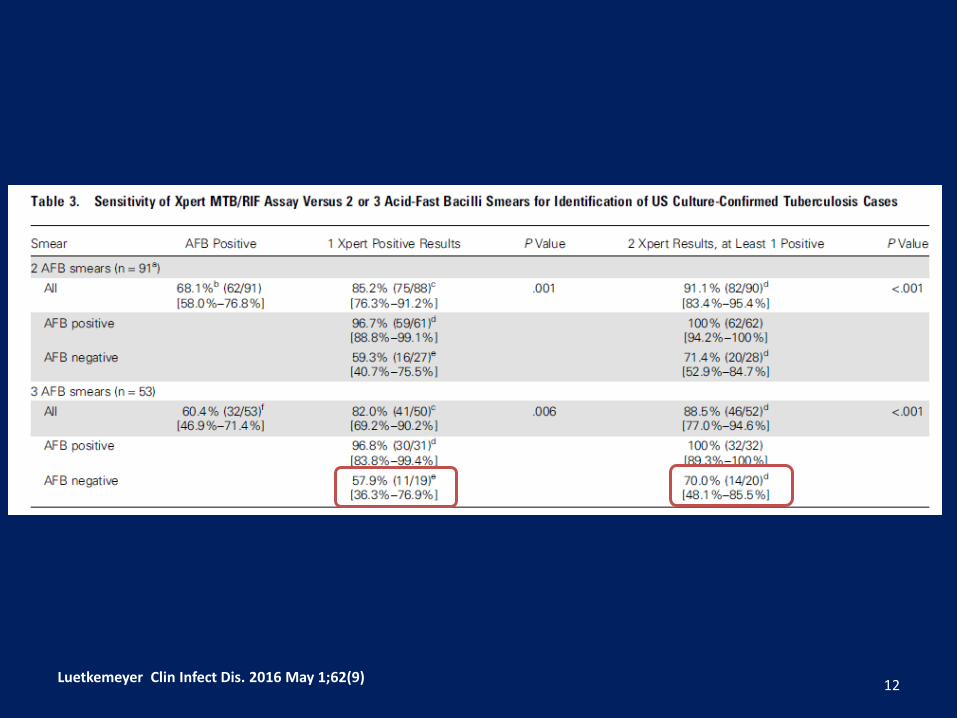
Luetkemeyer Clin Infect Dis. 2016 May 1;62(9) 12

Summary ACTG trial
Overall Smear positive
Smear Negative
NPV
1 Xpert 85.2% 96.7% 59.3% 99.7%
2 Xperts 91.1% 100% 71.4% 100%
13

Campos, Am J Respir Crit Care Med. 2008 Aug 1;178(3 14

Campos, Am J Respir Crit Care Med. 2008 Aug 1;178(3 15

Chaisson CID 2014: 59 16

Chaisson CID 2014: 59 17

Lippincott, Clin Infect Dis. 2014 Jul 15;59(2): 18

Lippincott, Clin Infect Dis. 2014 Jul 15;59(2): 19

Lippincott, Clin Infect Dis. 2014 Jul 15;59(2): 20

Lippincott, Clin Infect Dis. 2014 Jul 15;59(2): 21

Summary of trial data
• Improved sensitivity and specificity of NAA versus sputum AFB smear
• Cost savings by reducing time in A.I.I. and length of hospital stay
* Luetkemeyer, et al. ACTG and TBTC. Clin Infect Dis. epub 2/2/2016

FDA Response
23

FDA Approval of Xpert for A.I.I.
Either one or two sputum specimens can be used as an alternative to examination of serial acid-fast stained sputum smears to aid in the decision to discontinue A.I.I. for patients with suspected pulmonary TB

Purpose:
To provide guidance on the use of the Xpert to discontinue airborne infection isolation (A.I.I.) for persons with suspected, infectious pulmonary tuberculosis (TB)

Consensus Statement
• IS DOES NOT ADDRESS
– The diagnosis of TB
– When a TB case/suspect can be released from the hospital
• IT IS
– To help predict infectiousness
– To help determine clinical appropriateness to be removed from isolation
27

28

Case 1
• 91 year old male from Philippines
• Remote history of TB per patient
• Hemoptysis but no other TB symptoms
• Xpert positive
• Discontinue Isolation?
29

Case 1
30

Case 2
• 18 year old male from China
• IGRA negative
• CXR with LUL calcification consistent with granuloma disease
• Xpert negative
31

Case 2
32
Case 2
• Second Xpert negative
33

Case 2
34

Case 2
• 18 year old male from China
• IGRA negative
• CXR with LUL calcification consistent with granuloma disease
• Xpert negative x 2
35

Case 3
• 18 year old male from China
• IGRA positive
• CXR with LUL calcification consistent with granuloma disease
• Nonproductive cough
• Xpert negative
36

Case 3
37

Case 3
• Second Xpert negative
38

Case 3
39

Case 3
18 year old from China
IGRA positive
CXR with LUL calcification consistent with granuloma disease
Dry cough
• Discontinue isolation?
• What if he had hemoptysis instead of dry cough?
• What if it was winter time and everyone in dorm had a cough?
• What if he was smear positive?
40

Case 3
41

Case 3
• Discontinue isolation?
• REPORT TO HEALTH DEPARTMENT
42
Case 4
• 40 year US-born individual
• TST positive
• Had minimal contact to TB case
• Nonproductive cough
• CXR: minimal infiltrates RML
• Xpert negative
43

Case 4
44

Case 4
• Second Xpert positive
45

Case 4
46

47

48

49

50

51

Infectiousness
• Coughing
• Cavity in the lung
• TB disease of the lungs, airway, or larynx
• Undergoing cough-inducing or aerosol-generating procedures
• Not receiving adequate therapy

Xpert and A.I.I. Labelling Change: Operational Considerations
• Communication and coordination between clinicians and patient service providers are essential
– Nursing
– Respiratory Therapy
– Medical providers
– Laboratory
– IT / reporting platforms
– Institutional Infection Control
• Recognition of this process as independent of diagnostic protocol: Smears and cultures still must be obtained, followed-up

In The END, This Is Just The Beginning
• Data Collection and Analysis
– Infection Control programs should collaborate with the TB Laboratory and public health to collect and analyze data to evaluate the effectiveness methods used to determine discharge from A.I.I.
– Periodic analysis of protocol performance should be used to improve and/or modify policies and procedures

Summary
• Historically 3 smears used to determine discontinue of AII
• Can now use Xpert
• Consensus statement developed to assist with determining criteria to discontinue isolation
55

Summary
• DO NOT use consensus statement as a diagnostic algorithm
• If smells like TB, it is still TB
• Keep public health TB program aware of any suspected TB cases
56

Acknowledgements
• National Tuberculosis Controllers Association
• California Tuberculosis Control
• Slides borrowed from John Bernardo and Dave Ashkin
• The Consensus Committee
57
NAAT


















