Using Six Sigma for Process Improvement - · PDF filePracticing Six Sigma as the Designers...
72
Practicing Six Sigma as the Designers Intended Using Six Sigma for Process Improvement CATHOLIC HEALTH SERVICES The Ruby Team project at St. Anthony’s Rehabilitation Hospital represents, by all measures, a near- perfect Six Sigma implementation Mark Testa, EE, MBB Presentation by: Uniform Data System for Medical Rehabilitation 2012 UDSMR ® Annual Conference Buffalo, New York August 9–10, 2012 FIM, UDS-PRO, and UDSMR are trademarks of Uniform Data System for Medical Rehabilitation, a division of UB Foundation Activities, Inc.
Transcript of Using Six Sigma for Process Improvement - · PDF filePracticing Six Sigma as the Designers...

Practicing Six Sigma as the Designers Intended
Using Six Sigma for Process Improvement
CATHOLIC HEALTH SERVICES
The Ruby Team project at St. Anthony’s Rehabilitation Hospital represents, by all measures, a near-perfect Six Sigma implementation
Mark Testa, EE, MBB Presentation by:
Uniform Data System for Medical Rehabilitation 2012 UDSMR® Annual Conference Buffalo, New York August 9–10, 2012 FIM, UDS-PRO, and UDSMR are trademarks of Uniform Data System for Medical Rehabilitation, a division of UB Foundation Activities, Inc.

2
Access
FinancialStability
Excellence
CommunityInvolvement/
Advocacy
Collaboration/Partnerships
OrganizationalEffectiveness
To provide health care and services to those in need
To nurture an awareness of their relationship with God
To
assi
st p
eopl
e to
who
lene
ssT
o minim
ize human suffering
Catholic Health Services: CHS Mission & Goals: A Non-Profit Health Care Provider

3
Catholic Health Services: CHS Stakeholders:
■ 6500+ Persons Served Each Day
■ 10,000+ New People Request Our Services Each Year
■ 2,200 Employees
■ $11,000,000 of Charitable/Uncompensated Care in 2011
CATHOLIC HEALTH SERVICES
Catholic Health Services is the largest, most comprehensive, post acute continuum of care
system in the southeast United States

4
Catholic Health Services: CHS Prominent South Florida Post Acute Care Network:
■ 4 Sub-Acute Nursing and Rehabilitation Centers – 200 Beds
■ 3 Long-Term Care Facilities – 433 Beds
■ 3 Rehabilitation Hospitals – 88 Beds –1660 Patients 2011
■ Hospice Care
■ 4 Outpatient Therapy Clinics
■ 3 Physician Specialty Clinics
■ 2 Assisted Living Facilities – 124 Beds
■ 2 Home Health Agencies
CATHOLIC HEALTH SERVICES
Encompassing: 8 Service Lines 30 Facilities

5
Catholic Health Services: CHS Rehabilitation Hospitals Earn Top Ranking by UDSMR
CATHOLIC HEALTH SERVICES Note: 791 Facilities Included in 2011 UDSMR® Percentile Ranking
St. Catherine’s East & West
Ranked 97th Percentile for Outcomes
In 2011
97th
St. Anthony’s Ranked
93rd Percentile for Outcomes
In 2011
93rd
Up from: 25th Percentile in 2008 46th Percentile in 2009

6
What is Six Sigma ?
Six Sigma is a business management strategy which seeks to improve the quality of process outputs by identifying and removing the root causes of defects and key sources of variation § Data driven § Rigorous § Process oriented § Customer centric § Variance based § Statistically sound
CATHOLIC HEALTH SERVICES

7
How Did This Marriage Come About ?
CATHOLIC HEALTH SERVICES
Six Sigma Methodology
Acute Inpatient
Rehabilitation

8
More Specifically …
CATHOLIC HEALTH SERVICES
Retired Electronics
Vibrant Healthcare Network
Six Sigma Demands Bold / Engaged / Top Down Leadership
A new day was dawning for Healthcare in the U.S.
and the challenges are analogous to those faced by Corporate America in the 80s as the result of Asian competition
.... this was the burning platform from which Six Sigma was born
They acknowledged:
Engineer
.... At Catholic Health Services we are blessed with forward facing leadership at both the CEO and COO levels
Motorola Certified Six Sigma Master Black Belt
so why not look to Six Sigma in these challenging Healthcare times

9
How Was Six Sigma Launched At CHS ?
2. DMAIC: Structured Problem Solving Methodology
3. Actionable Data
Establishing a Six Sigma Foundation
Every organization is unique ………
1. Bullet Proof Metrics
CATHOLIC HEALTH SERVICES
Early Steps in the Right Direction = Big Returns

10
Bullet Proof Metrics
Customer Centric
Variance Based
Distortion Free
Deep and Wide
Displayed Graphically
Mark Testa
CATHOLIC HEALTH SERVICES

11
Bullet Proof Metrics
Customer Centric
Mark Testa
Measure what the customer feels Internal metrics can not be the end game

12
Bullet Proof Metrics
Customer Centric
Variance Based Reduce the variation and shift the mean
Mark Testa
Measure what the customer feels Internal metrics can not be the end game
Significance Testing is mission critical

13
Bullet Proof Metrics
Customer Centric Measure what the customer feels Internal metrics can not be the end game
Variance Based Reduce the variation and shift the mean
Distortion Free Data distortion leads to inconclusive results Timeliness is a source of distortion
Mark Testa
Significance Testing is mission critical

14
Bullet Proof Metrics
Customer Centric
Variance Based Reduce the variation and shift the mean
Distortion Free Data distortion leads to inconclusive results
Deep and Wide Summary data is an output … not an input Analytics demand patient level data
Mark Testa
Measure what the customer feels Internal metrics can not be the end game
Timeliness is a source of distortion
Significance Testing is mission critical

15
Bullet Proof Metrics
Customer Centric
Variance Based Reduce the variation and shift the mean
Distortion Free
Displayed Graphically Display in a manner that invokes right action
Mark Testa
Measure what the customer feels Internal metrics can not be the end game
Deep and Wide Summary data is an output … not an input Analytics demand patient level data
Timeliness is a source of distortion Data distortion leads to inconclusive results
Significance Testing is mission critical

16
UDSMR® Published Metric: External Gold Standard
CATHOLIC HEALTH SERVICES
Internal metrics that are deployed need to be Externally anchored ….
Seek always to understand how you are being measured
207 of the 400 patients met Targeted Performance Levels
Categorical Metric 48% Defective
Know the Rules of the Game
Facility Sub score
(% of Target)
2009 Overall National Ranking: 25th Percentile

17
DMAIC: Structured Problem Solving
Used when an existing process is failing to meet customer requirements or is not performing adequately.
CATHOLIC HEALTH SERVICES
Improve
Control
Measure
Define
Analyze

18
DMAIC: Structured Problem Solving
CATHOLIC HEALTH SERVICES
First Things
Fun Things
Highest Leverage
Nearly all organizations in the U.S. are Front End challenged ………
Don’t Seek Solutions to Problems You Don’t Understand
Improve
Control
Measure
Define
Analyze Don’t Purchase Solutions That Will Forever Be In Search of a Problem
And

19
CHS Digital Six Sigma Playbook
SERVICES
CATHOLIC HEALTH
Digital Six Sigma Playbook
DMAIC Edition
CATHOLIC HEALTH SERVICES
2012

20
Define Phase CHS Playbook M C I A D
Define Phase
Six Sigma Wisdom
1. Two-thirds of the Six Sigma projects that fail, fail because the project was poorly defined
2. The fate of the team is largely cast during this chartering phase
3. As a leader, your impact will never be greater than during this formative period
During the Define Phase, a team and its sponsors reach agreement on what the project is and what it should accomplish. This agreement is documented in a one page Project Charter. Six Sigma is a rigorous process and the Project Charter is the Enforcer of this rigor.
Mark Testa

PEM Performance Improvement Scorecard Linkage: Big Y: Become the Rehabilitation Provider of Choice by 2013 Small Y: UDSMR® Published National Percentile Ranking Vital X: FIM® Change
Project Risk Assessment Score: 19 of 20 Success probability: High
Business Case: The UDSMR® Program Evaluation Model (PEM) metric is a nationally recognized barometer of healthcare quality specific to Inpatient Rehabilitation Facilities. It promotes delivery of care that is effective, efficient, timely, safe, equitable and patient centric. Acute Hospitals seeking Best-in-Class, Post Acute Care Partners will look to PEM metric performance and rank
Opportunity Statement: For the full year of 2008, St. Anthony’s Rehabilitation Hospital received a National Percentile Ranking of 25% Focus on the Case Level Indicators weighted 60% in the PEM Model
Defect definition: Any patient whose FIM® Change (discharge FIM® rating minus admission FIM® rating) is lower than Targeted Performance Levels
Year-to-date November 2009 baseline: 37.2% defective
Goal Statement: Reduce the FIM® Change defect rate by 50% by May 2010 Defect Rate Target = 18.6%
Project Scope: In Scope: • FIM® Change: One of three equally weighted Case-Level
Indicators • All admissions to St. Anthony’s Rehabilitation Hospital Out of Scope: • All Other Components of the PEM Model
Project Plan Team Structure: Project Leader: Sponsor: Black Belt: Champions:
Team Members:
Task/Phase Start Date Target End Actual End Define Measure Analyze Improve
Control
M C I A D

22
Does the FIM® instrument support the organization’s mission ?
Patient Outcomes: To assist people to wholeness • Higher FIM® scores correlate well to higher probability of returning home • A return to Community extends and enhances Quality of Life
Professional Development: To create a Learning Organization • Professionals grow by challenging themselves with ever more demanding goals • Goals are effective only in the presence of performance feedback
Healthcare Reform: To become the Healthcare provider of choice • In a Bundled Service environment, Quality and Cost will be King
Making a Compelling Case for the Project Metric
Can the FIM® instrument support a performance-based culture ?
CATHOLIC HEALTH SERVICES
Good reason to pursue every FIM® point

Patient Centric Data Super Set Created
Deep and Wide Actionable Data
Made Possible by the Powerful UDS-PRO® Database Export Functionality Structured to Support All Manner of Statistical Analysis
•Included FIM® ratings for all admission, interim and discharge assessments •Extensive patient demographics
•Includes all CHS data entered into the UDS-PRO® System from 2007 to the present •8600 patient records with 350 data fields per record: 3,010,000 data elements

0.0
10
20
30
40
50
60
70
80
90
10
All
Cam
puse
s(20
09)
% C
omm
unity
0 10 20 30 40 50 60 70 80 90 100 110 1
Mid Pt FIM Score
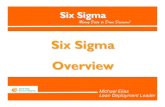
Percent to community = .0090 * total discharge FIM® rating + .0428
RSquare
RSquare Adj
Root Mean Square Error
Mean of Response
Observations (or Sum Wgts)
0.965786
0.961984
0.059538
0.630933
11
Summary of Fit
Model
Error
C. Total
Source
1
9
10
DF
0.90055657
0.03190329
0.93245986
Sum of
Squares
0.900557
0.003545
Mean Square
254.0493
F Ratio
<.0001 *
Prob > F
Analysis of Variance
n = 1392
Probability of Discharging to Community Regression Analysis Supports the Robust Nature of the FIM® Metric Design
All Campuses 2009
Customer Centric
It says to the clinician…. for each and every FIM® point earned, there is an increased probability that your patient will return Home
Functional independence is earned one point at a time
Textbook Threshold

25
Categorical Nature of the UDSMR® PEM Metric
CATHOLIC HEALTH SERVICES
Discharge FIM® Rating
# of
Pat
ient
s
42% Defective
70 Targeted Performance Level
Each patient undergoing rehabilitation has only two possible outcomes: 1. Meets the Performance Standard 2. Does not meet the Performance Standard:
In the Categorical World of the PEM Metric
Fail Pass
The Latter Being a Defect in Six Sigma speak ………
Clarification: the patient is not a defect the outcome is !

26
Discharge FIM® Rating
70 90 110 50
83 Mean
A
B
C
In a Parametric World Ruled by Averages, Outcomes for High Scoring Patients Offset the Outcomes for Lower Scoring Patients
Example: Average Discharge FIM® Rating of 83 Meets Targeted
Performance Level
Targeted Performance Level
Why a Categorical Metric ? It Embodies the Belief That No Patient Should Be Left Behind

27
Why a Categorical Metric ? It Embodies the Belief That No Patient Should Be Left Behind
Discharge FIM® Rating
70 90 110 50
In a Categorical World, Low Patient Outcomes Are Never Averaged Away.
Patient Outcomes Failing to Meet Targeted Performance Levels Are Logged as Defects to the Organization… as they should be
Categorical Metric: 33% Defective
A
B
C
Targeted Performance Level
Defective Outcome
Fail Pass

28
Six Sigma Improvement Methodology Hypothetical Example: Shifting the Mean / Reducing the Variation
CATHOLIC HEALTH SERVICES
Discharge FIM® Rating
# of
Pat
ient
s
42% Defective
70
Mean 83
Targeted Performance Level
Starting Point 42% defective
6

29
With a Categorical Metric Shifting the Mean Reduces Defects
CATHOLIC HEALTH SERVICES
70 Discharge FIM® Rating
# of
Pat
ient
s
18% Defective
Mean 88
Targeted Performance Level
6
Mean Shift 18% defective

30
CATHOLIC HEALTH SERVICES
70 Discharge FIM® Rating
# of
Pat
ient
s
5% Defective
88 Mean
Targeted Performance Level
With a Categorical Metric Decreasing Variation Reduces Defects Even Further
6
Variation Reduction 5% defective

31
With a Categorical Metric Setting the Key Targeted Performance Levels Is Critical
Internal and External Benchmarks: Best-in-Class • Observe what is possible • Calibrate expectations
Published National Norms: • eRehabData • Joint Commission • UDSMR
Historical In-House Performance: • Extrapolate from existing outcome trends • Leverage Clinician goal setting competencies
Categorical Levels Are Updated Periodically to Encourage Continuous Improvement

FIM® Item Entitlements
Facility: St. Anthony's Rehabilitation Hospital CMG 0110 Total FIM® Change Goal: 23.59
FIM® Item Entitlements Item Admission Discharge FIM® Change Stairs 1.0 1.7 0.7
Tub Shower 1.2 2.5 1.3
Toileting 1.1 2.5 1.4
Dressing Lower 1.2 2.6 1.4
Bladder 1.4 2.8 1.4
Walk Wheelchair 1.1 2.8 1.7
Bathing 1.5 2.9 1.4
Toilet 1.3 3.0 1.7
Bed Chair Wheelchair 1.3 3.1 1.8
Dressing Upper 1.7 3.4 1.7
Bowel 2.3 3.5 1.2
Grooming 2.3 4.0 1.6
Eating 2.9 4.3 1.4
Problem Solving 2.6 3.5 0.9
Memory 2.8 3.7 1.0
Expression 3.1 4.2 1.0
Interaction 3.4 4.4 1.0
Comprehension 3.4 4.4 1.0 Total 35.7 59.3 23.6
Note: Entitlements based on 2007 National Averages
FIM® Item Entitlements Allocating Total FIM® Change Discharge Goal to Individual FIM® Items
Entitlements assigned for both Admission and Discharge based on the profile of national averages specific to each CMG
National FIM® Item Profile for Stroke CMG 0110
Discharge
Admission

Testing Relationship Between Goal and Actual Outcome St. Anthony’s Rehabilitation Hospital 2009/2010 July
Our Clinicians demonstrated predictive skills that are being further developed into a core competency
20
30
40
50
60
70
80
90
10
11
12
Dis
char
ge T
otal
FIM
(TM
) Sco
re
40 50 60 70 80 90 100 110 120
Discharge Total FIM Goal
Discharge Total FIM® Score = -12.0673 + 1.0892 * Discharge Total FIM® Goal
Model
Error
C. Total
Source
1
657
658
DF
197063.14
96230.66
293293.80
Sum of
Squares
197063
146
Mean Square
1345.418
F Ratio
<.0001 *
Prob > F
Analysis of Variance
RSquare
RSquare Adj
Root Mean Square Error
Mean of Response
Observations (or Sum Wgts)
0.671897
0.671397
12.10247
84.87557
659
Summary of Fit
n = 680
Clinician Established Goal
Actu
al D
isch
arge
FIM
® R
atin
g

34
Measure Phase CHS Playbook M C I A D
Measure Phase
Six Sigma Wisdom
1. Average based measures give you only half the picture with regard to performance.
The purpose of the Measure Phase is to establish techniques for collecting data about current performance. This data will be utilized to identify and prioritize improvement opportunities as well as solidify a strategy for measuring improvement.
Mark Testa 9/30/09

35
Normal Distributions have a predictive nature The Empirical Rule: 68-95-99.7
CATHOLIC HEALTH SERVICES
68%
Applies to Normal Distributions
95%
+1s -1s -2s +2s +3s -3s mean
99.7%
Standard Deviation
Metrics Need to Be Variance Based

36
Why is it important ?
*
*
* *
* *
*
Jan Feb Mar Apr May Jun Jul Aug Sep
Simple Run Charts are Lacking in this regard
A
B
C
C
B
A
Visual data needs to Invoke Right Action
CATHOLIC HEALTH SERVICES
Display Graphically to Invoke Right Action
Pizza Party

37
Why is it important ?
*
*
* *
* *
*
Jan Feb Mar Apr May Jun Jul
*
*
Aug Sep
A
B
C
C
B
A
Visual data needs to Invoke Right Action
What is the Right Action ? What is the Right Question ?
CATHOLIC HEALTH SERVICES
Display Graphically to Invoke Right Action
Simple Run Charts are Lacking in this regard
Beatings Begin

38
Analyze Phase CHS Playbook M C I A D
Analyze Phase
Six Sigma Wisdom
1. Implementing low hanging fruit solutions can get you 10% to 20% improvement but may not be sustainable
2. A Six Sigma solution with data and analysis can find the 50% improvements that are sustainable
3. If as an organization you are willing to question your Beliefs, 68% to 100% improvements are possible
The purpose of the Analyze Phase is to conduct a data based search for the vital few root causes and to statistically validate them. Your role as a leader is to ensure that the team does not prematurely jump to solutions and that they use data and analysis to discover the most significant causes.
Mark Testa 9/30/09

39
Question your beliefs
CATHOLIC HEALTH SERVICES
Beliefs
Behaviors
Performance
Does your data support your organizational beliefs ? Can these beliefs be validated statistically ?
Prepare the Launch Pad:

40
Be a Player Not an Observer
What’s Required to Get the Team in the Game
1. Know the Rules of the Game 2. Know your Position/Role on the team 3. Know the Score at all times 4. Know what the Goal is 5. Know the time remaining on the clock
Anecdotal Evidence Active Management Opinions Knowing

Discharge FIM® Over/Under Targeted Performance Levels St. Anthony’s Rehabilitation Hospital: Full Year 2009 Starting Data Set
0%
3%
10%
25%
30%
24%
5%
2%
0% 0
-30 -20 -10 0 10 20 30 40 50
100.0%
99.5%
97.5%
90.0%
75.0%
50.0%
25.0%
10.0%
2.5%
0.5%
0.0%
maximum
quartile
median
quartile
minimum
54.41
37.8582
28.474
17.722
11.41
3.89
-4.48
-12.866
-22.014
-27.155
-30.41
Quantiles
Mean
Std Dev
Std Err Mean
Upper 95% Mean
Lower 95% Mean
N
3
1
0
4
2
4
Moments
Full Year 2009
38%
Histograms are the “go to tool” for visualizing your data and identifying opportunities
Distribution straddles the Pass/Fail line with 55% of patients teetering on the edge.
Normalized Across all CMGs
Variance Based
Targeted Performance Level
Display Data to Invoke Right Action
All discharge FIM® scores are organized into “buckets” 10 FIM® points wide

42
Improve Phase CHS Playbook M C I A D
Improve Phase
Six Sigma Wisdom
1. Teams have a tendency to adopt pet ideas especially under the influence of strong sponsors. Solutions looking for a Problem often arise at this stage.
The purpose of the Improve Phase is to demonstrate, with fact and data, that the proposed solutions solve the problem. Final decisions must be data driven
Mark Testa 9/30/09

Awareness and Access to Performance Feedback
UDSMR®
Model
PEM Metric
Establish Variance
Data Rich Patient Care Environment
Methodology
Targeted
Performance
Levels
Based
Metrics
Interdisciplinary
Structure
Awareness and Access to
Performance Feedback
Install
Strengthen
Team
… Teams don’t get better by just trying harder. Leaders need to create a learning environment

Control Chart Top Line Metrics
Variance Based
St. Anthony’s FIM® Change % Defective St. Anthony’s Length of Stay Efficiency
St. Anthony’s Discharge % Defective
20
30
40
50
60
Prop
ortio
n fo
r % D
efec
tive
with
out E
T to
Acu
te
C
B
A
C
B
A
02 03 04 05 06 07 08 09 10 11 12 01 02 03 04 05 06 07 08 09 10 11 12 01 02
Month/Yr
μ0=0.3557
LCL=0.2121
UCL=0.4993
P of % Defective without ET to Acute
Feb 2008 – Feb 2010
44.4% Feb.
35.6%
18.6% Goal
Process was out of statistical control
Should expect 68% of the plot points in Zone C

FIM® Tracking Sheet
Know the Score at All Times
Tracking sheet is updated each time a patient record is closed and provides daily feedback on month-to-date performance
18.6% Defective
0
0
Perf. Target A B C D E F G H I J K L M N O P Q R S T U V

UDSMR® Patient Profile
Know the Score at All Times
Utilized as a communication and marketing tool with physicians

Goal TRAC A Spreadsheet on Steroids
Know What the Goal Is Know the Score at All Times
Moving Beyond Clinical Silos
Manage Entitlements Establish Accountability
Set Priorities

48
Interdisciplinary Team Advocate Role
• Enhance accuracy of clinician’s “FIM® meters”
• Ensure the integrity of data, metrics and clinician accountability
• Provide continuity/communication between all disciplines
• Facilitate a Team Consensus Process among clinicians; seeking to establish a holistic, shared perception of a patient’s outcomes
• Provide this Consensus information to the PPS Coordinator for consideration
Know Your Position/Role On the Team

Core Interdisciplinary Team Consensus Process
Interdisciplinary Team Advocate Seeks Consensus 24 Hour Period Prior to Discharge
SLP OT
PT NSG
DR CM
PT
OT SLP
NSG
Core Team
Interdisciplinary Team
Team Advocate
PPS Coordinator: A Quality Resource: confirms that the Clinician notes in the medical record support the consensus scoring … if not, the medical record takes precedence.
Interdisciplinary Team
Note: consensus form is a communications tool and does not become part of Medical Record

Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
PEM Annual Report
(with ranking) Annually
Quarterly
Monthly
Weekly
Feb Mar Apr May Jun Aug Sep Jul Oct Nov Dec
Month-to-Date FIM® Tracking Sheet
PEM Qtrly Rpt
PEM Qtrly Rpt
PEM Qtrly Rpt
PEM Qtrly Rpt
Analytics at the Point of Care Relevant, Timely and Accurate Feedback
Daily
Collapsing time required to access performance data
First 3 Days Last 24 Hrs.
Today, at point of care, the clinician knows and manages goal performance in real time

51
Today’s Team is Fully Suited and On the Field
1. Know the Rules of the Game 2. Know your Position/Role on the team 3. Know the Score at all times 4. Know what the Goal is 5. Know the time remaining on the clock
Before Now 2.2 9.7 2.8 2.0 2.8 4.0
9.7 9.0 9.7 8.5
Score 0 to 10 with 10 being fully aware
Survey taken of Ruby Team members 7/1/10
Anecdotal Evidence Opinions
Active Management Knowing
This Not This

Now for the Results …..

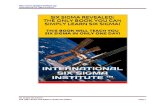
St. Anthony’s FIM® Change % Defective
Test 1: One point beyond Zone A Test 2: Nine points in a row in a single (upper or lower) side of Zone C or beyond Test 3: Six points in a row steadily increasing or decreasing (whole chart) Test 4: Two out of three points in a row in Zone A or beyond (upper or lower) Test 5: Four out of five points in Zone B or beyond (upper or lower)
Western Electric Rules for Significance Testing
Project targets a 48% reduction in FIM® Change defects to 18.6%
A new statistically significant process mean of 12.4% was established by the Ruby Team in June; far exceeding the chartered percent defective goal of 18.6% . This represents a 69% reduction in defects as reflected in the new process mean
69% Improvement
-10
0.0
10
20
30
40
50
60
70
Prop
ortio
n fo
r % D
efec
tive
with
out E
T to
Acu
te
C
B
A
C
B
A
C
B
A
C
B
A
1 2
09 10 11 12 01 02 03 04 05 06 07 08 09 10 11 12 01 02 03 04 05 06 07 08 09 10 11 12
Month/Year
Goal 18.6%
Sep 2008 – Dec 2010
40.4%
12.4%
New Process Remains Stable for 9 Consecutive Months

0%
3%
10%
25%
30%
24%
5%
2%
0% 0
-30 -20 -10 0 10 20 30 40 50
100.0%
99.5%
97.5%
90.0%
75.0%
50.0%
25.0%
10.0%
2.5%
0.5%
0.0%
maximum
quartile
median
quartile
minimum
54.41
37.8582
28.474
17.722
11.41
3.89
-4.48
-12.866
-22.014
-27.155
-30.41
Quantiles
Mean
Std Dev
Std Err Mean
Upper 95% Mean
Lower 95% Mean
N
3.2354023
12.477931
0.598271
4.4112711
2.0595335
435
Moments
FIM Chg Over/Under
2009 Full Year
3%
1%
6%
14%
24%
30%
17%
4%
-30 -20 -10 0 10 20 30 40 50
100.0%
99.5%
97.5%
90.0%
75.0%
50.0%
25.0%
10.0%
2.5%
0.5%
0.0%
maximum
quartile
median
quartile
minimum
49.31
49.31
43.695
35.52
27.41
20.11
10.29
-0.41
-21.64
-26.95
-26.95
Quantiles
Mean
Std Dev
Std Err Mean
Upper 95% Mean
Lower 95% Mean
N
18.194646
14.613828
1.468745
21.109323
15.27997
99
Moments
FIM Chg Over/Under
Qtr. 2 2010
10%
Shifted the mean: +15 FIM® pts
38%
Average Patient is now achieving outcomes 18 FIM® points above Targeted Performance Levels
3 FIM® points : too close for comfort in a Categorical based PEM metric world
FIM® Change Over/Under Targeted Performance Levels St. Anthony’s Rehabilitation Hospital: Full Year 2009 v.s. Qtr. 2 2010
Average Patient outcome was only 3 FIM® points above Targeted Performance Levels

55
FIM® Change
Discharge FIM® Rating
LOS Efficiency
Benefits
Ancillary Benefits

St. Anthony’s Discharge FIM® % Defective
Test 1: One point beyond Zone A Test 2: Nine points in a row in a single (upper or lower) side of Zone C or beyond Test 3: Six points in a row steadily increasing or decreasing (whole chart) Test 4: Two out of three points in a row in Zone A or beyond (upper or lower) Test 5: Four out of five points in Zone B or beyond (upper or lower)
Western Electric Rules for Significance Testing
49% Improvement
0.0
10
20
30
40
50
60
70
Pro
porti
on fo
r
% D
efec
tive
C
B
A
C
B
C
B
A
C
B
A
1 2
09 10 11 12 01 02 03 04 05 06 07 08 09 10 11 12 01 02 03 04 05 06 07 08 09 10 11 12
Trend Discharge Month
39.6%
20.0%
Sep 2008 – Dec 2010

St. Anthony’s Length of Stay Efficiency Sept 2008 through Dec 2010
Length of Stay Efficiency = FIM® Change / Length of Stay FIM® pts per day
64% Improvement
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
5.0
Mea
n(LO
S Ef
ficien
cy)
C
B
A
C
B
AC
B
A
C
B
A
C
B
A
C
B
A
1 2 3
20 20 20 20 20 20 20 20 20 20 20 20 20 20 20 20 20 20 20 20 20 20 20 20 20 20 20 20
Discharge Year/Month
FIM® velocity
3.23
3.60
2.19
An additional 1.4 FIM® points per day

3547 Patient Records Profiled / 750 Stroke Patients Identified
CHS Rehabilitation Impairment Group Distribution Stroke Patients Account for 21% of the CHS Case Load
0
20
40
60
80
100
Per
cent
N=3547
1 7 3 6 20 8 14 5 2 15 9 10 16 17 4 13 12 18 19 21 11
RIC
0
20
40
60
80
100
Cum
Per
cent
Plots
1 Stroke 7 Fractured Lower Extremity 3 Non-Traumatic Brain 6 Neurologic Conditions 20 Miscellaneous 8 Replacement of Lower Extremity 14 Cardiac
Top 7 RICs = 80% of the CHS Case Load
21%
Catholic Health Services Internal Use Only M. Testa 05/04/11
80% Cumulative Percent
Top 7 RICs
Pareto of RICs

Stroke Case Mix Group (CMG) Distribution Stroke Case Mix Heavily Weighted Toward Highest Impairment
Catholic Health Services Internal Use Only M. Testa 05/04/11
%
0
10
20
30
40
50
60
70
80
90
100
Perc
ent
0110 0108 0109 0107 0106 0105 0104 0102
CMG wo/Tier
0
10
20
30
40
50
60
70
80
90
100
Cum
Per
cent
Plots
68.0%
14.0%
8.5% 4.4%
2.0% 1.7% 1.0% .4%
Highest Impairment Lowest Impairment
Pareto of Stroke CMGs
82% Cumulative Percent

Individual Case Level Indicators
1.01 .8
1.8
2.8
2010
LOS Efficiency
1.45
1.89 National Norm 1.3
2.3
Community 58%
Sub Acute
21%
Acute 21%
Discharge Setting
Tier D 26%
Tier A 66%
Comorbidity Tiering
Expected Rehabilitation Length of Stay 24.2 days
Actual Rehabilitation Length of Stay 16.0 days
Stroke Patient Profile: St. Anthony’s Rehabilitation Hospital 101 Stroke Patient Records: Year 2010: Includes Re-Admits to Acute
Comorbidity
High
Low
Level
Tier B 8%
Tier C 4% Note: National norms are calculated for Joint Commission by UDSMR and are case mix CMG adjusted:
National Average
Upper 95% Confidence Limit
Lower 95% Confidence Limit
22.0
15
20
25
30
35
2010
FIM® Change
26.1
31.1
National Norm
National
61.5
2010
Discharge FIM® Rating
66.7
71.8
Norm
55
60
65
70
75
Catholic Health Services Internal Use Only M. Testa 05/04/11
M481 only
National Norm 55%
National Norm 15%
National Norm 30%

61
Control Phase CHS Playbook M C I A D
Control Phase
Six Sigma Wisdom
The purpose of the Control Phase is to institutionalize the process improvements and monitor ongoing performance.
1. If the Process Owner (Champion) was not part of the project team, there is a high probability that the process changes will meet with resistance at the point of implementation.
Mark Testa

62
Final Project Report and Presentation: Mandatory
In preparing the report, the team reaches consensus on exactly what process changes led to their ultimate success and documents these changes for posterity
If things go awry in the future, the Final Report is a valuable reference tool for quickly regaining control

St. Anthony’s FIM® Change % Defective
-10
0.0
10
20
30
40
50
60
70P
ropo
rtion
for %
Def
ectiv
e
with
out E
T to
Acu
te
C
B
A
C
B
A
C
B
A
C
B
A
1 2
09 10 11 12 01 02 03 04 05 06 07 08 09 10 11 12 01 02 03 04 05 06 07 08 09 10 11 12 01 02 03 04 05 06 07 08 09 10 11 12
Month/Year
Once the process changes became fully institutionalized the process remained in statistical control at the new process mean of 12.4% for 21 consecutive months
40.4%
12.4%
Sep 2008 – Dec 2011
69% Reduction in defects
21 consecutive months
21 Months Into the Control Phase and Still Firing on All Cylinders
Variation in patient outcomes had been dramatically reduced
Control Phase

St. Anthony’s FIM® Change % Defective
-10
0.0
10
20
30
40
50
60
70Pr
opor
tion
for %
Def
ectiv
e
with
out E
T to
Acu
te
C
B
A
C
B
A
C
B
A
C
B
A
1 2
09 10 11 12 01 02 03 04 05 06 07 08 09 10 11 12 01 02 03 04 05 06 07 08 09 10 11 12 01 02 03 04 05 06 07 08 09 10 11 12 01 02 03
Month/Year
Sep 2008 – Mar 2012
Preparing for the Inevitable
69% Reduction in defects
40.4%
12.4%
21 consecutive months
But then the Inevitable happened ….
Over time and with changes in team membership, defect levels began to rise as process rigor waned. Teams forgot what contributed to their success and old habits returned.
This is not at all unusual and should be expected
What was unusual, is how long it took before it occurred

St. Anthony’s FIM® Change % Defective
-10
0.0
10
20
30
40
50
60
70Pr
opor
tion
for %
Def
ectiv
e
with
out E
T to
Acu
te
C
B
A
C
B
A
C
B
A
C
B
A
1 2
09 10 11 12 01 02 03 04 05 06 07 08 09 10 11 12 01 02 03 04 05 06 07 08 09 10 11 12 01 02 03 04 05 06 07 08 09 10 11 12 01 02 03 04 05
Month/Year
Sep 2008 – May 2012
12.4%
40.4%
21 consecutive months
69% Reduction in defects
Additionally it was unusual how quickly the situation was remediated
With the Final Project Book in hand, the team quickly identified which of their documented success factors had been abandoned
Preparing for the Inevitable
This is why the Final Project Report is a key Best Practice

Externally Reported Externally Reported FIM® Change
Note: National norms are calculated for Joint Commission by UDSMR and are case mix CMG adjusted:
National Average Upper 99% Confidence Limit
Lower 99% Confidence Limit
St. Anthony’s
New Process
New Process

Externally Reported Externally Reported Discharge FIM® Rating
Note: National norms are calculated for Joint Commission by UDSMR and are case mix CMG adjusted:
National Average Upper 99% Confidence Limit
Lower 99% Confidence Limit
St. Anthony’s
New Process
New Process

Externally Reported Externally Reported Length of Stay Efficiency
Note: National norms are calculated for Joint Commission by UDSMR and are case mix CMG adjusted:
National Average Upper 99% Confidence Limit
Lower 99% Confidence Limit
St. Anthony’s
New Process
New Process

69
UDSMR® Published Metric: External Gold Standard
Year End 2011 Project Report Card
Facility Sub-score
(% of Target)
rd
National Ranked at 93rd Percentile Up from 25th Percentile
St. Anthony’s Rehabilitation Hospital

St. Catherine’s East FIM® Change % Defective The Solution Was Robust and Transferable
Test 1: One point beyond Zone A Test 2: Nine points in a row in a single (upper or lower) side of Zone C or beyond Test 3: Six points in a row steadily increasing or decreasing (whole chart) Test 4: Two out of three points in a row in Zone A or beyond (upper or lower) Test 5: Four out of five points in Zone B or beyond (upper or lower)
Western Electric Rules for Significance Testing
Metric Chartered
64% Improvement
Process proves transferable, yielding a new process mean identical to that achieved by the Ruby Team
0.0
10
20
30
40
50
60
Pro
port
ion
for
% D
efec
tive
C
B
A
C
B
A
C
B
A
C
B
A
C
B
A C
B
A
2 3 4
07 08 09 10 11 12 01 02 03 04 05 06 07 08 09 10 11 12 01 02 03 04 05 06
Trend Discharge Month
Jul 2009 – Jun 2011
34.2%
19.7%
12.3% 12.4% Goal
Internal National Benchmark 10.7% Jun

71
Adopted a Goal Centered Approach to Patient Care
Crafted and Installed Bullet Proof Metrics
Nurtured Interdisciplinary Concept into a Fully Functional Team Environment
Review The Key Ingredients For Success
Provided Real Time Performance Feedback
Introduced Variance Based Tools
Employed Analytics to Test Organizational Beliefs
Established a Data Rich Work Environment
Introduced a Structured Problem Solving Methodology: DMAIC
A Six Sigma Foundation Is Now In Place
…. and we are excited about leveraging our new found competency in Analytics

THANK YOU