
Impulsivity, Attention Deficits, and Addiction - Perspectives on Diagnoses and Treatment
Upload
erin-thomasCategory
view
216download
1
1
Using Diagnoses to Improve Treatment
Robert M. Gordon, Ph.D. ABPPJ&K Seminar 2013
1. How does diagnoses (DSM, ICD, PDM) affect treatment?
2. How to tailor treatment to the diagnoses of personality organization and personality patterns.

2
My Eclectic Background
• Undergrad focus on science and epistemology• Temple’s psychology department heavily influenced by Wolpe
and Lazarus. It was anti-psychoanalytic.• I studied with Rosnow and Lana the artifacts and assumptions in
research (applied epistemology).• After my Ph.D., I studied with Albert Ellis (Rational Emotive
Therapy), Salvador Manuchin, Jim Framo, and Peggy Papp (family therapy).
• For a while my primary identification was, “family therapist.” (AFTA, AAMFT Supervisor)
• Eventually, I became convinced that projections and transferences were the main issues in couples work and went on to study object relations (institute training and my psychoanalysis).

3
Paradigm Shift to Evidence Based Practice

4
An Integrative Theoretical Formulation Precedes an Integrative
Treatment
• Need for the best theoretical formulation that integrates research about the mind, brain, affects, cognitions, behaviors, temperament, and their interactions in an interpersonal context.
• Need for technical eclecticism based on the needs of the patient and EBP.

5
The New Three Core Competencies in Psychiatry
• Supportive Therapy (Rogerian)
• Cognitive- Behavioral Therapy (CBT)
• Long-Term Psychodynamic Psychotherapy

6
Our Brains Guided Us for Millions of Years without Consciousness or Rationality

7
Hypothalamic Sites that Generate Instinctual Behavioral
and Affective States in Mammals Panksepp (1982)

8
The Affective Parts of the Mammalian Brain are largely Non-Cognitive and Instinctual

9
Superego, Ego and Id was a First Step in Understanding a Brain in Conflict
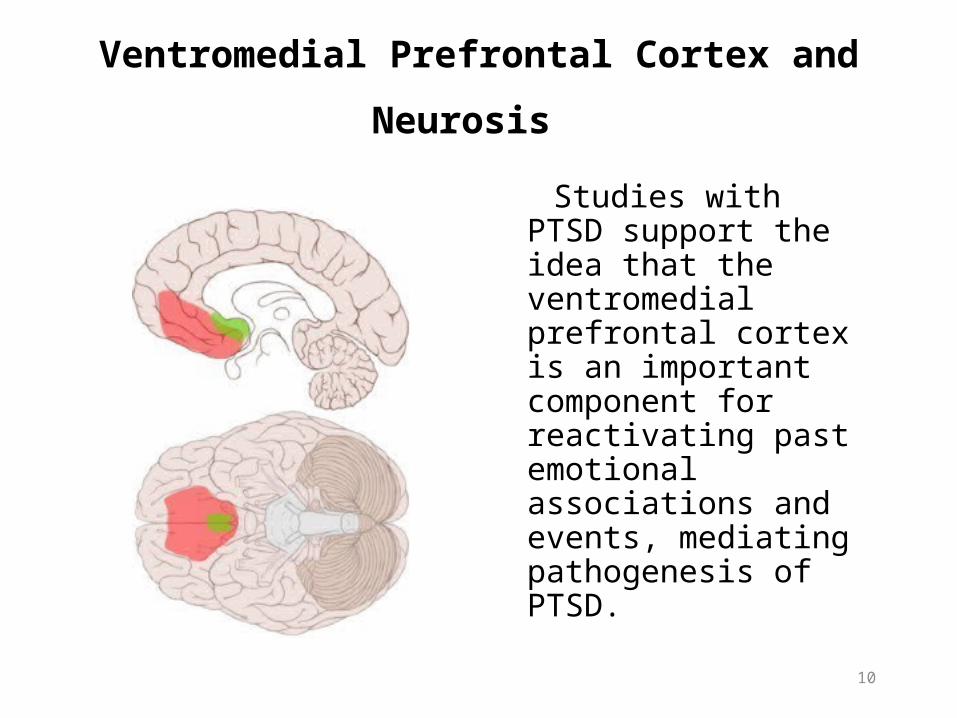
•The Amygdalae (A) are involved in the processing of emotions.•The Ventromedial prefrontal cortex (VMPC) moderates emotional reactions and sends signals to the Striatum (S) with input from past experiences. •If the associations are negative, the VMPC signals are inhibitory. The Striatum translates signals from the Amygdala and VMPC into body action.
VMPC A
S
10
Ventromedial Prefrontal Cortex and
Neurosis Studies with PTSD support the idea that the ventromedial prefrontal cortex is an important component for reactivating past emotional associations and events, mediating pathogenesis of PTSD.
11
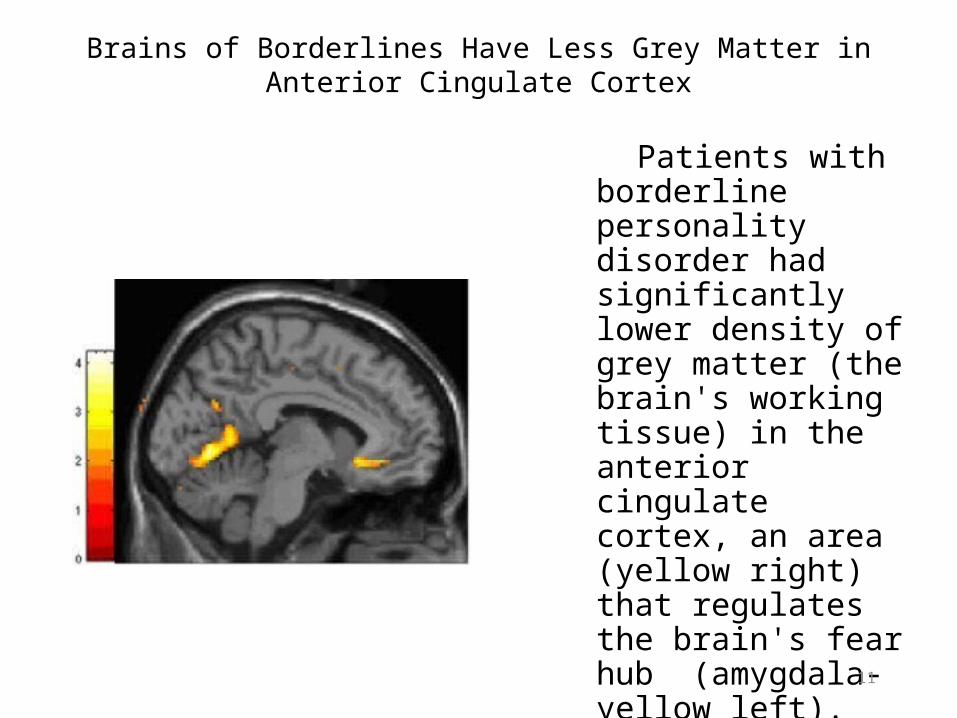
Brains of Borderlines Have Less Grey Matter in Anterior Cingulate Cortex
Patients with borderline personality disorder had significantly lower density of grey matter (the brain's working tissue) in the anterior cingulate cortex, an area (yellow right) that regulates the brain's fear hub (amygdala-yellow left).
MRI scan data shows the difference between patients and controls.

12
Brains of Borderlines Have More Grey Matter in Amygdala
Patients with borderline personality disorder had significantly higher density of grey matter in the brain's fear hub, the amygdala (red areas). MRI scan data shows where patients and controls differed.

13
Panksepp, J. (2003).Science, Oct 10th.
Herman & Panksepp, 1979
Damasio, et al., 2002
Emotions and attachment drives in mammals are similar and evolved for functional reasons. They may be affected by thoughts, but they are not created by them.

14
Attachment Security in Infancy and Early Adulthood: A Twenty-Year Longitudinal
Study.Walters, E. Merrick., S.; Treboux, D.; Crowell, J. and Albersheim, L. (2000),
Child Development.
• Researchers looked at relationship patterns in 50 young adults who were studied 20 years earlier as infants.
• Overall, 72% of the adults received the same secure verses insecure attachment classification they had in infancy.

15
Experimental Test of Unconscious Transference
• Study: subjects are subliminally shown aggressive (A) or positive (B) stimuli – and then rate a neutral stimulus (C)
– Subjects shown panel A subsequently rated the boy in panel C more negatively (Eagle, 1959)

16
Treat the Whole Person
• Blatt, (2006), Norcross (2002), Wampold (2001) have concluded that the nature of the psychotherapeutic relationship, reflecting interconnected aspects of mind and brain operating together in an interpersonal context, predicts outcome more robustly than any specific treatment approach per se.
• Westen, Novotny, and Thompson-Brenner (2004) have presented evidence that treatments that focus on isolated symptoms or behaviors (rather than personality, emotional, and interpersonal patterns ) are not effective in sustaining even narrowly defined changes.

17
Value of Insight into the Self
• 800 Psychologists ranked a list of 38 of the most beneficial things they got from their own psychotherapy.
• They listed first, “Self-understanding.”
• “Symptom relief” was halfway down the list
• Included in the survey were psychologists from all theoretical orientations (Behaviorists, Cognitive-Behaviorists, Psychoanalytic, etc.).
• Pope, K. T., B.G. (1994). Therapists as patients: A national survey of psychologists' experiences, problems, and beliefs. Professional Psychology: Research & Practice, 25(3), 247-258.

18
Effectiveness of Long-term Psychodynamic Psychotherapy A Meta-analysis
Leichsenring and Rabung (2008) JAMA, 3000,13,1551-1565.
• 23 LTPP studies (11 RCT efficacy and 12 effectiveness) total of 1053 patients with personality disorders, and multiple and complex problems.
• LTPP at least 1 year (an average of 151 sessions).
• Results LTPP better than 96% of those in short term therapies (CBT, DBT, SFT, CAT, FT, STPP, etc.) with changes in not only symptoms relief but with increases in mental capacities.

19
Importance of Transference and Attachment with BPD
• Clarkin, et al. (2007): 90 BPD randomly assigned to transference-focused psychotherapy (TFT), dialectical behavior therapy (DBT), or supportive therapy (ST).
• Patients in all 3 treatments showed significant positive change in depression, anxiety, global functioning, and social adjustment.
• Both transference-focused psychotherapy and dialectical behavior therapy were significantly associated with improvement in suicidality.
• Only transference-focused psychotherapy and supportive treatment were associated with improvement in anger.
• Transference- focused psychotherapy and supportive treatment were each associated with improvement in impulsivity.
• Only transference-focused psychotherapy was significantly predictive of change in irritability and verbal and direct assault.

20
Over-all Research
• Evidence Based short-term symptom focused treatments are all equally effective.
• Long-term psychodynamic therapies that focus on temperament, conflicts, affects, cognitions, behaviors, interpersonal context, child development, conscious and unconscious levels are better than symptom focused treatments in treating personality disorders.

21
Integrative Psychotherapeutic InterventionsGoing From Supportive, CBT and Psychodynamic
• Personal Qualities of the Therapist
• Maintaining the Therapeutic Frame
• Reassurance
• Listening
• Behavioral Mastery: Self-Soothing
• Cognitive Learning
• Clarifications
• Interpretations of mental life that affects subjective well-
being and relationships

22
Treatment of the Borderline Level Personality Disorder
• Behavioral Mastery: desensitization and self-soothing
• Cognitive Learning: how to better understand thoughts, feelings, and behaviors
• Clarifications and Confrontations: of the patient’s confusions, distortions and consequences of judgment and impulses
• Interpretations: focus on here and now defenses, transferences, enactments, and mentalization

23
Treatment of the Neurotic Level Personality Disorder
• Reconstructions: patients may benefit from a coherent, insightful narrative of their psychological history. Despite problems with recall and subjectivity, traumatic events can be recalled, mastered and integrated into a more cohesive identity.
• Interpretations: insight into unconscious resistances, defenses, transferences and enactments.

Kernberg’s Differentiation of Personality Organization That Preceded the PDM
Neurotic Borderline Psychotic•Identity +integrated - diffused -Integration
•Defensive +higher -primitive -Operations
•Reality + + -Testing

25
Borderline Personality OrganizationBasic Characteristics- Kernberg
Identity Diffusion No integrated concept of selfNo integrated concept of significant others
Primitive Defenses– Splitting– Idealization/devaluation– Projective identification– Omnipotent control– Denial Variable Reality Testing

26
Healthy Defense Mechanisms
Anticipation
Affiliation
Altruism
Humor
Self-Assertion
Self-Observation
Sublimation
Suppression
27
Neurotic Level Defenses
Displacement
Dissociation
Intellectualization
Rationalization
Isolation of Affect
Reaction Formation
Repression
Undoing

28
Borderline level Defenses
Idealization / Devaluation Omnipotence and Omnipotent controlDenial Projective identificationSplitting of self-image or image of othersActing outProjection

29
Psychotic Level
Delusional projection
Psychotic denial
Psychotic distortion

30
Anaclitic vs Introjective(according to S.Blatt)
•Anaclitic: Borderline, Histrionic, Dependent, Avoidant, Depressive anaclitic.
•Introjective: Schizoid, Paranoid, Antisocial, Narcissistic, Obsessive, Depressive introjective.
•Reference tools: Object Relations Inventory (ORI; Blatt et al., 2006)

Personality Disorders P Axis
Temperamental, Thematic, Affective,
Cognitive, and Defense patterns

32
P101. Schizoid Personality Disorders
• Contributing constitutional-maturational patterns: Highly sensitive,shy, easily overstimulated
• Central tension/preoccupation: Fear of closeness/longing for closeness
• Central affects: General emotional pain when overstimulated, affects so powerful they feel they must suppress them
• Characteristic pathogenic belief about self: Dependency and love are dangerous
• Characteristic pathogenic belief about others: The social world is impinging, dangerously engulfing
• Central ways of defending: Withdrawal, both physically and into fantasy and idiosyncratic preoccupations

33
P102. Paranoid Personality Disorders
• Contributing constitutional-maturational patterns: Possibly
irritable/aggressive
• Central tension/preoccupation: Attacking/being attacked by humiliating others
• Central affects: Fear, rage, shame, contempt
• Characteristic pathogenic belief about self: Hatred, aggression and dependency are dangerous
• Characteristic pathogenic belief about others: The world is full of potential attackers and users
• Central ways of defending: Projection, projective identification, denial, reaction formation

34
P103. Psychopathic (Antisocial) Personality Disorder P103.1 Passive/Parasitic: “con artist” P103.2 Aggressive: explosive, predatory, often violent
• Contributing constitutional-maturational patterns: aggressiveness, high threshold for emotional stimulation
• Central tension/preoccupation: Manipulating/being manipulated
• Central affects: Rage, envy
• Characteristic pathogenic belief about self: I can make anything happen
• Characteristic pathogenic belief about others: Everyone is selfish, manipulative, dishonest
• Central ways of defending: Reaching for omnipotent control

35
P104. Narcissistic Personality Disorders P104.1 Arrogant/Entitled: devalues, vain, commanding P104.2 Depressed/Depleted: idealizing, envious, easily hurt
• Contributing constitutional-maturational patterns: No clear data
• Central tension/preoccupation: Inflation/deflation of self-esteem
• Central affects: Shame, contempt, envy
• Characteristic pathogenic belief about self: I need to feel okay
• Characteristic pathogenic belief about others: Others enjoy riches, beauty, power, and fame; the more I have of those, the better I will feel
• Central ways of defending: Idealization/devaluation

36
Narcissistic PD: Narcissistic Injury
The Doberman threw himself out the second-story window after he realized the family had indeed named him “Binky.”

37
P105. Sadistic and Sadomasochistic Personality Disorders P105.1 Intermediate Manifestation: Sadomasochistic Personality Disorders:
alternate between attacking and feeling insulted
• Contributing constitutional-maturational patterns: Unknown
• Central tension/preoccupation: Suffering indignity/inflicting such suffering
• Central affects: Hatred, contempt, pleasure (sadistic glee)
• Characteristic pathogenic belief about self: I am entitled to hurt and humiliate others
• Characteristic pathogenic belief about others: Others exist as objects for my domination
• Central ways of defending: Detachment, omnipotent control, reversal, enactment

38
Sadistic PD: I am entitled to hurt others

39
P106. Masochistic (Self-Defeating) Personality Disorders P106.1 Moral Masochistic: self-esteem depends on suffering P106.2 Relational Masochistic: suffer for sake of relationship
• Contributing constitutional-maturational patterns: None known
• Central tension/preoccupation: Suffering/losing relationship or self-esteem
• Central affects: Sadness, anger, guilt
• Characteristic pathogenic belief about self: By manifestly suffering, I can demonstrate my moral superiority and/or maintain my attachments
• Characteristic pathogenic belief about others: People pay attention only when one is in trouble
• Central ways of defending: Introjection, introjective identification, turning against the self, moralizing

40
Masochistic Personality Disorder
“Penny for your thoughts, Arnold!”

41
P107. Depressive Personality Disorders P107.1 Introjective: self-critical, self-worth
P107.2 Anaclitic: concern with attachment issues
• Contributing constitutional-maturational patterns: Possible genetic predisposition
• Central tension/preoccupation: Goodness/badness or aloneness/relatedness of self
• Central affects: Sadness, guilt, shame
• Characteristic pathogenic belief about self: There is something essentially bad or incomplete about me
• Characteristic pathogenic belief about others: People who really get to know me will reject me
• Central ways of defending: Introjection, reversal, idealization of others, devaluation of self

Depressive Personality Disorder
Lodge owner Harold Shuffle saw only the negative side of things.

43
P107.3 Converse Manifestation: Hypomanic Personality Disorder
• Contributing constitutional-maturational patterns: Possibly high energy
• Central tension/preoccupation: Overriding grief/succumbing to grief
• Central affects: Elation, rage, unconscious sadness and grief
• Characteristic pathogenic belief about self: If I stop running and get close to someone, I’ll be traumatically abandoned, so I’ll leave first
• Characteristic pathogenic belief about others: Others can be charmed into not seeing the qualities that make people inevitably reject me
• Central ways of defending: Denial, idealization of self, devaluation of others

44
P108. Somatizing Personality Disorders
• Contributing constitutional-maturational patterns: Possible physical fragility, early sickliness, early abuse
• Central tension/preoccupation: Integrity/fragmentation of bodily self
• Central affects: alexithymia, inferred rage, distress
• Characteristic pathogenic belief about self: I am fragile, vulnerable, in danger of dying
• Characteristic pathogenic belief about others: Others are powerful, healthy, and indifferent
• Central ways of defending: Somatization, regression

45
Somatizing Personality Disorder
“My brother, Tilford, had trouble with hemorrhoids and he never did anything like this!”

46
P109. Dependent Personality Disorders
• Contributing constitutional-maturational patterns: Possible placidity, sociophila
• Central tension/preoccupation: Keeping/lossing relationships
• Central affects: Pleasure when securely attached; sadness and fear when alone
• Characteristic pathogenic belief about self: I am inadequate, needy, impotent
• Characteristic pathogenic belief about others: Others are powerful and I need their care
• Central ways of defending: Regression, reversal, avoidance
• Subtypes: Passive-Aggressive, Counterdependent
47
Dependent PD: Others are powerful and I need their care
“You’re gonna spoil that dog, Annie!”

48
P109. Dependent Personality Disorders
P109.1 Passive-Aggressive Versions of Dependent Personality Disorders
• Contributing constitutional-maturational patterns: Possibly irritable, aggressive
• Central tension/preoccupation: Tolerating mistreatment/getting revenge
• Central affects: Anger, resentment, pleasure in hostile enactments
• Characteristic pathogenic belief about self: I am inadequate, needy, impotent
• Characteristic pathogenic belief about others: Others are powerful and I need their care
• Central ways of defending: Regression, reversal, avoidance

49
Passive-Aggressive Personality Disorder
“It’s almost like they do it on purpose, isn’t it, Fred?!”

50
P109. Dependent Personality Disorders
P109.2 Converse Manifestation: Counterdependent Personality Disorder
• Contributing constitutional-maturational patterns: Possibly more aggressive than the overtly dependent type
• Central tension/preoccupation: Demonstrating lack of or shameful dependence
• Central affects: Contempt, denial of “weaker” emotions
• Characteristic pathogenic belief about self: I don’t need anyone
• Characteristic pathogenic belief about others: Others depend on me and require me to be “strong”
• Central ways of defending: Denial, reversal, enactment
51
P110. Phobic (Avoidant) Personality Disorders
• Contributing constitutional-maturational patterns: Possible anxious or timid disposition
• Central tension/preoccupation: Safety/danger relative to specific objects
• Central affects: Fear
• Characteristic pathogenic belief about self: I am safe if I avoid certain specific dangers
• Characteristic pathogenic belief about others: More powerful people can magically keep me safe
• Central ways of defending: Symbolization, displacement, projection, rationalization, avoidance
• Subtypes: Counterphobic

52
P110.1 Converse Manifestation of Phobic: Counterphobic Personality Disorders
• Contributing constitutional-maturational patterns: Unknown
• Central tension/preoccupation: Safety/danger
• Central affects: Contempt, denial of fear
• Characteristic pathogenic belief about self: I can face anything without fear
• Characteristic pathogenic belief about others: Others frighten easily and admire my bravery
• Central ways of defending: Denial, reaction formation, projection

53
P111. Anxious Personality Disorders
• Contributing constitutional-maturational patterns: Anxious or timid temperament
• Central tension/preoccupation: Safety/danger
• Central affects: Fear
• Characteristic pathogenic belief about self: I am in constant danger from forces unknown
• Characteristic pathogenic belief about others: Others are sources of either danger or protection
• Central ways of defending: Failure of defenses against anxiety, surface anxiety may mask unconscious deeper anxiety

54
P112. Obsessive-Compulsive Personality Disorders
P112.1 Obsessive: Self-esteem depends on thinking,ruminative
P112.2 Compulsive: Self-esteem depends on doing, meticulous
• Contributing constitutional-maturational patterns: Possible irritability, orderliness
• Central tension/preoccupation: Submission to/rebellion against controlling authority
• Central affects: Anger, guilt, shame, fear
• Characteristic pathogenic belief about self: My aggression is dangerous and must be controlled
• Characteristic pathogenic belief about others: Others try to exert control, which I must resist
• Central ways of defending: Isolation of affect, reaction formation, intellectualization, moralizing, undoing

55
Obsessive-Compulsive PD: Compulsive type
Once again Elliot Zambini’s tidiness ruins the act.

56
P113. Hysterical (Histrionic) Personality Disorders P113.1 Inhibited: reserved, naiveté, somatization P113.2 Demonstrative or Flamboyant: seductive, dramatic
• Contributing constitutional-maturational patterns: Possibly sensitivity, sociophila
• Central tension/preoccupation: Power and sexuality/other gender
• Central affects: Fear, shame, guilt (over competition)
• Characteristic pathogenic belief about self: My gender makes me weak, castrated, vulnerable
• Characteristic pathogenic belief about others: People of my own gender are of little value, people of the other gender are powerful, exciting, potentially exploitive and damaging
• Central ways of defending: Repression, regression, conversion, sexualization, acting out

57
P114. Dissociative Personality Disorders (Dissociative Identity Disorder/Multiple Personality Disorder)
• Contributing constitutional-maturational patterns: Constitutional capacity for self-hypnosis; severe early and repeated physical and/or sexual trauma
• Central tension/preoccupation: Acknowledging trauma/disavowing trauma
• Central affects: Fear, rage
• Characteristic pathogenic belief about self: I am small, weak, and vulnerable to recurring trauma
• Characteristic pathogenic belief about others: Others are perpetrators, exploiters, or rescuers
• Central ways of defending: Dissociation

58
P115. Mixed/Other
• For individuals with combinations of personality types or with particular patterns or themes

59
Implications for Treatment
Depressive Personality Disorder(Most Common type in Clinical Situations)
P107.1 Introjective: self-critical, preoccupied with self-worth,
guilt P107.2 Anaclitic: concerned with attachment issues, relatedness, trust, inadequacy (May combine with dependent or narcissistic personality disorder)

60
Treatment for Depressive P.D.
• The Mood disorder responds to medication, but not the personality disorder, which requires long-term intensive treatment.
• The introjective type tends to respond better to interpretations and insight.
• The anaclitic type tends to respond better to the actual therapeutic relationship. May respond well to short term interventions.

61
P107.3 Converse Manifestation: Hypomanic Personality Disorder
• Relatively stable state of inflated mood, high energy• Little guilt • Overly positive view of self• Superficial relationships due to fear of being
attached• Highly resistant to therapy• The mood disorder responds better to
pharmacological interventions, but medication does not help the personality disorder.

62
Treatment Implications:P107.3 Converse Manifestation: Hypomanic Personality Disorder
• The hypomanic type often flees from commitment and therefore does not stay long enough in treatment. The PDM suggests emphasizing that the commitment to the treatment is important to improvement.
• People with hypomanic personality disorders are most likely to be at the borderline level favoring defenses such as denial and the idealization of self and the devaluation others, as compared to those with depressive personalities who favor defensives such as repression, and the devaluation of self and the idealization of others.

63
Personality Structure and Treatment
• McWilliams points out that for many neurotic level people, the best time to make interpretations is when the patient is a state of emotional arousal, so that the patient is less likely to intellectualize the affect.
• With borderline clients, who require a supportive approach, the opposite consideration applies, because when they are very upset, it is hard for them to take anything in.

64
Take Home Message
• Neurotic Level Personality Disorders focus more on using insight into past
traumas that need to be worked through.• Borderline Level Personality Disorders focus
more on using here and now interventions to help with reality testing, better self control and self soothing.

65
Take Home Message
• Be technically eclectic mixing Supportive, CBT and Psychodynamic according to the needs of the patient (not according to your biases).
• Use a psychodynamic formulation so you will know what interventions are likely be most effective, and to communicate that you understand your patient at all levels of existence (not just seeing symptoms).

66
Consider Instruments Such as the PDC
• To guide your diagnostic and case formulation
• To keep in your chart• To assess progress

67
Take Home Message:Use the ICD with the PDM
1. Consider the over-all level of personality organization
2. Consider the personality patterns or disorders
3. Consider the mental capacities4. Consider the subjective experience of the
symptoms and use the ICD codes You will find that your greater empathy will
be felt by your patient, and this can greatly improve any treatment.

68


















