Using CPCSSN Data for Primary Care Research in Canada
46
Using CPCSSN Data for Primary Care Research in Canada Alan Kaplan MD CCFP(EM) FCFP Chairperson, Family Physician Airways Group of Canada Chairperson, Communities of Practice, Respiratory Medicine, College of Family Physicians of Canada
-
Upload
zoe-mitchell -
Category
Health & Medicine
-
view
109 -
download
2
Transcript of Using CPCSSN Data for Primary Care Research in Canada

Using CPCSSN Data for Primary Care Researchin Canada
Alan Kaplan MD CCFP(EM) FCFPChairperson, Family Physician Airways Group of Canada
Chairperson, Communities of Practice, Respiratory Medicine, College of Family Physicians of Canada

Outline
• Introduction to CPCSSN• CPCSSN Data Holdings• A Tour of CPCSSN Data Tables• Respiratory medicine in CPCSSN• Limitations in the use of CPCSSN for research• Who to contact
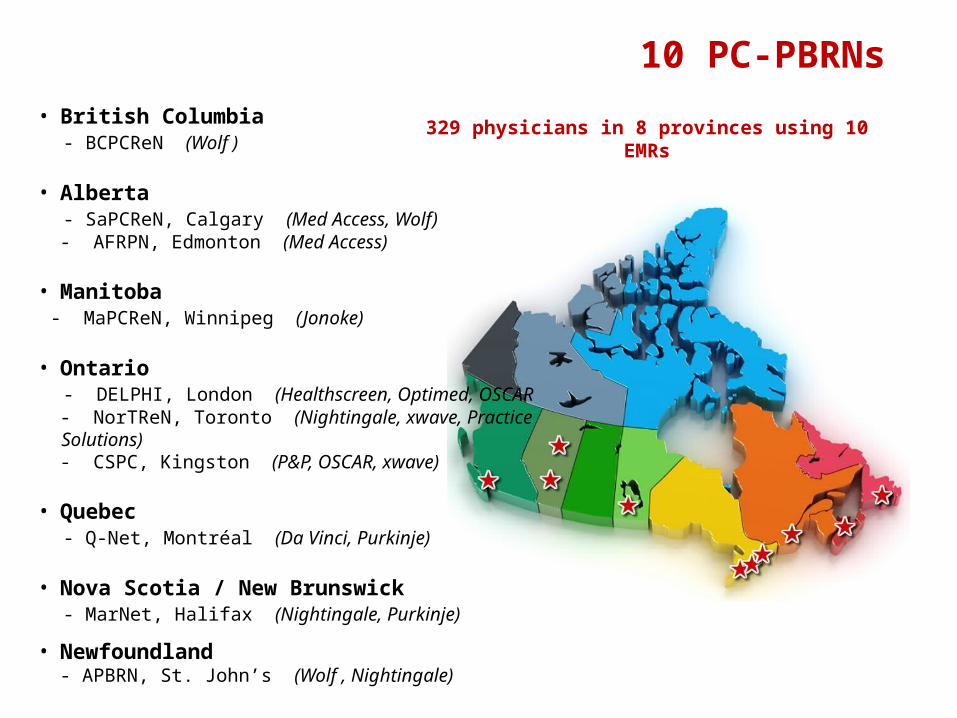
329 physicians in 8 provinces using 10 EMRs
10 PC-PBRNs• British Columbia - BCPCReN (Wolf ) • Alberta - SaPCReN, Calgary (Med Access, Wolf) - AFRPN, Edmonton (Med Access)
• Manitoba - MaPCReN, Winnipeg (Jonoke)
• Ontario - DELPHI, London (Healthscreen, Optimed, OSCAR - NorTReN, Toronto (Nightingale, xwave, Practice Solutions) - CSPC, Kingston (P&P, OSCAR, xwave)
• Quebec - Q-Net, Montréal (Da Vinci, Purkinje)
• Nova Scotia / New Brunswick - MarNet, Halifax (Nightingale, Purkinje)
• Newfoundland - APBRN, St. John’s (Wolf , Nightingale)
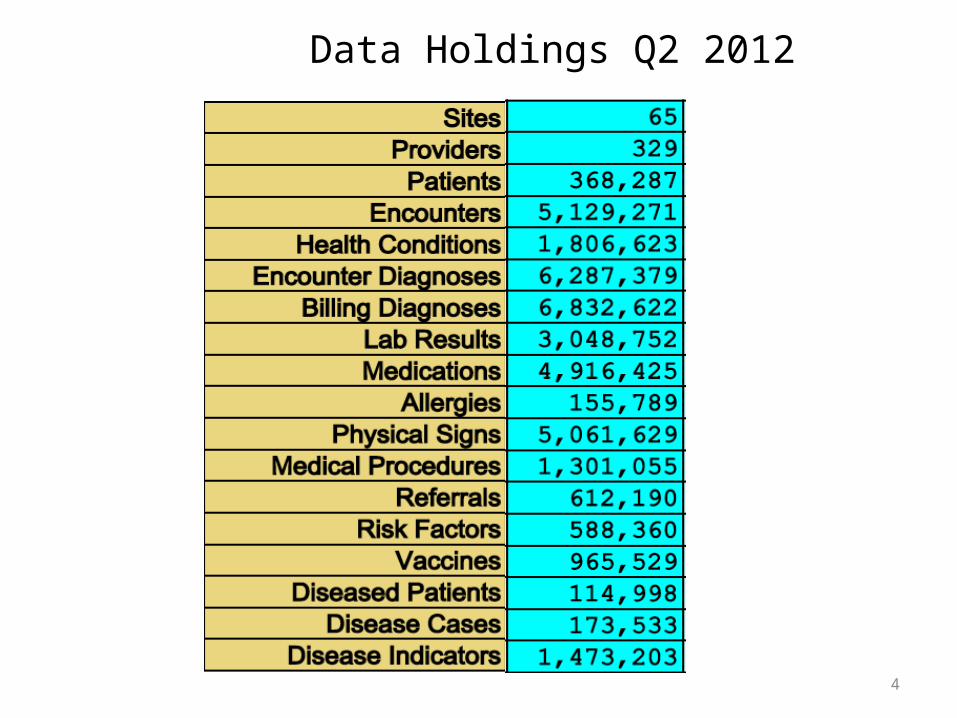
Data Holdings Q2 2012
4
5
Data Cleaning/Recoding
• Currently clean and recode the following fields
• Billing, Encounter and Problem List Diagnoses (ICD9)• Medications (ATC)• Lab results (LOINC)• Referrals (SNOMED CT)• Physical signs (Wt, Ht, BP, unit conversion, calculate BMI)• Vaccines (ATC)• Risk factors (smoking, alcohol, diet --Text)

6Patient Demographics
} < 5%
} < 5%
368,000 Records
7
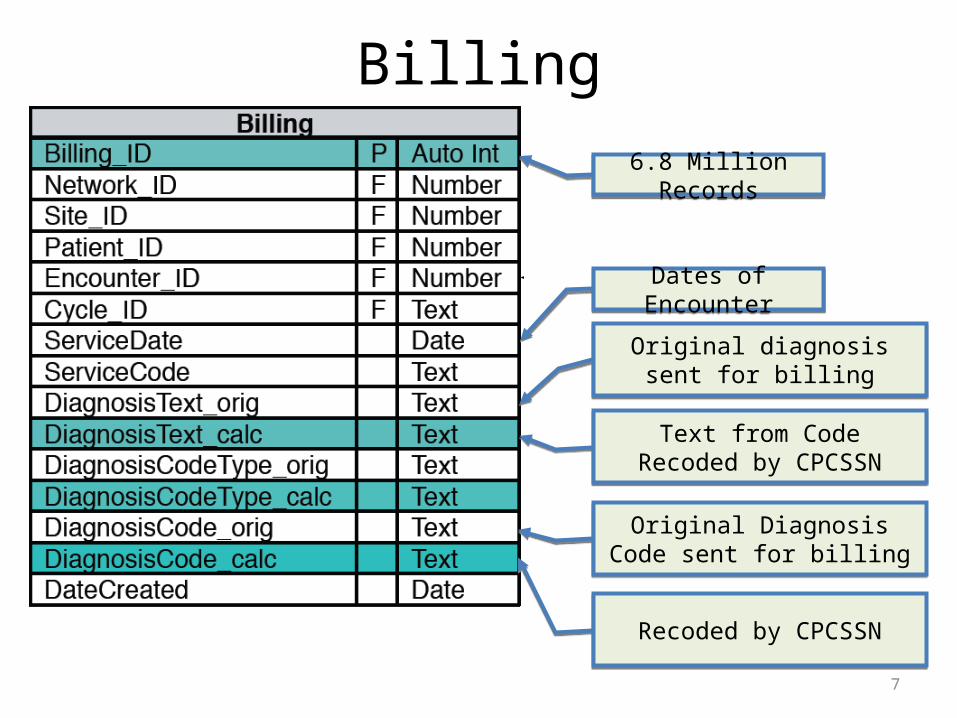
Billing
6.8 Million Records
Dates of Encounter
Original diagnosis sent for billing
Text from Code Recoded by CPCSSN
Original Diagnosis Code sent for billing
Recoded by CPCSSN

8
Research Discussion
• Useful for case finding• Useful for understanding deficiencies of using
billing information for clinical research
• There is some inconsistency in use of billing codes across the country
• CPCSSN attempts to recode all billing diagnosis codes to a standard version

9
Encounters
5.1 Million Records
Dates of Encounter
Data inconsistent across the Country
CPCSSN Cleaning Not Started
Active area of CleaningE.g., Office Visit, Phone, E-mail etc

Problem List Diagnoses
10
Original Diagnosis Written by UserE.g. DMT2
Recoded by CPCSSNE.g., Diabetes Mellitus, Type 2
} Not well populated
1.8 Million Records
Active = Problem ListInactive = Past Medical History

Problem List Diagnoses
11
List of cleaned up diagnoses
Chronic airway obstruction, not elsewhere classified (496)Bronchitis, not specified as acute or chronic (490)Chronic bronchitis (491)Emphysema (492)Diabetes mellitus (250)Depressive disorder, not elsewhere classified (311)Suicide and self-inflicted poisoning by solid or liquid substances (E590)Suicidal ideation (V62.84) Adjustment reaction (309)Post traumatic stress disorder (309.81)Major depressive disorder, recurrent episode (296.3)Bipolar I disorder, most recent episode (or current) (296.7)Mental disorders complicating pregnancy, childbirth, or the puerperium (648.4)Essential hypertension (401)Osteoarthrosis and allied disorders (715)Spondylosis and allied disorders (721)Total knee replacement (81.54)Total hip replacement (81.51)Polycystic ovarian syndrome (256.4)Abnormal glucose tolerance of mother complicating pregnancy childbirth or the puerperium (648.8)Secondary diabetes mellitus (249)
MORE BEING ADDED SOON
Other abnormal glucose (790.29)Migraine (346)Heart failure (428)Acute myocardial infarction (410)Old myocardial infarction (412)Other forms of chronic ischemic heart disease (414)Cardiac dysrhythmias (427)Essential and other specified forms of tremor (333.1)Esophageal varices with bleeding (456.0)Esophageal varices without bleeding (456.1)Angina pectoris (413)Other acute and subacute forms of ischemic heart disease (411)Calculus of kidney and ureter (592)Portal hypertension (572.3)Asthma (493)Dementias (290)Alzheimer's disease (331.0)Dementia with lewy bodies (331.82)Parkinson's disease (332)Epilepsy and recurrent seizures (345)Epileptic convulsions, fits, or seizures nos (345.9)

12
Research Discussion
• Sensitivity and specificity of problem list diagnoses not currently known, so cannot determine incidence and prevalence of disease from problem list alone
13
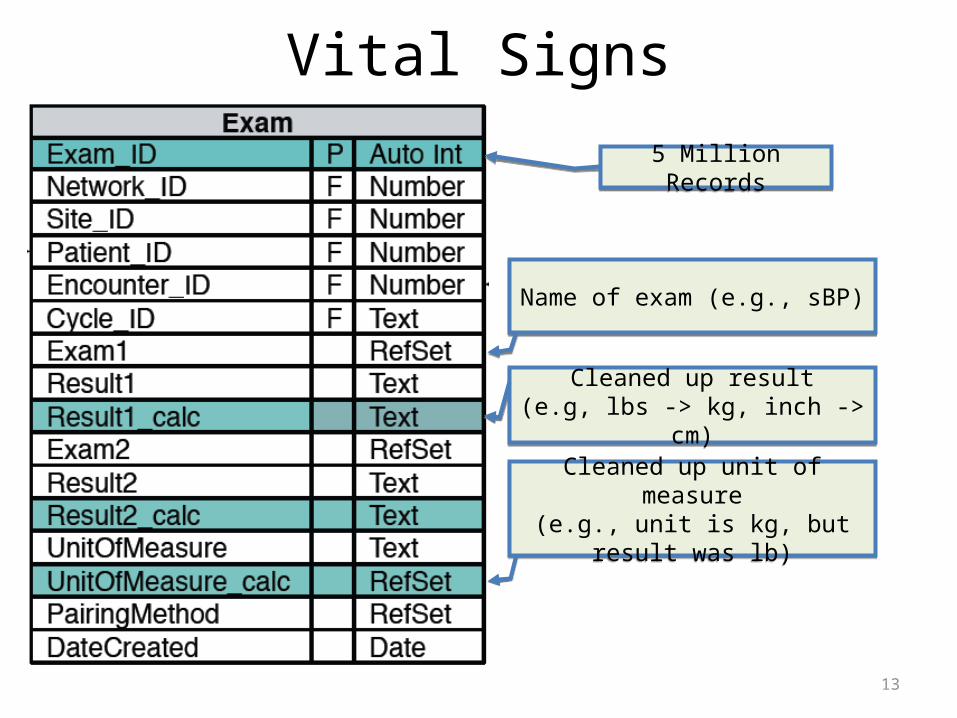
Vital Signs
Name of exam (e.g., sBP)
Cleaned up result(e.g, lbs -> kg, inch -> cm)
5 Million Records
Cleaned up unit of measure(e.g., unit is kg, but result was lb)
14
Research Discussion
• Currently have access to– sBP/dBP– Ht– Wt– BMI– Waist circumference
15
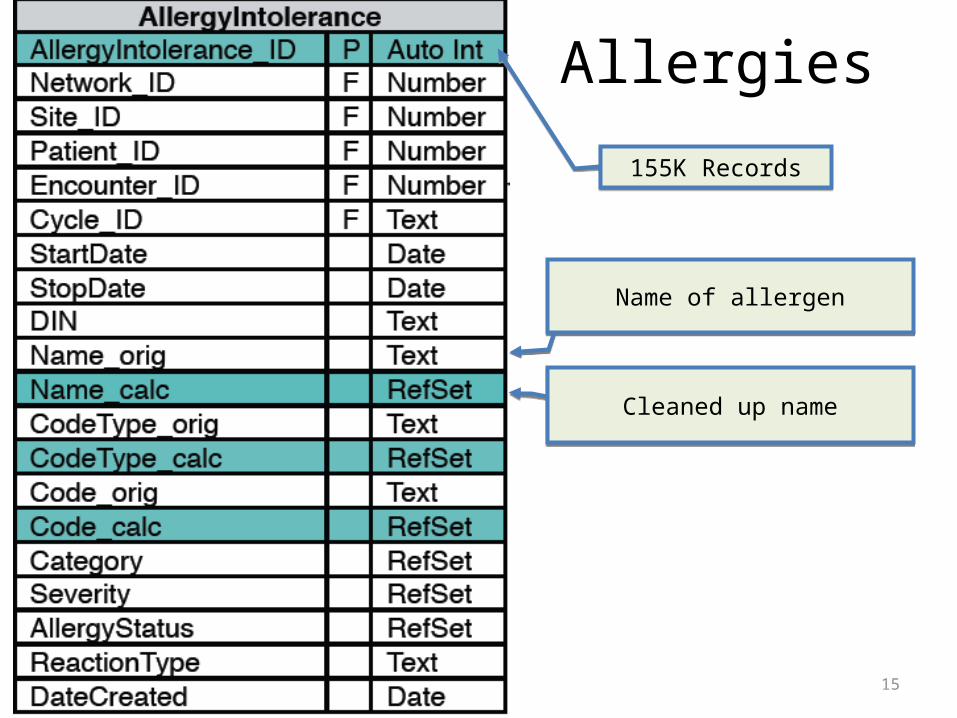
Allergies
Name of allergen
Cleaned up name
155K Records
16
Research Discussion
• Not yet cleaned, but will soon clean it• Focus of cleaning will be on medication
allergies– All other allergies will be retained as original text
• Useful when assessing why patients are not receiving medications for a particular disease

17
Risk Factors
Name of Risk Factor (e.g., smoking)
Cleaned up version of Risk Factors.
588K Records
Working on cleaning up Current Exposures & Cumulative Exposures

18
Laboratory Results
Original Lab Result Name(e.g., Hb A1c, HGbA1c, etc)
Recoded by CPCSSN 100% LOINC(e.g., HBA1C)
3 Million Records

19
Research Discussion• Currently only capturing the following
• One site does not capture labs yet
HDLTRIGLYCERIDESLDLTOTAL CHOLESTEROLFASTING GLUCOSEHBA1CURINE ALBUMIN CREATININE RATIOMICROALBUMINGLUCOSE TOLERANCE
20
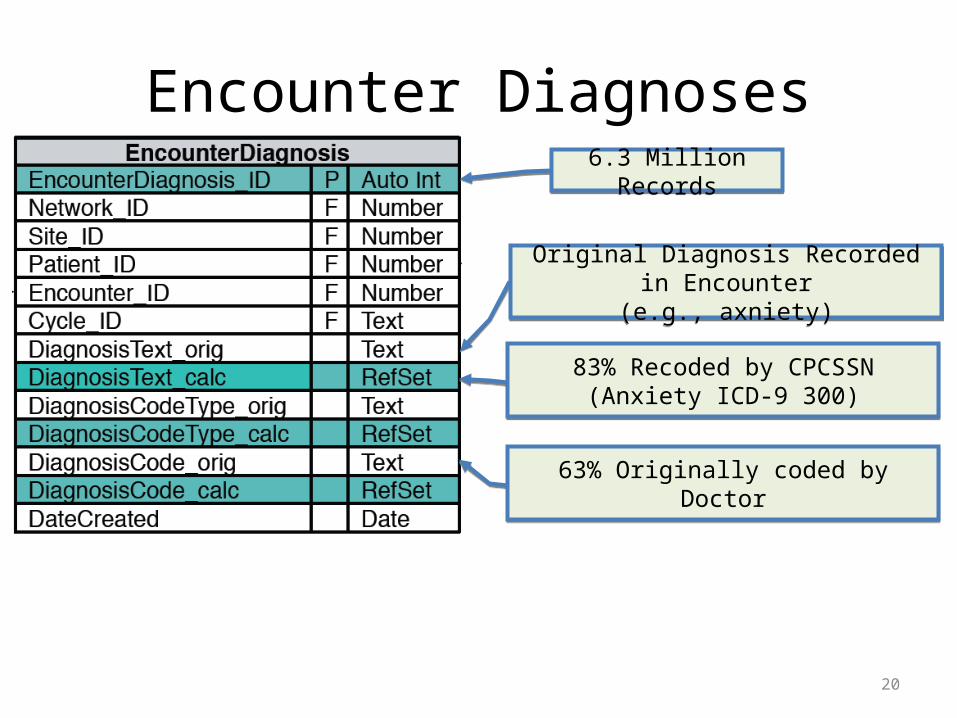
Encounter Diagnoses
Original Diagnosis Recorded in Encounter(e.g., axniety)
83% Recoded by CPCSSN(Anxiety ICD-9 300)
6.3 Million Records
63% Originally coded by Doctor

21
Research Discussion
• Not all EMRs capture Encounter Diagnoses in a structured manner
• This table is not ready for prime time across all sites, but may be useful for projects where data from just a few sites is acceptable

Medications
22
What the doctor orderedE.g., HCTZ 25 mg bid
91% Recoded by CPCSSNE.g., Hydrochlorthiazide
56% Coded as DIN
Strength 56%Dose 70%
Unit of Measure 84%Frequency 95%Duration 52%
Dispensed 86%
72% Coded by doctor (DIN + other)
91% Coded by CPCSSN (ATC)
4.9 Million Records
}
23
Research Discussion
• Medication name data is relatively clean• Medications coded as ATC
– Allows easy grouping by class
• Don’t have daily dose and months supply for many records –working on clean up

24
Referrals
Original Text of Referral
80% Recoded by CPCSSNSNOMED-CT
600 K Records
25
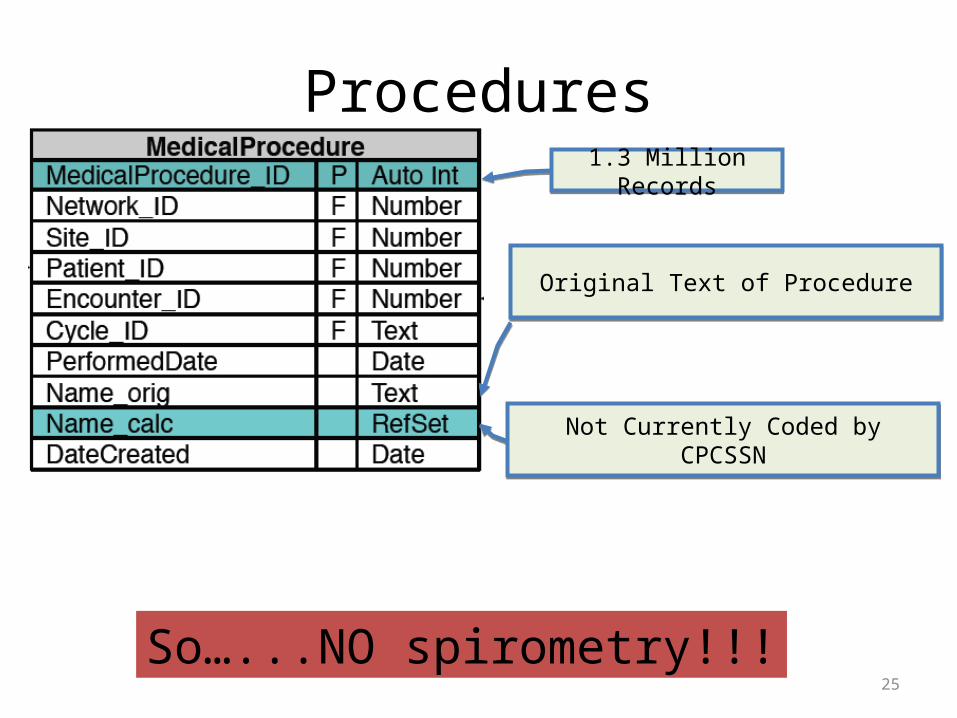
Procedures
Original Text of Procedure
Not Currently Coded by CPCSSN
1.3 Million Records
So…...NO spirometry!!!

26
Vaccines
What the doctor typed
93% Recoded by CPCSSN (ATC)
960 K Records
46% Coded by Doctor (DIN)
27
Limitations for Respiratory Disease
Currently studying 8 conditions:five chronic and mental health conditions
-hypertension, osteoarthritis,
diabetes, COPD and depression)
and three neurologic conditions
-Alzheimer’s and related dementias,
epilepsy and Parkinson’s disease.


Asthma –Text Diagnoses• Asthma 1996 1st time in life• Asthma 1999 ASTHMA 3 years• Asthma age 10• asthma and allergies• asthma and bronchitis • asthma attack postoperatively (493.) • Asthma- class IV work related • Asthma Condition • asthma diabetes • asthma diagnosed in 1999 and treated with rhinocort, ventolin and beclovent. off
all meds since a short course of treatment. • ?asthma equivalent cough
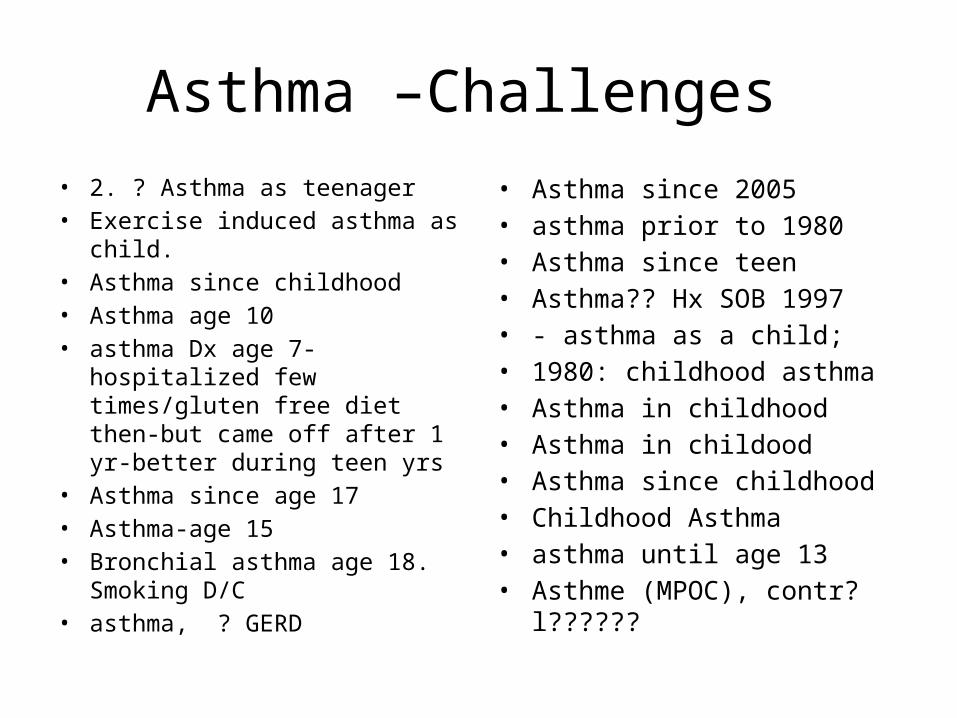
Asthma –Challenges • 2. ? Asthma as teenager • Exercise induced asthma as child. • Asthma since childhood• Asthma age 10• asthma Dx age 7-hospitalized few
times/gluten free diet then-but came off after 1 yr-better during teen yrs
• Asthma since age 17• Asthma-age 15 • Bronchial asthma age 18.
Smoking D/C • asthma, ? GERD
• Asthma since 2005• asthma prior to 1980 • Asthma since teen• Asthma?? Hx SOB 1997• - asthma as a child; • 1980: childhood asthma • Asthma in childhood• Asthma in childood• Asthma since childhood • Childhood Asthma • asthma until age 13 • Asthme (MPOC), contr?l??????

Smoking
• Smoking data in EMRs is particularly challenging• Most EMRs capture smoking data as text• There are a lot of ways to say ‘the patient does not
smoke’– Quit, ex-, non-, smoking =0, x-– Makes separating ex-/non- from smokers difficult using an
algorithmic approach• Dates are poorly captured• Cumulative exposure is poorly captured
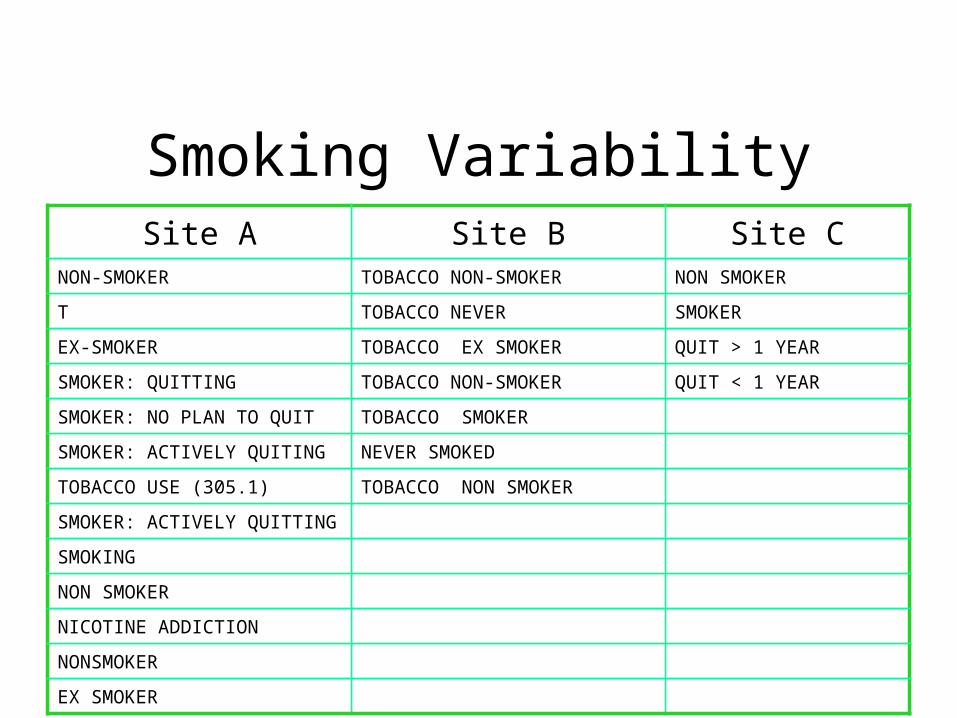
Smoking VariabilitySite A Site B Site C
NON-SMOKER TOBACCO NON-SMOKER NON SMOKER
T TOBACCO NEVER SMOKER
EX-SMOKER TOBACCO EX SMOKER QUIT > 1 YEAR
SMOKER: QUITTING TOBACCO NON-SMOKER QUIT < 1 YEAR
SMOKER: NO PLAN TO QUIT TOBACCO SMOKER
SMOKER: ACTIVELY QUITING NEVER SMOKED
TOBACCO USE (305.1) TOBACCO NON SMOKER
SMOKER: ACTIVELY QUITTING
SMOKING
NON SMOKER
NICOTINE ADDICTION
NONSMOKER
EX SMOKER
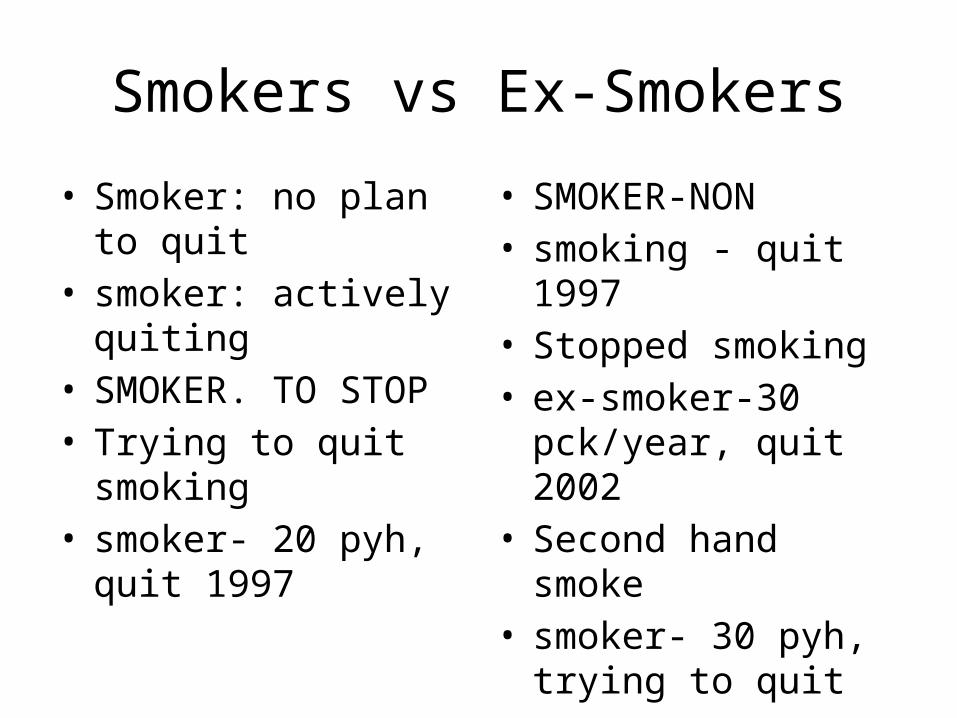
Smokers vs Ex-Smokers
• Smoker: no plan to quit • smoker: actively quiting • SMOKER. TO STOP• Trying to quit smoking• smoker- 20 pyh, quit
1997
• SMOKER-NON• smoking - quit 1997• Stopped smoking • ex-smoker-30 pck/year,
quit 2002 • Second hand smoke • smoker- 30 pyh, trying
to quit

Improving Smoking Data
• Smoking data is uniformly poor across the country and across EMRs
• EMRs don’t have structured data entry templates for smoking status
• EMRs need to be able to capture– Status: Smoker –Current, Former, Never– Current exposure: cig/day– Cumulative exposure: Pack-year history
36
Other groups working on this:
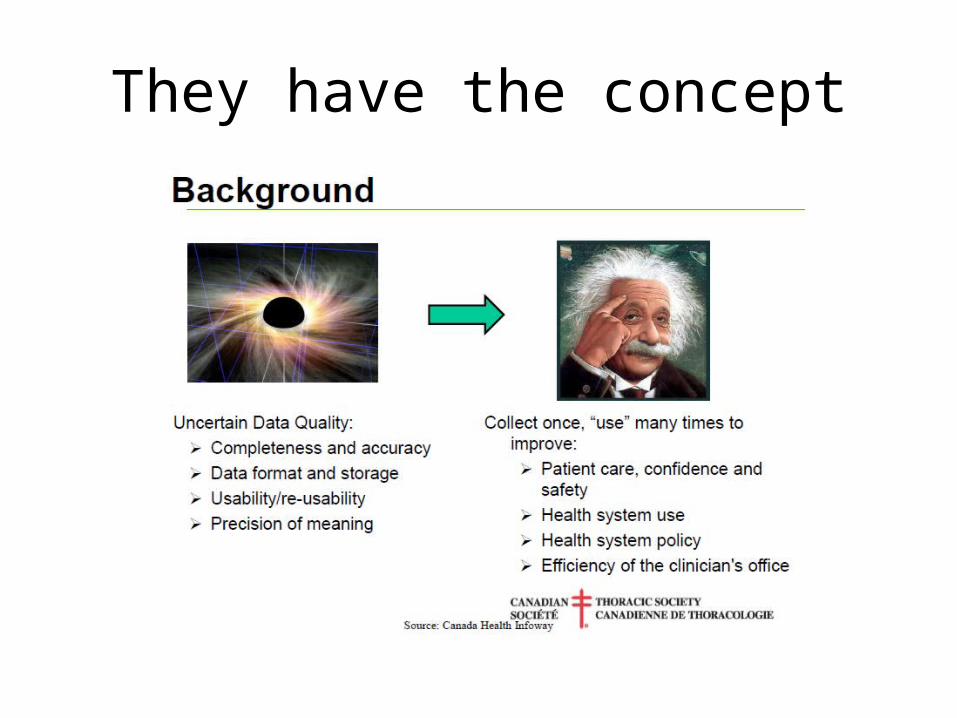
They have the concept

But, as of yet, no liasons…

Metropolitan Toronto database
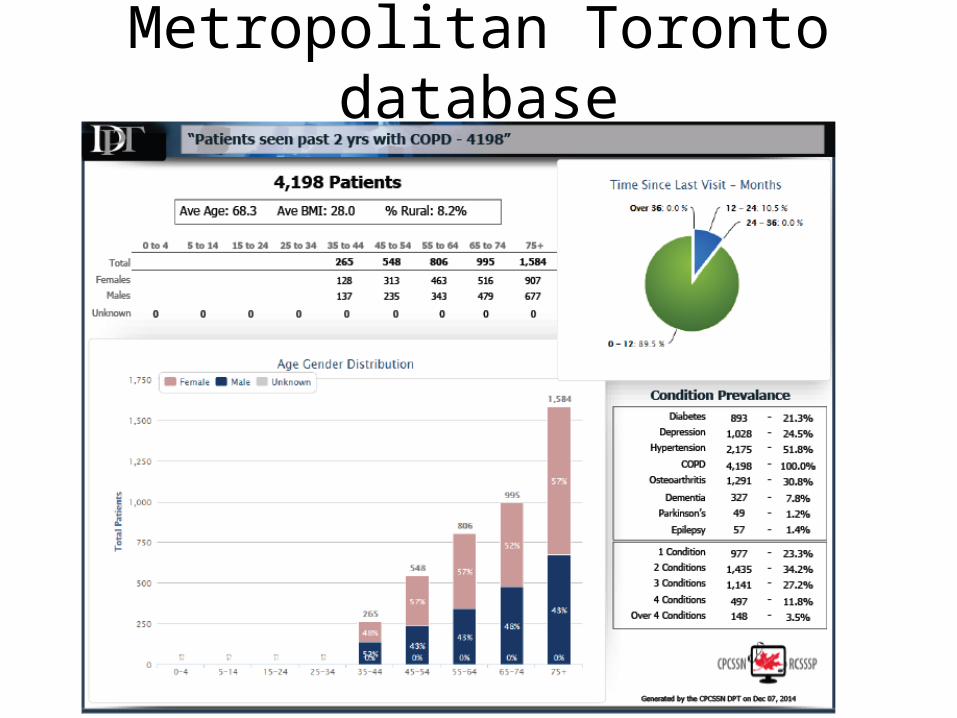
Metropolitan Toronto database

Research Opportunities• Population Health and Epidemiological Studies
– Incidence/Prevalence of disease– Impact of SES on health– Rates of treatment for diseases– Rates of disease control– Burden of illness and multi-morbidity
• Clinical –database studies– Comparative effectiveness– Case-Control– Exposure-Outcome– Quality Improvement– Associations– Intervention-Outcome– Guideline effectiveness
41
42
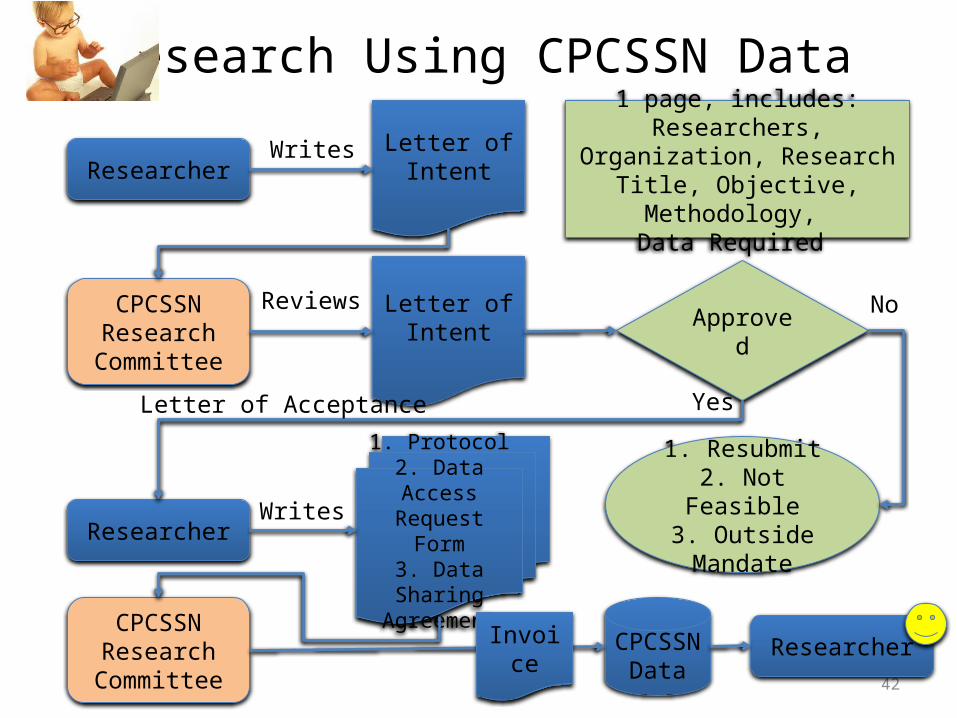
Research Using CPCSSN Data
ResearcherLetter of
Intent
CPCSSN Research
Committee
Writes
Letter of Intent
Reviews
1 page, includes: Researchers, Organization, Research Title,
Objective, Methodology, Data Required
Approved
1. Resubmit2. Not Feasible
3. Outside Mandate
No
Researcher
1. Protocol2. Data Access Request Form
3. Data Sharing Agreement
Letter of Acceptance Yes
Writes
CPCSSN Research
Committee
CPCSSN Data
ResearcherInvoice

43
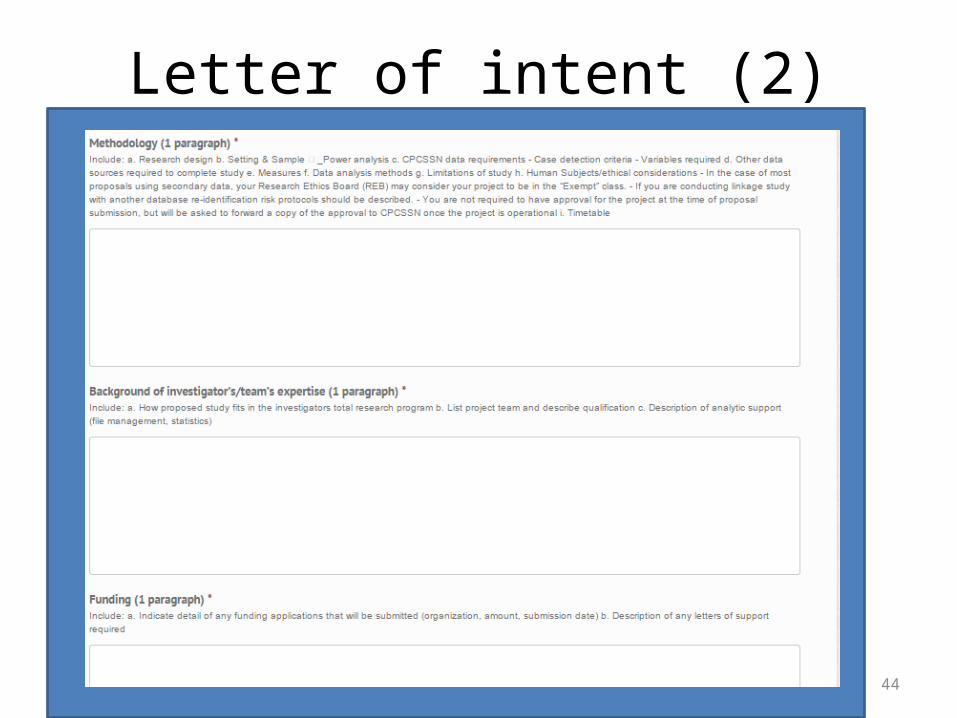
Letter of intent
44
Letter of intent (2)

CPCSSN ContactTyler Williamson, Senior Epidemiologist Canadian Primary Care Sentinel Surveillance Network
Centre for Studies in Primary CareQueen’s UniversityKingston ON K7L 5E9
Tel: (613) 533-9300, Ext. 73838Fax: (613) 533-9302e-mail: [email protected]
Mine: [email protected]
So, I have an opportunity to do a study with COPD, at least in Toronto group
• With what I have shown you, what would you suggest I do?
• Is there an opportunity to work with any of your existing projects?
• And then…funding…..