Study of malcolm baldrige health care criteria effectiveness and organizational performance

Using Baldrige Criteria to Achieve Performance ExcellencePatient Safety Improvement
atSSM Health Care
The Quality Colloquium at Harvard
August 27, 2003Presented by: Andrew Kosseff, MD, FACP
Medical Director of System Clinical Improvement

Agenda
SSM Health Care and MBNQA
Patient safety improvement

SSM Health Care (SSMHC)
Large Catholic health care system - St. Louis21 Hospitals, 3 nursing homes, home health care 4 Midwestern states5000 Physicians23,000 Employees$2 Billion revenue / year

1990 - CQI model adopted
1995 – MBNQA criteria added
1999 – MBNQA applications
The MBNQA Effort

Strong, committed leadershipMission centeredPerseveranceAttention to MBNQA feedback Conviction that the pursuit made us better
The Precursors of The MBNQA

Through our exceptional health care services,we reveal the healing presence of God
SSMHC’s Mission
Attend to our missionHave goals consistent with our missionHave mature improvement processesImplement effective system improvement initiativesUse comparisons to “best in class”
What MBNQA Means to SSMHC

Safety and Clinical ImprovementsSSMHC Clinical Collaboratives
Safety and Clinical ImprovementsSSMHC Clinical Collaboratives
The SSMHC Environment and The Clinical Collaboratives
The mission
The commitment to CQI
Our experience with the IHI Breakthrough Series

The Concept
By working together we can improve systemclinical performance resulting in exceptionalpatient care

Collaboratives 85 collaborative teams
Improving the Secondary Prevention of Ischemic Heart Disease ( Secondary Prevention) - 1/99
Improving Prescribing Practices (IPP) - 5/99
Using Patient Information to Improve Care (UPI) - 11/99
Enhancing Patient Safety Through Safe Systems (EPS) - 3/00
Improving the Treatment of Congestive Heart Failure (CHF) - 11/00
Achieving Exceptional Safety in Health Care (AES) - 1/02

Start of CollaborativeDesign
Collaborative
Prework
Continuous Improvement Phase
Active phase
Send out invitation
Team formation and data collection
Learning session #1
Project work and completion
Learning session #2, 3
Secondary Prevention
Data collection every 3 months
Conference calls every 2
months
CHF
AES

SSMHC’s Safety Improvement History
Pre - IOMIndividual caregiver and entity effortsIHI Collaborative – medication safetySSMHC Clinical Collaboratives
Post - IOMEnhancing Patient Safety Collaborative(EPS)Safety infrastructure changesAchieving Exceptional Safety Collaborative(AES)

Achieving Exceptional Safety in Health Care (AES)
Jan., 2002 .........Goal for the collaborativeTo have each entity adopt and implement 16 + recommended safety practices 3 year collaborative with 22 entities enrolled

16 + Recommended Practices1. Implement a near miss reporting system2. Eliminate dangerous abbreviations3. Design and implement an accurate patient medication list at
admission and discharge and avoid "home" medication and blanket orders
4. Implement an effective disclosure of unanticipated outcomes process
5. Provide and use protocols for high risk medications6. Implement a fall reduction process7. Implement a sentinel event review process8. Establish an entity Safety Center Team
Achieving Exceptional Safety in Health Care (AES)
yellow - upcoming collaborative recommended practice black - recommended practice in progress

16 + Recommended Practices9. Provide pharmacy rounding in ICU's10. Implement all recommended safety information technology
advances11. Implement 24 hour pharmacy coverage12. Provide a quarterly "state of safety report"13. Develop a protocol for proper timing of surgical antibiotic
prophylaxis14. Institute a needleless IV system15. Implement a protocol for glucose management of diabetic
patients undergoing surgery16. Implement a surgical site marking procedure to avoid
wrong limb surgery17. Effectively implement all JCAHO National Patient Safety
Goals18. Improve hand washing
Achieving Exceptional Safety in Health Care (AES)

Achieving Exceptional Safety in Health Care
Good
Use of Four Dangerous AbbreviationsAve. Performance of Collaborative Entities
0%
5%
10%
15%
20%
25%
Baseline Jan02(20)
March, 02(19) June, 02(20) Sept, 02(18) Dec, 02(19) March, 03(14)
Time of data collection
Per
cen
t u
se o
f D
As
SSMHC use of DAsEliminate “QD” for dailyEliminate “U” for unitsEliminate trailing zerosUse leading zeros

Achieving Exceptional Safety in Health Care
Good
Use of "QD" Instead of DailyAve. Performance of Collaborative Entities
0%
10%
20%
30%
40%
50%
60%
70%
BaselineJan02(19)
March, 02(18) June, 02(17) Sept, 02(14) Dec, 02(13) March, 03(12)
Time of data collection
Per
cen
t u
se o
f "Q
D"
SSMHC use of DAs

Achieving Exceptional Safety in Health Care
Good
Use of "Blanket Orders" Ave. Performance of Collaborative Entities
0%5%
10%15%20%25%30%35%40%45%
Baseline 2002 (14) March '03 (16) July '03 (17)
Time of data collection
Pe
rce
nt
us
e o
f "b
lan
ke
t o
rde
rs"
SSMHC Use of blanket orders

Near Miss Reporting and Safety Process Changes
Stimulate near miss reportingDemonstrate safety process changesMagnify benefits by collaborative sharing
Achieving Exceptional Safety in Health Care (AES)

Near Miss Safety Process Changes
Pharmacy staff re-educated on placement of narcotics in Pyxis
Enforced the transfer checklist that includes the process of discarding old labels on 3ICU
Near miss involving two look alike injectables being next to each other in Pyxis led to moving one of the meds to a different drawer
Separated out the different types of insulin in Pyxis, into different bins so staff are sure to pull the right type of insulin
Reviewing process use to document patient weights; changes recommended are to remove “lbs” and use “kg” on all forms andcomputer systems.
Achieving Exceptional Safety in Health Care (AES)
Near Miss Safety Process ChangesLiquid theophylline is available in pharmacy, as only thenonalcoholic type, to prevent the alcohol type being given toinfants/pediatric patients
Orange stripe on NG tube to avoid confusion w/ IV lines
Better identification of patients in “A” bed and “B” bed
Noted confusion re: acute coronary syndrome orders andthrombolytic orders, so revision of orders and education of staff was done
Stopped the practice of staff being able to override the lockout mode on PCA pumps.
Achieving Exceptional Safety in Health Care (AES)

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
base
line (
1/99)
April,
99Ju
ne, 9
9Sep
t. 99
June
, 00
Dec., 0
0Marc
h, 01
July,
01Dec
., 01
March,
02Ju
ne, 0
23rd
qrt02
(8)4th
qrt02
(7)1s
tqrt0
3(6)
Time of data collection
Per
cent
of M
I pat
ient
s tr
eate
d w
ith L
LA's
SSM average
Benchmark 00
Benchhmark 02
better
8 new entities join
Mehta, RH et al. Quality Improvement Initiative and Its Impact on the management of Patients with Myocardial Infarction. Arch Intern Med. 2000; 160: 3057-3062 Mehta, RH et al. Improving the Quality of Care for Acute Myocardial Infarction. JAMA 2002; 287: 1269-76.
Secondary PreventionPercent of MI patients treated with Lipid Lowering Agents (LLA's)
Average Performance of Collaborative Hospitals
Core measures
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
baseline (3-01)July, 01
Dec., 01March, 02
June, 023rdqrt02(11)
4thqrt02(9)1stqrt03(10)
Time of data collection
% M
I pat
ient
s di
scha
rged
on
beta
bl
ocke
rs
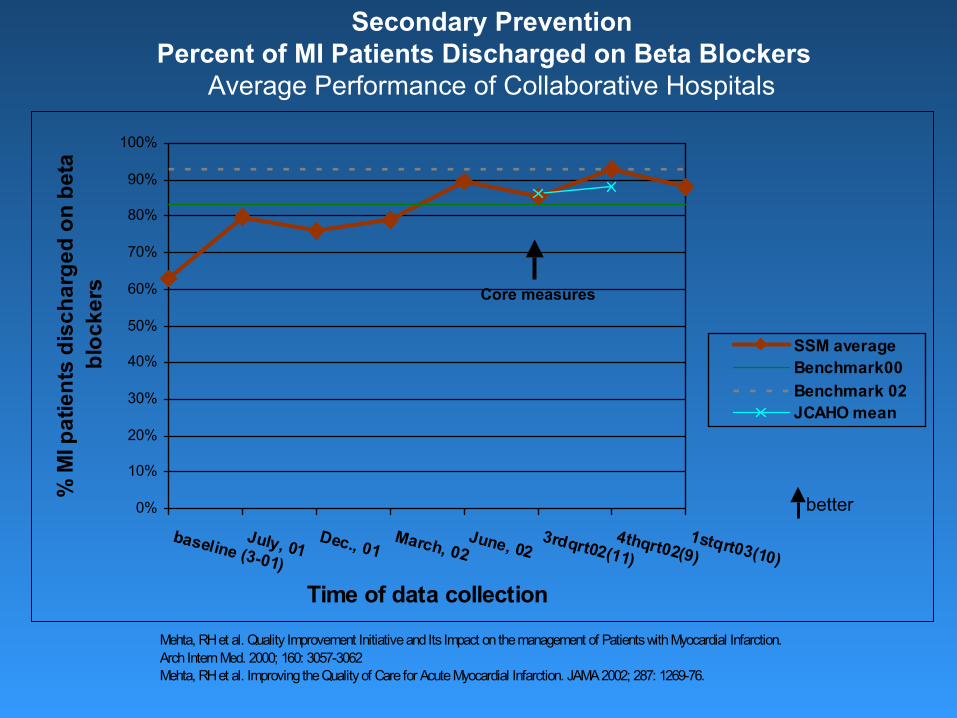
SSM averageBenchmark00Benchmark 02JCAHO mean
Secondary PreventionPercent of MI Patients Discharged on Beta Blockers
Average Performance of Collaborative Hospitals
better
Mehta, RH et al. Quality Improvement Initiative and Its Impact on the management of Patients with Myocardial Infarction. Arch Intern Med. 2000; 160: 3057-3062 Mehta, RH et al. Improving the Quality of Care for Acute Myocardial Infarction. JAMA 2002; 287: 1269-76.
Core measures

Results of SSMHC’s Collaborative Safety Improvement Efforts
Progress towards safer patient care
Recognition that patient safety is a top priority
Unexpected benefits and adventures

Andy Kosseff [email protected] 608-238-1337
For more detailed information about MBNQA:visit SSM’s website at www.ssmhc.com
or contact Paula Friedman, VP of System Improvement at 314-994-7840