Use of Cyclosporine A and Tacrolimus in Treatment of Vernal Keratoconjunctivitis
7
ALLERGIC AND IMMUNOLOGIC DISORDERS OF THE EYE AND NERVOUS SYSTEM (CH KATELARIS, SECTION EDITOR) Use of Cyclosporine A and Tacrolimus in Treatment of Vernal Keratoconjunctivitis Pakit Vichyanond & Panida Kosrirukvongs Published online: 28 April 2013 # Springer Science+Business Media New York 2013 Abstract Vernal keratoconjunctivitis is a sight-threatening inflammatory disease of conjunctiva and cornea. It is fre- quently observed in young children with the onset usually occurring in the first decade of life. Mild cases of VKC tend to remit with nonspecific and supportive therapy. In con- trast, severe cases are usually more protracted with remission/relapse occurring for a prolonged period of time. Although VKC is classified as an allergic eye condition, the role of allergens as an inciting factor is not clear. Pathogenesis of VKC involves roles for IgE, cytokines, chemokines, and inflammatory cells (T and B lymphocytes, mast cells, basophils, neutrophils, and eosinophils) with the release of their granular proteins, proliferation of fibroblasts, and laying down exuberant amounts of collagen fibers in the conjunctival tissue. In severe VKC cases—often of tarsal VKC—diagnostic giant papilla are classically observed on the upper tarsal plate, giving the classic ‘cobble-stone’ ap- pearance. Corneal ulcer can occur from the effect of eosin- ophilic granular proteins on corneal epithelium and by physical trauma by intense eye rubbing. Topical corticoste- roids, often required for controlling symptoms and signs in severe VKC, can lead to serious ocular complications. Immunomodulators that have been investigated for VKC treatment include topical ocular preparations of cyclospor- ine A and tacrolimus. Severe VKC responds promptly to topical cyclosporine A and tacrolimus, mostly within 1 month of therapy. Prolonged use of cyclosporine A and tacrolimus in VKC is safe and is tolerated by most patients without significant side effects. Recent investigations on the use of these two agents in VKC are the main purpose of this review. The use of cyclosporine A and tacrolimus are a major breakthrough in treatment for severe VKC, a debili- tating allergic eye disease in children. Keywords Vernal keratoconjunctivitis . VKC . Cyclosporine A . CsA . Tacrolimus . FK-506 Abbreviations AD Atopic dermatitis CsA Cyclosporine A FK-506 Tacrolimus VKC Vernal keratoconjunctivitis Introduction Vernal keratoconjuctivitis (VKC) is a severe inflammatory ocular disease involving conjunctiva and cornea. It can be viewed as the severe end of the spectrum of allergic eye disease, despite the fact that pathogenesis of VKC may not be entirely ‘allergy’ related’. It generally occurs in young children with the age of onset around 4–7 years [1–3]. If not properly treated, the disease can continue into late childhood and adolescence. Although many cases of VKC spontane- ously enter a remission phase, in some the disease continues into adulthood. VKC is a sight-threatening disease and can lead to blindness due to various reasons such as corneal opacity, glaucoma, and cataract. VKC is diagnosed by its classic presenting symptoms and signs. The patients are usually males around 10 years of age [3]. They generally present with intense eye itching and rubbing, eye irritation, tearing, ropy and thick eye discharge, and photophobia. Generally, three major types P. Vichyanond Division of Allergy and Immunology, Faculty Of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand P. Kosrirukvongs Department Of Ophthalmology, Faculty Of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand P. Vichyanond (*) Department Of Pediatrics, Faculty of Medicine Siriraj Hospital, Mahidol University, 2 Prannok Street, Bangkok 10110, Thailand e-mail: [email protected] Curr Allergy Asthma Rep (2013) 13:308–314 DOI 10.1007/s11882-013-0345-0
Transcript of Use of Cyclosporine A and Tacrolimus in Treatment of Vernal Keratoconjunctivitis

ALLERGIC AND IMMUNOLOGIC DISORDERS OF THE EYE AND NERVOUS SYSTEM (CH KATELARIS, SECTION EDITOR)
Use of Cyclosporine A and Tacrolimus in Treatmentof Vernal Keratoconjunctivitis
Pakit Vichyanond & Panida Kosrirukvongs
Published online: 28 April 2013# Springer Science+Business Media New York 2013
Abstract Vernal keratoconjunctivitis is a sight-threateninginflammatory disease of conjunctiva and cornea. It is fre-quently observed in young children with the onset usuallyoccurring in the first decade of life. Mild cases of VKC tendto remit with nonspecific and supportive therapy. In con-trast, severe cases are usually more protracted withremission/relapse occurring for a prolonged period of time.Although VKC is classified as an allergic eye condition, therole of allergens as an inciting factor is not clear.Pathogenesis of VKC involves roles for IgE, cytokines,chemokines, and inflammatory cells (T and B lymphocytes,mast cells, basophils, neutrophils, and eosinophils) with therelease of their granular proteins, proliferation of fibroblasts,and laying down exuberant amounts of collagen fibers in theconjunctival tissue. In severe VKC cases—often of tarsalVKC—diagnostic giant papilla are classically observed onthe upper tarsal plate, giving the classic ‘cobble-stone’ ap-pearance. Corneal ulcer can occur from the effect of eosin-ophilic granular proteins on corneal epithelium and byphysical trauma by intense eye rubbing. Topical corticoste-roids, often required for controlling symptoms and signs insevere VKC, can lead to serious ocular complications.Immunomodulators that have been investigated for VKCtreatment include topical ocular preparations of cyclospor-ine A and tacrolimus. Severe VKC responds promptly totopical cyclosporine A and tacrolimus, mostly within
1 month of therapy. Prolonged use of cyclosporine A andtacrolimus in VKC is safe and is tolerated by most patientswithout significant side effects. Recent investigations on theuse of these two agents in VKC are the main purpose of thisreview. The use of cyclosporine A and tacrolimus are amajor breakthrough in treatment for severe VKC, a debili-tating allergic eye disease in children.
Keywords Vernal keratoconjunctivitis . VKC .
Cyclosporine A . CsA . Tacrolimus . FK-506
AbbreviationsAD Atopic dermatitisCsA Cyclosporine AFK-506 TacrolimusVKC Vernal keratoconjunctivitis
Introduction
Vernal keratoconjuctivitis (VKC) is a severe inflammatoryocular disease involving conjunctiva and cornea. It can beviewed as the severe end of the spectrum of allergic eyedisease, despite the fact that pathogenesis of VKC may notbe entirely ‘allergy’ related’. It generally occurs in youngchildren with the age of onset around 4–7 years [1–3]. If notproperly treated, the disease can continue into late childhoodand adolescence. Although many cases of VKC spontane-ously enter a remission phase, in some the disease continuesinto adulthood. VKC is a sight-threatening disease and canlead to blindness due to various reasons such as cornealopacity, glaucoma, and cataract.
VKC is diagnosed by its classic presenting symptomsand signs. The patients are usually males around 10 yearsof age [3]. They generally present with intense eye itchingand rubbing, eye irritation, tearing, ropy and thick eyedischarge, and photophobia. Generally, three major types
P. VichyanondDivision of Allergy and Immunology, Faculty Of Medicine SirirajHospital, Mahidol University, Bangkok, Thailand
P. KosrirukvongsDepartment Of Ophthalmology, Faculty Of Medicine SirirajHospital, Mahidol University, Bangkok, Thailand
P. Vichyanond (*)Department Of Pediatrics, Faculty of Medicine Siriraj Hospital,Mahidol University, 2 Prannok Street, Bangkok 10110, Thailande-mail: [email protected]
Curr Allergy Asthma Rep (2013) 13:308–314DOI 10.1007/s11882-013-0345-0

of VKC have been described, i.e., limbal, tarsal, and mixed.In limbal VKC, perhaps the most common type [2, 3], theclassic Horner-Tranta’s dots are observed around the limbus.In tarsal VKC, classic giant papilla can be seen mainly onupper tarsal conjunctiva, upon inversion of the upper eyelids. Pathologically, the conjunctiva is infiltrated by avariety of inflammatory cells such as mast cells, basophils,T and B lymphocytes, neutrophils, and classically by eosin-ophils [4].The giant papilla are large collections of collagenfibers laid down by conjunctival fibroblasts [5]. On-goingresearch indicates that ocular inflammation in VKC is theculmination of the roles of IgE (although not all VKCpatients, particularly those of limbal type, are atopic), Th2lymphocytes, eosinophilic degranulation, and histamine-induced chemotaxis of fibroblasts [6–8]. Release of growthfactors such as PDGF, VEGF, nerve growth factors with up-regulation of adhesion molecules and release of chemokinesfor eosinophil chemotaxis (such as eotaxin) have been doc-umented in conjunctiva of VKC patients [4, 9]. These eventslead to intense inflammation and remodeling of conjunctivaltissue, particularly with a confluent laying down of collagentypes I and III forming giant papilla on conjunctival surface.Such intense inflammation and repair cycles render VKC aremodeling ocular allergic eye disease akin to subepithelialfibrosis of the lungs seen in asthma. Corneal injury canoccur as a result of the release of eosinophil granular pro-teins along with neutrophil elastase which are destructive tocorneal epithelium [10]. Corneal complications include su-perficial punctate keratitis, abrasion, shield ulcers,keratoconus, pseudogerontoxon and ultimately cornealopacification [11]. Posterior subcapsular cataract and glau-coma are not uncommonly observed due to prolonged use oftopical steroids to control ocular inflammation and forsymptomatic relief [12]. Ultimately, in severe VKC, withoutproper intervention, loss of vision is a grave possibility.
Conventional Therapy for VKC
Conventional therapy for VKC include physical removal ofconjunctival debris and inflammatory components (cells,mediators, irritants, allergens) from the conjunctival surfaceby eye rinsing and compressing with cool, soothing salinesolution or with artificial tears. Various topical ophthalmicpreparations are used as first-line therapy for VKC. Theseinclude ophthalmic preparations of antihistamines (such aslevocabastine and epinastine), mast cell stabilizers (such assodium cromoglycate, ketotifen, and lodoxomide) and dual-acting agents such as olopatadine [2, 13–16]. In mild VKC,these treatments are usually sufficient and can bring thedisease under control [17]. However, in severe VKC, par-ticularly in the tarsal and mixed types, inflammation is oftensevere and frequently requires topical corticosteroids to
induce remission. VKC is generally a relapsing disease withfrequent recurrences and thus severe cases are prone todevelop complications such as corneal complications andsteroid-related complications. Over the last 2 decades, at-tempts have concentrated on identifying immune modula-tors to suppress chemical and cellular components of theinflammation/repair cycle and to be steroid-sparing. In thisreview, recent developments on the use of cyclosporine Aand tacrolimus in VKC are reviewed to give readers anupdate on the ongoing attempts to alter the course of severeVKC.
Cyclosporine A (CsA)
Interest in using immunomodulators in treating VKC beganlong before current pathogenesis for this condition becameapparent. Since corticosteroids are frequently used in thetreatment of exacerbations, patients as well as physiciansrelied on this potent type of medications to suppress eyeirritation and to reduce serious corneal ulcer development.Serious ophthalmic complications from corticosteroids,such as posterior subcapsular cataract, increased intraocularpressure,glaucoma, corneal changes, and superimposed in-fections (bacterial and fungal), are major problems fromprolonged topical steroid use [12].
CsA is a cyclic undecapeptide metabolite of the fungusTolypocladium inflatum. CsA inhibits calcineurin, a calcium-dependent intracellular signaling protein by binding to itsreceptor, cyclophilin. As a result, production of major cyto-kines and chemokines from effector cells including T helpercells are inhibited. IL-4 and IL-5 production from Th2 cellsare inhibited by cyclosporine [18, 19]. Topical CsA has beenindicated for treatment of inflammation of the ocular surfaceresulting from decreased tear production in dry eyes [20].Application of 2 % cyclosporine eye preparation as an alter-native treatment of severe VKC began in the early 1990s [21,22]. In these pilot reports, response to cyclosporine was rapid,i.e, within 15 days of therapy. However, relapse was observedsoon after the therapy was discontinued. A randomizedplacebo-controlled trial among Italian children with VKC byPucci et al., confirmed the efficacy for 2 % cyclosporine eyedrops prepared in olive oil [1]. Patients who received cyclo-sporine demonstrated improvement of ocular symptoms andsigns within 2 weeks of therapy. At the end of 4 months,patients derived approximately 70 % improvement in symp-tom scores. However, giant papilla were less responsive toCsA [1]. Cyclosporine in oil is irritating and could lead toblepharitis, thus a more aqueous solution was desirable.Further investigation from Turkey by Kilic et al., using 2 %cyclosporine dispersed in artificial tears, indicated that pa-tients derived similar rates of improvement at 2 weeks [23].Similarly, Spadavecchia et al., utilizing cyclosporine eye
Curr Allergy Asthma Rep (2013) 13:308–314 309

drops in a lower concentration of 1.25 and 1 % prepared inartificial tears, also showed a similar and even more impres-sive improvement in symptoms and signs, suggesting thatCsA in liquid form could be more efficacious than oil-basedpreparation [24].
Recently, a new aqueous solution of CsA, utilizingpolyoxyl 40 stearate (MYS-40) as a surfactant, has beenreleased in Japan for the treatment of recalcitrant aller-gic conjunctival disease, not responding to conventionaltreatment. A much lower concentration of CsA (0.1 %)was formulated into an aqueous base. Due to the aque-ous nature of the solution, tissue distribution of thedrug, as studied in rabbit eyes, was found to be 28.5and 3.1 times higher than from CsA in oil-base andemulsion-in-oil preparations, respectively [25]. Tissuedrug concentrations of CsA in bulbar conjunctival tissuewere 1,373, 464 ,and 876 ng-eg/gm after 1 min ofapplication of aqueous CsA versus emulsion-in-oil ver-sus oil-base CsA preparations, respectively [25].Subsequently, a 6-month post-marketing study of thispreparation in the treatment of a large population withVKC and AKC among Japanese patients by Ebihara etal. became available [26]. Notably, the age of AKCpatients in this study was quite young (17 years, similarto VKC of 16 years). This indicates overlapping pre-sentations between VKC and AKC. Moreover, severalatopic features (such as asthma, allergic rhinitis, andatopic dermatitis) can be observed among typical VKCpatients. Patients with VKC responded promptly to theuse of this new aqueous solution (within 1 month) andhad minimal symptoms by the end of the 6-monthobservation period. Improvement in corneal lesionswas from 21.6 to 8.6 %. A large number of VKCpatients were able discontinue topical steroids (over30 %) as well as CsA during the study.
Side effects of CsA eye preparations are limited to burn-ing and eye stinging, which is usually restricted to a shortperiod of time after initiation (less than 2 weeks), althoughclose to 10 % of study participants dropped out due toadverse events from this lower concentration of CsA (0.1 % aqueous solution).
Efficacy studies of responses to CsA were mostly ofshort duration (less than 6 months). Results from thesestudies indicate that, although response to CsA occurredpromptly, the magnitude of response was not large.Nonetheless, response to prolonged use of CsA coulddeliver further benefit, and it was suggested from thesestudies that CsA should be used on a longer and con-tinuing basis in order to exert the most benefit and tobe steroid-sparing. In a recent publication by Lambiaseet al., 0.05 % emulsion-in-oil preparation of CsA wascompared to ketotifen eye drops in preventing recur-rence of VKC relapse over a 2-year period [27]. CsA
was almost twice as effective as ketotifen in preventingrecurrences of VKC. However, the use of CsA for thetreatment of relapse was not as effective as dexametha-sone. The result of this study confirmed earlier short-term studies that treatment with CsA does not complete-ly eliminate the need of the use of topical steroids [28].Again, the major difference between these latter reportsfrom the Ebihara study [26] was the difference in vehi-cle use in preparing CsA eye drops.
Tacrolimus
Tacrolimus is a 23-membered macrolide lactone compounddiscovered in 1984 from a fermentation of broth soil with abacteria, Streptomyces tsukubaensis. It possesses immunosup-pressant effects via inhibition of T cell activation. Tacrolimusbinds to immunophilin FK-binding protein (FKBP-12), whichin turn inhibits calcineurin, an intracytoplasmic signaling pro-tein, downstream from calcium-dependent calmodulin activa-tion. Such inhibition leads to further inhibition of NF-ATactivation and further transcription of IL-2 [29]. Tacrolimuswas approved for use as an immunosuppressant for livertransplantation in 1994, and was further extended to otherorgan transplantation. Tacrolimus was found to inhibit therelease of histamine and production of inflammatory media-tors, such as LTC4 from human basophils, when stimulatedwith Der p I, anti-IgE, and calcium ionophore-A23187 [30].The ratio of inhibition from tacrolimus when compared to thatof CsAwas up to 50-fold.
Recently, tacrolimus has been introduced into a ther-apeutic regimen for atopic dermatitis (AD). AD is arelapsing skin disorder in children caused by immuno-regulatory defects characterized by overproduction ofcytokines of both Th1 and Th2 in various phases ofthe disease. Since prolonged use of topical steroids inAD can lead to systemic absorption, topical tacrolimuswas investigated as an alternative therapy AD for asteroid-sparing effect. Large numbers of adults and chil-dren with AD were subjected to a controlled trial with0.1 % tacrolimus ointment. In an adult trial by Ruzickaet al., improvement of skin condition was seen as earlyas day 3 of therapy, with 83 % of subjects showingsignificant improvement after 3 weeks of treatment withthis drug [31]. Despite a large area of application,systemic absorption of tacrolimus was minimal. A trialin pediatric AD by Boguniewicz et al. indicated asimilar efficacy and safety profile as in adult AD [32].Based on these earlier studies, topical tacrolimus be-comes a part of main therapy for acute as well formaintenance therapy for AD [33, 34]. With this reason,we became interested in applying tacrolimus to thetreatment of VKC.
310 Curr Allergy Asthma Rep (2013) 13:308–314

Since the pathogenesis of VKC, in a manner similar to AD,includes intensive activation of inflammatory cells, the use ofan immunomodulator such as tacrolimus appears to be anappropriate alternative for these patients, particularly for thosewho do not respond well to CsA. In fact, in a model of humanbasophils, tacrolimus was found to be almost 50 times aseffective as CsA in inhibiting histamine release [30]. Using arat model with OVA-sensitized, experimental allergic/immune-mediated blepharoconjunctivits, Nishino et al. were able toshow an inhibition of conjunctival infiltrations with lympho-cytes and eosinophils by topical tacrolimus applied prior to achallenge with OVA eye drops [35]. During a similar period,our group became interested in using tacrolimus for the treat-ment of VKC, since severe VKC patients did not respondsatisfactorily to topical CsA in oil in our hands [2]. Sincetacrolimus is lipophilic and does not dissolve well in aqueoussolution, we prepared tacrolimus into a 1 % ophthalmic oint-ment using a standard opthalmic ointment base. In our pilottrial, single and multiple doses of 1 % topical tacrolimusophthalmic ointment was well tolerated among patients withVKC. No immediate or delayed adverse effects were noted.Wetherefore proceeded to a 4-week open trial of topical tacrolimusamong 10 pediatric patients with severe recalcitrant VKC, whodid not respond well to conventional VKC treatment [36].Seven of nine patients failed CsA 0.5 % in oil treatment. Allpatients required topical steroids intermittently for control oftheir exacerbations. Frequency of use of tacrolimus was oncedaily in 6 patients and twice daily in 4 patients. Most patientsresponded to tacrolimus within 1 week of treatment with areduction of symptoms of about 30 %. By the end of 4 weekstreatment, symptoms reduced to 20 % of baseline [36]. In fact,most patients were without any symptoms by the end of the4-week trial. No significant adverse effect was noted.Absorption of tacrolimus at the end of the 4-week study wasminimal (mean plasma level=0.29 ng/ml). After our first re-port, tacrolimus has been reported to be effective in treatingvarious inflammatory disorders of the eyes such as anteriorsegment diseases [37, 38], severe atopic blepharoconjunctivitis[39], atopic keratoconjunctivitis [40], and giant papillary con-junctivitis [41]. Interestingly, Attas-Fox reported an off-labeluse of 0.03 % dermatological tacrolimus to treat severe intrac-table conjunctivitis [42]. Patients were successfully treatedwithout any adverse effect and without systemic absorptionof the drug. In a report by Khierkan et al., 10 adult patients withVKC were treated with tacrolimus suspended in balanced saltsolution in a very low concentration (0.005 %) but with morefrequent eye applications (4 times daily). VKC symptomsrapidly declined within 1 month [43]. A reduction in papillarysize was observed with a prolonged duration of 15 months oftreatment. Interestingly, despite the fact that tacrolimus does notdissolve well in aqueous salt solution, adequate relief in symp-toms of patients in this study was seen, perhaps due to (1) highfrequency of use per day and (2) the prolonged period of the
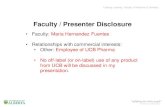
trial [43]. Despite the fact that tacrolimus was earlier reported tohave no effect on fibroblasts and did not cause skin thinning inprolonged use in AD, we have observed a significant reductionin conjunctival papillary size during our 3-year use oftacrolimus (Fig. 1; [44]). Such decrease in giant papillary sizewas observed in other trials with CsA [23] as well as insubsequent studies with tacrolimus [45, 46]. Interestingly, suchregression in giant papilla could be observed as early as 1 weekafter the initiation of tacrolimus in the latter two trials [45, 46].
With such a promising effect, we proceeded to compare1 % tacrolimus eye ointment with 2 % CsA eye drops in adouble-masked, controlled trial spanning a longer trial period(8 weeks). Twenty patients were enrolled in a double-blind,parallel trial. Again, most of the children in this study hadsevere VKC with mostly mixed-type (tarsal + limbal) indicat-ing a more recalcitrant degree of VKC. The sample size wascalculated based on 70% and 20 % efficacy of tacrolimus andCsA at 2 weeks of therapy, respectively [1, 36]. To oursurprise, both drugs were found to deliver almost the sameefficacy throughout this 8-week trial as shown in Fig. 2 [47].The fact that compliance in our second study was very goodand no patients dropped out may explain the similar efficacybetween the two drugs. In the additional 4 weeks after theblinding period, both groups of patients received tacrolimus asopen trial to determine further response to the drug. Totalocular symptom score (TOSS) further declined in both groups[47]. This illustrated that prolonged use of topical CsA as wellas tacrolimus will continue to show further efficacy, as wassuggested in a long-term study with CsA by Lambiase et al.[27]. However, adverse effects from CsA in our studies weremore apparent than from tacrolimus [47].
Perhaps the most recent interesting study with tacrolimuswas that by Ohashi et al., who employed a newly formulated
Fig. 1 External ocular photography of the left upper tarsal eye lid inone of our patients (J.S.) treated with tacrolimus at 0, 1, 12. and24 months. Note the marked improvement of conjunctival inflamma-tion at 1 month. There was a continuing improvement of conjunctivalhyperemia and a decrease in giant papilla size over the entire 24 monthsof therapy [44]
Curr Allergy Asthma Rep (2013) 13:308–314 311

aqueous suspension of tacrolimus (at a much lower concen-tration of 0.1 %) in treating 41 AKC and 14 VKC. With thisnovel preparation, dispersion of the drug was achieved by theuse of polyvinyl alcohol with benzalkonium chloride as pre-servative. Dosage of this 0.1 % tacrolimus emulsion dropswas only one drop in each eye twice daily. This aqueous-emulsion concept perhaps makes topical tacrolimus moreevenly distributed throughout the entire conjunctival tissueas with CsA aqueous-emulsion [25]. Clinical response to thisaqueous preparation was observed as promptly as 1 week forboth AKC and VKC. Notably, corneal defects as well giantpapilla improved within 1 week and continued throughout the4-week trial [46]. Apparently, interest in using tacrolimus inocular diseases is expanding, and we should look forward tomore encouraging results in the future [48].
Conclusions and Future Directions
Patients with VKC usually have significant disease uponpresentation, particularly among those with palpebral(tarsal) types. It is not uncommon to see patients with upperbilateral tarsal conjunctiva filled with large papilla greaterthan 5 mm in diameter. Such patients can be found not only
in ophthalmology clinics but also occasionally in generalpediatric clinics, as well as in allergy practices. Despite theknowledge that VKC commonly has an onset at 4–7 yearsof age, most patients were seen at age over 10 years [2, 3,49, 50]. This indicates that diagnosis of VKC is usuallymade late in the course of the disease. Partly, this is due tounder recognition of Tranta-Horner’s dot, failure to invertthe upper lid as a part of complete ophthalmologic exami-nation for patients with severe conjunctivitis and lack ofawareness of the diagnosis of VKC in children.
Unfortunately, cytologic examination of conjunctivalscrapings is rarely performed in ophthalmology or allergyclinics. With these shortcomings, several patients were notcorrectly diagnosed for a prolonged period prior to seeing anenthusiastic ‘allergy–ophthalmology’ specialist with a par-ticular interest in allergic eye disease. There is a need toimprove early diagnosis of VKC so that early interventioncan be implemented to prevent serious complications fromtopical steroids, damage to the cornea, or severe remodelingof conjunctiva that is not amenable to medical treatment.
The natural history of VKC, particularly in the earlyphase, is not fully understood. We do not understand whysome patients suffer from a milder limbal form of diseasewhile others go on to develop exuberant papilla on uppertarsal surface. Why are upper tarsal surfaces in VKC morevulnerable than lower tarsal plates? How soon can a smallfollicle develop into large papilla? Or it would ever progressat all? Does atopy play a major role in the progression of thedisease and, if so, would early intervention with CsA ortacrolimus change the natural course of the disease? Thesecrucial questions are essential parts of VKC managementbut have not been sufficiently addressed. Partly, this is dueto a lack of prospective studies to aid our understanding ofthe natural history of the disease. In fact, risk factors for thedevelopment of VKC have not been fully defined.Moreover, lack of animal models to study VKC adds todifficulty in understanding pathogenesis, progress, andproper intervention.
A collaborative research effort between allergy and oph-thalmology specialists in redefining better approach to di-agnosis and early management of VKC is needed.Unfortunately, such efforts are only available in limitedareas of the world (such as in Italy, Africa, and Japan).Moreover, research in this specific area (of ophthalmologyor allergy or combined) has not received much attention ineither specialty, as judged by limiting number of publica-tions in major journals, particularly in allergy. There is anurgent need for proper training for early detection andtreatment of VKC as well for basic and clinical researchand for drug development for VKC such as with CsA andtacrolimus. Improved diagnosis and therapy will eventuallylead to better visual acuity and better quality of life for theseunfortunate children.
Fig. 2 Mean ± SE total subjective symptom scores (TSSS) of VKCpatients randomized to receive CsA and FK-506 (12 patients each) atvarious time points. TSSS significantly decreased from baseline at the4th and 8th weeks in both groups (*p<0.05, **p<0.01). No differencewas observed between groups at any time point (p>0.05). Plots of datafrom the two groups, at each time point, are slightly overlapped. (Thisfigure was first published in the Asian Pacific Journal of Allergy andImmunology [47])
312 Curr Allergy Asthma Rep (2013) 13:308–314

Acknowledgments Funding for the authors’ research in topical CsAand FK-506 treatment for VKC came from the Research Funding of theFaculty of Medicine Siriraj Hospital, Mahidol University.
Conflict of Interest Pakit Vichyanond declares that he has no con-flict of interest.
Panida Kosrirukvongs declares that she has no conflict of interest.
References
Papers of particular interest have been highlighted as:• Of importance•• Of major importance
1. Pucci N, Novembre E, Cianferoni A, et al. Efficacy and safety ofcyclosporine eyedrops in vernal keratoconjunctivitis. Ann AllergyAsthma Immunol. 2002;89:298–303.
2. Kosrirukvongs P, Vichyanond P, Wongsawad W. Vernal keratocon-junctivitis in Thailand. Asian Pac J Allergy Immunol. 2003;21:25–30.
3. • Lambiase A, Minchiotti S, Leonardi A, et al. Prospective, mul-ticenter demographic and epidemiological study on vernal kerato-conjunctivitis: a glimpse of ocular surface in Italian population.Ophthalmic Epidemiol. 2009;16:38–41. A recent large study ex-amining epidemiology of VKC from Italy.
4. • Leonardi A. Vernal keratoconjunctivitis: pathogenesis and treat-ment. Prog Retin Eye Res. 2002;21:319–39. A must to read for allinterested in basic and clinical research of VKC.
5. Leonardi A, Abatangelo G, Cortivo R, Secchi AG. Collagen typesI and III in giant papillae of vernal keratoconjunctivitis. Br JOphthalmol. 1995;79:482–5.
6. Leonardi A, Curnow SJ, Zhan H, Calder VL. Multiple cyto-kines in human tear specimens in seasonal and chronic aller-gic eye disease and in conjunctival fibroblast cultures. ClinExp Allergy. 2006;36:777–84.
7. Leonardi A, Sathe S, Bortolotti M, et al. Cytokines, matrixmetalloproteases, angiogenic and growth factors in tears of normalsubjects and vernal keratoconjunctivitis patients. Allergy.2009;64:710–7.
8. Abu El-Asrar AM, Al-Mansouri S, Tabbara KF, et al.Immunopathogenesis of conjunctival remodelling in vernal kera-toconjunctivitis. Eye (Lond). 2006;20:71–9.
9. Leonardi A, Brun P, Tavolato M, et al. Growth factors and collagendistribution in vernal keratoconjunctivitis. Invest Ophthalmol VisSci. 2000;41:4175–81.
10. Trocme SD, Leiferman KM, George T, et al. Neutrophil andeosinophil participation in atopic and vernal keratoconjunctivitis.Curr Eye Res. 2003;26:319–25.
11. Iqbal A, Jan S, Babar TF, Khan MD. Corneal complications ofvernal catarrh. J Coll Physicians Surg Pak. 2003;13:394–7.
12. • Carnahan MC, Goldstein DA. Ocular complications of topical,peri-ocular, and systemic corticosteroids. Curr Opin Ophthalmol.2000;11:478–83. A complete comprehensive review of ocular com-plications of corticosteroids.
13. • Borazan M, Karalezli A, Akova YA, et al. Efficacy of olopatadineHCI 0.1 %, ketotifen fumarate 0.025 %, epinastine HCI 0.05 %,emedastine 0.05 % and fluorometholone acetate 0.1 % ophthalmicsolutions for seasonal allergic conjunctivitis: a placebo-controlledenvironmental trial. Acta Ophthalmol. 2009;87:549–54.Comparison of various topical treatments for ocular allergy.
14. Verin P, Allewaert R, Joyaux JC, et al. Comparison of lodoxamide 0.1%ophthalmic solution and levocabastine 0.05% ophthalmic suspension invernal keratoconjunctivitis. Eur J Ophthalmol. 2001;11:120–5.
15. Das D, Khan M, Gul A, Alam R. Safety and efficacy oflodoxamide in vernal keratoconjunctivitis. J Pak Med Assoc.2011;61:239–41.
16. Foster CS. Evaluation of topical cromolyn sodium in the treatmentof vernal keratoconjunctivitis. Ophthalmology. 1988;95:194–201.
17. • Mantelli F, Santos MS, Petitti T, et al. Systematic review andmeta-analysis of randomised clinical trials on topical treatments forvernal keratoconjunctivitis. Br J Ophthalmol. 2007;91:1656–61. Acomprehensive summary and meta-analysis of efficacy of varioustopical treatment regimen for VKC.
18. Farrell AM, Antrobus P, Simpson D, et al. A rapid flow cytometricassay to detect CD4+ and CD8+ T-helper (Th) 0, Th1 and Th2cells in whole blood and its application to study cytokine levels inatopic dermatitis before and after cyclosporin therapy. Br JDermatol. 2001;144:24–33.
19. Libetta C, Sepe V, Zucchi M, et al. The effect of sirolimus- orcyclosporine-based immunosuppression effects on T-cell subsets invivo. Kidney Int. 2007;72:114–20.
20. Tatlipinar S, Akpek EK. Topical ciclosporin in the treatment ofocular surface disorders. Br J Ophthalmol. 2005;89:1363–7.
21. BenEzra D, Pe’er J, Brodsky M, Cohen E. Cyclosporine eyedropsfor the treatment of severe vernal keratoconjunctivitis. Am JOphthalmol. 1986;101:278–82.
22. Secchi AG, Tognon MS, Leonardi A. Topical use of cyclosporinein the treatment of vernal keratoconjunctivitis. Am J Ophthalmol.1990;110:641–5.
23. Kilic A, Gurler B. Topical 2 % cyclosporine A in preservative-freeartificial tears for the treatment of vernal keratoconjunctivitis. CanJ Ophthalmol. 2006;41:693–8.
24. Spadavecchia L, Fanelli P, Tesse R, et al. Efficacy of 1.25 % and 1 %topical cyclosporine in the treatment of severe vernal keratoconjunc-tivitis in childhood. Pediatr Allergy Immunol. 2006;17:527–32.
25. Kuwano M, Ibuki H, Morikawa N, et al. Cyclosporine A formu-lation affects its ocular distribution in rabbits. Pharm Res.2002;19:108–11.
26. •• Ebihara N, Ohashi Y, Uchio E, et al. A large prospectiveobservational study of novel cyclosporine 0.1 % aqueous ophthal-mic solution in the treatment of severe allergic conjunctivitis. JOcul Pharmacol Ther. 2009;25:365–72. Report of an efficacy of anew aqueous base CsA solution in various forms of severe con-junctivitis including VKC.
27. •• Lambiase A, Leonardi A, Sacchetti M, et al. Topical cyclospor-ine prevents seasonal recurrences of vernal keratoconjunctivitis ina randomized, double-masked, controlled 2-year study. J AllergyClin Immunol. 2011;128:896–7 e9. Newer concept of treatment ofVKC using long-term treatment with topical CsA.
28. Daniell M, Constantinou M, Vu HT, Taylor HR. Randomisedcontrolled trial of topical ciclosporin A in steroid dependent aller-gic conjunctivitis. Br J Ophthalmol. 2006;90:461–4.
29. Shaw KT, Ho AM, Raghavan A, et al. Immunosuppressive drugsprevent a rapid dephosphorylation of transcription factor NFAT1 instimulated immune cells. Proc Natl Acad Sci U SA. 1995;92:11205–9.
30. de Paulis A, Cirillo R, Ciccarelli A, et al. FK-506, a potent novelinhibitor of the release of proinflammatory mediators from humanFc epsilon RI+cells. J Immunol. 1991;146:2374–81.
31. Ruzicka T, Bieber T, Schopf E, et al. A short-term trial oftacrolimus ointment for atopic dermatitis. European TacrolimusMulticenter Atopic Dermatitis Study Group. N Engl J Med.1997;337:816–21.
32. Boguniewicz M, Fiedler VC, Raimer S, et al. A randomized,vehicle-controlled trial of tacrolimus ointment for treatment ofatopic dermatitis in children. Pediatric Tacrolimus Study Group.J Allergy Clin Immunol. 1998;102:637–44.
33. Ring J, Alomar A, Bieber T, et al. Guidelines for treatment ofatopic eczema (atopic dermatitis) part I. J Eur Acad DermatolVenereol. 2012;26:1045–60.
Curr Allergy Asthma Rep (2013) 13:308–314 313

34. Schneider L, Tilles S, Lio P, et al. Atopic dermatitis: a practiceparameter update 2012. J Allergy Clin Immunol. 2013;131:295–9.e27.
35. Nishino K, Fukushima A, Okamoto S, et al. Suppression of exper-imental immune-mediated blepharoconjunctivitis in BrownNorway rats by topical application of FK506. Graefes Arch ClinExp Ophthalmol. 2002;240:137–43.
36. Vichyanond P, Tantimongkolsuk C, Dumrongkigchaiporn P, et al.Vernal keratoconjunctivitis: Result of a novel therapy with 0.1 %topical ophthalmic FK-506 ointment. J Allergy Clin Immunol.2004;113:355–8.
37. Cheng AC, Yuen K, Chan W. Topical tacrolimus ointment fortreatment of refractory anterior segment inflammatory disorders.Cornea. 2006;25:634. author reply.
38. Joseph MA, Kaufman HE, Insler M. Topical tacrolimus ointmentfor treatment of refractory anterior segment inflammatory disor-ders. Cornea. 2005;24:417–20.
39. Virtanen HM, Reitamo S, Kari M, Kari O. Effect of 0.03 %tacrolimus ointment on conjunctival cytology in patients withsevere atopic blepharoconjunctivitis: a retrospective study. ActaOphthalmol Scand. 2006;84:693–5.
40. Garcia DP, Alperte JI, Cristobal JA, et al. Topical tacrolimusointment for treatment of intractable atopic keratoconjunctivi-tis: a case report and review of the literature. Cornea.2011;30:462–5.
41. Kymionis GD, Goldman D, Ide T, Yoo SH. Tacrolimus ointment0.03 % in the eye for treatment of giant papillary conjunctivitis.Cornea. 2008;27:228–9.
42. Attas-Fox L, Barkana Y, Iskhakov V, et al. Topical tacrolimus0.03 % ointment for intractable allergic conjunctivitis: an open-label pilot study. Curr Eye Res. 2008;33:545–9.
43. Kheirkhah A, Zavareh MK, Farzbod F, et al. Topical 0.005%tacrolimus eye drop for refractory vernal keratoconjunctivitis.Eye (Lond). 2011;25:872–80.
44. Pacharn P, Visitsunthorn N, Jirapongsananuruk O, Vichyanond P.Vernal Keratoconjunctivitis (vkc) Treated With 0.1 % Fk-506Ophthalmic Ointment: Result Of A Three Years Follow-up. JAllergy Clin Immunol. 2007;119:S153.
45. • Tam PM, Young AL, Cheng LL, Lam PT. Topical tacrolimus0.03 % monotherapy for vernal keratoconjunctivitis–case series.Br J Ophthalmol. 2010;94:1405–6. An off-label use of dermato-logic preparation of FK-506 in VKC treatment.
46. •• Ohashi Y, Ebihara N, Fujishima H, et al. A randomized, placebo-controlled clinical trial of tacrolimus ophthalmic suspension 0.1 % insevere allergic conjunctivitis. J Ocul Pharmacol Ther. 2010;26:165–74.Efficacy of a new FK-506 suspension in AKC and VKC from Japan.
47. •• Labcharoenwongs P, Jirapongsananuruk O, Visitsunthorn N, et al.A double-masked comparison of 0.1 % tacrolimus ointment and 2 %cyclosporine eye drops in the treatment of vernal keratoconjunctivitisin children. Asian Pac J Allergy Immunol. 2012;30:177–84. The firstcomparative trial between topical CsA and FK-506 in VKC.
48. • Zhai J, Gu J, Yuan J, Chen J. Tacrolimus in the treatment ofocular diseases. BioDrugs. 2011;25:89–103. Review of FK-506 astopical treatment for various ocular diseases.
49. Leonardi A, Busca F, Motterle L, et al. Case series of 406 vernalkeratoconjunctivitis patients: a demographic and epidemiologicalstudy. Acta Ophthalmol Scand. 2006;84:406–10.
50. De Smedt S, Nkurikiye J, Fonteyne Y, et al. Topical ciclosporin inthe treatment of vernal keratoconjunctivitis in Rwanda, CentralAfrica: a prospective, randomised, double-masked, controlled clin-ical trial. Br J Ophthalmol. 2012;96:323–8.
314 Curr Allergy Asthma Rep (2013) 13:308–314