Use of aesthetic rhinoplasty procedures in reconstructive ... · the nasal framework. The...
5
British Journal of Oral and Maxillofacial Surgery 53 (2015) 44–48 Available online at www.sciencedirect.com Use of aesthetic rhinoplasty procedures in reconstructive nasal surgery Alireza Ghassemi a,∗ , Albert Rübben b , Behnam Bohluli c , Frank Hölzle a , Mehrangiz Ghassemi d a Department of Oral, Maxillofacial of Surgery, University Hospital of RWTH Aachen, Pauwelsstr. 30, 52074 Aachen, Germany b Department of Dermatology, University Hospital of RWTH Aachen, Pauwelsstr. 30, 52074 Aachen, Germany c Craniomaxillofacial Research Center, Azad University of Tehran, Tehran, Iran d Department of Orthodontics, University Hospital of RWTH Aachen, Pauwelsstr. 30, 52074 Aachen, Germany Accepted 15 September 2014 Available online 5 November 2014 Abstract Resection of cancer often involves the excision of underlying hard tissue, and some procedures in aesthetic rhinoplasty can be used in reconstructive nasal surgery to increase the margin of safety while still achieving an acceptable aesthetic and functional outcome. We have used techniques from aesthetic rhinoplasty to shape the nasal framework. Osteotomy and formation of the tip were used in 17 patients with defects (ranging from 1 to 3.5 cm in size) from the nasal root to the tip of the nose. After the underlying bony or cartilaginous framework, or both, had been removed, the resulting open roof deformity had to be corrected by osteotomy of the bony nasal wall and the tip shaped by excision and suturing, including insertion of the tip graft and columellar strut graft. After this, and narrowing of the nose, the defect was smaller and could be closed with local tissue without tension. There were no deformities in the contour, and patency of the airway was maintained. Patients were satisfied with both the aesthetic and functional results. Although the margin of safety was increased, shaping the nasal framework reduced the size of the defect, which allowed tension-free closure with a local flap. The operation requires a thorough knowledge of procedures used in aesthetic rhinoplasty. © 2014 The British Association of Oral and Maxillofacial Surgeons. Published by Elsevier Ltd. All rights reserved. Keywords: Tumour excision; Hump removal; Osteotomy; Tip-forming; Local flap Introduction Nasal reconstruction has always been a challenge for recons- tructive surgeons, and the use of a local flap provides the best options for colour, texture, and thickness. A successful reconstruction of the bony and cartilaginous scaffold should achieve a harmonious appearance. ∗ Corresponding author. Klinik für Zahn-, Mund-, Kiefer- und Plastis- che Gesichtschirurgie, Universitätsklinikum RWTH-Aachen, Pauwelsstr. 30, 52074 Aachen, Germany. Tel.: +49 241 8088247; fax: +49 2418082430. E-mail address: [email protected] (A. Ghassemi). A simple improvement in the nasal contour can have an appreciable impact on the overall appearance of the nose and on the patient’s self-confidence. Refinements have been suggested to minimise any noticeable deformity, 1,2 but the complexity of nasal contours is a challenge that demands the refinement of existing procedures. 3,4 During past decades there have been considerable advances in reconstructive surgery. Existing methods have been refined and new methods have been developed, including the use of microsurgical tissue transfer. 5–8 The introduction of aesthetic nasal “subunits”, although contro- versial, has contributed greatly to these refinements. 9–12 http://dx.doi.org/10.1016/j.bjoms.2014.09.011 0266-4356/© 2014 The British Association of Oral and Maxillofacial Surgeons. Published by Elsevier Ltd. All rights reserved.
Transcript of Use of aesthetic rhinoplasty procedures in reconstructive ... · the nasal framework. The...

UnAFa
b
c
d
AA
A
Rrudobwwtk©
K
I
Ntbra
c3
h0
British Journal of Oral and Maxillofacial Surgery 53 (2015) 44–48
Available online at www.sciencedirect.com
se of aesthetic rhinoplasty procedures in reconstructiveasal surgerylireza Ghassemi a,∗, Albert Rübben b, Behnam Bohluli c,rank Hölzle a, Mehrangiz Ghassemi d
Department of Oral, Maxillofacial of Surgery, University Hospital of RWTH Aachen, Pauwelsstr. 30, 52074 Aachen, GermanyDepartment of Dermatology, University Hospital of RWTH Aachen, Pauwelsstr. 30, 52074 Aachen, GermanyCraniomaxillofacial Research Center, Azad University of Tehran, Tehran, IranDepartment of Orthodontics, University Hospital of RWTH Aachen, Pauwelsstr. 30, 52074 Aachen, Germany
ccepted 15 September 2014vailable online 5 November 2014
bstract
esection of cancer often involves the excision of underlying hard tissue, and some procedures in aesthetic rhinoplasty can be used ineconstructive nasal surgery to increase the margin of safety while still achieving an acceptable aesthetic and functional outcome. We havesed techniques from aesthetic rhinoplasty to shape the nasal framework. Osteotomy and formation of the tip were used in 17 patients withefects (ranging from 1 to 3.5 cm in size) from the nasal root to the tip of the nose. After the underlying bony or cartilaginous framework,r both, had been removed, the resulting open roof deformity had to be corrected by osteotomy of the bony nasal wall and the tip shapedy excision and suturing, including insertion of the tip graft and columellar strut graft. After this, and narrowing of the nose, the defectas smaller and could be closed with local tissue without tension. There were no deformities in the contour, and patency of the airwayas maintained. Patients were satisfied with both the aesthetic and functional results. Although the margin of safety was increased, shaping
he nasal framework reduced the size of the defect, which allowed tension-free closure with a local flap. The operation requires a thoroughnowledge of procedures used in aesthetic rhinoplasty.
2014 The British Association of Oral and Maxillofacial Surgeons. Published by Elsevier Ltd. All rights reserved.
eywords: Tumour excision; Hump removal; Osteotomy; Tip-forming; Local flap
aas
ntroduction
asal reconstruction has always been a challenge for recons-ructive surgeons, and the use of a local flap provides the
est options for colour, texture, and thickness. A successfuleconstruction of the bony and cartilaginous scaffold shouldchieve a harmonious appearance.∗ Corresponding author. Klinik für Zahn-, Mund-, Kiefer- und Plastis-he Gesichtschirurgie, Universitätsklinikum RWTH-Aachen, Pauwelsstr.0, 52074 Aachen, Germany. Tel.: +49 241 8088247; fax: +49 2418082430.
E-mail address: [email protected] (A. Ghassemi).
cr
abiiv
ttp://dx.doi.org/10.1016/j.bjoms.2014.09.011266-4356/© 2014 The British Association of Oral and Maxillofacial Surgeons. Pu
A simple improvement in the nasal contour can have anppreciable impact on the overall appearance of the nosend on the patient’s self-confidence. Refinements have beenuggested to minimise any noticeable deformity,1,2 but theomplexity of nasal contours is a challenge that demands theefinement of existing procedures.3,4
During past decades there have been considerabledvances in reconstructive surgery. Existing methods haveeen refined and new methods have been developed,
ncluding the use of microsurgical tissue transfer.5–8 Thentroduction of aesthetic nasal “subunits”, although contro-ersial, has contributed greatly to these refinements.9–12blished by Elsevier Ltd. All rights reserved.

A. Ghassemi et al. / British Journal of Oral and Maxillofacial Surgery 53 (2015) 44–48 45
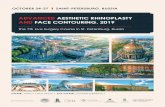
Fig. 1. Left lateral view of a 58-year-old woman after excision of a basal cellc
tattrntflTd
motn
P
Wardtrfbfl(trnoi
Fig. 2. Photograph of the same patient after excision of the tumour with anao
R
AnflwdcTprpam
sctle pressure with the fingers. The stability of the nasal wallwas maintained and tearing of the nasal mucosa avoided.
arcinoma from the tip of her nose (published with the patient’s permission).
Many variables, including the size and site of the defect,he shape of the nose, and the laxity of the covering skin,re important determinants of the choice of reconstructiveechnique. Osteotomy of the nose is an essential step in aes-hetic rhinoplasty to correct an open deformity of the nasaloof and an irregular nasal wall, or to narrow the width of theasal base.13 Many procedures have been developed to shapehe tip of the nose.14,15 Excision of the tumour and raising aap permit wide exposure of the nasal bones and cartilage.his allows exact manipulation of the nasal framework underirect vision.
Here we present our clinical experience in the adjust-ent of the nasal framework after excision of a tumour using
steotomy and tip-forming techniques. The method was usedo increase the margin of safety and reduce the size of theasal defect to allow primary closure of the residual defect.
atients and methods
e studied 17 patients with malignancies of the nose (7 mennd 10 women, mean age 65 (range 37–83) years). Afteresection of the tumours with clear margins, the size of theefects, which were on the nasal dorsum from the base tohe nasal tip, ranged between 1 and 3.5 cm. This includedesection of the underlying bony or cartilaginous (or both)ramework of the nose. For 5 patients we used unilateral orilateral advancement flaps from the cheek. Four had bilobedaps. We chose tissue from the nasal dorsum for 8 patientsFigs. 1 and 2). Tension-free closure was achieved satisfac-orily in all. We used a nasal osteotomy to correct the open
oof deformity, a large carbide burr was used to flatten theasal base, and a small diamond burr was used for the lateralsteotomy. The procedure was done under local anesthesian 9 patients, and under general anaesthesia in 8.Fm
dequate margin of safety. The design of the flap is marked on the dorsumf the nose (published with the patient’s permission).
esults
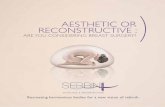
good aesthetic outcome was achieved in all 17 patients witho major complications. In the cases where an advancementap from the cheek was considered, secondary debulkingas required to improve the nasolabial region. An open roofeformity, resulting from removal of the hump (Fig. 3), wasorrected by lateral osteotomy of the bony nasal wall (Fig. 3).he osteotomy was easily done with a diamond burr after thelanned local flap had been dissected. This allowed accu-ate and precise control of the path of the osteotomy and theositioning of the bony lateral wall under direct vision. Thispproach allows various types of nasal osteotomy – lateral,edial, or transverse – as necessary.The osteotomy line was smooth and allowed a predictable
plit exactly as planned, and there were no unfavourable oromminuted fractures. The infracturing was achieved by gen-
ig. 3. After flap dissection, excision of the hump, and lateral osteotomyade with a diamond burr.

46 A. Ghassemi et al. / British Journal of Oral and Maxillofacial Surgery 53 (2015) 44–48
F patientt
racrrAt
D
Ns
ahaisooAtathe aesthetic outcome. Use of the nasal mucosa has also
ig. 4. Photographs taken after 8 months: (a) patient’s left lateral view, (b)he patient’s permission).
Lateral osteotomy, followed by digital infracturing, nar-owed the width and reduced the size of the defect. Inddition, the reduction of the cranial part of the lower lateralartilage and the tip-suturing techniques that we used alsoeduced the size. These procedures allowed the tension-freeeconstruction of the defect by local procedures (Fig. 4a–c).ll patients were satisfied with the result, whereas preopera-
ively they had been anxious about a possible deformity.
iscussion
asal reconstruction comprises controlled changes in thekeletal support structures and the soft tissue envelope to
oNr
’s right lateral view, and (c) the patient’s view from below (published with
chieve the desired results. Improvement in the nasal contouras an appreciable favourable impact on the patients’ overallppearance and self-confidence. There has been an increas-ng demand for optimal aesthetic and functional outcomes,o various techniques have been suggested for replacementf the soft tissue lost after resection of the cancer, dependingn the size and site of the defect and the tissue involved.2–8
dvances have been made during the past decade to achievehe best possible results in reconstructive rhinoplasty. Burgetnd Menick introduced the “subunits” philosophy to improve
10
ptimised the result of reconstruction in perforated defects.16
evertheless, there is a need for further improvement in theesults, and simplification of the procedure.

ral and
etaow
atcttsatntt
wrptmfp
fsaobulssro
fldiai
tub–mowfsdh
srttmuwc
fut
C
W
E
Tt
fi
R
1
1
1
A. Ghassemi et al. / British Journal of O
A small residual deformity of the nose can be seen, butven a small improvement can have a favourable impact onhe patient’s quality of life.1,2 If the principles of aestheticnd functional nasal surgery are followed, it can result in anutstanding repair, so the use of the appropriate techniqueill help to achieve the desired result.3,4
Skeletal support of the nose provides the main aestheticnd functional requirements of nasal reconstruction. It ishe framework that provides the support and shape of theovering soft tissue,5 and the restoration of the nasal con-our is integrally related to the composition and design ofhe nasal framework. The principles of reconstruction of thekeletal support are similar to those of aesthetic rhinoplasty,nd we have shown the importance of different techniqueshat are commonly used in aesthetic rhinoplasty to shape theasal framework. In addition, these techniques can be usedo reduce the size of the defect, allow easier replacement ofissue, and help to increase the margin of safety.
An alteration in the width of the nose by lateral osteotomy,hich is a usual part of aesthetic rhinoplasty, can be used in
econstructive nasal surgery.13 It is an integral part of rhino-lasty, and can be used to reshape the lateral contour, narrowhe base, realign the dorsum, and correct an open roof defor-
ity. Various methods and instruments have been introducedor this purpose.17–22 The osteotomy should be controllable,redictable, and easy to do.23
Depending on the site of the tumour, bone or cartilagerom the dorsum or cartilage from the nasal tip has to beacrificed to increase the margin of safety. This may lead ton open roof deformity, which can be corrected by osteotomyf the nasal wall. Once the soft tissue cover of the nose haseen dissected to close the defect, the osteotomy can be madender direct vision, which is controllable and precise with aimited potential for complications such as damage to theurrounding soft tissue. It can be done with an appropriateurgical burr.22,24 Tip-forming techniques used in aesthetichinoplasty can also help to shape the nasal tip, reduce the sizef the defect, and achieve an adequate margin of safety.14,15
After the lateral nasal wall is in position, various localaps can be used to close the defect without leaving a visibleeformity. We have been using these procedures, includ-ng osteotomy and tip-forming techniques, as an importantdjunct to other techniques in reconstructive nasal surgery tomprove the result.
Because the osteotomies were made under direct vision,hey could be made exactly along the planned path. These of a diamond burr allows the required osteotomy toe made exactly and easily – lateral, median, or transversewithout damaging the nasal mucosa or causing a com-inuted fracture pattern. We encountered no irregularities
f the dorsum, the nasal wall did not collapse, and thereere no unwanted fractures, which can cause comminuted
ractures and spicules. The establishment of the normal sub-urface architecture of the nose is essential to improve theefinition of nasal landmarks, even if the missing anatomyas been precisely duplicated. An adequate local flap with
1
Maxillofacial Surgery 53 (2015) 44–48 47
ufficient mobilisation and narrowing of the hard-tissueeduces the tension and improves the accuracy of the inser-ion of the flap. A soft tissue envelope similar in appearanceo the surrounding skin creates the visual impression of nor-
ality. The patient’s preoperative fear of having a deformedgly nose could be changed to postoperative satisfaction, soe were able to help to relieve the problems of excision of a
ancer. Even the relatives were astonished.We conclude that the techniques of aesthetic rhinoplasty,
rom osteotomy of the nasal wall to formation of the tip, areseful refinements that can optimise the outcome of recons-ructive nasal surgery.
onflict of interest
e have no conflict of interest.
thics statement/confirmation of patient’s permission
he patient has given us permission to publish the pho-ographs.
We have no financial interest and we did not have anynancial or material support concerning this study.
eferences
1. Essers BA, Nieman FH, Prins MH, et al. Determinants of satisfactionwith the health state of facial skin in patients undergoing surgery forfacial basal cell carcinoma. Patient Educ Couns 2006;60:179–86.
2. Kline RM. Aesthetic reconstruction of the nose following skin cancer.Clin Plast Surg 2004;31:93–111.
3. Barton Jr FE. Aesthetic aspects of nasal reconstruction. Clin Plast Surg1988;15:155–66.
4. Meyer R. Aesthetic aspects in reconstructive surgery of the nose. Aes-thetic Plast Surg 1988;12:195–201.
5. Menick FJ. A 10-year experience in nasal reconstruction with the three-stage forehead flap. Plast Reconstr Surg 2002;109:1839–61.
6. Moore EJ, Storme SA, Kasperbauer JL, et al. Vascularized radial fore-arm free tissue transfer for lining in nasal reconstruction. Laryngoscope2003;113:2078–85.
7. Walton RL, Burget GC, Beahm EK. Microsurgical reconstruction of thenasal lining. Plast Reconstr Surg 2005;115:1813–29.
8. Beahm EK, Walton RL, Burget GC. Free first dorsal metacarpal arteryflap for nasal lining. Microsurgery 2005;25:551–5.
9. Gonzales-Ulloa M. Selective regional plastic restoration by means ofesthetic unities (in Spanish). Rev Bras Cir 1957;33:527–33.
0. Burget GC, Menick FJ. The subunit principle in nasal reconstruction.Plast Reconstr Surg 1985;76:239–47.
1. Singh DJ, Bartlett SP. Aesthetic considerations in nasal reconstruc-tion and the role of modified nasal subunits. Plast Reconstr Surg2003;111:639–51.
2. Rohrich RJ, Griffin JR, Ansari M, et al. Nasal reconstruction-beyondaesthetic subunits: a 15-year review of 1334 cases. Plast Reconstr Surg
2004;114:1405–19.3. Kienstra MA, Sherris DA, Kern EB. Osteotomy and pyramid modifica-tion in the Joseph and Cottle rhinoplasty. Facial Plast Surg Clin N Am1999;7:279–94.

4 ral and
1
1
1
1
1
1
2
2
2
2
24. Ghasssemi A, Ayoub A, Modabber A, et al. Lateral nasal osteotomy:
8 A. Ghassemi et al. / British Journal of O
4. Toriumi DM. New concept in nasal tip contouring. Arch Facial Plast Surg2006;8:156–85.
5. Gruber RP, Weintraub J, Pomerantz J. Suture techniques for the nasal tip.Aesthet Surg J 2008;28:92–100.
6. Burget GC, Menick FJ. Nasal support and lining: the marriage of beautyand blood supply. Plast Reconstr Surg 1989;84:189–202.
7. Gryskiewicz JM, Gryskiewicz KM. Nasal osteotomies: a clinical com-parison of the perforating methods versus the continuous technique. PlastReconstr Surg 2004;113:1445–56.
8. Rohrich RJ, Janis JE, Adams WP, et al. An update on the lateralnasal osteotomy in rhinoplasty: an anatomic endoscopic comparisonof the external versus the internal approach. Plast Reconstr Surg
2003;111:2461–2.9. Kuran I, Ozcan H, Usta A, et al. Comparison of four different types ofosteotomies for lateral osteotomy: a cadaver study. Aesthetic Plast Surg1996;20:323–6.
Maxillofacial Surgery 53 (2015) 44–48
0. Mottura AA. Internal lateral nasal osteotomy: double-guarded osteotomeand mucosa tearing. Aesthetic Plast Surg 2011;35:171–6.
1. Ghassemi A, Prescher A, Talebzadeh M, et al. Osteotomy of the nasal wallusing a newly designed piezo scalpel – a cadaver study. J Oral MaxillofacSurg 2013;71:2155, e1–6.
2. Ghassemi A, Riediger D, Hölzle F, et al. The intraoral approach tolateral osteotomy: the role of a diamond burr. Aesthetic Plast Surg2013;37:135–8.
3. Rohrich RJ, Krueger JK, Adams Jr WP, et al. Achieving consistencyin the lateral nasal osteotomy during rhinoplasty: an external perforatedtechnique. Plast Reconstr Surg 2001;108:2122–32.
a comparative study between the use of osteotome and a dia-mond surgical burr – a cadaver study. Head Face Med 2013;9:41.