Apparent homozygous deletion identified in Alström syndrome patient
Upload
john-morganCategory
view
213download
0
(2008) 393–395
Clinical Imaging 32US, CT, and MR imaging of hepatic masses in Alström syndrome:a case report
John Morgana,⁎, Michael A. Sadlera, Stacey Siegelb
aDepartment of Radiology, St. Vincent's Hospital and Medical Center, New York, NY 10011, USAbDepartment of Radiology, VA Medical Center East Orange, East Orange, NJ 07018, USA
Received 15 January 2008; accepted 22 February 2008
Abstract
Alström syndrome is among the rarest genetic disorders described in the medical literature. It is characterized by retinal pigmentdegeneration, obesity, sensorineural deafness, non-insulin-dependent diabetes mellitus, progressive chronic nephropathy, cardiomyopathy,and hepatic dysfunction. Hepatic inflammation and fibrosis, which leads to cirrhosis, portal hypertension, and liver failure, is the finalpathway of the hepatopathy in Alström syndrome. We report a case of Alström syndrome with particular emphasis on hepatic findings.© 2008 Elsevier Inc. All rights reserved.
Keywords: Alstrom; Syndrome; Genetic; Rare; Hepatic
Alström syndrome is among the rarest genetic disordersdescribed in the medical literature. It is characterized byretinal pigment degeneration, obesity, sensorineural deaf-ness, non-insulin- dependent diabetes mellitus, progressivechronic nephropathy, cardiomyopathy, and hepatic dysfunc-tion. Hepatic inflammation and fibrosis, which leads tocirrhosis, portal hypertension, and liver failure, is the finalpathway of the hepatopathy in Alström syndrome. Uppergastrointestinal (GI) hemorrhage, secondary to portalhypertension, has been the initial symptom leading todeath in reported patients. To assist in the management ofthis disease, an increased awareness of Alström syndrome isessential to recognize the many manifestations of thiscomplex entity. We report a case of Alström syndromewith particular emphasis on hepatic findings.
With less than 100 cases reported in the medical literaturesince its first description in 1959, Alström syndrome isamong the rarest genetic disorders in the world [1]. Firstdescribed by Carl-Henry Alström in Sweden, Alström syn-
⁎ Corresponding author.E-mail address: [email protected] (J. Morgan).
0899-7071/08/$ – see front matter © 2008 Elsevier Inc. All rights reserved.doi:10.1016/j.clinimag.2008.02.031
drome is a progressive autosomal recessive genetic diseasethat presents with an array of manifestations [2]. Typicallypresenting in childhood or early adulthood, affected patientscharacteristically have retinal pigment degeneration, obesity,sensorineural deafness, non-insulin-dependent diabetes mel-litus, progressive chronic nephropathy, cardiomyopathy, andhepatic dysfunction [3]. Additional features include acantho-sis nigricans, hyperlipidemia, splenomegaly, and scoliosis.Extensive genetic research has recently localized Alströmsyndrome on chromosome 2p 12–13 [4]. Although it hasbeen described in various genetics, medical, and pediatricspecialty journals, Alström syndrome has not been describedin the radiologic literature and is likely unfamiliar to mostradiologists. We report a case of Alström syndrome withparticular emphasis on hepatic findings.
A 29-year-old woman with Alström syndrome diagnosed5 years prior presented to our institution with right upper andmid abdominal pain. Her past medical history was significantfor many of the classic features associated with her disease:blindness, deafness, diabetes, chronic nephropathy, hyperli-pidemia, cardiac valvular disease, and acanthosis nigricans.She also reported a history of chronic pancreatitis withprevious surgeries including a splenectomy and partial

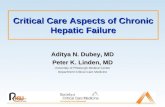
Fig. 1. (A) Enlarged echogenic liver with a brightly enhancingmass in the lefthepatic lobe. (B) Heterogeneously enhancing mass in the right hepatic lobe.
Fig. 2. Ultrasound examination demonstrated an enlarged, echogenic liverwith two isoechoic masses (Fig. 1A) as well as cholelithiasis with a positiveMurphy's sign.
394 J. Morgan et al. / Clinical Imaging 32 (2008) 393–395
pancreatectomy. Her laboratory findings on this admissionrevealed hyperglycemia (glucose = 215) and an elevatedgamma-glutamyl transpeptidase (GGT) of 98, as well asproteinuria and glycosuria. Computed tomographic (CT)scan demonstrated a brightly enhancing mass in the lefthepatic lobe (Fig. 1A). CT also showed a heterogeneouslyenhancing hepatic mass in the right hepatic lobe whichdemonstrated enhancement in the portal phase of imagingwith central lucency possibly representing fibrous scar (Fig.1B). Ultrasound examination demonstrated an enlarged,echogenic liver with two isoechoic masses (Fig. 2) as well ascholelithiasis with a positive Murphy's sign. Magneticresonance imaging examination revealed multiple hepaticmasses demonstrating intermediate T1 signal centrally withhigh signal peripherally and high T2 signal centrally withlow signal peripherally. After contrast administration, vividenhancement was seen during the arterial/early portal venousphase (Fig. 3) with only minimal to mild diminution in theenhancement pattern seen on later imaging. The patientunderwent an open cholecystectomy and biopsy of onehepatic mass, which was pathologically proven to represent ahepatocellular adenoma with pericellular fibrosis.
Alström syndrome presents in the liver as a fibrosing andinflammatory process. Lymphocytes infiltrate portal andparenchymal areas with or without piecemeal necrosis andwith or without limiting plate destruction. Hepatic inflam-mation and fibrosis, which leads to cirrhosis, portalhypertension and liver failure, is the final pathway of thehepatopathy in Alström syndrome. Our patient did notexhibit abnormalities in serum copper, ceruloplasmin,ferritin, alpha-1-antitrypsin phenotype, urine organic acids,plasma amino acids, or plasma carnitine. Testing forinfectious etiologies including EBV, CMV, hepatitis B,and hepatitis C were unremarkable. The inflammatorychanges which result in fibrosis in patients with Alströmsyndrome does not appear to be autoimmune because thetypical markers for autoimmune hepatitis are negative(normal ESR, negative antinuclear antibodies, antiliverand kidney microsomal antibodies, and anti-double-strandedDNA antibodies).
Since upper GI hemorrhage has been the initial symptomleading to death in reported patients with liver disease andportal hypertension that have died, aggressive treatment isnecessary in patients with portal hypertension and varices.Early referral for liver transplant should be done in patientswith portal hypertension. Since the hepatopathy of Alströmsyndrome is clinically silent early in the disease process,yearly testing after 5 years of age with ALT, GGT, alkalinephosphatase, and bilirubin should be done to detect thosepatients who are developing liver disease. When biochemicalabnormalities begin, careful follow-up for evidence of portalhypertension including ultrasound with Doppler, for evalua-tion of varices, splenomegaly, cirrhosis, and abnormal portal

Fig. 3. Multiple hepatic masses demonstrating intermediate T1 signalcentrally with high signal peripherally and high T2 signal centrally with lowsignal peripherally. After contrast administration, vivid enhancement wasseen in this right hepatic mass during the arterial/early portal venous phase.
395J. Morgan et al. / Clinical Imaging 32 (2008) 393–395
blood flow, is recommended in order to prevent an untimelydeath due to upper GI hemorrhage from varices. Thetreatment of the liver dysfunction in Alström syndrome issupportive, as in most other causes of end stage liver
disease. At this time, there are no preventative measuresknown that can halt the progression of the liver disease.What also remains unknown in Alström syndrome is why isthere such a wide phenotypic variation in the health andfunction of the liver.
As demonstrated by the patient's medical and surgicalhistory in this report, the clinical course of Alströmsyndrome can result in repeated hospital encounters. Wepresent a case of Alström Syndrome in which the cause ofhepatopathy was pathologically proven to be hepatocellularadenoma with extensive pericellular fibrosis. To assist in themanagement of this disease, an increased awareness ofAlström Syndrome is essential to recognize the manymanifestations of this complex entity.
Reference
[1] Makaryus AN, Popowski B, Kort Y, Mangion J. A rare case of Alströmpresenting with rapidly progressive severe dilated cardiomyopathydiagnosed by echocardiography. J Am Soc Echocardiogr 2003;16:194–6.
[2] Hung YJ, Jeng C, Pei D, Chou PI, Wu DA. Alström Syndrome in twosiblings. J Formos Med Assoc 2001;100:45–9.
[3] Awazu M, Tanaka T, Sato S, Anzo M, Higuchi M, Yamazaki K, MatsuoN. Hepatic dysfunction in two sibs with Alström syndrome: case reportand review of the literature. Am J Med Genet 1997;69:13–6.
[4] Macari F, Lautier C, Girardet A, Dadoun F, Darmon P, Dutour A, RenardE, Bouvagnet P, Claustres M, Oliver C, Grigorescu F. Refinement ofgenetic localization of the Alström Syndrome on chromosome2p 12.13by linkage analysis in a North African family. Hum Genet 1998;103:658–61.