Urology/Nephrology
44
Urology/ Nephrology Lecture Three—March 6 th , 2012
description
Urology/Nephrology. Lecture Three—March 6 th , 2012. Interstitial Cystitis. Interstitial Cystitis. “Painful Bladder Syndrome” Diagnosis of Exclusion Negative culture and cystology No other obvious cause (radiation, chemical, vaginitis, herpes, urethral diverticulum) - PowerPoint PPT Presentation
Transcript of Urology/Nephrology

Urology/Nephrology
Lecture Three—March 6th, 2012

Interstitial Cystitis

Interstitial Cystitis• “Painful Bladder Syndrome”• Diagnosis of Exclusion • Negative culture and cystology• No other obvious cause (radiation, chemical, vaginitis,
herpes, urethral diverticulum)• 18-40 people per 100,000• Affects both genders but most patients are
women• Higher prevalence in white and Jewish • average age 40 years
• Bladder problems in childhood• Up to 50% spontaneous remission (average 8
months)

Interstitial Cystitis• Etiology unknown• Most likely several diseases with similar
symptoms• Multiple theories as to possible cause• Increased epithelial permeability• sensory nervous system abnormalities• autoimmunity
• Associated with severe allergies, IBS, IBD

Signs and Symptoms• Pain with bladder filling, relieved by urination• Urgency, frequency, nocturia• Labs – urinalysis, urine culture, urine cytology,
urodynamic testing• Cystoscopy – distend bladder with fluid
(hydrodistention)• Glomerulations (submucosal hemorrhage)• Hunner’s Ulcers• Thinned bladder epithelium
• Differential Diagnosis – radiation, chemical, bacterial cystitis, herpes, vaginitis, bladder carcinoma, eosinophillic cystitis, tuberculous cystitis, urethral diverticulum, urethral carcinoma




Treatment• No cure – goal is symptomatic relief• Hydrodistention – done as part of work-up – 20-
30% see improvement• Oral medications• Amitryptyline (10-75 mg/day orally)• Nifedipine (30-60 mg/day orally) and other CCBs• Elmiron (100 mg 3x/day orally) – helps restore integrity to
bladder epithelium• Intravesical instillation of DMSO and heparin• TENS units• Acupuncture• Surgery – last resort—cystourethrectomy

Phimosis / Paraphimosis

Phimosis / Paraphimosis• Phimosis – inability to retract the distal foreskin
over the glans penis• Physiologic – occurs naturally in newborn males• Pathologic – inability to retract foreskin when it was
previously retractable or after puberty• Paraphimosis – foreskin cannot be pulled back
over the head of the penis – uncircumcised or partially circumcised males


Risk Factors• Phimosis – Poor hygiene, recurrent inflammation or
infection of glans or foreskin, forceful retraction of foreskin, elderly
• Patients with phimosis are at risk for developing paraphimosis when the foreskin is forcibly retracted past the glans and/or the patient or caretaker forgets to replace the foreskin after retraction.
• Penile piercings increase the risk of developing paraphimosis
• Impairment of venous/lymphatic flow to the glans leads to venous engorgement and worsening swelling arterial supply is compromised penile infarction/necrosis, gangrene

Phimosis - Signs and Symptoms• Physiologic – inability to retract the foreskin
during routine cleaning or bathing; "ballooning" of the prepuce during urination
• Pathologic – painful erections, hematuria, recurrent UTIs, preputial pain, weakened urinary stream
• The foreskin cannot be retracted proximally over the glans penis.• Physiologic – preputial orifice is unscarred and healthy
appearing.• Pathologic – contracted white fibrous ring may be visible
around the preputial orifice

Phimosis

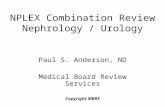
Paraphimosis – Signs and Symptoms• Painful, swollen glans penis • Uncircumcised or partially circumcised patient• Foreskin retracted behind glans penis and cannot
be replaced to its normal position• Tight, restricting ring around the glans • Flaccidity of penile shaft proximal to constriction• Glans – initially its normal pink hue and soft,
becomes increasingly erythematous/edematous, becomes firm and blue or black with necrosis
• Preverbal infant may present only with irritability or may be an incidental finding in a debilitated patient.

Paraphimosis

Treatment• Phimosis – rarely require emergency intervention
– outpatient urology referral• Paraphimosis – urologic emergency – immediate
intervention with goal of reducing foreskin to naturally occuring position over the glans penis• Manual reduction • Osmotic reduction • Puncture reduction • Hyaluronidase method • Aspiration • Vertical incision • Surgery (emergency circumcision)

Treatment

Treatment

Bladder Carcinoma

Bladder Carcinoma• 2nd most common urologic cancer• 2.7 : 1 male-to-female; average age at diagnosis –
65• Risk factors – cigarette smoking and industrial
dye/solvent• 98% are epithelial malignancies• 90% - urothelial cell carcinomas• 7% - squamous cell cancers• 2% - adenocarcinomas

Bladder Carcinoma• Hematuria is presenting symptom in 85-90%• Irritative voiding (frequency and urgency)• Many with no symptoms at all• Abdominal masses – if large or deeply infiltrating• Hepatomegaly or lymphadenopathy (if
metastasis)• Lymphedema of lower extremities – if locally
advanced or metastasis to pelvic lymph nodes

Bladder Carcinoma• Urinalysis – microscopic or gross hematuria, pyuria• Azotemia may be present on labs• Cytology – 80-90% sensitive in detecting higher
grade/stage cancers but less so in superficial or well-differentiated lesions (50%)
• Anemia—chronic blood loss or metastasis to marrow• Urinary tumor markers – under investigation • Imaging – Ultrasound, CT, or MRI may show filling defects• Cystourethroscopy/Biopsy – cystoscopy confirms
diagnosis; pt then undergoes transurethral resection and random biopsies
• Grading (cellular features) and staging (wall penetration and metastasis)


Treatment• Superficial – (Ta, T1) – complete transurethral
resection and intravesical chemotherapy• Invasive, Localized – (T2, T3) – risk of nodal
metastases and progression – radical cystectomy, radiation, or combination of chemotherapy and selective surgery or radiation
• Muscle invasive (T2 or greater) transitional cell carcinoma requires systemic chemotherapy
• READ – Specific forms of treatment (p. 1592)

Prognosis• Initially, 50-80% are
superficial (Ta, Tis, T1)• With proper treatment,
metastasis/progression are low and survival is excellent (81%)
• T2, T3 – 5 year survival ranges from 50-75%
• Long-term survival for pts with metastasis at initial presentation is rare

Testicular Cancer

Testicular Cancer• 2-3 new cases per 100,000
males in US each year• 90-95% of primary testicular
tumors are germ cell tumors• Nonseminomas – mixed cell
types (40%) embryonal cell carcinoma (20%), teratoma (5%), choriocarcinoma (<1%)
• Seminomas – 35%• Non-germinal neoplasms
• 5% of testicular tumors occur in pts with history of cryptorchidism but 15-10% of these occur in normal testis
• Testicular cancer is slightly more common on right than left

Testicular Cancer• Painless enlargement of the testis• Sensations of heaviness• Acute testicular pain 2o intratesticular hemorrhage –
10%• Asymptomatic – 10%• Metatstatic symptoms – 10% (back pain, cough,
lower extremity edema)• Discrete mass or diffuse testicular enlargement• Secondary hydrocele – 5-10%• Supraclaviuclar adenopathy• Abdominal mass• Gynecomastia – 5% (germ cell tumors)

Testicular Cancer• Labs – hCG, α-fetoprofen, LDH• Liver transaminases (metastasis) or anemia
• Imaging – scrotal ultrasound (extratesticular / intratesticular)
• Diagnosis – confirmed by inguinal orchectomy• Staging – chest/abdominal/pelvic CT scanning• Nonseminomas – Stage A – confined to testicle; Stage B –
retroperitoneal lymph node involvement; Stage C – distant metastasis• Seminomas – Stage I – confined to testicle; Stage II –
retroperitoneal lymph node involvement

Testicular Cancer• Initial Intervention – inguinal exploration with
early vascular control of spermatic cord structures• Examine testis for cancer – if unable to exclude
cancer, radical orchiectomy• 75% of stage I nonseminomas are cured by
orchiectomy alone• Stage I and II a/b seminomas – radical
orchiectomy and retroperitoneal irradiation• IIc and Stage III seminomas – chemotherapy

Testicular Cancer• Surveillance – monthly for first 2 years after
diagnosis/treatment then bimonthly for 3rd year • tumor markers at each visit• CXR/CT scans every 3 months• 80% of relapses in first 2 years• Nonseminoma prognosis – stage A with 96-100% 5
yr survival rate, stage B with 90% disease-free survival 5 yrs
• Stage I seminoma – 98%, Stage IIa seminomas – 92-94%
• Stage III seminoma – 95%• Disseminated disease – 55-80%

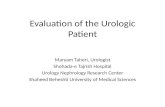
Prostate Cancer

Prostate Cancer• Most common noncutaneous cancer in US men• 2nd most common cause of cancer-related death• 218,000 new cases/yr and 27,000 deaths/yr• Clinical incidence does not equal prevalence on
autopsy• Over 40% of men over 50 y/o have prostatic carcinoma• Incidence increases with age
• Autopsy prevalence is similar world-wide, but clinical incidence varies and is high in North America/Europe, intermediate in South America, low in Far East
• Black race, + family history, high dietary fat intake

Prostate Cancer

Prostate Cancer• Most are associated with palpably normal
prostates and detected solely by elevated PSA• May have focal nodules or indurated areas on DRE• Urinary retention or neurologic symptoms –
epidural metastasis and cord compression• Obstructive voiding – usually due to BPH, but
large or locally extensive prostatic cancers may cause
• Lower extremity edema – lymph node metastasis• Back pain or pathologic fractures – skeletal
metastasis• Axial skeleton – most common site of metastasis

Prostate Cancer• PSA – glycoprotein made only by prostate cells (benign or
malignant) – corresponds with prostate volume• 10-15% of men will have elevated PSA on screening
• 18-30% of men with PSA 4.1-10 will have prostate cancer• 50-70% of pts with PSA > 10 will have cancer
• If not treated, PSA level correlates with volume and stage of disease• Organ confined – usually PSA <10• Advanced disease (seminal vesicle invasion, lymph node
involvement, occult metastases) – PSA >40• 98% of pts with metastatic cancer have elevated PSA
• 20% of pts who undergo radical prostatectomy have normal PSA
• Rising PSA after therapy = progressive disease• PSA increase of over 0.75 ng/mL per year is suspicious

Prostate Cancer• PSA – glycoprotein made only by prostate cells (benign or
malignant) – corresponds with prostate volume• 10-15% of men will have elevated PSA on screening
• 18-30% of men with PSA 4.1-10 will have prostate cancer• 50-70% of pts with PSA > 10 will have cancer
• If not treated, PSA level correlates with volume and stage of disease• Organ confined – usually PSA <10• Advanced disease (seminal vesicle invasion, lymph node
involvement, occult metastases) – PSA >40• 98% of pts with metastatic cancer have elevated PSA
• 20% of pts who undergo radical prostatectomy have normal PSA
• Rising PSA after therapy = progressive disease• PSA increase of over 0.75 ng/mL per year is suspicious

Prostate Cancer• Urinary retention/urethral obstruction – BUN/CR elevation• Bony metastasis – alkaline phosphatase, calcium• DIC (disseminated intravascular coagulation) – advanced• Biopsy – transrectal ultrasound guided biopsy• Spring-loaded 18-gauge biopsy needle• Transrectal US – staging (hypoechoic areas)• MRI – evaluate prostate and lymph nodes• Radionuclide bone scan – superior to plain skeletal films• Most metastases are multiple and usually in axial skeleton• Advanced local lesion, metastasis symptoms, high grade disease,
PSA >20• FNA (lymphadenopathy), plain films (bone scan)• CT is of limited use

Prostate Cancer• DRE alone – 1.5 - 7%, usually advanced cancers• Transrectal US – not appropriate for screening;
expensive, low specificity (high biopsy)• PSA combined with DRE – increased detection rate• Serial PSA – increases specificity (>0.75 ng/yr
increase is increased likelihood of cancer)• PSA density – in normal DRE and transrectal US –
serum PSA divided by volume of the prostate• Free serum PSA vs. protein-bound (lower free PSA
= increased odds of cancer)• Benefit of screening for prostate cancer is
controversial

Prostate Cancer• Localized—active surveillance is an option, but pts
with life expectancy > 10 years should get treatment – radiation vs. radical prostatectomy
• Radical Prostatectomy – seminal vesicles, prostate, ampulla of vas deferens removed• Modern surgery – usually preserves urinary continence and
may also preserve erectile function• Healthy patients with T1 and T2 cancers are ideal candidates• Advanced – rarely candidates for prostatectomy alone
• Radiation – external beam or implantation of radioisotopes
• Surveillance – older pts with small volume, well-differentiated cancers

Prostate Cancer• Cryosurgery – less invasive, positive biopsy rate 7-
23%• Metastatic – death is almost invariably due to
uncontrolled metastatic disease• Most prostate carcinomas are androgen-dependent and
70-80% of metastatic disease will respond to androgen deprivation (table 39-7)
• Prognosis – varies with stage, grade of cancer, PSA level, number and extent of + biopsies• Tables 39-8 and 39-9

Questions?