Urinary tract infections: Optimizing inpatient therapy · 2019-04-23 · •Urinary tract infection...
24
Urinary Tract Infections: Optimizing Inpatient Therapy Tucker Taufoou, PharmD PGY-1 Pharmacy Resident Providence St. Patrick Hospital, Missoula MT MPA Spring Seminar: April 27 th , 2019
Transcript of Urinary tract infections: Optimizing inpatient therapy · 2019-04-23 · •Urinary tract infection...

Urinary Tract Infections:
Optimizing Inpatient Therapy
Tucker Taufoou, PharmD
PGY-1 Pharmacy Resident
Providence St. Patrick Hospital, Missoula MT
MPA Spring Seminar: April 27th, 2019

Disclosure Statement
• IRB status: approved
• Co-investigators:
• Jayme Hartzell, PharmD, MS, BCPS
• Sadie Giuliani, PharmD, BCPS
• Conflict of interest: none
• Project sponsorship: none

Learning Objective
• Develop appropriate antimicrobial regimens for urinary tract infections
based on patient-specific factors

Background
• A urinary tract infection (UTI) of any part of the urinary system including kidneys, ureters, bladder, and urethra
• Prevalence of these infections worldwide is estimated at 150 million people every year with a healthcare cost of $3.5 billion annually in the United States alone
• Four subcategories
• Asymptomatic bacteriuria
• Uncomplicated cystitis
• Complicated cystitis
• Catheter-associated UTI


Background
• Asymptomatic bacteriuria
• Presence of one or more species of bacteria growing in urine (≥105 colony-forming
units [CFU]/mL or ≥108 CFU/L), irrespective of pyuria
• Absence of signs or symptoms attributable to UTI
• Pyelonephritis
• Fever (>99.9°F/37.7°C), signs or symptoms of systemic illness, flank pain, or
costovertebral tenderness

Background
• Uncomplicated cystitis
• Dysuria, urinary frequency or urgency, and/or suprapubic pain in the absence of vaginal symptoms (vaginal pruritus or discharge)
• Complicated cystitis
• Lacks a consensus definition
• Male, poorly controlled diabetes, symptoms >7 days, urologic abnormalities, urologic prosthetic material, or immunosuppression
• Catheter associated-UTI
• Signs and symptoms compatible with UTI with no other identifiable source of infection from a patient whose catheter has been removed within the previous 48 hours

Purpose
• The purpose of this study is to assess empiric antibiotic prescribing for
urinary tract infections before and after implementation of a treatment
algorithm

Methods
• Retrospective, single center, observational review
• Urinary tract infection algorithm with hospitalist, intensivist, and emergency
department provider education
• Empiric antibiotics derived from the Infectious Disease Society of America
guidelines and Providence St. Patrick’s antibiogram
• Data gathered via electronic medical record

Methods
• Inclusion criteria
• Diagnosis of asymptomatic bacteriuria, uncomplicated cystitis, pyelonephritis, or catheter-associated UTI
• Admission to inpatient units
• Exclusion criteria
• <18 years of age
• Pregnant
• Antibiotic use within seven days or empirically covering additional disease state

Methods
• Primary outcome
• Appropriate empiric antibiotic selection defined by treatment algorithm
• Secondary outcomes
• Days of antibiotic therapy
• Length of hospital stay
• 30-day readmission rates
• Length of time before de-escalation to oral therapy

Methods
• Sample size
• Assessed 50 patients diagnosed with UTI from January 2018-March 2018 and February
2019-March 2019 post algorithm implementation
• Statistical analysis
• Fisher’s exact test
• Two-tailed analysis

Results
Demographics and Characteristics Pre-algorithm Post-algorithm
Female, n (%) 37 (74) 27 (54)
Age, years (mean) 68 68
Weight, kg (mean) 165 75
Serum Creatinine, mg/dL (mean) 1.17 1.25
Penicillin allergy, n (%) 5 (10) 9 (18)
ICU, n (%) 3 (6) 1(2)

Results
13
1
20
10
6
14
6
14
10
6
Asymptomatic Bacteriuria
Uncomplicated Cystitis
Complicated Cystitis
Pyelonephritis
Catheter-associated UTI
Urinary Tract Infection Diagnosis
Pre-Algorithm Post-Algorithm

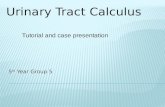
Results
• Primary Outcome
28
36
22
14
Pre-Algorithm Post-Algorithm
Appropirate Empiric Therapy Inappropriate Empiric Therapy
P=0.1443

Results
• Secondary Outcomes
Pre-Algorithm Post-Algorithm
Days of Antibiotic Therapy 7.31 (1-30) 7.44 (1-14)
Length of Hospital Stay 6.12 (1-30) 5.94 (1-20)
30-day Readmission 6 10
Length of Time Before De-escalation 2.53 (1-6) 3.1 (1-7)

Discussion
• Overall, empiric antimicrobial therapy for urinary tract infections improved post provider education and algorithm
• Although results were not statistically significant, a 20% improvement in prescribing is notable
• Strengths
• Local antibiogram used in combination with IDSA guidelines
• Algorithm approved by all infectious disease physicians at Providence St. Patrick Hospital
• Limitations
• Sample size, retrospective chart review, bias
• Unable to verify those originally diagnosed with asymptomatic bacteriuria
• Diagnosis was not always clear
• No external validity

Discussion
• Lessons Learned
• Have clinical pharmacists more involved in algorithm
• Document when algorithm was recommended and whether or not it was accepted
• Increase number of patients reviewed with documented urinary tract infection
• Identify patients by diagnosis code rather than antibiotics prescribed

Conclusions
• Empiric therapy better aligned with guideline directed antibiotics after
algorithm was implemented
• Length of therapy, de-escalation, and length of hospital stay are areas of improvement

Future Directions
• Education
• New IDSA guideline for asymptomatic bacteriuria
• Reinforce appropriate empiric prescribing for urinary tract infections
• Antibiotic de-escalation and length of therapy
• Questioning attitude for antibiotic therapy


Acknowledgments
• Co-investigators
• Jayme Hartzell, PharmD, MS, BCPS
• Sadie Giuliani, PharmD, BCPS
• Infectious Disease Physicians
• Claude Tonerre, MD
• Joshua Christensen, MD
• David Christiansen, MD

References
• Flores-Mireles, A.L., et al. “Urinary tract infections: epidemiology, mechanisms of infection and treatment options” Nature reviews. Microbiology vol. 13,5 (2015): 269-84.
• Bent S, Nallamothu B.K., Simel D.L., et al. Does this woman have an acute uncomplicated urinary tract infection? JAMA. 2002 May 22-29;287(20):2701-10.
• Nicolle L.E., Bradley S.F., Colgan R., et al. Infectious Diseases Society of America Guidelines for the Diagnosis and Treatment of Asymptomatic Bacteriuria in Adults, Clinical Infectious Diseases, Volume 40, Issue 5, 1 March 2005, Pages 643–654, https://doi.org/10.1086/427507
• Gupta K, Hooton T.M., Naber K.G., et al. International Clinical Practice Guidelines for the Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in Women: A 2010 Update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases, Clinical Infectious Diseases, Volume 52, Issue 5, 1 March 2011, Pages e103–e120, https://doi.org/10.1093/cid/ciq257
• Hooton T.M., Bradley S.F., Cardenas D.D., et al. Diagnosis, Prevention, and Treatment of Catheter-Associated Urinary Tract Infection in Adults: 2009 International Clinical Practice Guidelines from the Infectious Diseases Society of America, Clinical Infectious Diseases, Volume 50, Issue 5, 1 March 2010, Pages 625–663, https://doi.org/10.1086/650482
• High K..P, Clinical practice guideline for the evaluation of fever and infection in older adult residents of LTCF: 2008 update by the Infectious Diseases Society of America. Clin Infect Dis. 2009
• Nicolle L.E., Gupta K., Bradley S.F., et. al. Clinical Practice Guideline for the Management of Asymptomatic Bacteriuria: 2019 Update by the Infectious Diseases Society of America, Clinical Infectious Diseases, https://doi.org/10.1093/cid/ciy1121
![7 Catheter-associated Urinary Tract Infection (CAUTI) · UTI Urinary Tract Infection (Catheter-Associated Urinary Tract Infection [CAUTI] and Non-Catheter-Associated Urinary Tract](https://static.fdocuments.us/doc/165x107/5c40b88393f3c338af353b7f/7-catheter-associated-urinary-tract-infection-cauti-uti-urinary-tract-infection.jpg)