URINARY INCONTINENCE ˜UI˚ IN © MIMS
13
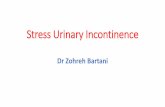
B1 Urinary Incontinence (1 of 13) URINARY INCONTINENCE UI IN WOMEN Yes No 1 Female presents w/ complaints of urinary incontinence (UI) 2 INITIAL ASSESSMENT Voiding dysfunction or significant pelvic organ prolapse? C Specialist referral MAJOR TYPES OF URINARY INCONTINENCE URGE INCONTINENCE OVERFLOW INCONTINENCE STRESS INCONTINENCE INCONTINENCE RELATED TO MEDICAL CONDITION MIXED INCONTINENCE TREATMENT See next page © MIMS © MIMS 2019
Transcript of URINARY INCONTINENCE ˜UI˚ IN © MIMS

B1
Urinary Incontinence (1 of 13)
URINARY INCONTINENCE UI IN
WOMEN
Yes
No
1Female presents w/ complaints of urinary incontinence (UI)
2INITIAL
ASSESSMENTVoiding dysfunction or significant pelvic organ
prolapse?
C Specialist referral
MAJOR TYPES OF URINARY INCONTINENCE
URGE INCONTINENCE
OVERFLOW INCONTINENCE
STRESS INCONTINENCE
INCONTINENCE RELATED TO
MEDICAL CONDITION
MIXED INCONTINENCE
TREATMENTSee next page
© MIM
S
© MIMS 2019

URIN
ARY
INCO
NTIN
ENCE
B2
Urinary Incontinence (2 of 13)
TREATMENT OF URINARY INCONTINENCE
IN WOMEN
URGE INCONTINENCE
OVERFLOW INCONTINENCE
STRESS INCONTINENCE
INCONTINENCE RELATED TO MEDICAL
CONDITION
MIXED INCONTINENCE
A Non-pharmacological therapy• Lifestyle interventions• Bladder retraining
B Pharmacological therapy• Antimuscarinic agents
A Non-pharmacological therapy• Lifestyle interventions
- CatheterizationC Specialist referral
• If surgical intervention is warranted
A Non-pharmacological therapy• Lifestyle interventions• Pelvic fl oor muscle exercises
B Pharmacological therapy• Consider Duloxetine
A Non-pharmacological therapy• Lifestyle interventions• Bladder retraining• Pelvic fl oor muscle exercises
B Pharmacological therapy• Antimuscarinic agents
Treat underlying medical conditionA Non-pharmacological therapy
• Lifestyle interventions• Bladder retraining• Use of anti-incontinence products
Not all products are available or approved for above use in all countries.Specifi c prescribing information may be found in the latest MIMS.
© MIM
S
© MIMS 2019

URIN
ARY
INCO
NTIN
ENCE
B3
Urinary Incontinence (3 of 13)
Yes
No
Not all products are available or approved for above use in all countries.Specifi c prescribing information may be found in the latest MIMS.
URINARY INCONTINENCE UI
IN MEN
Male presents w/ complaints of urinary incontinence (UI)
Urge, stress, or mixed incontinence?
URGE INCONTINENCE
STRESS INCONTINENCE
MIXED INCONTINENCE
3INITIAL
ASSESSMENTPost void residual
>100 mL &/or reduced fl ow
rate?
C Specialist referral
A Non-pharmacological therapy• Lifestyle interventions• Bladder retraining
B Pharmacological therapy• Antimuscarinic agents
A Non-pharmacological therapy• Lifestyle interventions• Pelvic fl oor muscle exercises
B Pharmacological therapy• Consider Duloxetine
A Non-pharmacological therapy• Lifestyle interventions• Bladder retraining• Pelvic fl oor muscle exercises
B Pharmacological therapy• Consider antimuscarinic agents
© MIM
S
© MIMS 2019

URIN
ARY
INCO
NTIN
ENCE
B4
Urinary Incontinence (4 of 13)
1 URINARY INCONTINENCE (UI)
Defi nitionsUrinary Incontinence (UI)• Complaint of involuntary urine leakageStress Urinary Incontinence• Involuntary urine leakage on eff ort or exertion or when coughing or sneezing • Occurs during increased intraabdominal pressure that overcomes sphincter mechanism in the absence of
bladder contraction• Irritative voiding symptoms & nocturia are absent• May be caused by poor pelvic support or intrinsic sphincter defi ciency• Stress urinary incontinence in men is primarily associated w/ surgery of the prostateUrge Urinary Incontinence• Involuntary urine leakage due to detrusor overactivity, associated w/ or immediately preceded by urgency• Patients are unable to hold back their urine when they feel the intense need to void• May be caused by detrusor myopathy, neuropathy, bladder CA, stones or infectionsMixed Urinary Incontinence• Involuntary urine leakage associated w/ both urgency & w/ exertion, eff ort, coughing or sneezing• Present when the bladder outlet is weak & detrusor is overactiveOverfl ow Incontinence• Also referred to as “incomplete emptying”, which describes the dribbling or continuous leakage associated w/
incomplete bladder emptying• May be caused by bladder overdistention, impaired detrusor contraction &/or bladder outlet obstruction• Associated symptoms include weak urinary stream, intermittency, hesitancy, frequency & nocturiaIncontinence related to reversible medical conditions• Transient incontinence
- Arises from an acute medical condition aff ecting the lower urinary tract - Symptoms resolve when the medical condition is addressed & treated
• Functional incontinence - Arises from chronic impairment of physical &/or cognitive functioning - Diagnosis of exclusion - Symptoms may resolve by improving patient’s functional status, treating comorbidities & changing medications
Overactive Bladder (OAB) Syndrome• Urgency w/ or w/o urge incontinence usually accompanied w/ complaints of frequency & nocturiaRisk Factors for UI• Irreversible factors
- Increasing age, race, educational attainment, family history, childhood nocturnal enuresis or daytime wetting, multiparity, forceps delivery, menopause, hysterectomy, surgery for pelvic organ prolapse
• Reversible factors - Body mass index >30, smoking, high caff eine intake, participation in high-impact sports, diabetes, depression, CNS disorders, recurrent UTI, constipation, drugs, pelvic organ prolapse, environmental barrier
© MIM
S
© MIMS 2019

URIN
ARY
INCO
NTIN
ENCE
B5
Urinary Incontinence (5 of 13)
2 INITIAL ASSESSMENT IN WOMEN
Detailed History• Onset & course of UI• Associated lower urinary tract symptoms
- Urgency, urinary frequency, nocturia, hesitancy, straining during urination, interrupted voiding, incomplete emptying
Voiding Diary• Patient should be asked to complete a voiding diary that includes the following:
- Frequency, volume & timing of incontinence, largest single volume voided - Precipitants to incontinence (eg coughing, sneezing, caff eine, alcohol, exercise, sounds of running water)
• Optimum duration of diary is between 24 hr-7 daysOther Components of History• Pregnancies & mode of delivery• Past surgeries, sexual function, bowel function (including constipation & fecal incontinence)• Impact on quality of life• History of prolapse• Prior incontinence therapies, including surgical treatments undertakenMedication History• Drugs causing urinary retention w/ or w/o urinary frequency
- Alpha-adrenergic agonists (Pseudoephedrine, Phenylpropanolamine) - Anticholinergic medications (tricyclic antidepressants, sedating antihistamines, Benzatropine, antipsychotics)
• Drugs causing stress incontinence - Alpha blockers (Prazosin, Terazosin, Doxazosin) - ACE inhibitors if they induce cough - Loop diuretics & alcohol may overwhelm ability to get to the bathroom in time
• Use of conjugate equine estrogens increases the risk of developing UI & worsens pre-existing UIPhysical ExamComprehensive physical exam should include the following:• Examine the general condition of the patient• Cardiovascular exam to assess the presence of volume overload• Palpate abdomen for mass or tenderness• Genital exam
- Inspect vaginal mucosa for atrophy, narrowing of introitus, vault stenosis & infl ammation - Bimanual exam to evaluate presence of masses or tenderness - Assess whether pelvic support is adequate or not - Check for urethral hypermobility - Check for presence of cystocele, rectocele & enterocele
• Direct observation of urine loss using cough stress test• Rectal exam
- Assess sphincter tone & bulbocavernosus refl ex• Neurologic exam
- Observe gait & look for presence of muscular atrophy or neurologic defi cits - Check vibration & peripheral sensation for the presence of peripheral neuropathy
Diagnostic Exams• Urinalysis w/ or w/o urine culture
- Urine cytology, in the presence of hematuria or pelvic pain• Serum creatinine & BUN to check for renal function• Voiding cystogram to check for stress incontinence, cystocele & degree of urethral motion• Intravenous pyelogram to rule out developmental abnormalities, tract anomalies & presence of fi stula• Renal ultrasound• In the evaluation of women w/ uncomplicated stress incontinence, imaging studies of the upper or lower
urinary tract should not be routinely done
Not all products are available or approved for above use in all countries.Specifi c prescribing information may be found in the latest MIMS.
© MIM
S
© MIMS 2019

URIN
ARY
INCO
NTIN
ENCE
B6
Urinary Incontinence (6 of 13)
3 INITIAL ASSESSMENT IN MEN
Detailed History• Helps in categorizing UI to stress, urge or mixed UIVoiding Diary• Patient should be asked to complete a voiding diary that includes the following:
- Frequency, volume & timing of incontinence - Precipitants to incontinence (eg coughing, sneezing, caff eine, alcohol, exercise, sounds of running water)
• Optimum duration of diary is between 24 hr-7 days• Also known as micturition time charts, frequency/volume charts, bladder diariesOthers• Past surgeries, sexual function, bowel habits (including constipation & fecal incontinence)• Impact on quality of life• Medication historyPhysical Exam• Abdominal, rectal, sacral, neurological• Digital rectal exam to assess prostate size, shape & consistency & to check for other rectal pathologiesDiagnostic Exams• Urinalysis w/ or w/o urine culture
- Should be part of the initial assessment - If infection found, treat then reassess
Post Void Residual (PVR) Volume• Amount of urine that remains in the bladder after voiding
- Indicates poor voiding effi ciency• Should be part of the initial assessment in the male patient as its presence is associated w/ UI symptoms• Catheterization is most accurate, but ultrasound may be preferred to avoid infection risk & it has higher patient
acceptability• Presence of voiding dysfunction is considered in patients w/ persistent PVR >100 mLFlow Rate• Determined by detailed clinical historyPad testing• By using an absorbent pad worn over a period of time or during a protocol of physical exercise, urine loss is
measured• Can be used to quantify the presence & severity of UI & also patient’s response to treatmentNote: Consider specialist referral in a patient w/ a complex history (eg recurrent incontinence or incontinence associated w/ hematuria, pain, recurrent urinary tract infections, prostate irradiation, pelvic surgery or radiotherapy, &/or voiding symptoms).
2 INITIAL ASSESSMENT IN WOMEN (CONT’D)
Diagnostic Exams (Cont’d)Cough Stress Test• Patients who have not recently voided urine may be asked to stand over a pad, then they should cough
vigorously• Observe if there is leakage of urine on the pad• Abrupt leakage gives a diagnosis of stress incontinence while delayed leakage suggests mixed incontinencePost Void Residual Volume (PVRV)• Consider if patient has symptoms of voiding dysfunction or history of recurrent urinary tract infection, previous
anti-incontinence surgery, signifi cant pelvic prolapse or spinal cord injury• Catheterization is the most accurate method, but ultrasound may be preferred for higher patient acceptability
& to avoid infection - PVRV <50 mL is considered adequate emptying while PVRV >200 mL is inadequate
Note: Consider specialist referral in a patient w/ a complex history (eg recurrent incontinence or incontinence associated w/ hematuria, pain, recurrent urinary tract infections, suspected fi stula, pelvic surgery or radiotherapy, pelvic organ prolapse, &/or voiding symptoms)
Not all products are available or approved for above use in all countries.Specifi c prescribing information may be found in the latest MIMS.
© MIM
S
© MIMS 2019

URIN
ARY
INCO
NTIN
ENCE
B7
Urinary Incontinence (7 of 13)
A NON-PHARMACOLOGICAL THERAPYLifestyle InterventionsFluid Intake• Average amount of fl uid needed per day is calculated based on patient’s lean body mass• Encourage patients to modify their fl uid intake to produce a 24-hr urinary output between 1-2 L
- A very large or small urine volume output can contribute to urinary incontinenceDiet• Certain foods contain stimulants that may exacerbate symptoms of incontinence
- Heavy or hot spices - Fruits or juices w/ acidic pH - Corn syrup, sugar, honey
• Use of artifi cial sweeteners may also contribute to urge incontinenceCaff eine• Studies suggest that decreasing caff eine may improve frequency & urgency• Eg coff ee, tea, carbonated drinks & hot chocolateWt Loss• In morbidly obese women, massive (surgically induced) wt loss has been shown to signifi cantly decrease
incontinence - Should be considered as fi rst-line treatment
• Moderate wt loss may also decrease incontinenceSmoking Cessation• Smoking >20 cigarettes per day is considered to reinforce urinary incontinenceUse of Anti-incontinence Products• Pads & products that help contain urine loss may be benefi cial• Absorbent products are temporary means to absorb urine & help protect skin & clothing
- May also be used as adjunct to behavioral & pharmacological treatment• Urethral occlusive products
- Artifi cial device inserted into or placed over urethral meatus - Keep patients drier, but more diffi cult & expensive to use compared to absorbent products
• Catheters - Eg indwelling urethral catheters, suprapubic tubes & intermittent self-catheterization - Some patients improve w/ temporary continuous Foley catheterization wherein bladder capacity returns to normal & voluntary detrusor function improves
- Intermittent catheterization is the best form of bladder draining for those who are not physically or mentally handicapped
• Penile clamps for men• Intravaginal devices for womenBladder Retraining• May be off ered as a 1st-line treatment in urge UI or mixed UI• � ere is some evidence that retraining for an overactive bladder is more eff ective than no treatment in patients
w/ urge incontinence• Tends to be more eff ective if urge symptoms are mildUrge Suppression Training• Patient should be instructed to:
- Sit down, if possible, or stand quietly when urge occurs - To perform Kegel exercises (squeeze pelvic fl oor muscles) quickly several times w/o relaxing fully between squeezes - Relax rest of body & focus on another task for distraction - Once the urge subsides, patient should see how long he/she can wait before going to the toilet (eg 30 sec the 1st time, 1 min the next, etc)
Outpatient Bladder Training Protocol• Typically begin w/ a voiding interval of 1 hr during waking hr
- Increase by 15-30 min per wk depending on patient tolerance of the schedule until a 2- to 3-hr voiding interval is achieved
• May start w/ a shorter voiding interval if baseline micturition patterns reveal daytime voiding pattern <1 hr
© MIM
S
© MIMS 2019

URIN
ARY
INCO
NTIN
ENCE
B8
Urinary Incontinence (8 of 13)
A NON-PHARMACOLOGICAL THERAPY (CONT’D)Pelvic Floor Muscle Exercises• Currently known as pelvic fl oor muscle training (PFMT)• A program where repeated voluntary pelvic fl oor muscle contraction is taught by a healthcare professional for
prevention & treatment of UI• Should be the 1st line of therapy to be off ered for at least 3 mth duration in patients suff ering from stress or
mixed incontinence, it can also be off ered to elderly & post-natal women - Improves the function of the pelvic fl oor muscles - Involves recruitment of pelvic fl oor muscle strengthening & skill training
- Contraction of pelvic fl oor muscle causes inward lift of the muscles, resulting to increase in urethral closure pressure, stabilization & resistance to downward movement - Biofeedback may promote awareness of the physiological action of pelvic fl oor muscles by visual, tactile or auditory means - Weighted vaginal cones are used to facilitate strengthening of pelvic fl oor muscles through passive & active contraction of the muscles which prevents the cones from slipping out of the vagina - Electrical stimulation uses electrical current to stimulate the pelvic fl oor muscles or to normalize refl ex activity
- Strengthens the external urinary sphincter; builds up pelvic fl oor muscles to prevent prolapse & helps retrain the bladder
- However, more good-quality evidence is needed to prove the clinical & cost eff ectiveness of these conservative therapies for UI
• Digital assessment of pelvic fl oor function prior to initiating therapy should be undertaken only by a properly trained clinician
• Pelvic fl oor exercises should be considered for male patients following radical prostate surgery as there seems to be some benefi t
• In men w/ complaints of post-micturition dribble, both pelvic fl oor muscle exercises & urethral milking appear to be eff ective
Developing Pelvic Floor Muscle Exercise Routines• Program should be individualized but should include exercises for both fast- & slow-twitch muscle fi bers• Perform until the muscle fatigues, several times a day• Usual program consists of 3 sets of 8 repetitions, each sustained for 6 seconds, done 3x per wk• Should be practiced x 15-20 wk & continued on a maintenance basis
© MIM
S
© MIMS 2019

URIN
ARY
INCO
NTIN
ENCE
B9
Urinary Incontinence (9 of 13)
Not all products are available or approved for above use in all countries.Specifi c prescribing information may be found in the latest MIMS.
B PHARMACOLOGICAL THERAPY
Antimuscarinic Agents• Act mainly during the urinary storage phase, decreasing urge & increasing bladder capacity• All available antimuscarinic agents decrease the frequency of urgency & incontinence episodes eff ectively• Product should be selected on the basis of cost & tolerability• Antimuscarinic therapy should be tried for 4-12 wk to assess benefi ts & side eff ects
- If eff ective & tolerable, reassess after 6 mth to ascertain continuing need - If patient did not tolerate or failed therapy, may consider giving a diff erent antimuscarinic agent
Considerations Regarding Antimuscarinic � erapy in Men• If OAB exists w/o evidence of bladder outlet obstruction, then 1st line therapy w/ antimuscarinics can be
considered• In men w/ concomitant bladder outlet obstruction, bladder outlet resistance should be appropriately treated
before considering the addition of antimuscarinics for OABListed in alphabetical order:Darifenacin• Clinical eff ectiveness has been documented in several random controlled trials• Onset of action is seen by wk 2 of therapyFesoterodine• � e 8-mg daily dose has been shown to be more eff ective than the 4-mg daily dose of Tolterodine ER in treating
& improving urge incontinence but risk of side eff ects is higherOxybutynin• Smooth muscle relaxation of the urinary bladder occurs by inhibiting the action of acetylcholine paralyzing
the smooth muscles• � e immediate release form of Oxybutynin is recognized for its effi cacy & newer agents are compared to it
once effi cacy over placebo has been determined• Newer agents have been shown to be as effi cacious but may have improved dosing schedules or side eff ect
profi lesPropiverine• Shown to have both antimuscarinic & calcium antagonistic actions (importance of calcium antagonist
component has not been established)• Has a documented benefi cial eff ect in the treatment of detrusor overactivity (DO) & has an apparent acceptable
side eff ect profi leSolifenacin• Has a well-documented eff ect in OAB/DO & adverse eff ect profi le seems acceptable• Studies have shown decrease in incontinence episodes, voids per day & urgency episodes along w/ increase in
bladder capacityTolterodine• Has selectivity for urinary bladder• Several studies have documented signifi cant reduction in micturition frequency & in the number of incontinence
episodes• Reduction in wkly urge incontinence & total incontinence in women are similar between extended-release
products of Oxybutynin & Tolterodine; tolerability is also comparable• Long-acting formulations have improved tolerability w/o impairing eff ectivenessTrospium• Signifi cantly decreases average frequency of toilet voids & urge-incontinent episodes compared to placebo
- Decreases smooth muscle tone in the bladder - Eff ective for treatment of OAB
• Consider to give in patients w/ cognitive dysfunction• Eff ects occur by wk 1 of therapy & nocturnal frequency decreases signifi cantly by wk 4• Dry mouth appears to occur in comparable frequency as TolterodineBeta-adrenoceptor AgonistMirabegron• May be given to patients w/ urge incontinence• Improvement of urge incontinence is better than w/ placebo• Side eff ects appear mild & are not clinically signifi cant
© MIM
S
© MIMS 2019

URIN
ARY
INCO
NTIN
ENCE
B10
Urinary Incontinence (10 of 13)
Not all products are available or approved for above use in all countries.Specifi c prescribing information may be found in the latest MIMS.
B PHARMACOLOGICAL THERAPY (CONT’D)Peripherally-Acting Muscle RelaxantBotulinum toxin A• May be off ered as a bladder wall injection to:
- Patients w/ urgency urinary incontinence or overactive bladder who have failed antimuscarinic therapy - Patients w/ urodynamic studies showing bladder storage impairment who have failed antimuscarinic therapy
• Patients must be informed of the following: - Risk of increased postvoid residual urine is high & there may be a need to self-catheterize - Risk of developing urinary tract infection - Long-term side eff ects are still uncertain
• Patients at risk of renal complications should have monitoring of their upper urinary tractSerotonin & Norepinephrine Reuptake InhibitorDuloxetine• May be considered in patients w/ moderate to severe stress incontinence
- Equally eff ective in improving stress incontinence symptoms in patients w/ mixed urinary incontinence• Should only be used as part of a management plan that includes 2 wk pelvic fl oor muscle exercises• � erapy should be evaluated after 2-4 wk for eff ectiveness & tolerability• Patients who continue therapy should be reassessed after 12 wk to assess progressEstrogen• Postmenopausal women may be off ered vaginal estrogen therapy especially if vulvovaginal atrophy symptoms
are present
C SPECIALIST REFERRAL
Consider immediate referral to a specialist in the following conditions:• Incontinence w/ abdominal &/or pelvic pain• Hematuria in the absence of an infection• Suspected fi stula• Complex neurological conditions (eg Parkinson’s disease, spinal cord injury)• Abnormal fi ndings (eg pelvic mass or symptomatic organ prolapse beyond the hymen)Consider elective referral to a specialist in the following conditions:• Persistent symptoms after an adequate therapeutic trial• Uncertain diagnosis & lack of reasonable treatment plan• Signifi cant increase in PVRV that does not resolve after treatment of possible precipitants (eg medications,
stool impaction)• Prior pelvic surgery or pelvic irradiation• Desire for surgical treatment
© MIM
S
© MIMS 2019

URIN
ARY
INCO
NTIN
ENCE
B11
Urinary Incontinence (11 of 13)
All dosage recommendations are for non-pregnant & non-breastfeeding women, & non-elderly adults w/ normal renal & hepatic function unless otherwise stated.
Not all products are available or approved for above use in all countries.Products listed above may not be mentioned in the disease management chart but have been
placed here based on indications listed in regional manufacturers’ product information.Specifi c prescribing information may be found in the latest MIMS.
Dosage Guidelines
NEUROMUSCULAR DISORDER DRUG
Drug Dosage Remarks
Distigmine Initial dose: 5 mg PO 24 hrlyAfter 1 wk, 5-10 mg PO every 2-3 days depending on the reaction
Adverse Reactions• GI eff ects (N/V, diarrhea, enterospasms); Ophtha eff ect (miosis);
CV eff ect (bradycardia); Resp eff ect (bronchospasm); Other eff ects (increased salivation & lacrimation, sweating, muscle spasms & tremor, muscle weakness, diffi culty in swallowing)
Special Instructions• Contraindicated in patients w/ severe vagotonia or dominance
of the parasympathetic part of the autonomic nervous system• Take the whole dose on an empty stomach, 30 min before breakfast
PERIPHERALLY-ACTING MUSCLE RELAXANT
Drug Dosage Remarks
Botulinum toxin A
200 u IM into detrusor muscle via a fl exible or rigid cytoscope
Adverse Reactions• Inj site reactions (pain, tenderness &/or bruising); Other eff ects
(fever, fl u, facial paresis, neck pain); Dermatological eff ects (rarely skin rash, pruritus)
Special Instructions• Contraindicated in patients w/ myasthenia gravis,
Eaton-Lambert syndrome, acute UTI & urinary retention who are not routinely doing clean intermittent self-catheterization
• Use w/ caution in patients at risk of angle-closure glaucoma, amyotrophic lateral sclerosis, pregnant, childn <12 yr & elderly
OESTROGENS, PROGESTERONES & RELATED SYNTHETIC DRUGS
Drug Dosage Remarks
Estriol 0.5 mg (1 application) vag at night for 1st few wkGradually reduce dosage based on symptom reliefMaintenance dose: 0.5 mg vag 2x/wk
Adverse Reactions• Irritation or itching at application site, breast discomfort or painSpecial Instructions• Use with caution in patients w/ leiomyoma, endometrial
hyperplasia, 1st degree heredity for breast cancer, HTN, DM, severe liver disorders, severe headache, SLE, epilepsy, asthma, otosclerosis, thromboembolic disorders
• Avoid in patients w/ known or suspected breast cancer, estrogen-dependent tumors, undiagnosed vag bleeding, untreated endometrial hyperplasia, thrombosis, thromboembolism, acute liver disease, porphyria
• Discontinue use if jaundice or liver function deterioration, signifi cant increase in BP or new onset of migraine-type headache occurs
© MIM
S
© MIMS 2019

URIN
ARY
INCO
NTIN
ENCE
B12
Urinary Incontinence (12 of 13)
All dosage recommendations are for non-pregnant & non-breastfeeding women, & non-elderly adults w/ normal renal & hepatic function unless otherwise stated.
Not all products are available or approved for above use in all countries.Products listed above may not be mentioned in the disease management chart but have been
placed here based on indications listed in regional manufacturers’ product information.Specifi c prescribing information may be found in the latest MIMS.
Dosage Guidelines
QUINOLONE
Drug Dosage Remarks
Pipemidic acid
400 mg PO 12 hrly
Adverse Reactions• GI eff ects (nausea, abdominal pain); CNS eff ects (muscular weakness,
myalgia, intracranial hypertension); Other eff ects (exanthematous or urticarial skin rashes)
Special Instructions• Use w/ caution in patients w/ impaired renal or hepatic function, CNS
damage, convulsion; strong sunlight exposure• Avoid in lactating patients
SEROTONIN & NOREPINEPHRINE REUPTAKE INHIBITOR
Drug Dosage Remarks
Duloxetine 40 mg PO 12 hrlyReassess after 2-4 wkIf intolerable side eff ects occur: Decrease dose to 20 mg PO 12 hrly
Adverse Reactions• CNS eff ects (insomnia, fatigue, headache, dizziness, tremor); GI eff ects (dry
mouth, constipation, nausea, anorexia, decreased appetite); Ophtha eff ects (blurred vision); Misc eff ects (increased sweating, hyponatremia has been reported rarely; suicide ideation can occur)
Special Instructions• Avoid in women w/ hepatic dysfunction• Use w/ caution in patients w/ a history of mania, bipolar disorder &/or
seizures, in combination w/ antidepressants, in patients w/ increased intraocular pressure or those at risk for acute narrow-angle glaucoma
• Taper slowly at discontinuation of therapy
URINARY ANTISPASMODICS
Drug Dosage Remarks
Mirabegron 50 mg PO 24 hrly
Adverse Reactions• Tachycardia, urinary tract infections• Uncommon: Cardiac eff ects (palpitations, atrial fi brillation); GI eff ects (dyspepsia,
gastritis); Other eff ects (rash, pruritus, joint swelling, increased liver enzymes)Special Instructions• Use w/ caution in patients w/ severe renal impairment or end-stage renal disease,
severe or moderate hepatic impairment, severe uncontrolled hypertension, history of QT prolongation or taking drugs known to prolong QT interval
Antimuscarinic AgentsFlavoxate 200 mg PO
6-8 hrlyAdverse Reactions• CNS eff ects (nervousness, vertigo, fatigue, headache, confusion); CV eff ects
(tachycardia, palpitation); GI eff ects (dry mouth & throat, abdominal pain, constipation); Ophtha eff ects (blurred vision, increased intraocular pressure); Other eff ects (dysuria, hypersensitivity reactions, hyperpyrexia, eosinophilia, leukopenia)
Special Instructions• Contraindicated in patients w/ pyloric or duodenal obstruction, intestinal
lesions or ileus, achalasia, GI hemorrhage, obstructive uropathies of the lower urinary tract, myasthenia gravis, severe ulcerative colitis, toxic megacolon, glaucoma
• Use w/ caution in the elderly & in patients w/ coronary artery disease, congestive heart failure, arrhythmias, autonomic neuropathy, hepatic & renal impairment© M
IMS
© MIMS 2019

URIN
ARY
INCO
NTIN
ENCE
B13
Urinary Incontinence (13 of 13)
Please see the end of this section for the reference list.
All dosage recommendations are for non-pregnant & non-breastfeeding women, & non-elderly adults w/ normal renal & hepatic function unless otherwise stated.
Not all products are available or approved for above use in all countries.Products listed above may not be mentioned in the disease management chart but have been
placed here based on indications listed in regional manufacturers’ product information.Specifi c prescribing information may be found in the latest MIMS.
Dosage Guidelines
URINARY ANTISPASMODICS (CONT’D)
Drug Dosage Remarks
Antimuscarinic Agents (Cont’d)Darifenacin Initial dose: 7.5 mg PO
24 hrly After 2 wk, may increase dose to 15 mg PO 24 hrly if no adequate response
Adverse Reactions• GI eff ects (dry mouth, constipation, abdominal pain,
diarrhea); Ophtha eff ects (blurred vision, dry eyes); CNS eff ects (drowsiness, headache); CV eff ects (palpitations, arrhythmias, tachycardia); GU eff ects (urinary retention, dysuria); Other eff ects (angioedema, skin reactions)
Special Instructions• Avoid in patients w/ urinary or gastric retention,
uncontrolled narrow-angle glaucoma & in patients at risk for these conditions
• Use w/ caution in patients w/ GI obstructive disorders, severe constipation, ulcerative colitis, myasthenia gravis, controlled narrow-angle glaucoma; in patients w/ signifi cant bladder outfl ow obstruction
Darifenacin• Avoid in patients w/ severe hepatic impairment; use w/
caution if moderate impairmentFesoterodine• Use w/ caution in patients w/ renal & hepatic impairment,
concomitant use of CYP3A4 inhibitorsPropiverine• Monitor hepatic enzymes during long-term therapySolifenacin • Avoid in patients w/ severe renal dysfunction or in those w/
moderate-severe liver disease Trospium• Use w/ caution in patients w/ moderate-severe hepatic
impairment• Use w/ caution in patients w/ renal impairment
Fesoterodine fumarate
4-8 mg PO 24 hrly
Oxybutynin Regular release: 5 mg PO 8-12 hrlyElderly: Up to 5 mg PO 8 hrlyExtended release:5-10 mg PO 24 hrly; may be adjusted by 5 mg/day by intervals of ≥1 wkMax dose: 30 mg/day
Propiverine 15 mg PO 8-12 hrlySolifenacin 5-10 mg PO 24 hrlyTolterodine Regular release:
2 mg PO 12 hrly Extended release:4 mg PO 24 hrlyMay decrease to 2 mg PO 24 hrly depending on response & tolerability
Trospium 20 mg PO 12 hrly or 15 mg PO 8 hrly
VASOCONSTRICTOR
Drug Dosage Remarks
Midodrine hydrochloride
2.5-5 mg PO 8-12 hrly Adverse Reactions• Cardiac eff ects (bradycardia, supine & sitting hypertension);
Other eff ects (paresthesia & pruritus mainly of the scalp, chills, urinary urgency, retention & frequency)
Special Instructions• Monitor blood pressure, slowing of heart rate may occur• Use w/ caution in patients w/ urinary retention, orthostatic
hypotension, diabetes, renal & hepatic impairment; concomitant use w/ other vasoconstrictor drugs
• Avoid in patients w/ increased blood pressure, severe organic heart disease, acute renal disease, pheochromocytoma, thyrotoxicosis© MIM
S
© MIMS 2019