
URINARY ELIMINATION DISORDERS
111
URINARY ELIMINATION DISORDERS Trina Domanais, RN, MN,MAN
Transcript of URINARY ELIMINATION DISORDERS

URINARY ELIMINATION DISORDERS
Trina Domanais, RN, MN,MAN

• The renal system is responsible for maintaining homeostasis in the body by carefully
• regulating fluid and electrolytes, acid – base balance,
• removing wastes, and
• providing hormones responsible for red blood cell production, hypertension and bone metaboliam


LOWER URINARY SYSTEMA. Bladder
- Its main function is for storage of urine. As volume of urine increases, starting from 300-500 ml, awareness of the need to void develops.
- Voluntary voiding is accomplished by stimulation of the parasympathetic nerve fibers causing coordinated contraction of the detrusor muscle and the bladder body.
B. Urethra
• The urethra drains urine from the bladder to an exterior opening of the body, the external urethral orifice.
• In females, the urethra is about 3 to 4 cm. (1.5 in.). In males, the urethra is about 15 to 20 cm (6 to 8 in.) Micturition, or urination, is the process of releasing urine from the bladder into the urethra.

• Kidneys
• The two kidneys lie on the posterior wall of the abdomen outside the peritoneal cavity.
• weighs about 150g is about the size of an indented region called the hilum through which passes the renal artery and vein, lymphatic, nerve supply.
• The outer part is the cortex and inner region called medulla.
• The medulla is divided into multiple cone shaped masses called renal pyramids.
• The base of each pyramid terminates in the papilla, which projects into the space of renal pelvis, a funnel shaped continuation of the upper end of the ureter.
• The outer border of the pelvic is divided into minor calyces, the walls up the calyces, pelvis that contain contractile elements that propel the urine toward the bladder, where urine is stored until it is emptied by micturition.
• The functional unit of the kidney is the nephron.

NEPHRONS
• Millions of nephrons are present in each human kidney which aid in the urine production and process of removing metabolic waste products from the blood. These significant structures extend between the cortex and the medulla. At one end of the nephron is closed, expanded and folded into a double-walled cuplike structure called the Bowman’s capsule. This capsule encloses glomerulus, the nephron’s primary structure in filtering function.
•

FUNCTIONS OF KIDNEY• Kidney performs different functions in order to maintain
homeostasis in the body by excreting metabolic waste products and reabsorbing necessary elements for the body. The following are the functions of the kidney:
1. Formation of urine
• The formation of urine happens in three phases which are filtration, reabsorption and secretion. Each of these processes happens in the body in order to create homeostasis by removing those metabolic waste products and reabsorbing helpful substances.
• a. Filtration. The filtration process is nonselective, passive process which forms essential blood plasma without blood protein but both of it is normally too large to pass through the filtration membrane. If any of the two appeared in the urine, it would mean that there is a problem in the glomerular filters. The water and solute are smaller than proteins that are forced through the capillary walls and pores of Bowman’s capsule into the renal tubule.

• b. Reabsorption. Tubular reabsorption is achieved by active and passive transfer mechanism Sodium, potassium, calcium, phosphate, and uric acid are actively reabsorbed.
• c. Secretion. Some of substances such as hydrogen and potassium ion, creatinine, and ammonia, move from the peritubular capillary blood and secreted by the tubule cells into the filtration.
• Excreting nitrogenous waste products , unnecessary and excess substances .

FUNCTIONS OF KIDNEY• 2. Body’s Water Volume Regulator
• Antidiuretic hormone (ADH), also called vasopressin.
• Vasopressin is produced in the hypothalamus and stored in nearby pituitary gland. Receptors in the brain monitor the blood’s water concentration causing the release of ADH in the bloodstream if the amount of salt and other substances is too high.
• 3. Excretion of Metabolic Waste Products
• Waste, drugs, & metabolites. 25g to 30g of urea is produced as the end product of protein breakdown and excreted daily making it the major waste product of protein metabolism. Other waste products are creatinine, phosphates and sulfates. Uric acid, formed as a waste product of purine metabolism, is also eliminated in the urine.

FUNCTION OF THE KIDNEYS4. Blood Pressure Regulator
• Regulating blood pressure is linked to the kidneys' ability to excrete enough sodium chloride (salt) to preserve normal sodium balance, extracellular fluid volume and blood volume.
5. Regulation of Acid-Base Balance.
• It helps maintain normal pH by retaining or excreting hydrogen ions and regenerating lost buffer. The kidneys excrete acids that the lungs cannot excrete and they can excrete hydrogen ions or reabsorb bicarbonate to correct acidosis.

FUNCTION OF THE KIDNEYS6. Regulation of Red Blood Cell Production.
• Erythropoietin stimulates the bone marrow to produce red blood cells, thereby increasing the amount of hemoglobin available to carry oxygen.
7. Vitamin D Synthesis
• The kidneys are also responsible for the final conversion of inactive vitamin D to its active form, 1,25-dihydroxychole-calciferol. Vitamin D is necessary for maintaining normal calcium balance in the body.
8. Secretion of Prostaglandins
• The kidneys also produce prostaglandin E and prostacyclin, which have a vasodilatory effect and are important in maintaining renal blood flow.

RENAL EXCRETORY STUDY1. URINALYSIS - assessed the nature of the urine produce and evaluates the color,ph and specific gravity, determines the presence of glucose (glycosuria, protein, blood(hematuria), ketones ( ketonuria) and analyzes sediment for cells (WBC, called pyuria, casts bacteria, crystals)
Nursing Responsibilities:
• Cleanse perineal area, spread labia and cleanse meatus from front to back using antiseptic sponge, for males, retract foreskin for uncircumcised penis and cleanse glans antiseptic sponge, must be analyze 1 hour after of collection,
2. For 24 Hour urine collection ( creatinine clearance) discard the first voided urine, collect all subsequent urine in a sterile container for 24 hours.
3. Kidney, ureter ,bladder X-ray (KUB ) - plain film abdominal flat plate x-ray identifying the number and size of kidneys with tumors, malformations and calculi ; no special preparations needed


4. IVP – fluoroscopic visualization of the urinary tract after injection with a radiopaque dye
Nursing Responsibilities - Test for iodine sensitivity, enema before the procedure, 8 hours, NPO, push fluids after.
5. ULTRASOUND – non- invasive visualization of the kidney, ureter, bladder through the use of sound waves
• Nursing Responsibilities- Supine position, NPO not required, cleanse conducting gel from skin after the procedure

CYSTOSCOPY∙ CYSTOSCOPY – use of lighted scope to inspect the
bladder (CYSTOSCOPE); maybe use to remove tumors, stones, or other foreign materials or use to implant radium, place catheters in the ureters.
• Nursing Responsibilities Before the Procedure
• Explain the procedure will be done under local or general anesthesia, secure consent, administer sedative as ordered, NPO for general anesthesia, or NPO after light breakfast for local anesthesia, enema as ordered ,let client assume a lithotomy position
• Post Procedure
• Mild analgesic or warm sitz bath to relieve pain, I &O and temperature monitoring, explain that
• hematuria expected post 24-48 hours, assess for clots, burning sensation upon urination maybe felt, and
• force fluids.


RENAL BIOPSY∙ – removal of kidney tissue for microscopic study
• Open method promotes better visualization but high risk for infection, close method none by aspiration with a fine needle and has less risk for infection
• Nursing Responsibilities before and during the procedure
• Secure consent,NPO after midnight,assess hemoglobin and coagulation studies ,assist client to assume
• Prone position with a pillow below the abdomen, apply pressure for 20 minutes on the aspirated area after the procedure
• Post Procedure
• Flat bedrest for 24 hours, monitor for hemorrhage, hypotension, dizziness, tachycardia ,pallor , back, flank and shoulder pain, avoid strenuous activities, coughing, sneezing and straining, encourage fluid to avoid urinary retention and clots, monitor hemoglobin, assess for hematuria and if present should cease 24 hours after the procedure. Administer analgesics

SERUM ELEC, SERUM BUN, SERUM CREATININE
∙ Blood chemistry and Hemoglobin tests - these tests or panels are groups of tests that measure many chemical substances in the blood that are released from body tissues or are produced .For kidney function, creatinine and blood urea nitrogen .
• Nursing Responsibilities – NPO is not required for BUN , hemoglobin and creatinine , instruct the client not to eat red meat a day prior to creatinine test ,intake of red meat can affect the result.
•


URINARY TRACT INFECTION• An infection (UTI) cause by bacteria, virus, fungus,
that occurs in the urinary tract.
• has indwelling catheter,
• urinary retention,
• urinary and fecal incontinence
• poor perineal hygiene practice
• renal scarring from previous infection,
• decrease ureteral peristalsis, presence of urinary tract obstruction
• female
• sexual activity
Causative microorganisms are
Escherichia coli ,
Staphylococcus,
Streptococcus,
Enterobacter
klebsiella and
Aerobacter,
Pseudoaeriginosa.

PATHOPHYSIOLOGY


URETHRITIS1. URETHRITIS – is inflammation of the urethra.
Causes
• Escherichia coli
• Chlamydia Trichomonas
• Neisseria gonorrhoeae
• herpes simplex virus type 2),
• trauma, or hyper-sensitivity to chemicals in products such as vaginal deodorants,
• spermicidal jellies,
• bubble bath detergents.

SIGNS AND SYMPTOMS
∙ Dysuria
∙ Frequency
∙ Urgency
∙ and bladder spasms
∙ A urethral discharge may be noticed.

MEDICAL MANAGEMENT
Medical Diagnosis
• Urinalysis
• Urethral smear

MEDICAL TREATMENT
• Antimicrobials
• Find the partner, test the partner, treat the partner
• IV hydration

NURSING CARE

NURSING INTERVENTION• Sitz baths are soothing and may reduce the pain
• . Instruct female patients to wipe from front to back after toileting, and to void before and after sexual intercourse .
• Discourage bubble baths and vaginal deodorant sprays.
• Instruct uncircumcised male patients to clean the penis under the foreskin regularly.
• Advise patients to void after swimming.
• Perineal Care
• Avoid Douche
• Increase OFI


CYSTITIS2. CYSTITIS - is inflammation of the urinary bladder.
Causes
• Bacterial contamination
• prolonged immobility
• renal calculi
• urinary diversion
• indwelling catheters
• radiation therapy
• Some types of chemotherapy.

PATHOPHYSIOLOGY


SIGNS AND SYMPTOMS∙ Urgency∙ Frequency∙ Dysuria∙ Hematuria∙ nocturia∙ bladder spasms∙ Incontinence∙ low-grade fever. ∙ Urine may be dark, tea colored, or
cloudy. ∙ Fever∙ Fatigue∙ pelvic or abdominal discomfort∙ bladder spasms experienced as
pain behind the symphysis pubis.

DIAGNOSTIC TESTS• Urinalysis
• culture and sensitivity.
• USD of KUB

MEDICAL TREATMENT
• Antibiotic
• mild analgesic: acetaminophen
• Phenazopyridine (pyridium) ( pain reliever)
• Oxybutynin chloride (Ditropan may be ordered for 2 to 3 days to decrease discomfort and bladder spasms.

NURSING CARE


NURSING CARE • Advise patient to complete the entire course of antibiotics and take
analgesics as ordered.
• If phenozopyradine is given, advise patient that the drug causes red-orange urine Warm sitz bath , oral fluid intake 30m/kg of fluid per day.
• To reduce risk of future infection, teach patient to,
• wear cotton undergraments
• avoid tight-fitting clothing in the perineal area
• take shower instead of tub bath, avoid caffeine drinks, apple, grapefruit, orange these irritates the bladder
• maintain high fluid intake and void often
• Wiping from front to back after voiding for female and drink a glass of water after swimming
• before and after intercourse to flush the bacteria.

PYELONEPHRITIS

. PYELONEPHRITIS3. PYELONEPHRITIS – inflammation of the renal pelvis. It may affect one or both kidneys.
Cause
• Acute pyelonephritis is most often caused by an ascending bacterial infection, but it may be bloodborne.
• Chronic pyelonephritis most often is the result of reflux of urine from inadequate closure of the ureterovesical junction during voiding.
• It is also usually caused by long standing UTIs with relapses and reinfections, may even lead to chronic renal failure .


ACUTE
• High fever
• Chills
• Nausea & vomiting
• dysuria.
• Severe pain or a constant dull ache in the flank area.
CHRONIC
• fatigue
• hypertension
• increase BUN and creatinine
• a slight aching over one or both kidneys.

DIAGNOSTIC TESTS• Urinalysis
• Urine culture sensitivity
• CBC
• IVP
• Cystoscopy

MEDICAL TREATMENT• Antibiotics
• Urinary tract anti-septics: Nitrofurantoin
• Analgesics: Mefenmic Acid, Ibufropen
• antispasmodics : Urinex, Uricol, Uretrate
• Adults are advised to dink at least eight 8-oz glasses of fluids daily.
• Intravenous fluids
• Increase OFI
• . Dietary salt and protein restriction
• follow-up cultures to determine whether the infection has been resolved.

NURSING CARE

NURSING CARE
• Record the presence of signs and symptoms,
• Assess history of previous urinary disorders,
• Increase oral fluid intake at least 8 oz of glasses a day,
• Advise patient to complete the entire course of antibiotics and take analgesics as ordered.
• Limit physical activity and exercise
• Protein and salt dietary restrictions if advised by the physician.
• Report if s/sx re-occurs

Group A Beta Hemolytic Streptoccoci






NURSING CARE

NURSING CARE
• Assessment• Check Labs• Administer meds :Antibioticsm Anti Inflammatory• Limit OFI to 1L/ day• Hydrations• Perineal Care• Treat Sorethroat• Vaccine

NURSING DIAGNOSIS

B.OBSTRUCTIVE DISORDERS•Renal calculi is the formation of stones in the urinary tract . These are crystalline structures that form from the components of urine.


FACTORS FOSTERING CALCULI FORMATION
∙ Concentrated urine
∙ Excessive intake of vitamin D, animal protein, oxalates, sodium, sucrose, vitamin C, calcium based antacids
∙ Familial history
∙ Immobility, urine stasis, sedentary lifestyle
∙ Altered urine pH
∙ Lack of kidney substance that inhibits calculi formation

COMPONENTS
1.Calcium salts (phosphate and oxalate)
2. Uric acid
3. magnesium
4. Ammonium phosphate (struvite) or cystine.



MEDICAL DIAGNOSIS
• Urinalysis
• Urine culture and sensitivity
• IVP
• KUB ultrasound
• Computed tomography (CT) scan

MEDICAL ,SURGICAL AND PHARMACOLOGIC MANAGEMENT
Phases of Stone Management
1. Acute phase
a. Narcotics: Tramadol
b. Antispasmodic:
c. Anti –emetic: Plasil
warm bath to relieve flank pain
2. Elimination of stone• Waiting to be passed out
• Mechanical intervention
• Surgical intervention
3. Long term prevention of recurrence• OFI (3-4l/day), diet, medication

PHARMACOLOGIC MANAGEMENT99
1.potassium citrate therapy - It attaches to calcium in the urine, preventing the formation of mineral crystals ; prevents the urine from becoming too acidic .
2.Thiazides – increases urinary Ca excretion
3. Allopurinol – prevents formation of uric acid nidus
• FOR SMALL STONES
4. Alpha blockers or α-adrenergic-antagonist - It relax muscle tension in the ureter and facilitate passage
• E.g. tamsulosin
5. Sodium bicarbonate
6. Pain relievers; NSAIDS, NARCOTICS

SURGICAL AND NON-SURGICAL MANAGEMENT OF STONE
• Surgical management are indicated if there is progressive renal damage, obstruction of urine flow , presence of infection and severe pain.
1. Nephrolithotomy (removal of kidney stones)
2. Ureterolithotomy (removal of stones in the ureters) .

NEPHROLITHOTOMY


NON SURGICAL MANAGEMENT
1.Ureteral Stent- are small tubes inserted into the ureter to treat or prevent a blockage that prevents the flow of urine from the kidney to the bladder.

LITHOTRIPSY

2. Lithotripsy is a process of eliminating a calculus in the renal pelvis, ureter , bladder by crushing the stone. It can be accomplished by Extracorporeal shock wave lithotripsy (ESWL) which utilizing sound, laser, or shockwave energy with a use of a lithotripter. It is guided by an ultrasound probe, the energy is directed to the stone through a water-filled cushion.

• Cystoscopy/Ureteroscopy - use of lighted scope or a tube inserted into the urethra into the bladder and ureters to remove stone and uses a laser fiber to crush the stone in the case of ureteroscopy.


• Percutaneous nephrolithotomy
• – The surgeon creates a tunnel directly through the skin into the kidney and uses ultrasound or electrohydrolysis to break the stone into pieces.
• This approach is usually used when stones are large and cannot be broken with lithotripsy.

DIET MODIFICATION
• Increase OFI 8 glass per day
• Limit salty food• Limit Calcium intake• Green Leafy
vegtables

Acid Ash Diet ( To acidify the urine)
Alkaline Ash Diet ( To alkalinize the urine)
Calcium Stonescranberry, prune juice,meat, egg, poultry,fish,grapes, whole grainslimit milk and other dairy products
Oxalate Stones milk, vegetables, fruits except prunes, cranberry, plumsAvoid tea, chocolate, rhubarb, spinach
Uric Acid Stones -
Reduce foods high in purine like liver, brain, kidneys, venison, shellfish, meat soup, gravies, legumes

NURSING CARE

NURSING MANAGEMENT1. Administer prescribed analgesics
2. Reassure client that most stones smaller than 4mm can pass out spontaneously
3. Provide education to prevent future and recurrence of stone
4. Encourage increase OFI
5. instruct client to avoid foods that contribute to the diagnosed type of stone
6. Instruct client to use OS when straining for urine with kidney stones fragment
7. Adhere to diet modification

NURSING DIAGNOSES

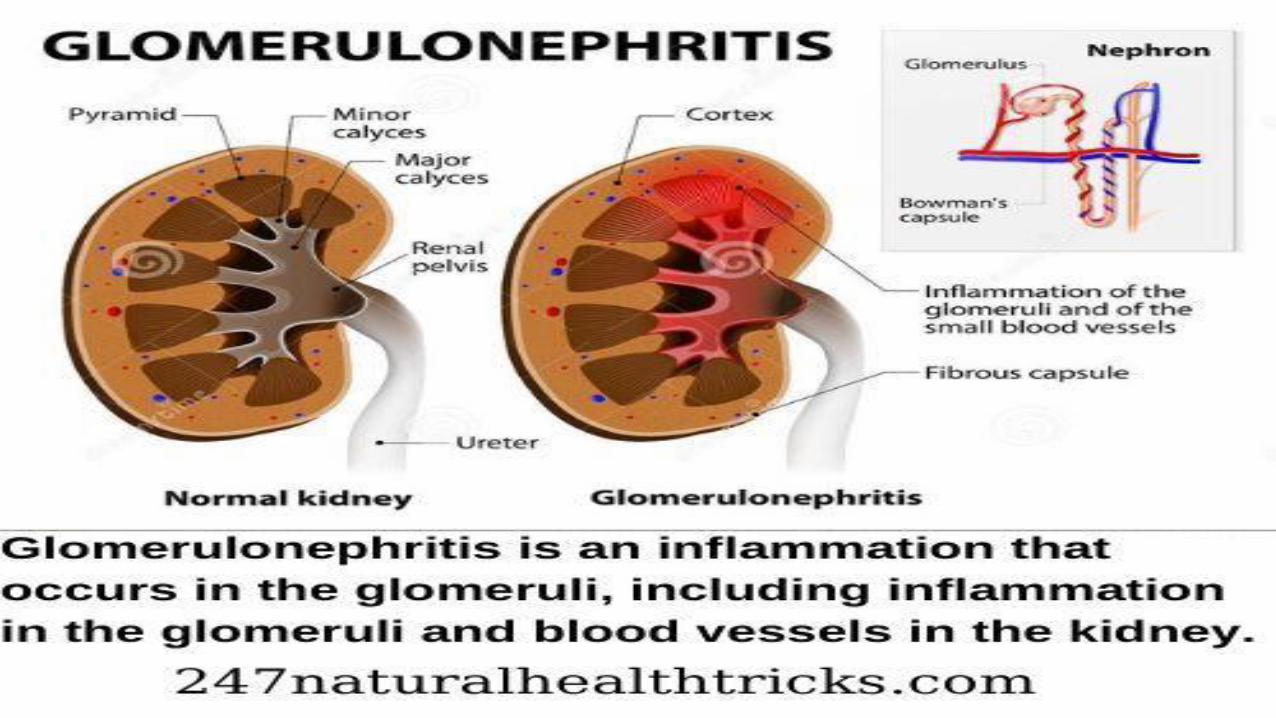
C. GLUMERULAR DISORDERS
• Nephrotic Syndrome - is an alteration of kidney function caused by increased glomerular basement membrane permeability to plasma protein (albumin).
• Altered glomerular permeability result in characteristic symptoms of gross proteinuria, generalized edema (anasarca), hypoalbuminemia, oliguria, and increased serum lipid level (hyperlipidemia).
• It maybe primary, wherein the pathology is the kidney itself or secondary of which nephrotic syndrome is the renal manifestation of a systemic disease .Nephrotic syndrome , usually occurs in children between ages 2-6 but may affect adults , both sexes and any race.






MEDICAL DIAGNOSIS
• Urinalysis, serum albumin, renal ultrasound and biopsy. Serologic studies for infection and immune abnormalities e.g. antinuclear antibody.
•


MEDICAL/PHARMACOLOGIC MANAGEMENT
• • Blood-pressure medications , ACE inhibitors and ARBs, which curb the pressure in the glomeruli and lower the amount of protein in the urine
• • Diuretics to reduce swelling
• • Cholesterol-lowering drugs
• • Blood thinners, or anticoagulants
• • Corticosteroids
• • Limit salt to reduce swelling and low in saturated fats and cholesterol diet.
• • Dialysis if conservative management is not effective .



NURSING CARE

NURSING MANAGEMENT
• 1. limit oral fluid intake, low sodium, protein and saturated food sources diet
• 2. I & O
• 3. Skin care
• 4. Reverse isolation, vit c rich diet
• 5. Monitor lymphocytes & wbc
• 6. Monitor complications ( pulmonary edema, hypertension, CHF, renal failure,stroke, )
• 7. Report fever, malaise & adverse effects of meds
•

NURSING DIAGNOSIS



NEUROGENIC BLADDER
• . Neurogenic Bladder - - urinary bladder malfunction due to neurologic dysfunction emanating from internal or external trauma, disease or injury.
• - Interference of the bladder normal mechanism cause by the disruption of the central and peripheral nervous system
Review of The Neuro Anatomy
• - The normal function of the urinary bladder is to store and expel urine in a coordinated, controlled fashion. This coordinated activity is regulated by the central and peripheral nervous systems. Normal voiding is essentially a spinal reflex , modulated by the central nervous system (brain and spinal cord), which coordinates function of the bladder and urethra.


PATHOPHYSIOLOGY• Normal bladder function relies on
information travelling through neural pathways from the cerebral cortex, through the spinal cord, and on to the bladder to coordinate normal micturition and urinary continence.
• When this pathway is damaged, it can result in loss of bladder sensation and also the loss of the coordination between urethral sphincter and its muscles,
• these muscles may not contract even when the bladder fills or the person has the urge to void, leading to bladder dysfunction such as urinary incontinence and retention (Mauk 2012).

TYPES OF NEUROGENIC BLADDER
A. Spastic- Sensory and voluntary control of urination is disrupted partially or totally. The stimuli generated by bladder filling cause frequent spontaneous detrusor muscle contraction and involuntary emptying caused by disruption of CNS transmission above the sacral spinal cord segment.
Causes:
1) Spinal cord injury- most common cause
2) Stroke
3) MS- immune mediated inflammatory disease attacking the myelin and axons
4) CNS lesions

TYPES OF NEUROGENIC BLADDERB. Flaccid- damage to the sacral spinal cord at the level of the reflex arc, cauda equina, sacral nerve roots leading to loss of detrusor muscle tone resulting to overdistention, weak and ineffective detrusor muscle contraction.
Causes:
1) Spinal shock phase (6-12 weeks)in SCI
2) Myelomeningocele or meningocele – type of neural tube birth defect wherein the backbone and spinal canal don’t close before the baby is born; a type of spinal bifida
3) Peripheral neuropathies- DM most common cause ,metabolic derangement of the Schwann cell results in segmental demyelination and impaired nerve conduction.
4) MS
5) Chronic alcoholism
6) Prolonged overdistention of the bladder

• Symptoms of Neurogenic Bladder
• Overactive bladder, frequent urination, stress incontinence.urge incontinence ,urinary retention, underactive bladder ( bladder cannot send signal when full)

DIAGNOSTIC TEST PURPOSE PROCEDURE NURSING RESPONSIBILITY1) Urine culture, Urianalysis Detect UTI Urine sample Midstream clean catch
1) Creatinine, BUN
* ascending infection, vesicoureteral reflux in neurogenic bladder can damage kidneys
Determine kidney damage Blood extraction Avoid meat
1) Postvoid bladder scan
*>50mL means ineffective detrusor muscle contraction Less than 50mL PVR is adequate bladder emptying
Over 200mL PVR indicates inadequate emptying
Children-20mL PVR is considered abnormal
Elderly-50-100 ml PVR is considered normal
Measures residual urine in the bladder shortly void;
this can be accomplished through ultrasound, bladder scan, or by directly measuring the urine volume drained by a urinary catheter. Urinary catheterization is the gold standard for measuring the post-void residual.
Explain the procedure
1) Cystometography To evaluate bladder filling and
detrusor muscle function
Shows the relationship of intravesical pressure with the changing volume of urine in the bladder
Double lumen catheter is inserted into the bladder, 50 ml is introduce in one lumen and pressure is recorded through the other lumen
∙ 10cms water for 50-400ml of urine
Explain the procedure
1) CYSTOSCOPY To determine presence of bladder lesions
Flexible cyctoscope inserted into the bladder , using also video system and irrigating medium
Explain procedure, local or GA maybe use,
Supine or lithotomy position

MEDICAL MANAGEMENT OF NEUROGENIC BLADDER
• GOAL: Maintain continence and avoid complication associated with overfilling or incomplete emptying of bladder through self-care. Thus, teaching is the primary intervention.
I. MEDICATIONS
GOAL:
• - increase or decrease contractility of detrusor muscle.
• - increase/decrease internal sphincter tone.
• - relax external urethral sphincter.

ANTICHOLINERGIC DRUG TO PREVENT SPASTIC BLADDER
CHOLINERGIC DRUGS TO STIMULATE MICTURITION
1. Darifenacim (Enablex)2. Oxybutynin (Ditropan )3. Solifenacin succinate (vesicare)4. Trospium (santural)5. Tolterodine (destrol)6. Propantheline bromide
(pro-bannthine)7. Flavoxate hcl (urispas)
*inhibits response to acetylcholine relaxing the detrusor muscle and increase sphincter tone*acetylcholine is a neurotransmitter causing muscle to contract,activate pain responses,regulates endocrine and REM sleep functions
1. bethanechol chloride (Urecholine)*stimulates parasympathetic NS increasing detrusor muscle tone producing contraction strong enough to produce micturition

III.BLADDER RETRAINING• Measures to stimulate reflex voiding for patients with spastic neurogenic bladder
• • Stroke or pinch abdomen, inner thigh, glans penis (trigger points to stimulate urination)
• • Pulling pubic hair
• • Tapping suprapubic region
• • Inserting gloved finger to rectum and gently stretch anal sphincter
• • Crede’s method- applying suprapubic pressure with finger of one or both hands
• ALERT: may stimulate SNS causing sudden increase of blood pressure for patients with SCI (autonomic dysreflexia -medical emergency )
• • Valsalva maneuver- bearing down while holding one’s breath
• CATHETERIZATION- intermittent for patients with SCI

SURGICAL MANAGEMENT
• Maybe required when urination can’t be effectively managed using conservative measures.
• 1)Rhizotomy- destruction of the nerve supply to the detrusor muscle or the external sphincter for patients with hyperreflexia or spasticity.
• 2)Urinary diversion-
• 3) Implantation of artificial sphincter


NURSING CARE

NURSING MANAGEMENT
1. Promote urinary drainage and continence
2. Prevent complication
3. Teach patient and family self-care techniques
4. Hydration rounds
5. Monitor I & O
6. Diaper, weight diaper
7. Change catheter twice a week
8. Preventive measure for infection




















