Urgent Care Improvement Board: 4 Hour Performance December ... · The graph to the right shows the...
13
Urgent Care Improvement Board: 4 Hour Performance December 2014
Transcript of Urgent Care Improvement Board: 4 Hour Performance December ... · The graph to the right shows the...

Urgent Care Improvement Board: 4 Hour Performance December 2014

Executive Summary
Improvement Trajectory
■ The target trajectory is to achieve between 81.8% and 93.3% for 2014/15 Q4; 88.4%
most likely. The trajectory has been refreshed to reflect December 2014 actual
performance and all types from April 2014. The most likely performance trajectory
outcome is January 85.45% , February 90% and March 90.3%.
■ Clarification and confirmation of SRG plans in line with the expected trajectory
improvements is required.
Key performance measures for the Trust are improving since the introduction of the
Urgent Care Improvement Programme, specifically during the 4 hour step up
improvement period.
Key issues and root causes
■ ED admission rate increased in month 38.6% (target 37.5%), reflection of the increased
patient acuity. Estimated that the rate would have been lower if Medical Assessment Unit Area
C (MAC) had been functional for the whole month, due to escalation preventing admission
avoidance and utilising alternative pathways.
■ Ambulance conveyance (+7% in FY14/15); weekly peak increase of 16.9% highest recorded
level
■ ED is performing well regarding time to treatment performance and patient feedback
■ Majority of 4 hour breaches remain attributable to bed availability (70.5%)
■ Impact of the community ORCP schemes during December, to be quantified and the response
to demand and DTOC increases inadequate.
Planning
■ The Trust is continuing to run its Urgent Care Improvement Programme
■ Key project for the 2014/15 Programme the development of both Medical and Surgical GP
direct admissions to the Medical and Surgical Assessment Units – operational 12th November.
Requires review following period of prolonged escalation and the use of this capacity due to
bed capacity demand – trolleys replaced with beds.
■ Medium term improvement to support delivery from November 2014, including sustaining all
urgent care schemes, delivery of GP expected pathways as direct admissions to both
Medicine and Surgery and the delivery of CCG Operational Resilience and Capacity plans
(ORCP). ECIST visit completed 17th December 2014 to review progress.
■ Final stage involves the implementation of a community wide urgent care strategy across the
four CCGs – learning from prolonged escalation and RCA in November 2014 requires SRG
leadership to lead outcome and recommendations.
■ Performance based upon no greater than 15 DTOC’s in total across all CCG’s.
Current Performance
■ December 4 hour performance was not achieved; 84.2% (All Types includes Urgent Care
Centre Activity)
■ Weekly red performance throughout December; Trust in prolonged Red escalation and
Black escalation from the 27th December 2014
■ Q3 4 hour performance not achieved ; 90.6%
Governance and Assurance
■ The RUH Urgent Care Improvement Board is responsible for the programme and
reports monthly to both Management Board and Board of Directors.
■ ECIST planned follow up site visit completed 17th December 2014; report awaited.
■ RUH to receive feedback from the Wiltshire CCG 100 Day Challenge at the 15th
January 2015 System Resilience Group. Urgent SRG focus required for Q4.
■ November BaNES RCA; specific focus on community response to demand, late
presentation and all providers to review ORCP schemes to ensure recued non
elective admission and contribution to 4 hour performance.

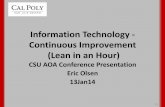
The graph to the right shows
the current trajectory.
RUH 4 hour step up
improvement plan commenced
8th September 2014 and stage 1
completed 31st October 2014.
Key action to continue to
review 4hr performance daily in
Stage 2, linking performance to
ongoing delivery of the Step up
plan operational actions.
Daily monitoring of the
Medically Expected and
Medical and Surgical Direct GP
admission pathways in place.
Ongoing metric review will
confirm that the actions taken
are supporting 4 hour Step up.
Reportable through the Urgent
Care Improvement Board.
Clarification and confirmation
of SRG ORCP plans and
delivery in line with the
expected trajectory
improvements is required.
Current Trajectory
Week
Ending
Actual
Performance
Standard
06/04/2014 86.0% 95%
13/04/2014 92.7% 95%
20/04/2014 97.7% 95%
27/04/2014 96.8% 95%
04/05/2014 95.4% 95%
11/05/2014 97.1% 95%
18/05/2014 97.0% 95%
25/05/2014 94.9% 95%
01/06/2014 94.6% 95%
08/06/2014 88.1% 95%
15/06/2014 90.2% 95%
22/06/2014 93.5% 95%
29/06/2014 96.1% 95%
06/07/2014 98.0% 95%
13/07/2014 96.7% 95%
Week Ending Actual
Performance
Standard
20/07/2014 94.7% 95%
27/07/2014 94.5% 95%
03/08/2014 96.3% 95%
10/08/2014 92.6% 95%
17/08/2014 89.0% 95%
24/08/2014 90.8% 95%
31/08/2014 87.5% 95%
07/09/2014 91.4% 95%
14/09/2014 94.9% 95%
21/09/2014 95.5% 95%
28/09/2014 96.9% 95%
05/10/2014 96.5% 95%
12/10/2014 90.9% 95%
19/10/2014 87.7% 95%
26/10/2014 95.8% 95%
Week Ending Actual
Performance
Standard
02/11/2014 95.7% 95%
09/11/2014 90.1% 95%
16/11/2014 93.0% 95%
23/11/2014 97.0% 95%
30/11/2014 96.1% 95%
07/12/2014 92.6% 95%
14/12/2014 82.0% 95%
21/12/2014 85.0% 95%
28/12/2014 84.1% 95%
04/01/2015 68.8% 95%

3
DRAFT FOR DISCUSSION PURPOSES ONLY Current Performance
84.2% of patients meeting the 4 hour
performance target in December 2014.
Stage 2 of the Step Up Improvement in
place. Focus on Medical Ambulatory
Care development (MAU Area C GP
expected admissions) and Surgical
Ambulatory Care extension of hours.
Services went live 12th November 2014,
and sustaining delivery up to and
including 15th December after which
due to escalation beds used the
functionality was lost.
NHS England Type 1 performance
benchmarking RUH ranked 70 of all
NHS Trusts. In December there were
no green weeks.
Diagnostic shows; reduced
performance due to the impact of
norovirus, increase in ambulance
activity, non-elective admission
increases, loss of direct admission
pathway changes due to the scale of
escalation required to manager
demand; and reduced community
response from the 16th December.
Performance could have been
improved by 5.3% if all ORCP schemes
delivered as per trajectory.
Key action to remain focused on de-
escalation, regaining direct admission
pathways, flow and back door. No
identified Emergency Department
Issues.
The Trust has not consistently met the 4 hour performance target
over the last 2 years, achieving 91.9% in FY12/13, 93.7% in
FY13/14 and is currently 93.0% FY 14/15 year to date.
4 hour performance has been achieved for 2 of the first 9 months of
the year (see table above). The Trust therefore identified the need
for a Step Up Improvement plan to further improve performance
which is overseen by the Urgent Care Improvement Board.
NHS England benchmarking for November 2014, the RUH ranked
70 of all NHS England Trusts, reduced by one place compared to
November 2014. Overall FY 14/15 year to date 1.3% above NHS
England FY 14/15 year to date compliance (improved compared to
last month).
Performance below expected national compliance and currently
below RUH trajectory. Performance could have been improved by
3.4% if all schemes delivered as per trajectory – RUH 3.1%,
BaNES 1.2%, Wiltshire 0.7% and Somerset 0.3%
Diagnostic: Compared to trajectory assumptions Green to Go and
DTOC patients increased from the 11th and 19th December
respectively contributing to a reduced back door flow and an
increase in patients with a LoS > 14 days. RUH bed capacity
reduced from the 2nd December to the 15th December due to wards
closed to new admissions, peaking at 25 empty beds on the 8th
December. For the whole of December there were 6 wards closed
for a total of 41 days; 13 confirmed cases, and 181 bed days lost.
In response twenty planned escalation beds opened from the 11th
December
2014/15 ED 4 Hour Performance (All Types)
in mitigation and the RUH lost the function of both medical and
surgical Area C’s from the 16th December due to the front door
demand for bed capacity (non elective admissions increased by
4.8%). Ambulance conveyance sustained daily increase from the 11th
December, peaking at 16.9% w/e 27th December and continuing to
rise into January, in line with South West reported activity levels and
unprecedented national demand for Emergency services preceding
and during the Christmas period. RUH reported overall admission to
discharge imbalance from the 15th and increasing towards and during
the Christmas period reducing the Trusts resilience to respond and
the opening of at its peak 93 escalation beds; early analysis
demonstrates that the community was under pressure with regard to
sufficient capacity and an inability to respond to reduce DTOC and
Green to Go. Medical and Surgical pathways changes for GP direct
admissions as per ORCP had a positive impact on performance and
GP direct admissions up to and including the 15th December., when it
ceased to provide additional bed capacity in escalation.
Conclusion: Performance deteriorated at the start of the month due
to the impact of norovirus, mitigated by opening of escalation
capacity. Increasing ambulance conveyance and non-elective
admissions from the 16th necessitated the opening of additional
escalation; however the community's capacity to respond from the
11th greatly reduced RUH resilience, and subsequent level of
escalation. Review of escalation required due to the significant
contribution of Medical Assessment Area C to 4 hour performance.
No identified issues with ED performance.
Financial Year Quarter Month Attendances 4 Hour Breaches Performance
April 6516 436 93.3%
May 7189 248 96.6%
June 7106 491 93.1%
July 7197 255 96.5%
August 6732 570 91.5%
September 6865 361 94.7%
October 7006 448 93.6%
November 6747 406 94.0%
December 6837 1081 84.2%
2014/2015
1
2
3

4
DRAFT FOR DISCUSSION PURPOSES ONLY Factors Contributing to Adverse Performance
Four Hour performance
affected in month by;
• Norovirus
• All planned and unplanned
escalation open
• Increased days lost to
DTOC
• Increased Green patients
• Unprecedented levels of
Ambulance activity
• Increased medical outliers
• Increased non-elective
admissions
Four hour performance is not adversely affected by a single factor but
a combination of factors including principally although not limited to the
following ;
•Number of Medical outlier days
•Average Adult Acute Beds Occupied
•Average Adult Length of stay
•Average Green Inpatients
•Number of adult discharges
Statistical analysis has shown that some of these factors have a
stronger impact on 4 hour performance than others. Monthly
performance analysis over time indicates that poor flow out of the
hospital and the consequences of this (such as increased number of
medical outliers and an overall increase in occupancy markers of
reduced flow) has the most significant impact on performance.
ED attendances . On average this financial year the Trust has seen a
3.2% increase in ED attendances compared to the same period last
year. In December however, activity was broadly in line with last
December (+0.8% or +45 patients).
Non-Elective Admissions. There has been a 4.6% rise in NEL
admissions (1200 patients to month 9). In December this trend
continued with a 4.8% increase on last December (+150 patients).
NHS BaNES variance from last year peaked in December at 14.1%
(average until November was 3%).
Ambulance activity. Overall ambulance conveyance (+7% in
FY14/15). From the 11th December the Trust experienced 3 weeks of
sustained high activity. This was in line with the South West
Ambulance Service Trust reported activity across the whole area and
National demand.
Green to Go. The number of Green inpatients started to rise on the
11th Dec (79) and by the 18th were at 122. Although this figure then
stabilised it remained at an average of 101 over the period. The
proportion of Green patients that were official DTOCs took a stepped
increase on the 19th December and remained at that level until 6th
January.
Non-Elective Length of Stay. For December there was no material change,
average of 6.6 days in line with previous months. The impact of acuity,
increased DTOC and Green to Go may not be seen until January
performance reporting as many of the long length of stay patients are still
active inpatients.
Delayed Transfer of Care (DTOC). Analysis of the number of ‘days lost to
DTOC’ shows that NHS BaNES and NHS Somerset levels peaked on the w/e
21st Dec having grown steadily for the preceding 4 weeks. NHS Wiltshire
however started to rise w/e 14th Dec and was still rising w/e 4th Jan. All CCGs
have historically had higher levels of days lost but all three experienced an
upward trend in the run-up to the Christmas period.
Bed Capacity. In response to the loss capacity due to norovirus, additional
complexity of patients and reduced flow at the back door, the Trust increased
its acute bed base by 20 beds on the 11th December and increased further on
the 27th (averaging total beds open 615 , peaking 630 on the 4th Jan).
Patient Flow. At the start of December, despite periods of red escalation and
high breach numbers, recovery flow was regained. However despite
increasing unplanned escalation beds to manage both demand and mitigate
bed closures due to norovirus on the 11th December and again on the 27th
due to demand alone flow was not regained. Four consecutive days of low
discharges 25-28 Dec added a final factor to reduced performance.
Medical Outliers. Throughout the month medical outliers have been
relatively constant at 25. The week following Christmas saw a stepped
increase in medical outliers (into the increased acute bed base) peaking to
100 from the 29th onwards.

5
DRAFT FOR DISCUSSION PURPOSES ONLY Ambulance Conveyance Review
Ambulance activity
increased by 7% compared
to FY 13/14
3 Weeks of sustained
activity in December;
peaking at a weekly
average increase of 16.9%
Weekend ambulance
activity continues to
demonstrate a marked
increase. Highest levels
compared to the last 5
years
Ambulance activity is a
marker of acuity, linked to
non-elective admission
increase
Analysis by South West
Ambulance Foundation
Trust required to
understand the source of
demand i.e. 999, 111 or
HCP
Ambulance conveyance rates in 2014/15 financial year have been
consistently above 2013/14 activity.
Overall ambulance conveyance (+7% in FY14/15).
From the 11th December the Trust experienced 3 weeks of
sustained high activity. This was in line with the South West
Ambulance Service Trust reported activity across the whole area
and National demand.
No data has been made available with regard to the proportion of
999, 111 or HCP arrivals and this is expected through the system
resilience groups as part of the review of this exceptional period.
When compared to the same period last year there have been
significant increases during this period; peaking at 16.9% ,the
highest recorded level.
Daily ambulance activity data is collected as part of the 4 hour
improvement step up scorecard and has been shown statistically to
link to 4 hour performance outcome. Whilst daily activity
increased specifically during three weeks of December it is also
important to note that activity continues to increase on Saturday
and Sunday; at its peak 100 ambulance arrivals on Sunday 7th
December. Ambulance conveyance is used as a marker of patient
acuity and this links to the increase in non-elective demand; 4.8%
increased compared to FY13/14. Without the step up of community
response the RUH resilience to manage the demand during these
peak periods is reduced.
The following chart shows the daily activity ED conveyance activity
throughout December, peaking over the Christmas period comparing
RUH (red ), GWH (blue) and Salisbury (green).
Period Last Year This year Variance % Variance
w/e 21st Dec 527 602 75 14.2%
w/e 28th Dec 499 582 83 16.6%
w/e 4th Jan 537 628 91 16.9%
The following chart shows the weekly activity profile of ambulance
conveyance comparing the last financial year and also the 5 year
profile. Activity in December is significantly higher than the last 5
financial years.

Overview:
The Trust has created a low and high range target reduction per
week based on their calculation of how many breaches each
scheme will save.
The majority of the reduction in Q3 relates to the Trust’s step up
plan which was planned to take partial effect in October and full
effect from 1st November 2014. The impact of this is a forecast
trajectory of between 97.3% and 99.7% in December 2014 which
was not delivered in month. December has not seen the impact of
the community schemes as anticipated in line with the ORCP to
reduce breaches as per the forecast trajectory.
Improvement Trajectory – 4 Hour Step Up Improvement Plan
The step up plan had three work
streams, front door, flow and
backdoor and twenty immediate
recovery actions were
identified.
Individual plans tracked using
the 4 Hour Step up Daily
Scorecard.
The trust anticipates that the
combined key actions will
reduce the number of breaches
in the Trust through a
combination of front door and
back door improvements.
The low range target is for a
reduction of 49 breaches a week
whilst the stretch target is for a
reduction of 105 breaches per
week.
The analysis shows that the
Trust will need internal and
external plans to deliver the
stretch target in order to
achieve the 4 hour standard in
both February and March 2015.
January performance has been
affected by the prolonged
period of Black escalation at the
end of December into January;
at the time of reporting it is not
possible to achieve the standard
for January.
RUH GP direct admissions to the Medical Assessment Unit only has
directly contributed the avoidance of 174 breaches in month (part
month effect due to prolonged escalation) which would have
improved 4 hour performance by 2.5%.
Further system wide plans are anticipated to take effect in time for
winter. The Trajectory shows that all schemes (excluding the UCC
counting) will need to achieve 60-70% of the stretch target to
maintain performance during February and March.
The target trajectory is to achieve between 95.0% and 95.4% for
Q4. The trajectory has been refreshed to reflect December 2014
actual performance and all types from April 2014.
Forecast Trajectory
Month Low Range Stretch Target
Apr-14 92.7% 92.7%
May-14 96.3% 96.3%
Jun-14 92.4% 92.4%
Jul-14 96.1% 96.1%
Aug-14 90.5% 90.5%
Sep-14 94.3% 94.3%
Oct-14 95.2% 96.3%
Nov-14 96.8% 98.7%
Dec-14 97.3% 99.7%
Jan-15 94.1% 97.5%
Feb-15 93.7% 96.8%
Mar-15 96.0% 99.5%
Impact on 4 hour wait performance
Month
RUH Sirona Wiltshire Somerset SWAST Dorothy House Primary Care UCC Total
Low High Low High Low High Low High Low High Low High Low High Low High Low High
Oct-14 1.1% 2.2% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 1.1% 2.2%
Nov-14 2.3% 4.4% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.5% 0.2% 2.8% 4.6%
Dec-14 2.2% 4.3% 0.5% 0.9% 0.0% 0.0% 0.0% 0.2% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.4% 0.0% 3.1% 5.5%
Jan-15 2.2% 4.3% 0.5% 0.9% 0.6% 1.5% 0.0% 0.2% 0.1% 0.2% 0.0% 0.1% 0.0% 0.1% 0.9% 0.4% 4.3% 7.6%
Feb-15 2.0% 3.9% 0.4% 0.8% 0.6% 1.4% 0.0% 0.2% 0.1% 0.2% 0.0% 0.1% 0.0% 0.1% 0.8% 0.4% 3.9% 7.0%
Mar-15 2.3% 4.4% 0.5% 0.9% 0.6% 1.6% 0.0% 0.2% 0.1% 0.2% 0.0% 0.1% 0.0% 0.1% 0.6% 0.1% 4.1% 7.6%

Appendix 1 December 2014 System Resilience Group Bath and North East Somerset CCG
4 Hour Improvement Trajectory
■ The RUH target trajectory is to achieve between 95.0% and 95.4% % for Q3. The
trajectory has been refreshed to reflect December 2014 actual performance and all
types from April 2014.
■ Clarification and confirmation of SRG plans in line with the expected trajectory
improvement of between 7 and 14 breaches avoided per week for BaNES CCG
SRG.
■ Total BaNES contribution to adverse 4 hour performance in December = 1.2%
Key issues and Root Causes
■ ED attendance has increased by 0.7% compared to 13/14
■ Non-elective ED admissions has increased by 14.2% compared to 13/14
■ Trust wide average numbers of Green to Go total 107 (BaNES daily average 36) and 165 >
14 days length of stay
■ Trust wide average number of complex discharge daily average 7
■ High level of delayed transfers of care (DTOC) – monthly snapshot 4.9%
Planning
■ The Trust is continuing to run its Urgent Care Improvement Programme
■ The Board initiated an improvement plan to regain performance through September
and October 2014, stage 1 evaluated
■ Medium term approach to support delivery from November 2014 in place, including
care system planning and the delivery of CCG Operational Resilience and Capacity
plans (ORCP)
■ Based upon no greater than 5 DTOC’s
■ Final stage involves the implementation of a community wide urgent care strategy
across the four CCGs supporting 4 hour position
Current Performance
■ December 4 hour performance was not achieved; 84.2% (All Types)
■ Year to date 4 hour performance has been achieved for 2 of the first 9 months
■ CCG contribution to adverse performance (all DTOC and complex patients) equivalent to
20 x 4 hour breaches = 0.3%
Governance and Assurance
■ BaNES CCG System Resilience Group (SRG) KPI monitoring
■ RUH Urgent Care Improvement Board and Management Board
■ Urgent Care Provider Forum Key Projects and overview of progress
Diagnostic Exception Reporting
■ Early analysis indicates increasing green and DTOC pressures building from the 16 th
December 2014.
Low Stretch
Step down beds x20↑ Discharge 3 3 Investment ORCP/Recruitment/Staffing
Night sitting service
Admission avoidance
↑Discharge
0 1 Recruitment
DN clinics at the weekend
↑ Discharge 0 1 Transport
Discharge at the weekend↑ Discharge 3 4 Investment ORCP/Recruitment/Staffing
IV Therapy↑ Discharge 1 2 Investment ORCP/Recruitment/Staffing
SWASFT Mobile rapid response/fallers Admission avoidance 0 1Investment ORCP/Recruitment/Staffing
Dorothy House Hospice at Home↑ Discharge
0 1Investment ORCP
Primary Care Extra GP Sessions
ED Attendance Avoidance
Admission avoidance 0 1
Investment ORCP/Recruitment/Staffing
Sirona
Scheme Potential Benefit Per Week Breach
Avoidance
Risks to Delivery

Appendix 2A December 2014 System Resilience Group Wiltshire CCG
4 Hour Improvement Trajectory
■ The RUH target trajectory is to achieve between 95.0% and 95.4% % for Q3. The
trajectory has been refreshed to reflect December 2014 actual performance and all
types from April 2014.
■ Clarification and confirmation of SRG plans in line with the expected trajectory
improvement of between 9 and 22 breaches avoided per week for Wiltshire CCG
SRG.
■ Total Wiltshire contribution to adverse 4 hour performance in December
0.7%
Key issues and Root Causes
■ ED attendance has decreased by 6.6% compared to 13/14
■ Non-elective ED admission decreased by -1.2% compared to 13/14
■ Trust wide average numbers of Green to Go total 107 (Wiltshire daily average 45)and
165 > 14 days length of stay
■ Trust wide average number of complex discharge daily average 7
■ High level of delayed transfers of care (DTOC) – monthly snapshot 6.7%
Planning
■ The Trust is continuing to run its Urgent Care Improvement Programme
■ The Board initiated an improvement plan to regain performance through September
and October 2014, stage 1 evaluated
■ Medium term approach to support delivery from November 2014, including care system
planning and the delivery of CCG Operational Resilience and Capacity plans (ORCP)
■ Final stage involves the implementation of a community wide urgent care strategy
across the four CCGs supporting 4 hour position
■ Based upon no greater than 5 DTOC’s
Current Performance
■ December 4 hour performance was not achieved; 84.2% (All Types)
■ Year to date 4 hour performance has been achieved for 2 of the first 9 months
■ CCG contribution to adverse performance (all DTOC and complex patients) equivalent
to 46 x 4 hour breaches = 0.7%
Governance and Assurance
■ Wiltshire CCG System Resilience Group (SRG) KPI monitoring
■ RUH Urgent Care Improvement Board and Management Board
Diagnostic Exception Reporting
■ RUH seeking feedback from 100 Day Challenge as drawing to a close
■ Early analysis of RCA indicates DTOC pressures at the beginning of the month,
continued from October
Low Stretch
Community Escalation CapaictyAdmission avoidance
?Discharge
1 3 Staff capacity
Overnight community support Admission avoidance 0 0 Recruitment
GWH community cluster teams Admission avoidance 1 3 Recruitment
Healthcare professional l ine Admission avoidance 0 0 None
Help to live at home brokerageAdmission avoidance
?Discharge
1 2 Care Home Capaicty
Step up and step down capacity ?Discharge 5 7 New model not tested
Simple point of access and rapid
response
Admission avoidance
?Discharge
1 3 None
Additional POC ? Discharge 0 1 Care Home Capaicty
Domicill iary Care Support ? Discharge 0 1 Staff capacity
Additional Hospital Social Care
Capacity
? Discharge 0 1 Staff capacity
Primary Care Nursing Home
Initiative Admission avoidance0 1 Primary Care Capacity
Wiltshire
Scheme Potential Benefit Per Week Breach
Avoidance
Risks to Delivery

9
DRAFT FOR DISCUSSION PURPOSES ONLY Appendix 2B Wiltshire CCG Factors Contributing to Adverse 4 Hour Performance
Social Care: Funded
packages of care have
reduced since Christmas
The number of intermediate
care clients has been
steadily increasing overall.
Long stays noted in the
period after Christmas
causing a reduction in
capacity and flow.
Social Care Packages have decreased since December 2014;
both help to live at home and care home packages. The chart
below show the activity throughout
The number of intermediate care clients has increased
throughout December 2014, however in the period after
Christmas long stays are noted; limiting capacity and flow.

Appendix 3 December 2014 System Resilience Group Somerset CCG
4 Hour Improvement Trajectory
■ The RUH target trajectory is to achieve between 95.0% and 95.4% % for Q3. The
trajectory has been refreshed to reflect December 2014 actual performance and all
types from April 2014.
■ Clarification and confirmation of SRG plans in line with the expected trajectory
improvement of between 1 and 5 breaches avoided per week.
■ Total Somerset contribution to adverse 4 hour performance in December =
0.3%
Key issues and Root Causes
■ ED attendance has decreased by 6.8% compared to 13/14
■ Non-elective ED admission decreased by 9.3% compared to 13/14
■ Trust wide average numbers of Green to Go total 107 (Somerset daily average 18)
and 165 > 14 days length of stay
■ High level of delayed transfers of care (DTOC) 5.2% monthly snapshot
Planning
■ The Trust is continuing to run its Urgent Care Improvement Programme
■ The Board initiated an improvement plan to regain performance through September
and October 2014, stage 1 evaluated
■ Medium term approach to support delivery from November 2014, including care system
planning and the delivery of CCG Operational Resilience and Capacity plans (ORCP)
■ Final stage involves the implementation of a community wide urgent care strategy
across the four CCGs supporting 4 hour position
■ Based upon no greater than 3 DTOC’s
Current Performance
■ December 4 hour performance was not achieved; 84.2% (All Types)
■ Year to date 4 hour performance has been achieved for 2 of the first 9 months
■ CCG contribution to adverse performance (all DTOC and complex patients) equivalent
to 10 x 4 hour breaches = 0.1%
Governance and Assurance
■ Somerset CCG System Resilience Group (SRG) KPI monitoring
■ RUH Urgent Care Improvement Board and Management Board
Diagnostic Exception Reporting
■ Early analysis indicates DTOC pressures increasing towards the end of the month
Low Stretch
Enchanced out of Hospital Care Admission avoidance 0 1 None
Home Care Packages ?Discharge 0 1 None
Crisis Support Night Sitting Admission avoidance 0 1 Recruitment
GP Weekend Response Admission avoidance 1 2 GP Capacity
Mental Health Admission avoidance 0 0 Recruitment
Somerset
SWASFT
Scheme Potential Benefit Per Week Breach
Avoidance
Risks to Delivery

Appendix 4 RUH Operational Resilience and Capacity Summary of Assurance December 2014
RUH Key Performance Indicators
Key issues and Root Causes
■ Non-emergency patient transport
Planning
■ The Trust is continuing to run its Urgent Care Improvement
Programme
■ The Board initiated an improvement plan to regain 4 hour
performance through September and October 2014. Stage 1
completed and reported.
■ Medium term approach to support delivery from November 2014,
including care system planning and the delivery of CCG Operational
Resilience and Capacity plans (ORCP)
■ Final stage involves the implementation of a community wide urgent
care strategy across the four CCGs
Current Performance
■ All RUH schemes on plan
Governance and Assurance
■ RUH Urgent Care Improvement Board and Management Board
■ BaNES and Wiltshire CCG formal contract review of NPTS (Arriva)
completed 1st December 2014
■ KPI’s for all community ORCP schemes required to determine
impact upon 4 hour trajectory – key action for all SRG’s
Core ORCP Funding - Summary of plan to achieve requirement
Provider
Estimated
Costs in
2014/15
BaNES
Agreed
ORCP
Funding
(41.3%)
Wiltshire
Agreed
ORCP
Funding
(44.3%)
Somerset
Agreed
ORCP
Funding
(14.4%)
KPI Oct-14 Nov-14 Dec-14 Comments
95% 4 Hour Performance
(all types) 93.6% 94.0% 84.2%
Step up improvement plan in place as per the RUH Urgent Care Programme
which has been extended to moniotr the Surgical and Medical Assessment
Areas and the management of GP expected patients.
Total Trust Wide Beds Open
(monthly daily average).
Plan to open 22
9 6 24 Monthly average escalation beds open
Increased radiology capacity CT/MRI/US to support ED, MAU,
SAU, ESAC and Medical Ambulatory Care.
£389,870 £161,016 £173,000 £0
% CT/MRI inpatient
requests completed in 24
hours (target 80%)
85.6% 87.9% 89.4%CT/MRI scans completed within 24 hours of request (inpatient); continuous
improvement demonstrated.
Scheme A: Weekend discharge registrar (10am to 6pm
Saturday and Sunday).
Scheme B: Acute Oncology. Increase the service to 7 days per
week -
Scheme A: Evening ward rounds Medical Assessment Unit.
Scheme B: Increasing Medical Ambulatory Care Capacity until
8pm Monday to Friday (Medical Assessment Unit Area C -
MAC)
Weekend and Evening
Consultant MAU Ward
Rounds average number of
patient reviews (target
average 6 patient reviews
per round)
N/A 14 6 November 2014 service implemented. Proceeding as planned.
% of Medical direct
admissions to MAU Area C
discharged on the same
day. Target 20% snapshot
N/A 32.10% 18.8%
November 2014 service implemented. Performance from the 16th December
2014 reduced due to the escalation status of the hopsital and the requirement
to use the assessment areas. Performance from 01/12/14 to 15/12/14 26.9%.
4 Hour Performance (all
types) Target 95%93.6% 94.0% 84.2% Step up improvement plan in place as part of Urgent Care programme
Total Trust Wide Beds Open
(month average). Plan to
open 10
N/A N/A 4Capital works commenced on plan. Beds open 15th December 2014 as
planned. Additional 6 beds to open as per plan 19th January 2015
Additional non-emergency patient transport to support
patient flow during periods of high discharges and if discharge
needs to be less than the 4 hour NSL and Arriva contracted
response times. Piloted in 2013/14 programme and very
successful with x2 crews. Plan to use x1 crew 11:00-20:00 day
seven days per week which will be managed by the RUH
transport lead who will maximise activity.
£49,500 £20,444 £0 £0 4 per day 32 40 49
Additional capacity to support discharge. Subject to ongoing audit (led by
RUH transport lead with BaNES CCG). Capacity limited by level of funding
received against original plan. Block booking of additional capacity in place at
the end of December continuing into January 2015.
£19,000 £0
£0
Flexible non-elective medical bed capacity. 12 beds have
been identified to be used during periods of escalation and 10
beds overnight
£1,191,051 £491,904 £264,000 £100,000
29
Number of Discharge
reviews reported via the
Discharge Registrar (target
24)
28
(revised figure from
November report
due to improved KPI
reporting)
47November 2014 start as per ORCP; October start in line with identified
operational requirement. Proceeding as planned.
£97,000 £0£219,623 £90,704
Additional capacity on core specialty wards to support flexible
capacity modeling. Detailed bed modeling has been
completed by the RUH BIU team, in addition to demand
predictions (based upon 5 year averages) supporting flexible
capacity during periods of highest demand. 4 beds to open
mid December 2014 and a further 6 by the end of December.
£102,124 £42,177 £45,000
£43,913 £18,136

12
DRAFT FOR DISCUSSION PURPOSES ONLY Appendix 5 December 2014 RUH Urgent Care Improvement Programme
Overall assessment of the Urgent Care
Programme in December is AMBER.
Front Door. Medical ambulatory care activity
increased in month, direct impact of MAC
from 12th November 2014; this would have
been higher if not in escalation.
Median wait to treatment target sustained.
Continued focus on Medical Ambulatory Care
development (MAU Area C GP expected
admissions) and Surgical Ambulatory Care
extension of hours. Specific reference to use
in escalation and the services role in
supporting front door activity
Introduction of MAC has lowered the post
post take ward round number to below target
(i.e. reduced MAU length of stay), increased
in escalation.
Flow. Sustained adult bed occupancy,
increased medical outliers. All markers of the
trust in escalation, increased ED admission
rate and increased acuity. All seen from the
11th December.
Backdoor. Adult non-elective LoS in line with
target. Non-elective geriatric LoS average
sustained.
Overall decrease in bed days lost due to
DTOC and complex discharges.
Remain focused on Flow and Back Door as no
identified Emergency Department Issues.
ECIST planned site visit completed on the 17th
December 2014 – MAC/SAU and Trauma
Pathway review. Excellent feedback received.
Overview: The Trust has not consistently met the 4 hour performance
target in 2014/15. The diagnostic of 4 hour performance focused on
the impact of norovirus, days lost to DTOC, increasing green patients,
unprecedented ambulance activity and the use of all planned and
unplanned escalation to manage the demand and mitigate against the
community's reduced response. Review of the Trust escalation is
required due to the significant contribution of Medical Assessment
Area C to 4 hour performance.
Front Door. Urgent Care Improvement Board to review the impact of
the Medical and Surgical Assessment Areas and GP direct admission
pathways on 4 hour performance. Conservative estimate that 174
breaches could have been avoided and patient flow supported if MAU
Area C was fully operational from the 16th December and not used in
escalation, would have contributed 2.5% to the 4 hour performance
position . No identified issues with ED performance.
Flow: Four additional POU beds on line mid December 2014 in line
with ORCP, 6 further beds to be opened 19th January 2015 on
schedule.
Backdoor Metrics: 2 of the 5 metrics are green. The impact of acuity,
increased DTOC and Green to Go on non-elective LoS may not be
seen until January data as many of the long length of stay patients are
still active inpatients. Expect most metrics to be red in January 2015.
.
2014/15 Urgent Care Programme Trust Metrics
Conclusion: Continued focus on Flow and Backdoor actions and
improvement as per the step up improvement evaluation
recommendations to the Board of directors in November. ECIST report
due mid January 2015 – actions will be reviewed at the January 2015
Urgent Care Improvement Board and will be reported to management
board in February. Excellent feedback given on the day, specifically
with regard to the success of the MAC implementation since the 7th
October 2014 ECIST visit.
Key Actions;
1) Ongoing review of the GP direct admission pathway to the Medical
Assessment Unit (MAU) Area C. KPI monitoring through UCIB in
place daily. Contribution to 4 hour performance significant and
therefore its role in trust escalation needs to be considered by the
Chief Operating Officer and Divisions (including SAU Area C).
2) 4 hour step up improvement scorecard integrating MAC and ESAC
performance measures in place.
3) RUH ORCP scheme implementation and KPI monitoring in place
4) Wiltshire CCG ED attendance audit and anticipatory care planning
to support ED attendance avoidance.
5) ECIST recommendations awaited and appropriate action plan
development.
6) Focus on “sustain” work streams.