Updates on Drug Reimbursement Model ...Total 169 289 3.7 10.6 31.3 10.0 New Drug Listing Time Course...
39
Director Hsueh Yung (Mary) Tai Division of Medical Review and Pharmaceutical Benefits National Health Insurance Administration, Taiwan Oct. 15, 2020 1 Updates on Drug Reimbursement Model of Taiwan’s NHI System
Transcript of Updates on Drug Reimbursement Model ...Total 169 289 3.7 10.6 31.3 10.0 New Drug Listing Time Course...

Director Hsueh Yung (Mary) TaiDivision of Medical Review and Pharmaceutical Benefits
National Health Insurance Administration, TaiwanOct. 15, 2020
1
Updates on Drug Reimbursement Model
of Taiwan’s NHI System

Outline
Pharmaceutical Reimbursement System and
Expenditure in Taiwan
Principles and Procedures of drug listing
Optimization of Reimbursement Model
Conclusion
2

Pharmaceutical Reimbursement System and
Expenditure in Taiwan
3

The insured
Co‐payment
Medical care providers
NHIA
supportive funding
Claim
Reimbursement
NHI ICcard
Premium
Medical service
The Framework of NHI
4

CoverageCompulsory enrollment for all citizens and legal residents
Administration Single‐payer system run by the government
Financing Premiums
Benefits Uniform package, copayment required
Providers About 93% of healthcare providers contracted with NHI
Payment Plural payment programs under the global budget payment systems
Privileges Premium subsidies and copayment waivers for the disadvantaged
5
NHI Characteristics

Catastrophic disease Chronic disease (OPD) Others
Year Expenditure(million)
Growth rate % Expenditure
(million) Growth rate % Expenditure
(million) Growth rate %
2012 1,403 6.0% 30.7% 2,197 ‐2.9% 48.0% 977 ‐2.6% 21.4%
2013 1,529 8.9% 30.8% 2,442 11.2% 49.1% 1,000 2.2% 20.1%
2014 1,590 4.1% 30.7% 2,571 5.3% 49.6% 1,023 2.3% 19.7%
2015 1,632 2.5% 31.2% 2,597 1.0% 49.6% 1,006 ‐1.2% 19.3%
2016 1,735 6.4% 31.6% 2,713 4.5% 49.4% 1,045 3.7% 19.0%
2017 1,877 8.2% 31.7% 2,977 9.7% 50.3% 1,065 2.0% 18.0%
2018 2,032 8.2% 32.2% 3,187 7.0% 50.5% 1,094 2.5% 17.3%
2019 2,142 5.4% 31.9% 3,442 8.0% 51.2% 1,132 3.6% 16.9%
1. OPD chronic disease medications contribute to half of total drug expenditure . Medications used for catastrophic diseases contribute to around 30% of total drug expenditure.
2. The expenditure on OPD chronic disease medications shows higher growth rate.
6
Factors Contribute to the Growth of Drug Expenditure

ATC category Percentage
L Antineoplastic and immunomodulating agents 22%J Antiinfectives for systemic use 16%C Cardiovascular system 15%A Alimentary tract and metabolism 14%N Nervous system 10%B Blood and blood forming organs 9%R Respiratory system 4%M Musculo‐skeletal system 3%G Genito urinary system and sex hormones 2%S Sensory organs 2%
H Systemic hormonal preparations, excl. sex hormones and insulins 1%
D Dermatologicals 1%V Various 1%P Antiparasitic products, insecticides and repellents 0%
Total 100% 7
Distribution of Expenditure by Category of Drugs

Principles and Procedures of Drug Listing
8

Pay for Value
Health Technology Assessment
(HTA)
Health Technology Assessment
(HTA)
Subjects Subjects
ComparatorsComparators
Relative effectiveness
Relative effectiveness
CBA/CEA/PE
CBA/CEA/PE
Budget impactBudget impact
Ethical/legal/social/political
impact
Ethical/legal/social/political
impact
9

Classification of Drugs Listed
Drugs submitted for listing
• New active ingredient(s)• New dosage form• New route of
administration• Combined preparation
with new effect
Originators BA/BE
generics Common
generics
N
Y
Category 1 new drugs
Category 2 new drugs (2A, 2B)
New items
New drugs
Biosimilars
10
N

composed of stakeholders to ensure decision making for drug listing and reimbursement
Healthcare Providers
Scholars and Experts
13
The Insured
Employers
Health Regulatory Authority (MoHW)
Drug Regulatory Authority (TFDA)
93
31
1
11
The Suppliers 3
PBRS Joint Meeting
2Patients

Category Pricing Mark‐ups
1 Breakthrough Median price of A‐10 countries • domestic clinical trials (10%)
• domestic pharmaco‐economic study (up to 10%)
• better therapeutic effects (up to 15%)
• greater safety (up to 15%)• more convenient (up to
15%)• pediatric preparations with
clinical implications (up to 15%)
2A Me‐better
Capped at A‐10 median price• lowest price in A10• price in original country• international price ratio• treatment‐course dosage
ratio• a combination drug is priced
at 70% of the sum of each ingredient’s price, or at the price of the single active ingredient.
2B Me‐too
12
A‐10 reference countries:Australia, Belgium, Canada, France, Germany, Japan, Sweden, Switzerland, US, UK.
Pricing of New Drug (1)

13
Pricing of New Drug (2)
A new drug that demonstrates significant clinical value and is first introduced in Taiwan among the world
Based on actual transaction price
Cost calculation method
The listing prices of A‐10 countries of the new drug and its comparators

14
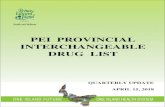
Year of listing
No. of cases
No. of items
Minimum(month)
Average(month)
Maximum (month)
Median(month)
2013 19 26 4.2 7.8 12.9 7.7
2014 23 45 4.0 8.4 14.9 7.9
2015 22 40 6.3 11.5 22.0 10.0
2016 17 26 7.3 11.3 21.1 10.4
2017 29 50 7.3 12.0 31.3 8.9
2018 26 51 7.3 11.7 28.2 10.2
2019 33 51 3.7 11.5 19.1 10.6
Total 169 289 3.7 10.6 31.3 10.0
New Drug Listing Time Course (from submission to listing)

• Drug suppliers disagree with the pricing results, resubmit, or submit additional documents
• Uncertainty in efficacy/ cost‐benefits
• Limited improvement in efficacy or similar in value compared to existing therapy, but more expensive
• High‐expenditure innovative drugs with huge budget impact
15
Interfering Factors of Pricing Process

Principle of Pricing Generics and Biosimilars
16
100Originators
BA/BE generics
Common generics
90
80
Capped at 80% of the lowest price of the listed originators.
Capped at 90% of the lowest price of the listed originators.
85Biosimilars Capped at 85% of the lowest price of the listed originators.

Pricing Process for Generics and Biosimilars
17
Submission NHIA Preliminary Pricing Results
PBRS Joint Meeting Listing

Optimization of Reimbursement Model
18

19
Current Challenges
Aging population
Escalating cost of new
drugs(e.g. IO, cell/gene
therapy)
Limited NHI resources vs. unlimited medical needs
Uncertainties in clinical efficacy of new drugs
(e.g. due to fast tract approval)

20
How to cope with Uncertainties(1)
Uncertainties in CostMEA
Good Submission Practice (GSP)/ co‐dependent
test
Horizon Scanning The Submission Principles for
High Expenditure Cancer New
Drugs
Mandatory PE study for high
expenditure new cancer drugs (start
from 2020)

21
How to cope with uncertainties (2)
Clinical uncertainties
Biomarkers
Registry(RWE)
Refined HTA(HTR)

22
I. Managed Entry AgreementII. Good Submission PracticeIII. Horizon ScanningIV. Improve Treatment Outcome through BiomarkersV. Utilization of Real World EvidenceVI. Refined HTA
Optimization of Reimbursement Model

I. MEAs Models in Taiwan
Category Mechanism of MEAs Models
1. Performance‐based 1. Ensure the improvement in overall survival
2. Ensure the progression‐free survival
3. Refund / payback based on response rate etc.
2. Financial‐based 1. Fixed‐rate refund / payback
2. Free doses
3. Payback for co‐prescribed drugs
3. Mutual share by negotiation
Mutual share of refund / payback among pharmaceutical products with the same ingredient or pharmacological category.
• Any one (or more than one) of the models be chosen on a case by case basis.
• Mutual share of drug expenditure between the supplier and the insurer via refund/ payback.
23

24
Specify the dossier required for submissionCreate a check‐list for submission dossier and MEA proposal
Create a self‐assessment sheet for cost‐benefit analysis
II. Good Submission Practice (GSP)
Improve the completeness and quality of submission dossier
Accelerate pricing review process

HS
Clinical trial
Register for market approval
Submit for Listing
Enter market
R&D
Listing
Horizon Scanning HTA
III. Horizon Scanning (1)

20212020
26
III. Horizon Scanning (2)
The end of Nov.
Deadline for HS registration
2022 2023
Reference for estimating the budget for 2022
Datacollected
(Pilot program)
• New drug • New reimbursed indication
1st yr 2st yr
1st yr

27
Platform for Registration for Horizon Scanning

28
Platform for Registration for Horizon Scanning‐New Drug

29
Platform for Registration for Horizon Scanning‐New Indication

IV. Improve Treatment Outcome through Biomarkers (1)
Identification of biomarkers
Improved patient outcomes
Patient sample
+ + =
Identify Patient
Right Treatment
Patient Benefit
Diagnostic test results inform treatment
decision
30
Ex: Examination of PD-L1 expression prior to the treatment with cancer immuno-therapies

31
Submission of co‐dependent technology• Co‐dependent: two related technology (ex:
gene examination to be done before the use of medication)
• If the reimbursement of a new drug may give rise to additional expenditure on a technology that is not yet covered by NHI, the technology shall be submitted for listing at the same time.
IV. Improve Treatment Outcome through Biomarkers (2)

Registry
RWE utilization
Renew reimbursement
32
V. Utilization of Real World Evidence

Registry System for Cancer Immuno‐therapies (1)
33
Type of Cancer No. of Patient
Melanoma 206
Lung cancer 716
Lymphoma 18
Urothelial carcinoma 322
Head and Neck Cancer 457
Gastric Cancer 253
Hepatocellular carcinoma 453
Renal cell carcinoma 158
Merkel cell carcinoma 3
Total 2586
As of Sep. 29, 2020

Registry System for Cancer Immuno‐therapies (2)
– To evaluate the value of cancer immuno‐therapies and to regularly review their reimbursement restrictions, NHIA has established a registry system for these medicines to collect data including:– Type and stage of cancer– Results of genetic examinations (ex: EGFR/ALK wild type)– Results of biomarker examinations– Treatment outcomes– Severe side effects– Reasons for treatment withdrawal
34

VI. Refined HTA
35
• Assess new drugs and expansion of indication
• Evaluate risk sharing scheme
• Re‐assess the reimbursement efficiency of listed medical products
(TFDA) (NHIA)
Strike a balance between new drug accessibility and affordabilityHorizon scanning

Conclusion
36

Allocate global budget/new drug budget vianegotiation
Allocate global budget/new drug budget vianegotiation
How to allocate resources to deal with emerging pricey new drugs
How to allocate resources to deal with emerging pricey new drugs
Consider cost vs. benefit while making choices
Consider cost vs. benefit while making choices
Effective
Not effective
Global budget
New drug budget
37
Conclusion

38
4‐Win Situation
NHIA Patients
Medical Care Providers Industry
Pay for Value

THANK YOU FOR YOUR ATTENTION
39