Updates in management of multiple myeloma Mohamed ... · Updates in management of multiple myeloma...
100
Updates in management of multiple myeloma Mohamed Abdelmooti 12.2014
Transcript of Updates in management of multiple myeloma Mohamed ... · Updates in management of multiple myeloma...

Updates in management of multiple myeloma
Mohamed Abdelmooti 12.2014

Management of multiple myeloma
1. Management of transplant-eligible patients
2. Management of transplant-ineligible patients
3. Complications of MM and their management

Criteria for Diagnosis of symptomatic MM*: International Myeloma Workshop Consensus Panel (2011):
1. Clonal bone marrow plasma cells ≥10% 2. Presence of serum and/or urinary monoclonal protein:
Ig G > 3.5 g / dl.; Ig A > 2 g / dl.; or BJP > 1 g / 24 hr urine. (except in patients with non-secretory MM†)
3. ≥1 CRAB features of end-organ damage: • C: Calcium elevation (>11.5 mg/L)
• R: Renal dysfunction (serum creatinine > 2 mg/dL)
• A: Anemia (Hb < 10 g/dL)
• B: Bone disease (lytic lesions, osteoporosis, fractures)
*All 3 criteria must be met. † ≥10% clonal plasma cells are required for the diagnosis of non-secretory MM.

What are factors that determine high-risk disease?
Disease-‐specific factors
• ISS stage (B2M & albumin)
• Extramedullary disease
• Plasma cell leukemia
• LDH • High prolifera>on rate • Plasma labelling index
• Cytogene>c abnormali>es
Pa>ent-‐specific factors
• Age • Co-‐morbidi>es, e.g. renal failure, spinal cord compression
ISS: Interna5onal Staging System
• t(4;14) • t(14;16) • del17p • 1q gain

Response: IMWG uniform Criteria (2011)
sCR CR VGPR PR
SPEP Nega5ve Nega5ve Nega5ve Posi5ve
IF Nega5ve Nega5ve Posi5ve Posi5ve
sFLC ra5o Normal Abnormal Abnormal >50% decrease
Serum M-‐protein
Nega5ve
Nega5ve ︎ >90% reduc5on
>50% reduc5on
24-‐hr urinary M-‐protein
Nega5ve
Nega5ve ︎<100 mg <100 mg <200 mg
PCs in BM
• <5% • No clonal PCs by IHC
<5%
<5%
>50% reduc5on
ST PCM Disappearance Disappearance Disappearance >50% reduc5on

Assessment of MRD: • Immunophenotypic CR (by multiparametric flow
cytometry >4 colors) • Molecular CR (by ASO*-PCR): (Sensitivity 10-4 - 10-6)
•
Rajkumar et al, Blood 2011, 117 (18): 4691-5
Response outside BM (Imaging techniques): • MRI: number of persisting focal lesions. • PET-CT: negativity
• *Allele-specific oligonucleotides


Association between depth of response and outcome
1. >VGPR is better than <VGPR (PFS) 2. CR is better than <CR (in transplant setting and in
elderly) (PFS and OS) 3. Sustained CR is important (OS) 4. MRD- is better than MRD+ (PFS and OS) 5. Number of focal lesions in whole-body MRI after
ASCT had significant impact on OS 6. PET-CR after ASCT conferred superior PFS and OS
1. Moreau et al. Blood 2011;117:3041-‐4 2. Mar6nez-‐lopez et al. Blood; 118(3):529-‐534; 3. Gay F et al. Blood;117:3025-‐31. 4. Barlogie et al. Cancer 2008;113(2):355–359 5. Paiva et al; Blood. 2008, 112: 4017-‐4023; 6. López-‐Pérez et al . Leukemia 2000 7. Hillengass et al. ASH 2011 (Abstract 1812) 8 Zamagni et al. ASH 2011 (Abstract 826)

Front-‐line therapy of mul>ple myeloma

Criteria to start treatment
1. Patients with asymptomatic MM:
Immediate chemotherapy does not offer any survival benefit over that provided by delayed chemotherapy, as convincingly demonstrated by several controlled studies and confirmed by a recent meta-analysis pooling the results of these trials
2. Treatment must be started immediately in patients with MM and related organ damage [I, A].
ESMO Minimum Clinical Recommendations, 2005 Kyle, et al, NEJM, 2004

Front-‐line therapy of mul>ple myeloma
I. Transplant-‐eligible Pa>ents

Management of Newly Diagnosed Myeloma
Every newly diagnosed myeloma pa5ent should be assessed for fitness to undergo ASCT: 1. Age < 60–65 years: not the only factor 2. Good performance status 3. Adequate organ func5on 4. No significant comorbidi5es.
Kaushansky et al, William’s Hematology (2010)
Combina>ons that include alkyla>ng agents (esp. melphalan) should be avoided à damage to normal HSCs à impossible to collect stem cells for ASCT

Treatment paradigm for pa>ents who are eligible for autotransplanta>on (ASCT)

Induc5on Therapy
Role: Reduc5on of tumor burden prior to ASCT

Induc5on Therapy VAD: Q4w « Vincris5ne: 0.4 mg iv over 4-‐24 hr qd d1-‐4 « Adriamycin: 9 mg/m2 iv over 4-‐24 hr qd d1-‐4 « Dexamethasone : 40 mg IV (or PO) qd d1-‐4, 9-‐12, 17-‐20
• Has been the standard induc5on regimen for many years • However, it achieve a CR rate of only 5-‐10% with >VGPR rate of 18-‐44%
• The need for admission, CVL, alopecia. • Has been replaced by novel drugs à beder CR rates pre-‐transplant
Reece, Hematology (2005)

Ludwig et al. Oncologist 2011;16(4): 388-‐403
+ DEXA
+ Adria or CPA
+ CPA
T R V VT or VR
POM-‐d POM-‐V
POM: Pomalidomide
POMCyD
Biaxin [clarithromycin]

Thalidomide-‐Based Induc5on regimens:
Regimen Drugs Response before ASCT
Median Survival
VS VAD
CR >VGPR PFS OS
Thal/dex (TD) q4w
• Thalidomide: 100-‐200 mg po qd • Dexamethasone: 40 mg po qd d1-‐4, 9-‐12, 17-‐20 for odd cycles and d1-‐4 only for even cycles
14% 31% 47 m 65% (5y)
NA
CTD q4w
• Cyclophosphamide: 500 mg/w • Thalidomide: 50 à 200 mg/d • Dexamethasone: 20 mg/day on days 1 to 4 and 15 to 18
13% 43% 26 m 72 m • Beder RR • Similar PFS • Similar OS
TAD q4w
• Thalidomide: 200 mg orally, days 1 to 28
• Adriamycin: 9 mg/m2 IV d 1-‐4 • Dexamethasone: 40 mg on d1-‐4
3% 37% 34 m 73 m • Beder >VGPR • Beder PFS • Similar OS

Lenalidomide-‐Based Induc5on regimens:
Regimen Drugs Response before ASCT
Survival
CR >VGPR OS
RD q4w
• Revlimid: 25 mg po qd d1-‐21 • Dexamethasone (HD): 40 mg d 1-‐4, 9-‐12, and 17-‐20
5% 50% 87% (1y)
Rd q4w
• Revlimid: 25 mg po qd d1-‐21 • dexamethasone (LD): 40mg/w
4% 40% 96% (1y)
RAD q4w
• Revlimid: 25 mg on days 1-‐21 • Adriamycin: 9 mg/m2 IV days 1-‐4 • Dexamethasone: 40 mg on days 1-‐4 and 17-‐20
13% 52% NA
Not Vs conven>onal therapy
(p=0.0002) (p=0.04
Rajkumar et al, Lancet Oncol., 2010.

Bortezomib-‐Based Induc5on regimens:
Regimen Drugs Response before ASCT
Median Survival
VS VAD
CR >VGPR PFS OS
Vel/dex Q3w
• Velcade: 1.3 mg/m2 iv d1, 4, 8 and 11
• Dexamethasone: 40 mg po d1, 4, 8 and 11
15% 38% 36 m 81% (3y)
• Beder RR • Beder PFS • Similar OS
PAD Q3w
• Bortezomib: 1.3 mg/m2 iv bolus d1, 4, 8, 11
• Adriamycin: 4.5-‐9 mg/m2 iv d1-‐4 • Dexamethasone: 40 mg po d1-‐4, 8-‐11, 15-‐18 of cycle 1 then d1-‐4 of cycles 2-‐4
11% 42% 36 m Not reached
• Beder RR • Beder PFS • Beder OS
VCD Q3w
• Velcade: 1.3 mg/m2 iv d1, 4, 8, 11 • Cyclophosphamide: 500 mg/m2/day IV on d1, 8, and 15
• Dexamethasone: 40 mg d1,4, 8,15
15% 37% NR NR • NR
• Bortezomib-based induction regimens highly effective. • Bortezomib/dex: could be considered as a backbone for induction
therapy before autologous transplantation.

Bortezomib + IMiD-‐Based Induc5on regimens (triplet regimens): VS DOUBLET Regimens
Regimen Drugs Response before ASCT
Survival VS Doublet regimens
CR >VGPR PFS OS
VTD Q3w
• Velcade: 1.3 mg/m2 iv d1, 4, 8 and 11
• Thalidomide: 100-‐200 mg/d. • Dexamethasone: 40 mg daily on 8 of the first 12 days.
19% 62% 68%m (3y)
86% (3y)
VS TD: • Beder RR • Beder PFS • Similar OS
vtD • velcade: 0.8-‐1 mg/m2 iv d1, 4, 8 and 11
• thalidomide: 50 mg/d. • Dexamethasone: 20 mg po d1, 4, 8 and 11
13% 49% NR NR VS VD: • Beder RR
VRD • Velcade: 1.0 or 1.3 mg/m2 d1, 4, 8, 11.
• Revlimid: 15 to 25 mg d1-‐14. • Dexamethasone: 40 or 20 mg d1, 2, 4, 5, 8, 9, 11, 12.
29% 67% 75% (1.5y)
97% (1.5y)
• NR
H i g h e s t 3-drug regimens are superior to 2-drug regimens

Four-‐drug Induc5on regimens:
Regimen Drugs Results
VTDC Q3w
• Velcade: 1.3 mg/m2 d1, 4, 8, 11. • Thalidomide: 100 mg daily d1-‐21 • Dexamethasone: 40 mg/d on days 1-‐4 and 9-‐12 • Cyclophosphamide: 400 mg/m2 IV on days 1 and 8
• CR 31% • OR 96% • Increased G3/4 toxici5es
RVCD Q3w (EVOLUTION)
• Revlimid: 15 mg/day D1-‐14 • Velcade: 1.3 mg/m2 d1, 4, 8, 11. • Cyclophosphamide: 100–500 mg/m2 D1 and 8 • Dexamethasone: 40 mg D1, 8, 15.
• CR 36% • >VGPR 68%
Ludwig, JCO, (2012) Kumar S, et al. Blood. 2008;112: [abstract 93].
4-drug induction regimens are not superior to three-drug combinations due to higher toxicities.


ASCT in MM

ASCT for MM
Four prospective randomized European studies have established that auto-HSCT confers superior overall survival and/or event-free survival when compared to standard chemotherapy therapy.
Atta eta al, NEJM (1996) Child et al, NEJM (2003); Palumbo et al, Blood (2004) Farmland et al, JCO (2005)


International Myeloma Foundation (IMF) (Evidence-based…2011/2012):
ASCT as planned part of “frontline therapy”: Recommendations:
1. ASCT is strongly considered in “front-line therapy for MM” à improved RRs (CR>90%) and OS with TRM <5%
2. Standard conditioning regimen is Melphalan 200 mg/m2 (NO TBI)
3. Stem cell purging… NOT recommended 4. PBSCs > BM: easy & rapid. 5. Pre-ASCT induction: Thal/Dex, Vel/Dex, VTD, Len/dex. 6. Planned tandem ASCT: Only if did NOT attain at least
VGPR after 1st SCT, otherwise investigational!

Allogeneic SCT for Multiple Myeloma
1. RIC Allo-SCT: Current data do not its universal use for myeloma and attention needs to be paid to RIC strategies including:
• Conditioning • Auto à RIC • Immunosuppression • Role of DLI. • Integration of Novel Drugs in RIC-Allo programs
2. MAC Allo-SCT should not be considered standard treatment, and should only be considered in selected population of patients in the context of a clinical trial.


Aims of consolida>on or maintenance therapy aeer ASCT
Consolida>on: • Improve response/induce deeper response following therapy
• By administra5on of treatment for a limited period
Maintenance: • Maintain response achieved following therapy
• By administra5on of treatment for a prolonged period Reduce the risk
Reduce the risk of relapse Extend PFS and OS

Consolidation: (V/VTD/VRD)
• To be considered for pts who do not achieve >VGPR after ASCT.
• Leads to improvement in depth of response • PFS is improved with VTD or V consolidation.

Maintenance:
Thalidomide Lenalidomide Bortezomib Dose 100 mg daily PO 10 mg daily PO for
21 days every month 1.3 mg/m2 either: • Every 2 weeks or • On days 1, 4, 8, 11 every 3 months
Dura>on for at least 1 y Till progression 2-‐3 years
PFS improvement In 7/8 trials In 3/3 trials In 2/2 trials
OS improvement In 2/8 trials In 2/3 trials In 1 trial
Risk categories In standard-‐risk only
Work in “all risk” groups
Work in “all risk” groups
Tolerance Low: PN & #QoL • Beler tolerated • ++ SPM (2/3 trials)
Beler tolerated

Front-‐line therapy of mul>ple myeloma
(II) Transplant-‐ineligible Pa>ents

Management of Newly Diagnosed Myeloma
Transplant-‐ineligible Pa>ents: 1. Age > 60–65 years: not the only factor 2. Poor performance status 3. Inadequate organ func5on 4. Significant comorbidi5es
Kaushansky et al, William’s Hematology (2010)
Goal of therapy: Palliative
Age and organ damage correlate with poor OS

Front-‐line treatment of MM (II) Non-‐transplant sejng: Induc>on
Q Melphalan Prednisone Thalidomide Velcade Revlimid Vs MP
MP 4w 8-‐10 mg/d PO for 7 ds
60 mg/d po for 7 days
-‐-‐ -‐-‐
-‐-‐
NA
MPT 4w
4 mg/m2/d po for 7 ds
40 mg/m2/d po for 7 ds
100 mg/d po 5ll disease progression
-‐-‐ -‐-‐ • Beder RR and PFS (5/5) • Beder OS (2/5 trials) • 6.6-‐month OS benefit
VMP 6w 9 mg/m2d po for 4 ds
60 mg/m2/d po for 4 ds
-‐-‐ 1.3 mg/m2 iv d1, 4, 8, 11, 22, 25, 29, 32
-‐-‐
• Beder PFS. • Beder OS. • 13.3-‐month OS benefit
MPR-‐R 4w 0.18 mg/kg po for 4 ds
2 mg/kg/d po for 4 ds
-‐-‐
10 mg/d po for 21 ds Q4w un5l disease progression.
• Beder PFS • Same 4y OS
These data lend support to the use of MPT (or VMP) as the standard of care in elderly MM

T VT R
Study MPT + T (3 studies)
• VMPT-‐VT Vs VMP • VMP Vs VTP à VT VS VP maintenance
MP vs MPR vs MPR-‐R maintenance
PFS Improved in 2/3 Improved in 1/2 Improved
OS Improved in 1/3 Improved in 1/2 Small OS benefit esp. in >65 yr.
AEs Higher rate of G 3-‐4 PN Increased SPM
Front-‐line treatment of MM (II) Non-‐transplant sejng: Maintenance

In Maintenance
X2
Summary/Conclusions:

Elderly pa5ents: Op5mizing treatment tolerability through modified treatment schedules

Considera>ons when trea>ng elderly pa>ents: • Decrease in func5onal capacity: PS, ac5vi5es of daily living, cogni5ve func5on
• Comorbidity (renal, pulmonary, hepa5c, cardiac, bone marrow insufficiency, polyneuropathy)
• Disability and Frailty (weakness, poor endurance, weight loss, low physical ac5vity, slow gait speed)
• Increased prevalence of unfavorable prognos5c factors (B2M>3.5 ug/mL, albumin <3.5 g/dL, Hb < 10 g/dL, ISS stage III)1
• Polypharmacy (?drug interac5ons) • Decreased capacity to tolerate toxicity:
― Increased rates of therapy discon5nua5on ― Decreased Cumula5ve dose intensity
1Ludwig et al. J Clin Oncol 2010;28(9):1599-‐605
2Ludwig et al. Blood 2009;113(15):3435-‐42

Strategies to improve the tolerability of treatment:
• Changing treatment schedules
–Reduc5on in frequency of dosing (e.g. weekly bortezomib) à reduced PN.
–Reduc5on in drug dosage: (THAL100, LEN15, v1 in vtD)
• Changing the route of administra5on
– e.g. SC bortezomib à reduced PN.



Relapsed/Refractory Myeloma
Management of Mul5ple Myeloma (Cont.)

Patterns of relapse in myeloma
Biochemical Symptomatic M-component Increased Increased Symptoms Asymptomatic Symptomatic CRAB Criteria Absent Present Soft tissue PCM & lytic bone lesions
No new lesions • New lesions • >50% increase in
existing lesions Re-treatment • Should not be immediately
started • Initiate therapy with doubling
of serum M-protein within 2 months or increase of urine M-protein >500 mg/24hr
Immediate treatment
IMWG Consensus Statement, 2011

Treatment at relapse Consider SCT
Front-line with novel agent?
Survival is extended with novel agent
Yes No
Bortezomib-based, e.g. • Bortezomib +/- dex • Bortezomib/PLD* • VCD, PAD
IMiD-based, e.g. • Len/dex* • Thal +/- dex • CTD
Bortezomib + IMiD-based, e.g. • VMPT • VTD
*Data available from phase 3 randomized clinical trials Ludwig et al. Oncologist. 2011;16:388-403
Use novel agent

Treatment at relapse
Repeat or change front-line treatment?
treatment after:
• Long remission • No toxicity concerns
from first-line treatment
class after:
• Short remission • Toxicity concern from previous line
Yes
Switch drug Repeat
Consider SCT
Front-line with novel agent?
No
Ludwig et al. Oncologist. 2011;16:388-403
Front-‐line consisted of
Thal-‐based Bortz-‐based
Thal-‐based Bortz-‐based LEN-‐based
t

Considera>ons in case of specific complica>ons
• Renal impairment
― Bortezomib-‐based
― Thalidomide-‐based
― Lenalidomide-‐based (dose modifica5on mandatory)
• Current or recent thromboembolic or cardiovascular events:
― Bortezomib-‐based
― Lenalidomide-‐based following prophylaxis guidelines
• Treatment-‐related peripheral neuropathy
― Lenalidomide-‐based

Dimopoulos et al. ASH 2013 (Abstract 3177), poster presentation
Bortezomib + dex versus bortezomib monotherapy in relapsed MM (n=218)
*P < 0.001
Bortezomib-Dex 13.6 months
Single-agent Bortezomib: 7 months P=0.003
OS comparable between arms
Response rates Bortezomib-Dex Single-agent bortezomib (n=109) (n=109) ORR (CR + PR) 75%* 41%* CR 10% 8% PR 65% 33%
TTP
Better with Bor-Dex
Retrospective matched-pairs analysis:

Salvage ASCT: Myeloma-X Ph 3 prospective study (n= 174)
Cook et al. ASH 2013 (Abstract 765), oral presentation
• Results (median follow-up 12 months):
• Conclusion – First prospective study to demonstrate superior duration of
response for 2nd salvage ASCT
ASCT Cyclophosphamide weekly
(No=98) (No=85) P
Median TTP 19 months 11 months < 0.0001
3year OS 80.3% 62.9% 0.2332
• Pts in relapse following prior ASCT • PAD induction (bortezomib, doxorubicin, dexamethasone) • Randomization: MEL200-ASCT versus CPA weekly x 12

Newer agents for R/R myeloma:
1. Carfilzomib (Kyprolis) IV: G2 proteasome inhibitor
2. Pomalidomide (Pomalyst capsule): G3 IMiD
3. Bendamustine (Trenada) IV: alkylating agent
4. Oral Proteasome Inhibitors: Ixazomib, Oprozomib.

Carfilzomib (Kyprolis vial 60mg ) in in rel/ref MM
• Carfilzomib is a G2 proteasome inhibitor that selectively and irreversibly binds to the proteasome,
• Provides sustained proteasome inhibition without off-target effects
• No significant treatment-related PN
• Dose: 20 mg/m2/day IV (10 min) in cycle 1 (days 1,2,8,9,15,16) and if tolerated increase Cycle 2 & subsequent cycles daily doses to 27 mg/m2/day (repeat cycle every 28 days).
• With Low dose dex à ORR of 67%
Berenson et al. ASH 2013 (Abst. 1934)

Thalidomide analog (3-‐amino-‐thalidomide):
1. Less myelosuppressive effects than lenalidomide.
2. Less cons5pa5on & neuropathy than thalidomide.
Pomalidomide (Pomalyst Capsule 4 mg):
Dose: 4 mg once daily orally on Days 1-‐21 of repeated 28-‐day cycles un5l disease progression.

MM-003 Phase 3 : Pomalidomide + low-dose dex versus high-dose dex in rel/ref MM
Dimopoulos et al. ASH 2013 (Abstract 408), oral presentation
Updated PFS and OS results median follow-up 15.4 months
POM + LoDex HiDex
(n=302) (n=153) P
ORR 31% 10% < 0.001
Median PFS 4.0 months 1.9 months <0.001
Median OS 13.1 months 8.1 months 0.009
Regardless of the presence of del17p or t(4;14)

ORR (>PR) of Carfilzomib and Pomalidomide combinations in in rel/ref MM
Carfilzomib Pomalidomide
Each + LD Dex 67%1 31%2-‐48%3
Both + LD Dex 64%4
With LD Dex & LEN 78%5 -‐-‐-‐
With LD Dex & Bor -‐-‐ 75%6
1. Berenson et al. ASH 2013 (Abst. 1934) 2. Dimopoulos et al. ASH 2013 (Abstract 408), 3. Baz et al. ASH 2013 (Abst. 3200)
4. Shah et al. ASH 2013 (Abst. 690) 5. Wang et al. JCO. 2011; 29: (Abst. 8025) 6. Richardson et al. ASH 2013 (Abst. 1969)

New Therapeutic Algorithm
<65 years 65-‐75 years >75 years 1st Line • Induc>on: VD (VCD-‐VTD)
• ASCT • Maintenance: LEN
Full-‐dose combina>on: MVP (MPT-‐RD)
Reduced-‐dose combina>on: mpt (rd-‐mvp)*
1st Relapse VD RD vd* 2nd Relapse RD VD rd* 3rd Relapse • Carfilzomib
• Pomalidomide 4th Relapse TD
VD: Velcade + Dexamethasone VCD: Velcade + Cyclophosphamide + Dexamethasone RD: Revlimid + Dexamethasone VTD: Velcade + Thalidomide + Dexamethasone TD: Thalidomide + Dexamethasone MPT: Melphalan + Prednisone + Thalidomide MVP: Melphalan + Velcade + Prednisone *Reduced-‐dose

Complications of Multiple Myeloma

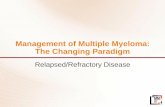
RenalFailure
Hyperviscosity Amyloidosis
MonoclonalProtein
Anaemia
LL 6
BonePains
Hypercalcaemia
Bone Destruction
Release ofCytokines
MarrowInfiltration
Infections
ImmuneDeficiency
MM
MULTIPLE MYELOMA: Complications
70%
<2% 25%
70%
25%
12-15%
98%
◗ Lytic lesions ◗ Fractures ◗ Osteopenia
Bone pains
• IL6
• IgA • AL
SC compression
5-10%

Mechanism of bone resorption:
Plasma cells à macrophage inflammatory protein 1α (MIP-1) à
• ++osteoblasts à ++Receptor Activator of Nuclear Factor-κB Ligand (RANKL) à osteoclastic activation
• -- bone lining cells à Reduction in the level of osteoprotegerin (OPG) (natural antagonist of RANK ligand)
• Increase in the ratio of RANKL:OPG à activation of osteoclasts à bone resorption.

Bone pains
§ Sites: back > chest > extremities § Causes: osteolytic lesions, fractures and osteoporosis § Worsen with movement, not at night (unlike metastasis) § Management:
• Morphia or transdermal fentanyl • Avoid NSAIDs: precipitate RF or exaggerate
corticosteroid-induced gastritis • Splinting or vertebroplasty • Increase mobility when pain is controlled to avoid
increase in bone decalcification, hypercalcemia and DVT.
Sattva and Dunbar, Bethesda Clin. Oncol. (2005)

Management of Bone Disease
Cellular Effects of Bisphosphonates: 1. Osteoclast inhibition and apoptosis 2. Inhibit production of cytokines that stimulate osteoclasts (IL-6,
VEGF, RANKL) 3. Tumor cell apoptosis 4. Synergistic anti-tumor effects with anticancer treatments 5. Inhibition of adhesion molecules 6. Anti-angiogenic 7. Direct effect on Myeloma (may slow tumor growth)
Djulbegovic, et al Cochrane Database of Systematic Reviews(2002)
Bisphosphonates:
Meta-analysis of 10 trials: Adding bisphosphonates to the treatment of myeloma reduces vertebral fractures and pain but not mortality

Management of Bone Disease IV Bisphosphonates: Side Effects
• Flu-like symptoms (fever, myalgias, arthralgias) • Occurs usually 12-48 hrs following the infusion • Lasts 6-24 hrs • Occurs in a minority of pts (10-20%) • Not observed with continued dosing • Similar frequency with different drugs
• Renal dysfunction • Ocular (rare, with pamidronate): scleritis • Osteonecrosis of the jaw

Use of Bisphosphonate in MM: {ASCO recommendations 2007}
Indications: ◗ Plain radiograph(s) à lytic destruction of bone ◗ Compression fracture of the spine from osteopenia ◗ Osteopenia with no radiographic evidence of lytic bone
disease.
Not recommended in: ◗ Patients with solitary plasmacytoma or smoldering or
indolent myeloma without documented lytic bone disease ◗ Patients with MGUS.
Management of Bone Disease
Kyle et al., JCO 2007.

Use of Bisphosphonate in MM: {ASCO recommendations 2007} Drugs used : ◗ Pamidronate (Aredia) 90mg IV (≥2hours) every 4 weeks or
◗ Zoledronic acid (Zometa) 4 mg IV (15 min) every 4 weeks
◗ 9.5-fold greater risk for the development of osteonecrosis of the jaw with zoledronic acid compared with pamidronate, patients may prefer pamidronate to zoledronic acid
Management of Bone Disease
Kyle et al., JCO 2007.

Use of Bisphosphonate in MM: {ASCO 2007} Duration of therapy: ◗ Therapy with bisphosphonates be given monthly for a
period of two years ◗ At two years, the physician should seriously consider
stopping bisphosphonates in patients with responsive or stable disease, but their further use is at the discretion of the treating physician.
◗ For those patients in whom bisphosphonates were withdrawn after two years, the drug should be resumed upon relapse with new onset skeletal related events.
Management of Bone Disease
Kyle et al., JCO 2007.

Use of Bisphosphonate in MM: {ASCO 2007}
Rate of infusion is the key factor in prevention of renal dysfunction: Rates faster than 0.3-0.7 mg/min are associated with renal dysfunction
Pre-existing Renal impairment: ◗ Mild-to-moderate (cr cl 30 to 60 mL/min):
v Should receive a reduced dosage of zoledronic acid. v No changes in infusion time or interval are required.
◗ Severe renal impairment (cr cl <30 mL/min): v Zoledronic acid is not recommended v Pamidronate reduced dose administered over 4 to 6
hours is recommended
Kyle et al., JCO 2007.

Use of Bisphosphonate in MM: {ASCO 2007} Renal monitoring: Serum creatinine should be monitored before each dose of pamidronate or zoledronic acid: • Renal deterioration without apparent cause during
bisphosphonate therapy, zoledronic acid or pamidronate should be withheld.
• When the serum creatinine returns to within 10% of the baseline levelà Bisphosphonate therapy can be resumed, at the same dosage as that before treatment interruption.
Management of Bone Disease
Kyle et al., JCO 2007.

Osteonecrosis of the Jaws (ONJ):
• A severe "bone" disease, associated with bisphosphonate therapy that affects the jaws
• Incidence 5% • Although ONJ can occur spontaneously, most
cases occur in patients after a tooth extraction or other invasive dental procedure
• Exposed infected necrotic bone in the maxillofacial region that does not heal within 8 weeks.
• Presents as pain and/or numbness in the affected area, soft-tissue swelling, drainage, and tooth mobility.
Terpos et al, Ann Oncol (2009)

Osteonecrosis of the Jaws (ONJ):
Risk factors: – Duration of bisphosphonate exposure (5-15% at 4 yr).
– Invasive dental procedures such as extractions (50%).
Prevention: (ASCO 2007) – Dental evaluation prior to starting bisphosphonates – Maintain excellent oral hygiene – Avoid dental procedures while receiving
bisphosphonate. – Antibiotic prophylaxis before dental procedures.
Dimopoulos et al, Ann Oncol (2009)

Osteonecrosis of the Jaws (ONJ): Management:
– Usually conservative: • Discontinuation of bisphosphonates • Limited debridement • Antibiotic therapy • Topical mouth rinses.
– Surgical resection of necrotic bone should be reserved for refractory cases.
– Healing of ONJ in 75% patients.
Khan et al, J Rheumatol (2008)

Hypercalcemia
Clinical presentation: 1. GIT: Anorexia, nausea, vomiting, constipation 2. Dehydration 3. Neurological: weakness, depression, apathy, coma 4. Renal tubular damage: polyuria, polydipsia, rising
creatinine. 5. ECG : Short QT interval, arrhythmias.
Mellstedt , Ann Oncol (2007)

Hypercalcemia: Management: Treatment of MM-related hypercalcemia should be started at a corrected serum Ca level > 12 mg/dL:
• Aggressive hydration: with 3-4 L saline / 24 hrs.
• Dexamethasone: 40 mg I.V. daily for 4 days.
• Intravenous diuretic therapy (e.g. furosemide) à ++ renal clearance of calcium
• Bisphosphonates are given if no response occurs or if the hypercalcemia is severe. A single dose of pamidronate or Zoledronic acid will normalize the calcium levels within 24-72 hours in most patients.
He et al, Cochrane Database Syst Rev (2003)

Pathological Fracture: • Fractures of long bones: fixation and
medullary nail à PO irradiation. • In vertebral fractures: surgery is usually not
indicated. Send for radiotherapy. • I.V. bisphosphonate therapy. • If the heart is in the irradiation field, delay
adriamycin and cyclophosphamide treatment.

• All patients should immediately receive high-dose dexamethasone therapy (grade A).
• Patients who have neurologic impairment (deficits and/or symptoms) should also receive local radiotherapy within 24 h of diagnosis (grade C).
• Surgery (laminectomy or Kyphoplasty) is not indicated unless there is spinal instability or vertebral collapse à post-operative radiotherapy (grade B).
BAROSI et al, Haematologica (2004)
Spinal cord compression (SCC)
• C/P: pain (local or radicular), weakness, sensory disturbance and/or sphincter dysfunction

Radiotherapy:
Indications: • To control pain that is refractory to narcotics • Big osteolytic lesions. • Significant osteolytic lesions in weight-bearing bone (for fear
of pathological fracture). • Cord compression. • Extramedullary plasmacytoma.
Supportive care in myeloma
Caution: • Limit the amount of radiation that is administered because
radiation to large areas of bone can limit the amount of systemic chemotherapy that can be administered
• Should be discouraged if stem cell transplant is planned.

Trea5ng the myeloma pa5ent with renal impairment


Causes of renal failure in MM
1. Cast nephropathy 2. Hypercalcemia 3. Volume depletion (dehydration) 4. Primary amyloidosis 5. IV contrast dye 6. Nephrotoxic meds

Causes of renal failure in MM
1. Cast nephropathy 2. Hypercalcemia 3. Volume depletion (dehydration) 4. Primary amyloidosis 5. IV contrast dye 6. Nephrotoxic meds

Decreased renal clearance of FLC à ++ sFLC à direct tubular injury.

How to reduce sFLC levels?
― Effec5ve chemotherapy -‐-‐-‐ Novel agents
― Direct removal of FLCs from serum -‐-‐-‐ PE, HD
Management of myeloma kidney: Time to target FLCs?
Hutchison et al. Am Soc Nephrology (2011);22(6): 1129-‐1136


Drugs used in myeloma kidney
In RI* HD Dexa Thalidomide Lenalidomide Bortezomib +DEX
Rate of improvement
Rapid Slow Rapid Very Rapid (1-‐2.5 ms)
Dura5on of response
Not sustained Sustained Sustained Sustained
Response rate
Not high Most pts with moderate RI
In some pa5ents with Len/Dex
60%
Safety Safe Safe Increased myelosuppression
Safe
Dose reduc5on
Not needed Not needed Mandatory Not needed
Conclusion Highly ac5ve Used with cau5on
Feasible and effec5ve with dose adjustments
The recommended treatment in any degree of RI.
*renal impairment
HDT/ASCT (Mel140); procedure: restricted to pa5ents <60 years with chemotherapy-‐sensi5ve disease and good PS

Why does plasma exchange (PE) not work? • Effectively clears the intra-
vascular volume
• Therefore extra-vascular component is not cleared
• FLCs are 80% extra-vascular
• Therefore, total body load of FLCs is not significantly reduced
Clark et al Ann Int MED (2005)
• Extended (6 h) High Cut-Off (HCO) Hemodialysis is more effective for FLC removal than PE
Direct removal of FLCs from serum

Light chain amyloidosis (AL) :
• C/P: carpal tunnel syndrome or generalized edema (NS)
• < 60 years + <2 organs involved and no severe heart involvement à HDC/SCT.
◗ Between 60 and 65 years or creatinine > 2 mg/dL à SCT should be considered with caution and the melphalan dose should be reduced.
◗ Not eligible for HDC/SCT à standard MP
◗ Refractory or relapsing patients: intermediate dose dexamethasone and thalidomide
BAROSI et al, Haematologica (2004)

Anemia:
◗ Treatment of reversible causes of anemia such as iron, folate, or vitamin B12 deficiency
◗ Treatment of the underlying disease and improvement in renal function.
◗ Blood transfusion
◗ Erythropoietin
Supportive care in myeloma

Anemia: Erythropoietin therapy (ASCO recommendations 2010) • Strong recommendation against the use of ESAs to treat
patients with MM who are not receiving concurrent CT.
• Begin treatment with CT and observe the hematologic outcomes achieved solely through tumor reduction before considering epoetin.
• If an increase in Hb is not observed after CT à treatment with epoetin or darbepoetin can be initiated.
• Risk of thromboembolism: previous history of thromboses, prolonged periods of immobilization and treatment with thalidomide or lenalidomide and doxorubicin or corticosteroids
Supportive care in myeloma

Infections: • Suppressed humoral and cell-mediated immunity from
the disease and the added effects of therapy.
• Principal organisms: S. pneumoniae and H. influenzae.
• HZ activation is also common and requires antiviral therapy to prevent dissemination (esp. with bortezomib)
• Patients should be vaccinated against S. pneumoniae, H. influenzae, and influenza (annual vaccine).
BAROSI et al, Haematologica (2004)
Supportive care in myeloma

Hyperviscosity: ◗ Specially with Ig A MM
◗ C/P: Mucosal hemorrhage, visual abnormalities, HF, seizures, vertigo.
◗ The serum viscosity levels do not correlate well with the symptoms.
◗ Symptomatic hyperviscosity should be treated with plasma exchange (every 3-5 days) until definite therapy can be initiated.
◗ A decision to perform plasmapheresis depends on the symptoms and changes in the ocular fundus.
◗ Chemotherapy should be started promptly once hyperviscosity has been stabilized by plasma exchange
BAROSI et al, Haematologica (2004)
Supportive care in myeloma

Complications of New Myeloma Therapy
1. Venous Thromboembolism (VTE)
2. Peripheral Neuropathy (PN)
3. Hematological adverse events

Emergent Complications of New Myeloma Therapy
1. Venous Thromboembolism (VTE): Type: • Oral regimens à DVT or pulmonary embolism • Infusional regimens à CVL-related thrombosis (~50%) Incidence: • Highest during the first 3 to 4 months following diagnosis • Most VTEs occur within the first 60 days of therapy,
coinciding with maximum cytoreduction. • Varied according to drugs used à
Johnson et al, Blood (2008)

Emergent Complications of New Myeloma Therapy
1. Venous Thromboembolism (VTE) (DVT, Pulmonary):
Thalidomide:
Facon et al, Lancet (2007)
%VTE Therapy
~3-4% Dexamethasone alone or MP
~2-3% Thalidomide alone
14-26% THAL/DEX
12-20% MPT

1. Venous Thromboembolism (VTE) (DVT, Pulmonary)
Lenalidomide: • Single-agent: does not appear to increase VTE • Lenalidomide + dexamethasone à marked increased in
VTE risk. • The risk is higher with higher dexamethasone doses,
administration of erythropoietin, and concomitant administration of other agents ( with CPA 14%)
Bortezomib: • Did not seem to increase the risk of VTE, at least not in
patients with relapsed or refractory disease.
Palumbo et al Leukemia (2008) Richardson et al, Blood (2006)

Prevention of VTE:
Based on the assessment for number of risk factors for VTE:
1. Myeloma-related (hyperviscosity, newly diagnosed status) 2. Therapy-related (most important)
• High-dose dexamethasone (>480 mg/month) • Doxorubicin, Multiagent chemotherapy • EPO • CVL
3. Patient-related : – Age >60. – History of VTE – Inherited thrombophilia (e.g. deficiencies of antithrombin III,
proteins C, and S) – Immobilization – Surgery
4. Comorbidities: infections, DM, cardiac or renal, obesity.
Palumbo, et al Leukemia (2008)

1. Venous Thromboembolism (VTE):
Thromboprophylaxis: (ASCO guidelines 2013)
(1) Low-dose aspirin for patients with <1 risk factor for VTE (2) LMWH: once a day, or (3) Full-dose warfarin for:
– Patients with > 2 risk factors for VTE – All patient receiving concurrent HD DEX or doxorubicin.
• Randomized study showed no differences in incidence in VTE among the three prophylaxis regimens in patients receiving thalidomide combinations
• In elderly pts: WAR showed less efficacy than LMWH • Recommended duration of prophylaxis is 6-12 months

Emergent Complications of New Myeloma Therapy
2. Peripheral Neuropathy Drugs: • Bortezomib:
• Grade 3/4 PN: ~20% of newly diagnosed & 30% of relapsed • When combined with lenalidomide à neuroprotective effect.
• Thalidomide`: • PN in 75%: esp. high dose (400 mg), long duration of therapy. • Switching to lenalidomide will usually improve PN
Should be distinguished from other causes such as: – Paraneoplastic neuropathies, – AL amyloidosis. – Neurotoxic chemotherapy (vincristine or cisplatinum) – Diabetes mellitus
Richardson, Br J Hematol, (2009)

Emergent Complications of New Myeloma Therapy
2. Peripheral Neuropathy:
Clinical findings:
Type Presenting symptom Thalidomide Bortezomib Sensory Hypoesthesia, paresthesia:
numbness, tingling, pin-prick sensation, hyperesthesia
Common Rare
Neuropathic pain Rare Common Ataxia, gait disturbance Rare Rare
Motor Tremors Common Rare Weakness Rare Rare
Autonomic GIT Constipation Constipation CVS Bradycardia Orthostatic
hypotension Others Impotence ---
Sonneveld et al. ASH Educ Program 2010

2. Peripheral Neuropathy: Dose adjustment:
PN Sensory (Paraesthesiae)
Motor (Weakness)
Thalidomide Dose Bortezomib Dose
G1 • Mild, or • Loss of tendon
reflexes
On exam/testing only
• Asymt.: no action • Symt.: 50% reduction
• Asymt.: no action • Symt.: reduction to
1mg/m2 or Weekly administration Not interfering with function* or ADL**
G2 • Moderate, • Mild • Discontinue • If PN resolves, restart
at 50% reduction.
• Reduction to 1mg/m2
weekly. Interfering with function*, but not
interfering with ADL**
G3 • Intolerable • Marked Discontinue • Discontinue. • If PN resolves, restart
at 0.7 mg/ m2 weekly. Interfering with ADL**; bracing or
assistance to walk (cane or walker)
G4 • Disabling • Paralysis Discontinue Discontinue
Time to resolution of symptoms Longer time 3 months-2 years
Sonneveld et al. ASH Educ Program 2010
*Function (instrumental): preparing meals, shopping for groceries or clothes, using telephone **Activities of Daily Living: bathing, dressing and undressing, feeding self, using the toilet

2. Peripheral Neuropathy:
• Change of schedule (e.g. weekly Bortezomib), • Change of administration route (e.g. S.C. Bortezomib) • Switch to non-neurotoxic agent • Chemoprotectives: Vit. B12, folic acid, antioxidants (vit
E), glutathione, L-carnitine . • Symptom relief:
• Pain relievers: NSAIDs, tramadol, lidocaine patch • Anti-seizure medications: gabapentin (Neurontin),
pregabalin (Lyrica), carbamazepine (Tegretol). • Neurotrophic drugs: Cerebrolysin • Antidepressants: Amitriptyline, Nortriptyline,
Duloxetine, Venlafaxine.
Apfel and Zochodne, Neurology (2004) Sonneveld et al. ASH Educ Program 2010

Emergent Complications of New Myeloma Therapy
3. Hematological adverse events:
Bortezomib Lenalidomide Thalidomide Toxic effect on BM No Yes No Neutropenia: • G3/4 (<1000) • Pattern
• FN
14% Transient, with rapid recovery to baseline Uncommon
40-70% Need for HGFs in 34-49% 3.4%
13%
7%
Thrombocytopenia: • G3/4 (<50.000) • Pattern
30% Cyclical: with recovery to baseline
15% Progressive
Uncommon
Anemia: • G3/4 (<8 g)
10%
13%
Rare

Bortezomib: • Withheld at the onset of G4 toxicity (ANC<500, PLT<25.000). • Once the toxicity has resolved, treatment may be restarted at a 25%
reduced dose
Dose Modifications in Hematological adverse events
Lenalidomide: • PLT <30,000: Interrupt LEN. If PLT return to ≥30,000, restart at 15 mg. • ANC <1,000: Interrupt LEN. If ANC return to ≥1,000, restart at 25 mg. • For each subsequent ANC or PLT drop, interrupt & resume at 5 mg less
than the previous dose. • Do not dose below 5 mg daily
Thalidomide: • ANC= 500–1,000: consider G-CSF or reduce thalidomide dose by 50%. • ANC <500: Stop the thalidomide and consider G-CSF until ANC > 500. • Thalidomide may then be restarted at a 50% dose reduction.

Confidential – not for external use
THANK YOU