Updates in cancer genetic testing
33
Lauren Schenck Genetic Counselor, LCGC
-
Upload
peninsula-coastal-region-of-sutter-health -
Category
Health & Medicine
-
view
510 -
download
2
Transcript of Updates in cancer genetic testing

Lauren Schenck Genetic Counselor, LCGC

I have no financial relationships or conflicts of interest to disclose in relation to this presentation

Review of genetic counseling and cancer genetics
How common is inherited cancer? Red flags in a family history that should
prompt a genetics evaluation Overview of hereditary breast and ovarian
cancer (HBOC) and Lynch syndrome Update in genetic testing: panel tests
Assess personal and family history of cancer ◦ Is genetic testing appropriate in the family? ◦ Identify the most informative family member to test ◦ Determine and order the most appropriate genetic test(s)
Provide patient-oriented education about hereditary cancer syndromes and genetic testing
Interpret genetic test results, help patients and their
physicians understand and apply genetic test results to medical management decisions, and assist with patient’s psychosocial adjustment
Connect patients to supportive, informative and research-
related resources

Cancers diagnosed younger than average ◦ Breast cancer <50 yo ◦ Colon cancer <50 yo
Multiple family members with similar or related cancers ◦ Breast and ovarian ◦ Colon and uterine ◦ Melanoma and pancreatic
Rare cancers ◦ Male breast cancer ◦ Ovarian cancer ◦ Triple negative breast cancer (<60 yo)
People diagnosed with cancer more than once Multiple generations affected by related cancers AJ ancestry + breast and/or ovarian cancer

Hereditary breast and ovarian cancer (HBOC) Lynch syndrome

Genes: BRCA1, BRCA2 Most significant cancer risk: breast, ovarian Management: ◦ Females: high risk breast cancer screening OR mastectomy, BSO ◦ Males: PSA, breast awareness, consideration of mammograms

Breast cancer Gynecological cancer Cancer, unknown

Recommendations: ◦ Bilateral mastectomy or high risk surveillance
following breast cancer tx ◦ BSO ◦ Genetic testing for family members

Breast cancer Gynecological cancer Cancer, unknown
Also carries the BRCA1 mutation

Genes: MLH1, MLH2, MSH6, PMS2, EPCAM Most significant cancer risk: colon, uterine Management: Colonoscopy every 1-2 years,
consideration of hysterectomy and BSO (females)
1994-1995 Myriad patent on BRCA1 & BRCA2
2012 Ambry offers NGS, Without BRCA
2013 Supreme Court rules human genes cannot be patented
TODAY Many new labs and panels!
Which genetic testing
lab?
Most appropriate
test?

There are more than 50 well described cancer susceptibility syndromes, many of which can result from mutations in more than one gene

Benefits Limitations
Many genes analyzed ◦ Higher mutation
detection rate Often same cost as
single gene tests ◦ Generally cheaper than
multiple single gene tests One blood/saliva
sample
Unknown results Genes without
management guidelines

Benefits Limitations
Many genes analyzed ◦ Higher mutation
detection rate Often same cost as
single gene tests ◦ Generally cheaper than
multiple single gene tests One blood/saliva
sample
Unknown results Genes without
management guidelines
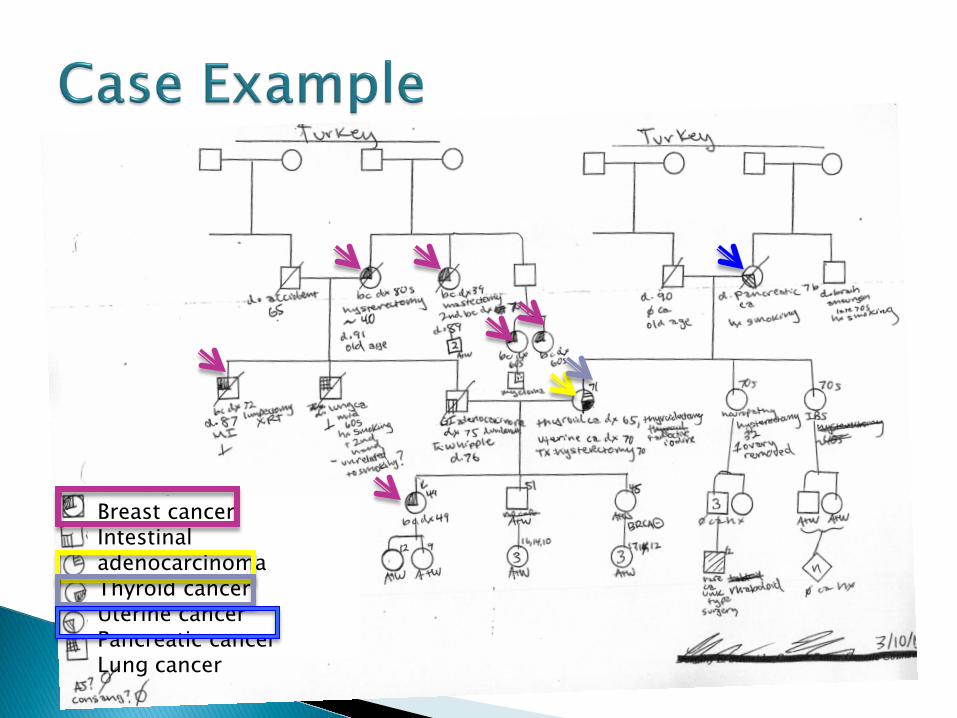
Breast cancer Intestinal adenocarcinoma Thyroid cancer Uterine cancer Pancreatic cancer Lung cancer


Studies suggest 2-4 fold increased risk of breast cancer in female carriers
Possible increased risks of pancreatic cancer Individuals with two ATM mutation have Ataxia
Telangiectasia (AT) ◦ Severe childhood onset condition involving
progressive ataxia often beginning at age 5yo or earlier, telangiectasia of the conjunctivae, immunodeficiency ◦ Cancer risks: leukemia, lymphoma ◦ Increased sensitivity to radiation

Recommendations: ◦ High risk breast cancer surveillance ◦ Genetic testing for family members
NOT a carrier of the ATM mutation
Presumably ATM mutation carrier

Benefits Limitations
Many genes analyzed ◦ Higher mutation
detection rate Often same cost as
single gene tests ◦ Generally cheaper than
multiple single gene tests One blood/saliva
sample
Unknown results Genes without
management guidelines
Important to assess personal and family history to determine:
Is a panel appropriate? Which genes?

68y female recently diagnosed with breast cancer
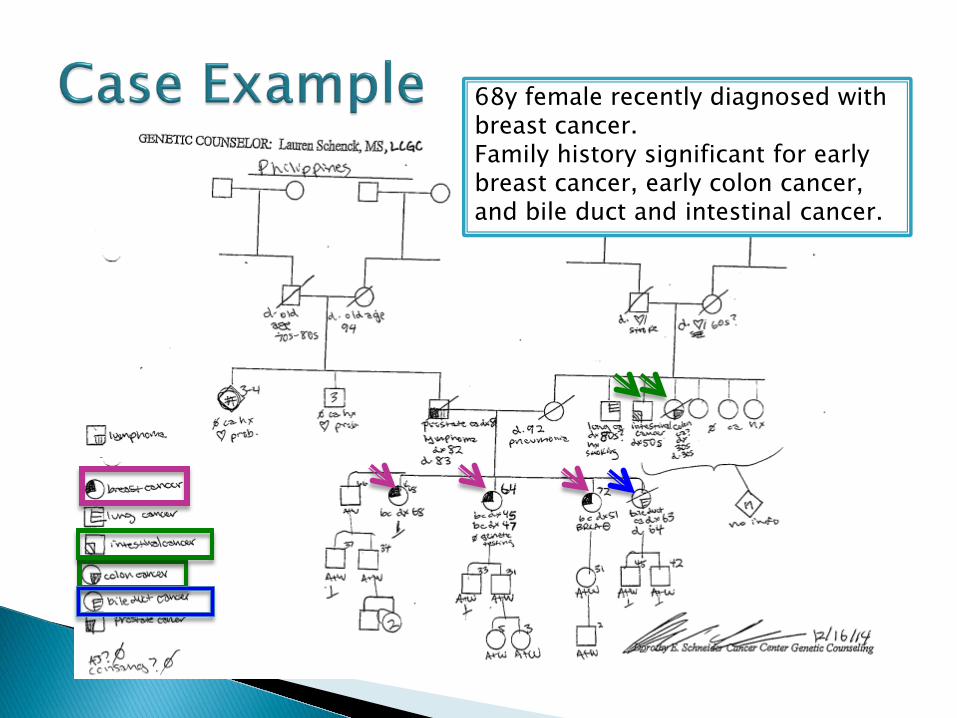
68y female recently diagnosed with breast cancer. Family history significant for early breast cancer, early colon cancer, and bile duct and intestinal cancer.

Benefits Limitations
Many genes analyzed ◦ Higher mutation
detection rate Often same cost as
single gene tests ◦ Generally cheaper than
multiple single gene tests One blood/saliva
sample
Unknown results Genes without
management guidelines

Breast cancer screening ◦ Oncology care team recommendations
Colon cancer screening ◦ Close blood relatives begin colon screening 5-10
years younger than earliest colon cancer diagnosis ◦ Continuation of colonoscopies at the intervals
recommended by gastroenterologist aware of personal and family history

Not all laboratories’ panels are created equal ◦ # of genes ◦ Sensitivity ◦ Portion of gene analyzed and how thorough ◦ Technology used for mutation confirmation ◦ Prices, billing policies, turnaround time, reporting ◦ VUS rates among labs ◦ Protocols for VUS reporting and reclassification

Not all laboratories’ panels are created equal ◦ # of genes ◦ Sensitivity ◦ Portion of gene analyzed and how thorough ◦ Technology used for mutation confirmation ◦ Prices, billing policies, turnaround time, reporting ◦ VUS rates among labs ◦ Protocols for VUS reporting and reclassification

Not all laboratories’ panels are created equal ◦ # of genes ◦ Sensitivity ◦ Portion of gene analyzed and how thorough ◦ Technology used for mutation confirmation ◦ Prices, billing policies, turnaround time, reporting ◦ VUS rates among labs ◦ Protocols for VUS reporting and reclassification

Comprehensive cancer risk assessment Personalized screening and management
recommendations Most appropriate and cost effective genetic
testing Supportive resources for your patients Saves you time!


http://www.cancer.gov/about-cancer/causes-prevention/genetics/brca-fact-sheet
http://www.cancer.gov/types/colorectal/hp/colorectal-genetics-pdq#section/all
http://www.nccn.org/professionals/physician_gls/pdf/genetics_screening.pdf
http://www.nccn.org/professionals/physician_gls/pdf/genetics_colon.pdf
Cancer Risks and Mortality in Heterozygous ATM Mutation Carriers http://jnci.oxfordjournals.org/content/97/11/813.short
http://www.mills-peninsula.org/cancer/services/genetic-counseling.html