Updates in Asthma and COPD - cdn.ymaws.com · UPDATES IN ASTHMA AND COPD Audrey Umbreit, PharmD,...
39
UPDATES IN ASTHMA AND COPD Audrey Umbreit, PharmD, BCACP MAPA Pharmacology Conference May 11, 2018
Transcript of Updates in Asthma and COPD - cdn.ymaws.com · UPDATES IN ASTHMA AND COPD Audrey Umbreit, PharmD,...
UPDATES IN ASTHMA
AND COPD Audrey Umbreit, PharmD, BCACP
MAPA Pharmacology Conference
May 11, 2018
Objectives
• Review GINA and GOLD guidelines
• Identify patients who would benefit from the following medications: • anti-IgE
• anti-IL5
• Roflumilast
• Chronic macrolide therapy
• Compare / Contrast new inhaler devices • Ellipta
• Respiclick
• Respimat
• Apply the outcomes of new studies to patient case examples
Abbreviations
Medications
• LABA = long acting beta agonist
• LAMA = long acting anti-muscarinic agent
• LTRA = leukotriene receptor antagonist
• ICS = inhaled corticosteroid
• OCS = oral corticosteroid
• PDE4I = phosphodiesterase-4 inhibitor
• SABA = short acting beta agonist
• SAMA = short acting anti-muscarinic agent
Other Abbreviations
• GINA = Global Initiative
for Asthma
• GOLD = Global initiative
for chronic Obstructive
Lung Disease
• PRN = as needed
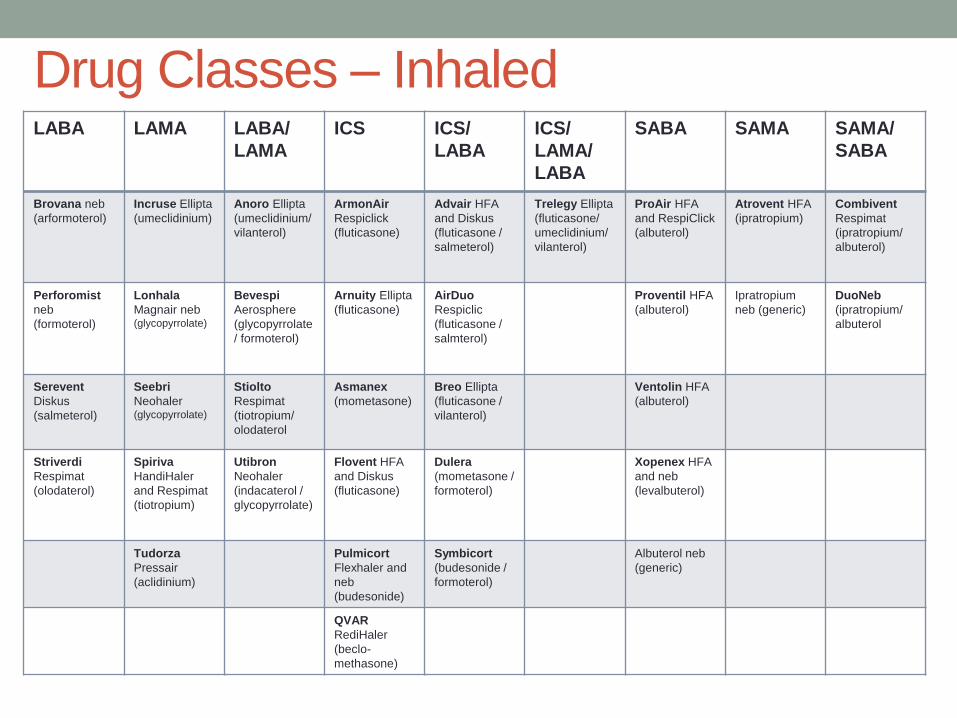
Drug Classes – Inhaled LABA LAMA LABA/
LAMA
ICS ICS/
LABA
ICS/
LAMA/
LABA
SABA SAMA SAMA/
SABA
Brovana neb
(arformoterol)
Incruse Ellipta
(umeclidinium)
Anoro Ellipta
(umeclidinium/
vilanterol)
ArmonAir
Respiclick
(fluticasone)
Advair HFA
and Diskus
(fluticasone /
salmeterol)
Trelegy Ellipta
(fluticasone/
umeclidinium/
vilanterol)
ProAir HFA
and RespiClick
(albuterol)
Atrovent HFA
(ipratropium)
Combivent
Respimat
(ipratropium/
albuterol)
Perforomist
neb
(formoterol)
Lonhala
Magnair neb (glycopyrrolate)
Bevespi
Aerosphere
(glycopyrrolate
/ formoterol)
Arnuity Ellipta
(fluticasone)
AirDuo
Respiclic
(fluticasone /
salmterol)
Proventil HFA
(albuterol)
Ipratropium
neb (generic)
DuoNeb
(ipratropium/
albuterol
Serevent
Diskus
(salmeterol)
Seebri
Neohaler (glycopyrrolate)
Stiolto
Respimat
(tiotropium/
olodaterol
Asmanex
(mometasone)
Breo Ellipta
(fluticasone /
vilanterol)
Ventolin HFA
(albuterol)
Striverdi
Respimat
(olodaterol)
Spiriva
HandiHaler
and Respimat
(tiotropium)
Utibron
Neohaler
(indacaterol /
glycopyrrolate)
Flovent HFA
and Diskus
(fluticasone)
Dulera
(mometasone /
formoterol)
Xopenex HFA
and neb
(levalbuterol)
Tudorza
Pressair
(aclidinium)
Pulmicort
Flexhaler and
neb
(budesonide)
Symbicort
(budesonide /
formoterol)
Albuterol neb
(generic)
QVAR
RediHaler
(beclo-
methasone)

ASTHMA
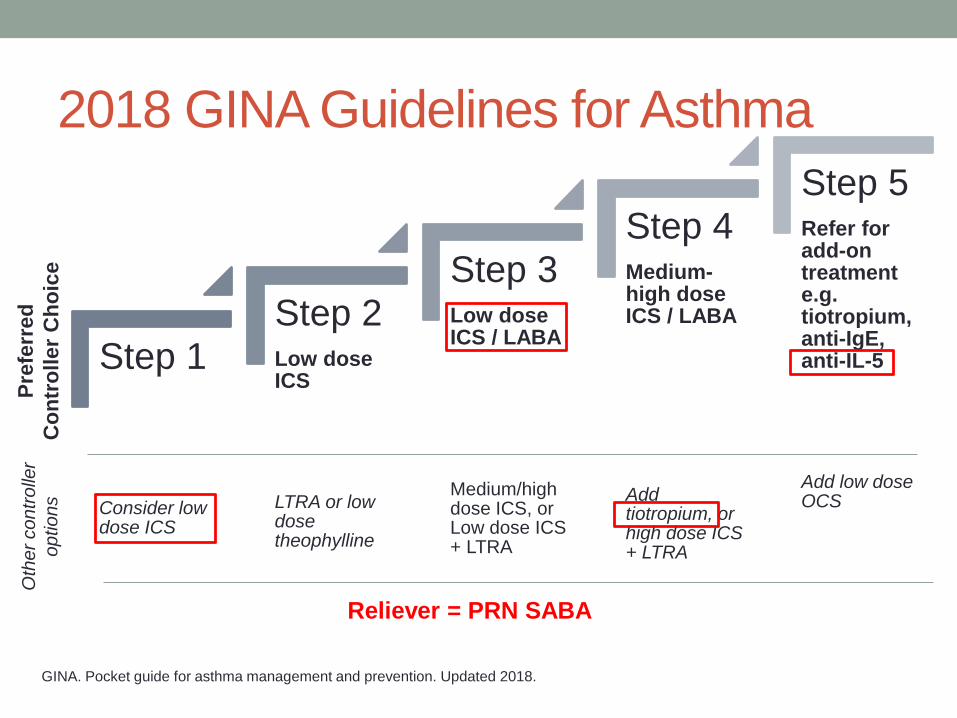
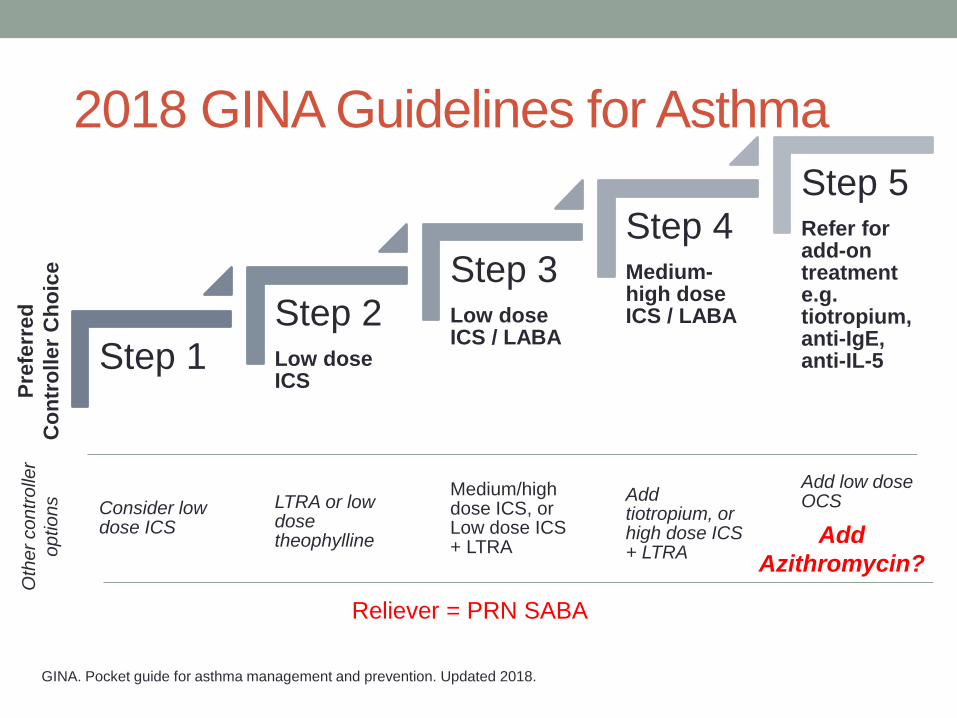
2018 GINA Guidelines for Asthma
Step 1
Consider low dose ICS
Step 2 Low dose ICS
LTRA or low dose theophylline
Step 3 Low dose ICS / LABA
Medium/high dose ICS, or Low dose ICS + LTRA
Step 4 Medium-high dose ICS / LABA
Add tiotropium, or high dose ICS + LTRA
Step 5 Refer for add-on treatment e.g. tiotropium, anti-IgE, anti-IL-5
Add low dose OCS
GINA. Pocket guide for asthma management and prevention. Updated 2018.
Pre
ferr
ed
Co
ntr
oller
Ch
oic
e
Oth
er
co
ntr
olle
r
op
tio
ns
Reliever = PRN SABA
• Step 1 • It is explained that the reason ICS should be considered for
patients with mild asthma (rather than prescribing SABA alone) is to reduce their risk of serious exacerbations (Pauwels, Lancet 2003;
O’Byrne AJRCCM 2001; Reddel Lancet 2017)
• Steps 3-4 • From the large FDA LABA safety studies: adding LABA to ICS in a
combination inhaler reduces risk of exacerbations and improves symptoms and lung function, compared with the same dose of ICS alone, but with only a small reduction in reliever use (Stempel NEJM 2016, Peters NEJM 2016)
• Step 5 and Box 3-14: management of severe asthma • Subcutaneous benralizumab (monoclonal anti-IL5 receptor α
antibody) is another add-on treatment for patients aged ≥12 years with severe eosinophilic asthma
Treatment steps – changes in 2018
What’s new in GINA 2018? Slide from www.ginasthma.org
• Perimenstrual (catamenial) asthma – new section added
• Asthma worse premenstrually in ~20% women
• More common in older women, higher BMI, longer duration and
more severe asthma; often have dysmenorrhea, shorter cycles,
longer bleeding; aspirin-exacerbated respiratory disease more
common (Sanchez-Ramos Exp Rev Respir Med 2017)
• Add-on treatment: oral contraceptives and/or LTRA may be helpful
• The recommendation against stopping ICS during
pregnancy has been reinforced
• ICS reduce the risk of exacerbations in pregnancy (Evidence A) (Schatz AAAI 2005; Murphy Clin Chest Med 2011)
• Stopping ICS increases the risk of exacerbations in pregnancy
(Evidence A) (Murphy Thorax 2006)
Perimenstrual asthma, and asthma in
pregnancy
What’s new in GINA 2018? Slide from www.ginasthma.org

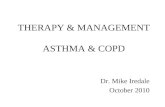
Biologic Medications for Asthma:
Mechanism of Action Anti-IL5 (benralizumab,
mepolizumab, reslizumab)
Anti-IgE (omalizumab)
Image from www.pharmacodia.com Image from severeasthma-birmingham.co.uk

Test your skills #1
Which of the following patients would be a candidate for
mepolizumab (anti-IL5)?
A) 6 y/o with severe asthma, ACT = 19, eosinophil count of
150cells/µL, currently taking high-dose ICS
B) 25 y/o with severe asthma, ACT = 16, eosinophil count
of 300cells/µL, currently taking high-dose ICS + LABA
C) 32 y/o with severe asthma, ACT = 15, eosinophil count
of 100cells/µL, currently taking high-dose ICS + LABA
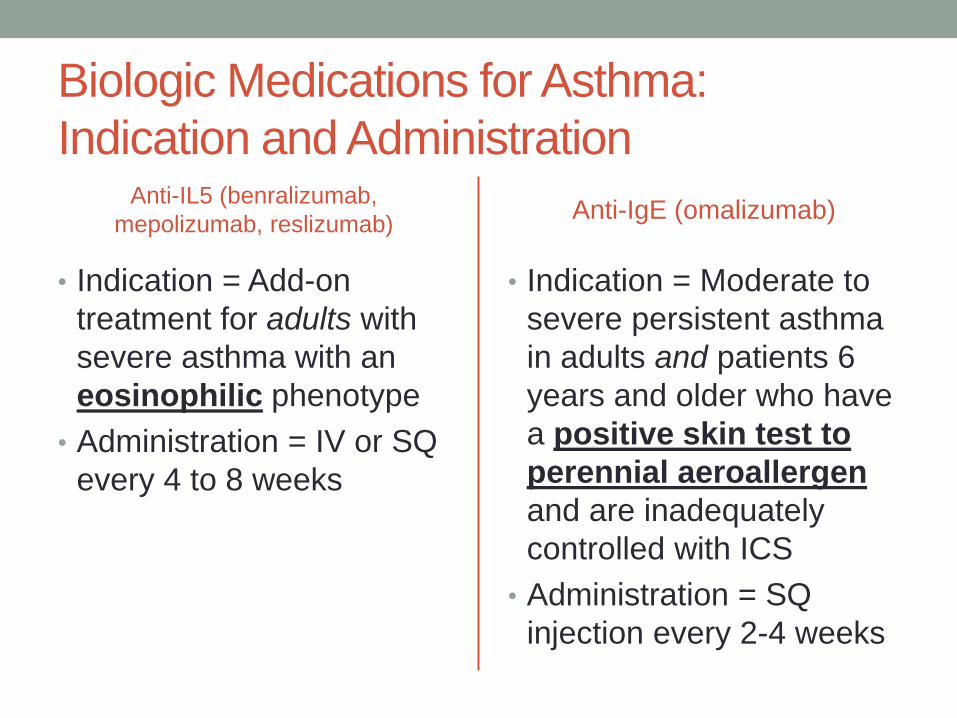
Biologic Medications for Asthma:
Indication and Administration Anti-IL5 (benralizumab,
mepolizumab, reslizumab)
• Indication = Add-on
treatment for adults with
severe asthma with an
eosinophilic phenotype
• Administration = IV or SQ
every 4 to 8 weeks
Anti-IgE (omalizumab)
• Indication = Moderate to
severe persistent asthma
in adults and patients 6
years and older who have
a positive skin test to
perennial aeroallergen
and are inadequately
controlled with ICS
• Administration = SQ
injection every 2-4 weeks
Test your skills #1
Which of the following patients would be a candidate for
mepolizumab (anti-IL5)?
A) 6 y/o with severe asthma, ACT = 19, eosinophil count of
150cells/µL, currently taking high-dose ICS
B) 25 y/o with severe asthma, ACT = 16, eosinophil
count of 300cells/µL, currently taking high-dose ICS
+ LABA
C) 32 y/o with severe asthma, ACT = 15, eosinophil count
of 100cells/µL, currently taking high-dose ICS + LABA
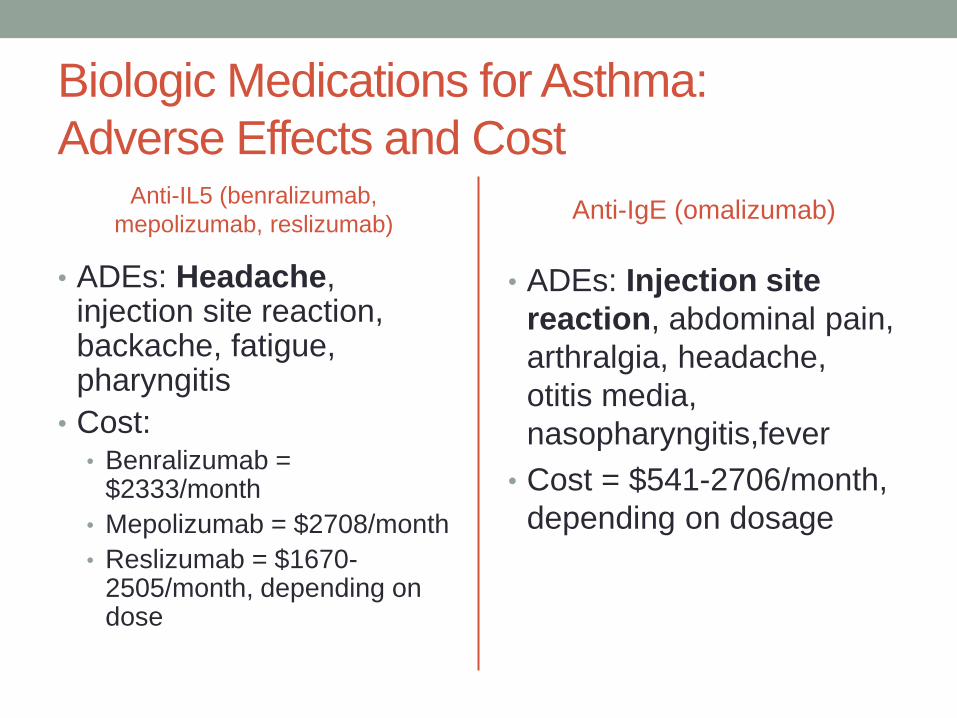
Biologic Medications for Asthma:
Adverse Effects and Cost Anti-IL5 (benralizumab,
mepolizumab, reslizumab)
• ADEs: Headache, injection site reaction, backache, fatigue, pharyngitis
• Cost: • Benralizumab =
$2333/month
• Mepolizumab = $2708/month
• Reslizumab = $1670-2505/month, depending on dose
Anti-IgE (omalizumab)
• ADEs: Injection site
reaction, abdominal pain,
arthralgia, headache,
otitis media,
nasopharyngitis,fever
• Cost = $541-2706/month,
depending on dosage
COPD
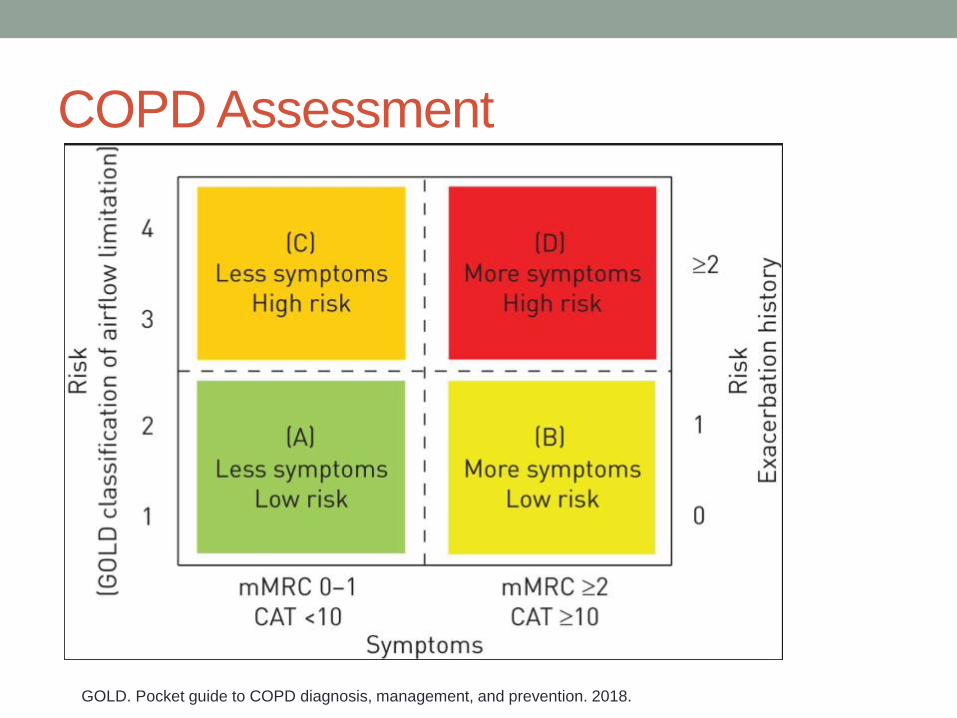
COPD Assessment
GOLD. Pocket guide to COPD diagnosis, management, and prevention. 2018.

Test your skills #2
What therapy would be the best choice to add for a 66y/o
COPD patient in Group D, current FEV1<50% predicted,
already taking LAMA/LABA +ICS and has chronic
bronchitis with recurrent exacerbations?
A) Roflumilast
B) Low-dose oral steroid
C) Theophylline
D) Macrolide antibiotic
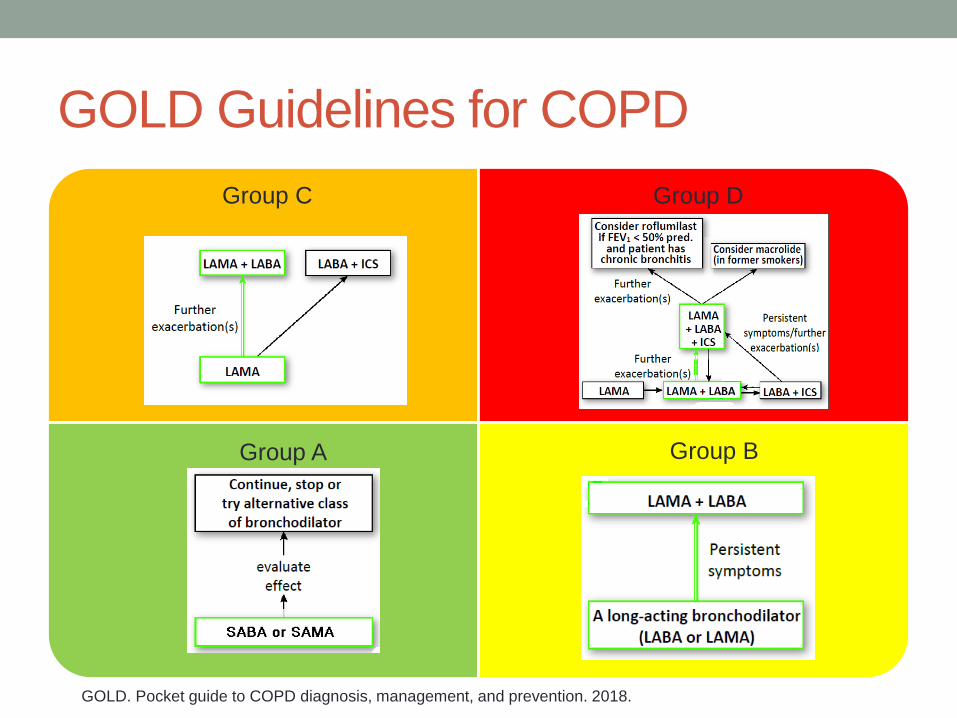
GOLD Guidelines for COPD
Group C
Group A
Group D
Group B
GOLD. Pocket guide to COPD diagnosis, management, and prevention. 2018.
Test your skills #2
What therapy would be the best choice to add for a 66y/o
COPD patient in Group D, current FEV1<50% predicted,
already taking LAMA/LABA +ICS and has chronic
bronchitis with recurrent exacerbations?
A) Roflumilast
B) Low-dose oral steroid
C) Theophylline
D) Macrolide antibiotic
Roflumilast
• Dose = 500mcg orally once a day
• Mechanism of action: PDE4 inhibitor – leads to increased
cAMP in lung cells, reduced neutrophil and eosinophil
count in the lungs
• Contraindicated in moderate-severe liver impairment
• Adverse effects
• Decreased weight
• Diarrhea, nausea
• Backache, headache
• Cost = $375 per month
New inhaler devices
• Ellipta
• Respiclick
• Respimat

Ellipta
• Anoro = LAMA/LABA
(umeclidinium/vilanterol)
• Arnuity = ICS (fluticasone)
• Breo = ICS/LABA
(fluticasone/vilanterol)
• Incruse = LAMA
(umeclidinium)
• Trelegy = ICS/LAMA/LABA
(fluticasone / umeclidinium
/ vilanterol)
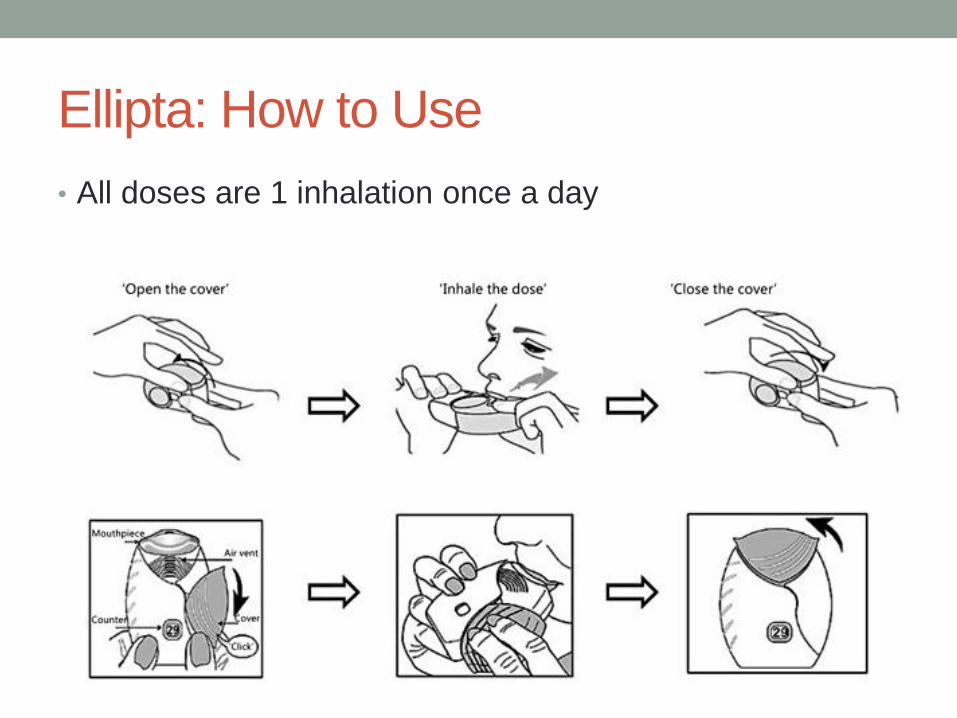
Ellipta: How to Use
• All doses are 1 inhalation once a day
Respiclick
• Armonair = ICS
(fluticasone)
• ProAir = SABA (albuterol)
• AirDuo = ICS/LABA
(fluticasone/salmeterol)
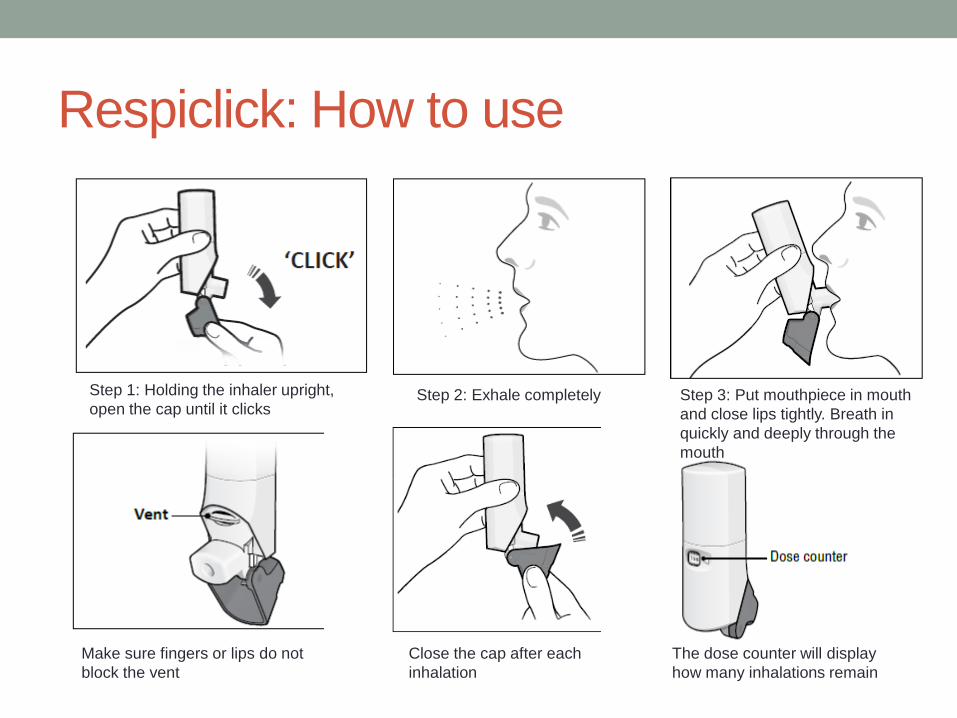
Respiclick: How to use
Step 1: Holding the inhaler upright,
open the cap until it clicks Step 2: Exhale completely Step 3: Put mouthpiece in mouth
and close lips tightly. Breath in
quickly and deeply through the
mouth
Make sure fingers or lips do not
block the vent
Close the cap after each
inhalation
The dose counter will display
how many inhalations remain
Respimat
• Combivent = SAMA/SABA
(ipratropium/albuterol)
• Spiriva = LAMA
(tiotropium)
• Stiolto = LAMA/LABA
(tiotropium/olodaterol)
• Striverdi = LABA
(olodaterol)
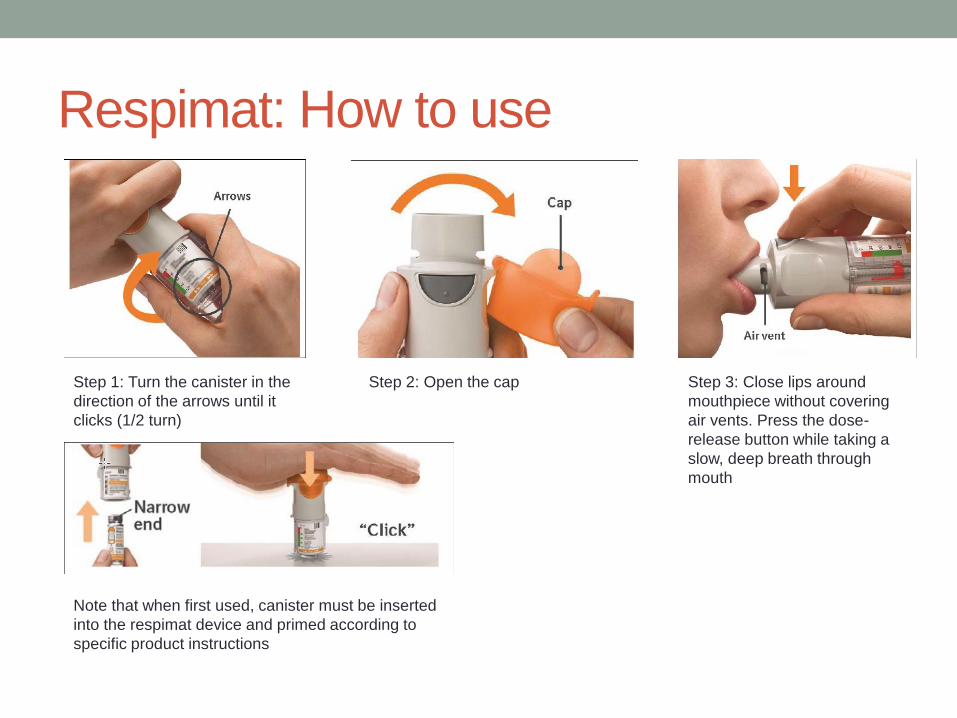
Respimat: How to use
Step 1: Turn the canister in the
direction of the arrows until it
clicks (1/2 turn)
Step 2: Open the cap Step 3: Close lips around
mouthpiece without covering
air vents. Press the dose-
release button while taking a
slow, deep breath through
mouth
Note that when first used, canister must be inserted
into the respimat device and primed according to
specific product instructions
Importance of Verifying Inhaler Technique

NEW CLINICAL TRIALS
Clinical Trials
• AMAZES: Effect of azithromycin on asthma exacerbations
• IMPACT: Effect of once-daily LABA/LAMA/ICS combo vs
LAMA/LABA and LABA/ICS

AMAZES
• N=420 adults with symptomatic asthma despite ICS/LABA
• Exclusion: Polonged QTc, hearing impairment
• Azithromycin 500mg three times per week vs. Placebo
• Duration – 48 weeks
• Primary endpoint: rate of asthma exacerbations
The Lancet 2017 390, 659-668DOI: (10.1016/S0140-6736(17)31281-3)

Results
The Lancet 2017 390, 659-668DOI: (10.1016/S0140-6736(17)31281-3)
NNT = 6
Step 1
Consider low dose ICS
Step 2 Low dose ICS
LTRA or low dose theophylline
Step 3 Low dose ICS / LABA
Medium/high dose ICS, or Low dose ICS + LTRA
Step 4 Medium-high dose ICS / LABA
Add tiotropium, or high dose ICS + LTRA
Step 5 Refer for add-on treatment e.g. tiotropium, anti-IgE, anti-IL-5
Add low dose OCS
2018 GINA Guidelines for Asthma
GINA. Pocket guide for asthma management and prevention. Updated 2018.
Pre
ferr
ed
Co
ntr
oller
Ch
oic
e
Oth
er
co
ntr
olle
r
op
tio
ns
Reliever = PRN SABA
Add
Azithromycin?
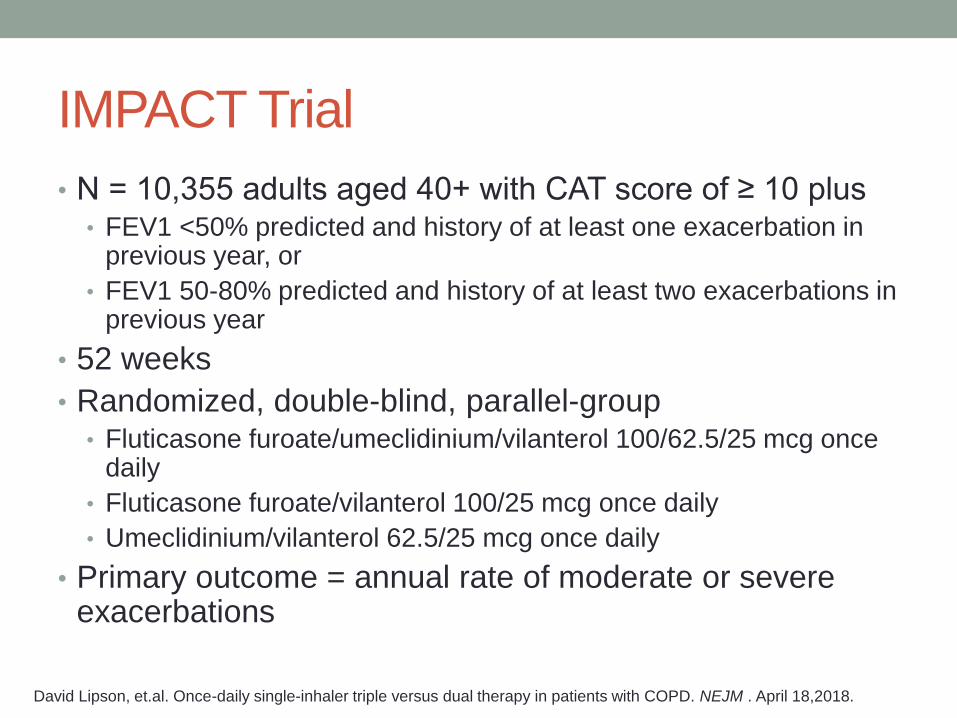
IMPACT Trial
• N = 10,355 adults aged 40+ with CAT score of ≥ 10 plus • FEV1 <50% predicted and history of at least one exacerbation in
previous year, or
• FEV1 50-80% predicted and history of at least two exacerbations in previous year
• 52 weeks
• Randomized, double-blind, parallel-group • Fluticasone furoate/umeclidinium/vilanterol 100/62.5/25 mcg once
daily
• Fluticasone furoate/vilanterol 100/25 mcg once daily
• Umeclidinium/vilanterol 62.5/25 mcg once daily
• Primary outcome = annual rate of moderate or severe exacerbations
David Lipson, et.al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. NEJM . April 18,2018.
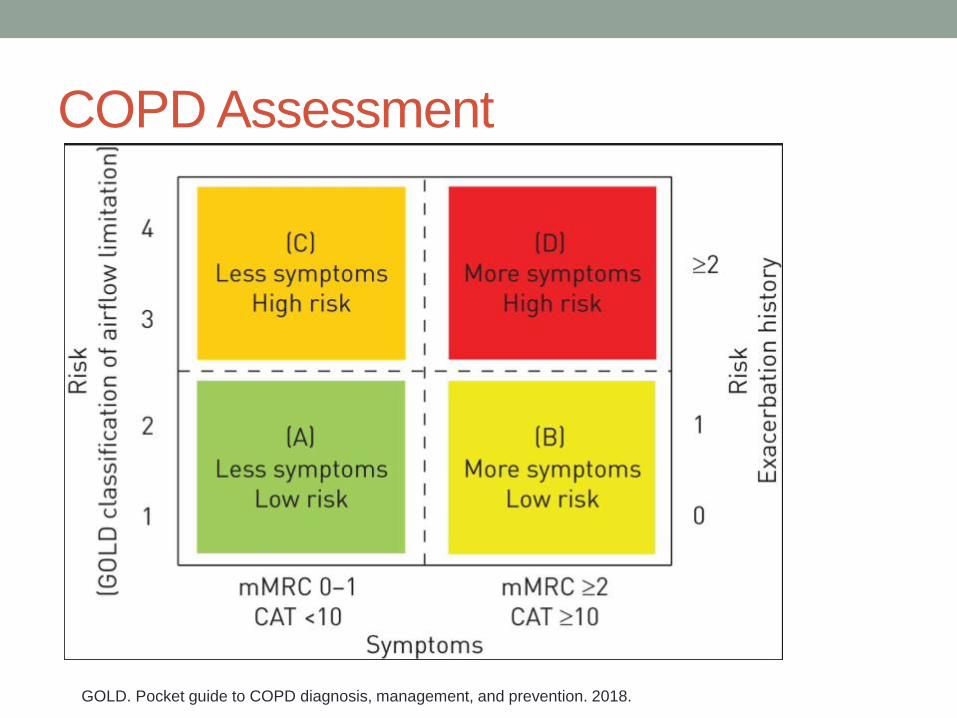
COPD Assessment
GOLD. Pocket guide to COPD diagnosis, management, and prevention. 2018.
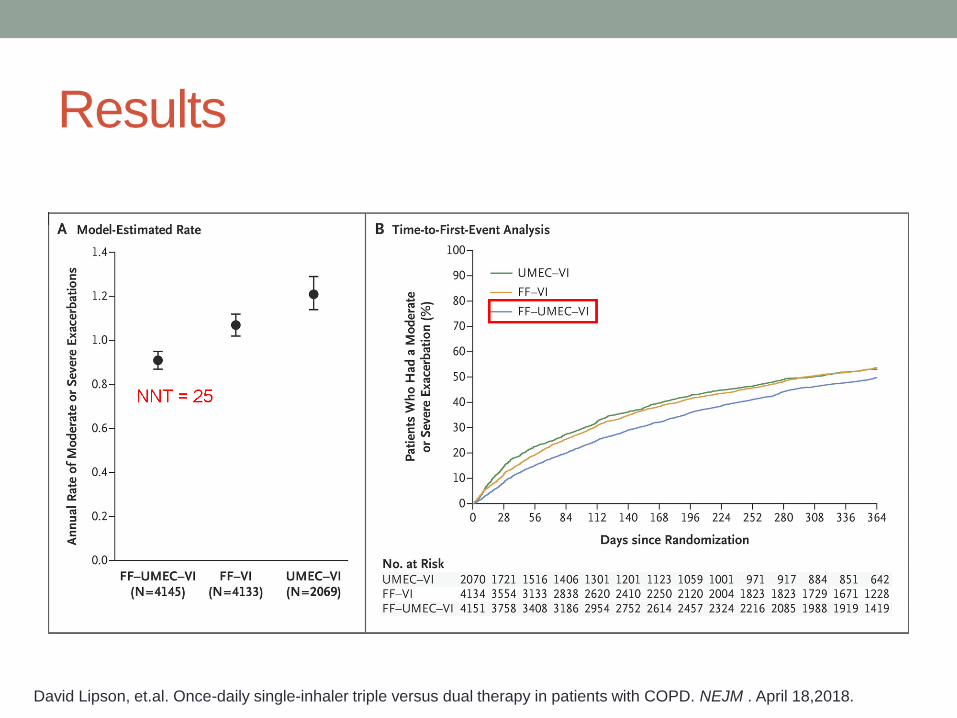
Results
David Lipson, et.al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. NEJM . April 18,2018.
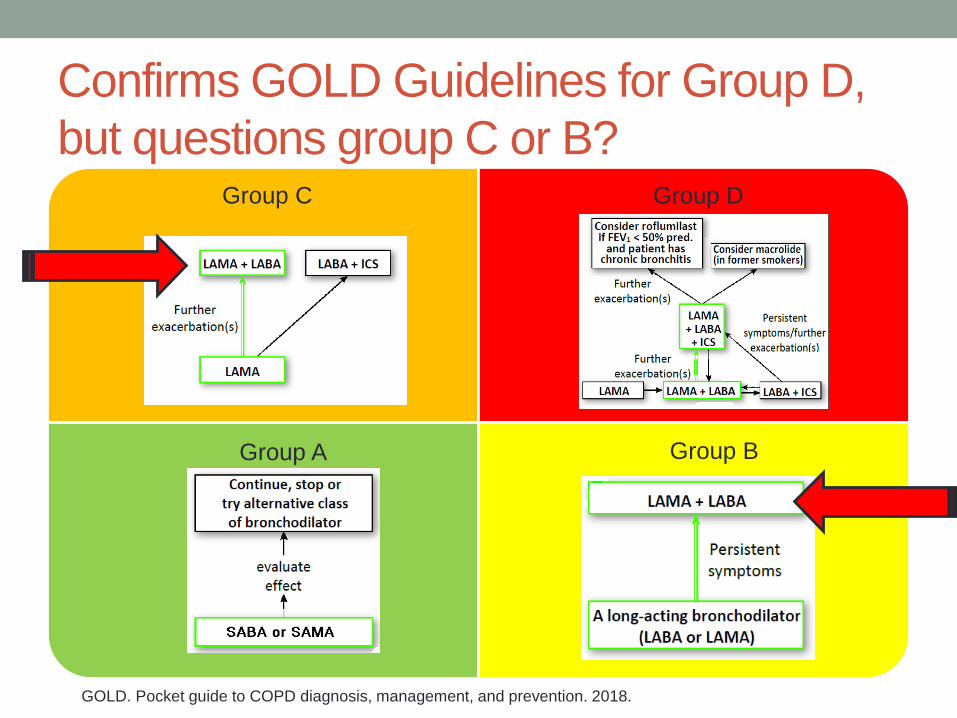
Confirms GOLD Guidelines for Group D,
but questions group C or B?
Group C
Group A
Group D
Group B
GOLD. Pocket guide to COPD diagnosis, management, and prevention. 2018.

Put all the pieces together…patient case
• 48 y/o male with asthma comes to clinic c/o cough
• PMH: Former smoker (quit 3 months ago), HTN, allergic rhinitis. Has had 2 ED visits for asthma exacerbations in last six months
• Current medications: • Symbicort 160/4.5 2 puffs two
times per day (pt admits that he forgets second dose often)
• Albuterol inhaler 2 puffs every four hours as needed (currently using 3-4 times per day)
• Montelukast 10mg daily
• Fluticasone nasal spray 2 sprays each nostril once daily
• Lisinopril 10mg once daily
• Labs:
• ACT = 12
• Eosinophils: 300 cells/µL
• Spirometry: FEV1 = 60%
predicted; FEV1/FVC =
0.68

Patient case continued
• What may be contributing to patient’s symptoms?
• What medication changes would you make?
-ACE inhibitor causing cough?
-Poor inhaler technique/nonadherence?
-Undiagnosed COPD?
-Eosinophilia?
-Add LAMA?
-Switch Symbicort to once daily ICS/LABA?
-Educate on proper inhaler technique?
-Switch lisinopril to ARB?
-Add anti-IL5?
-Add Azithromycin 500mg three times a week?
Apply this to your practice…
• New treatments for asthma include tiotropium, biologics
• New inhaler devices include Respimat, Respiclick and
Ellipta
• AirDuo is first generic ICS/LABA
• Trelegy Ellipta – first once daily triple therapy
(ICS/LABA/LAMA) for COPD
• In future, watch for biologics to be approved for COPD
and possibly macrolide antibiotics for asthma