Updated recommendations for control of surgical site infections
51
Recommendations for Control of Surgical Site Infections DR. MUHAMMAD JAWAD PGT – I Surgical Unit – III Services Hospital, Lahore
-
Upload
muhammad-jawad -
Category
Healthcare
-
view
137 -
download
0
Transcript of Updated recommendations for control of surgical site infections
Recommendations for Control of
Surgical Site Infections
DR. MUHAMMAD JAWAD
PGT – I
Surgical Unit – III
Services Hospital, Lahore

OBJECTIVE
• to provide updated guidelines for the prevention of surgical wound infections based upon review and interpretation of the current and past literature

Surgical Site Infection CDC defines • A surgical site infection is an infection that
occurs after surgery in the part of the body where the surgery took place. Surgical site infections can sometimes be superficial infections involving the skin only. Other surgical site infections are more serious and can involve tissues under the skin, organs, or implanted material.

Criteria for defining SSIs
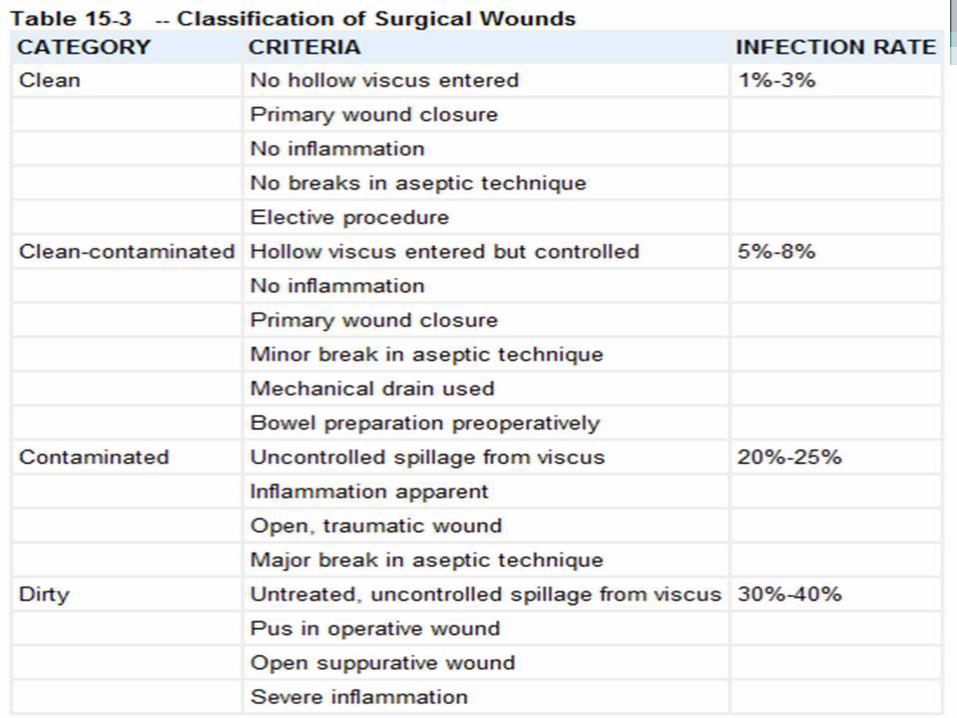

Classification Of Surgical Wounds
According to Risk of Infection• a. CLEAN WOUND (I):
• 1.5 – 5.4% infection rates
• Elective cases, primarily closed and undrained
• Nontraumatic, uninfected, no inflammation
• No break in asepsis
• Respiratory, alimentary, genitourinary or oropharyngeal tracts not entered
• Hernia repair, breast biopsy

• B. CLEAN – CONTAMINATED WOUND:
• 2.1 – 9.5% infection rate
• Alimentary, respiratory, genito-urinary tract entered under controlled conditions and w/o unusual contamination
• Minor break in technique
• Mechanical drainage
• Appendectomy, biliary tract
• C. CONTAMINATED WOUND
• 3.4 – 13.2% infection rates
• Open, fresh traumatic wound
• Gross spillage from gastrointestinal tract
• Entrance of genitourinary or biliary tracts in presence of infected urine and bile
• Major break in technique
• Penetrating abdominal trauma, large tissue injury, enterotomy during bowel obstruction

• D. DIRTY AND INFECTED WOUND
• 28 – 40% infection rates
• Traumatic wound with retained devitalized tissue, foreign bodies, fecal contamination or delayed treatment
• Perforated viscus encountered
• Acute bacterial inflammation with pus encountered during operation

Surgical site infections • Surgical site infections
have been shown to
compose up to 20%
of all of healthcare-
associated infections.
At least 5% of patients undergoing a surgical
procedure develop a
surgical site infection
Risk Factors for SSI: The Patient
• Age• Nutritional status• Diabetes• Nicotine use• Obesity• Coexistent infection• Colonization• Altered immune response• Long preoperative stay
Dr.T.V.Rao MD11
UPDATED RECOMMENDATIONS FOR
CONTROL OF SURGICAL SITE
INFECTIONS
• J. WESLEY ALEXANDER
• JOSEPH S. SOLOMKIN
• MICHAEL J. EDWARDS
• Annals of Surgery Vol 253, Number 6, June 2011
• REDUCTION IN CONTAMINATION
(ASEPSIS)

OPERATING ROOM ENVIRONMENT
• Microbes in the air of the operating room
• High efficiency particulate air (HEPA) filters provide the best environment
• Limiting traffic and idle conversations in the operating room (OR) are essential
• perforation of surgical gloves• The risk of infection with glove perforation was significantly greater in
those procedures in which no antimicrobial prophylaxis was given.

PREOPERATIVE BATHING WITH ANTISEPTIC
AGENTS

• Preoperative showering with chlorhexidine has been shown to reduce the number of organisms at the incision site better than using povidoneiodine or soap and water
• Additional use of a cloth impregnated with chlorhexidine
• recent meta-analyses - nonsignificant reduction in wound infections in large numbers of patients

HAIR REMOVAL
• incidence of wound infection would increase when hair gets into a surgical wound
• evidence suggests that not removing hair is associated with the least infection.
• When deemed by the surgeon that hair should be removed, shaving should never be used.
• Clipping the hair with care the most satisfactory method
• studies support hair removal done immediately before operation

SKIN DECONTAMINATION
• Hand scrubs of 2 to 3 minutes using a chlorhexidine/alcohol based product
• best reduction in microbes - with an iodine povacrylex/alcohol (4.8%) or chlorhexidine/alcohol-based products(8.2%).
• The only randomized trial - >40% reduction in total SSIs among patients undergoing clean-contaminated surgery who had received a single chlorhexidine-alcohol scrub v/s povidone-iodine scrub
INCISE DRAPES


• used for at least 50 years.
• Adhesiveness to the skin has been shown to improve with an initial alcohol or tincture of iodine solution prep of the skin
• This type of drape application is also cost effective when compared to skin preparation with povidone iodine alone.

REDUCTION IN CONSEQUENCES OF
CONTAMINATION
(ANTISEPSIS)

SUTURES
• a variety of suture materials impregnated with antibacterial substances and antibiotics including triclosan, silver, gentamicin and neomycin; have shown the feasibility of reducing bacterial counts in wounds.

Nonrandomized Observational Study
• - 2088 operations - wound infection rate
0.00%
2.00%
4.00%
6.00%
8.00%
10.00%
12.00%
Antibacterial Non- AB
• Continuous sutures of the same material > fewer infections than interrupted sutures,
possibly because of
reduction in tissue necrosis at suture sites , more even distribution of tension
less suture material is left in the wound

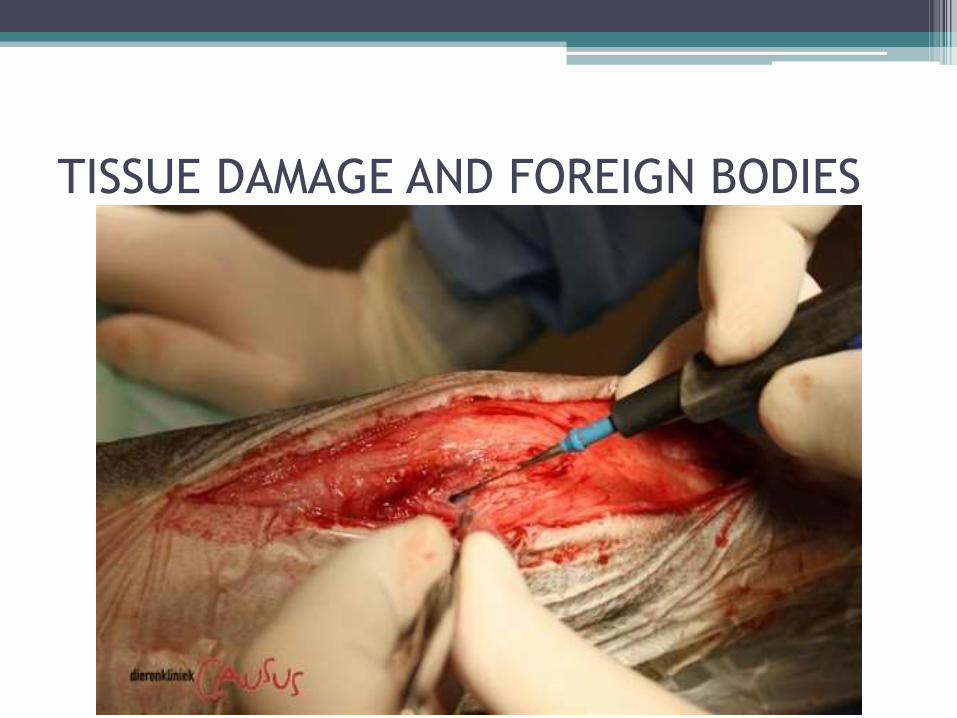
TISSUE DAMAGE AND FOREIGN BODIES

• Frequent use of electrocautery for opening of wounds > may increase the incidence of infection
• expert consensus > use primarily for pinpoint treatment of bleeders
• obliteration of all potential dead spaces is effective

DRAINS
• Closed suction drainage > useful when production of large amounts of subcutaneous fluid is expected (such as abdominoplasty) or to detect leaks.
• Drains have been used effectively to instill local antibiotics at the end of operations.
• No benefit of the use of closed suction drains in specific types of operations including
colorectal surgery , uncomplicated liver resection,laparoscopic cholecystectomy, uncomplicated open cholecystectomy, abdominal surgery, gastric bypass surgery , incisional hernia repair , ascular surgery ,
thyroid procedures, meian sternotomy , and tissue expander implant

PROPHYLACTIC TOPICAL
ANTIMICROBIALS• topical irrigation of wound with an antibiotic is
more effective when the type of topical antibiotic is different from the systemic antibiotic being given, with evidence that they are additive.
• TIMING is crucial
• NO deep 30 day SSI when irrigation with kanamycin every 4.7 minutes throughout operative procedure v/s 0.73% without antibiotic lavage
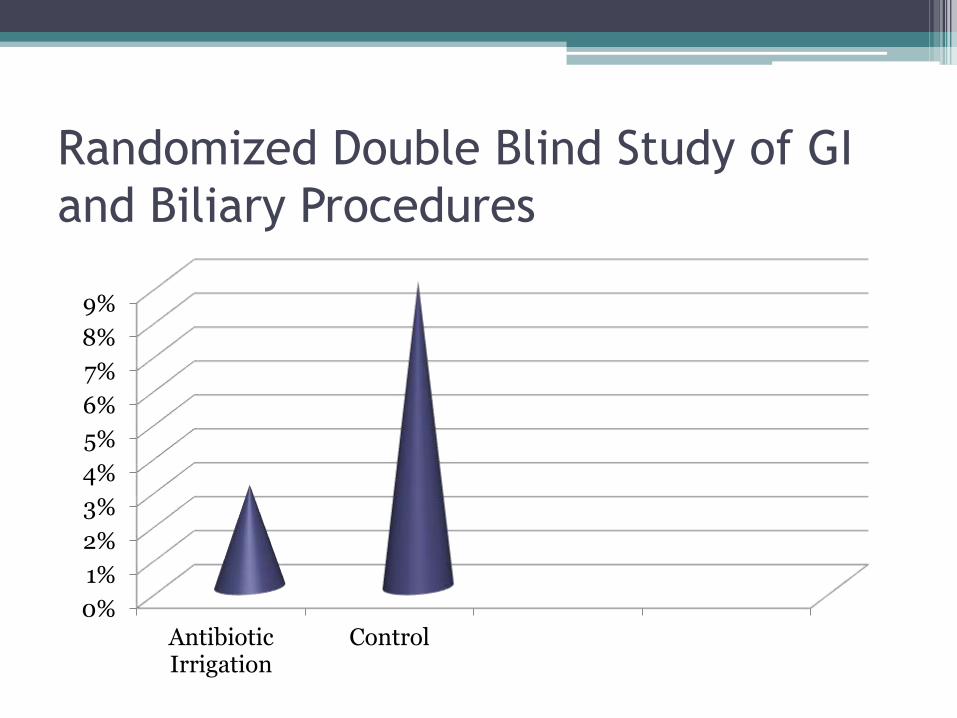
Randomized Double Blind Study of GI
and Biliary Procedures
0%
1%
2%
3%
4%
5%
6%
7%
8%
9%
AntibioticIrrigation
Control

Irrigation with Penicillin in 368 Clean
General Surgical Procedures
0.00%
0.50%
1.00%
1.50%
2.00%
2.50%
3.00%
3.50%
AntibioticIrrigation
(0.27)
No Antibiotic

In a More Recent Study
• In Gastric Bypass surgery of morbidly obese patients, Kanamycin in sub-cutaneous wound for 2 hours
>out of 772 patients
only ONE primary deep SSI (0.13%)
TWO secondary deep infections
SYSTEMIC PROPHYLACTIC ANTIBIOTICS
• A recent “meta-analysis of meta-analyses”
a generalized benefit regardless of the degree
of contamination

Timing of Administration
• preoperative administration of antibiotics were superior to postoperative administration
• “golden period” - in first 2 hours before surgery

Modifying Factors
• renal function, (clindamycin, metronidazole)
• body weight, (higher dose)
• half-life of the antibiotic,
• Use of cardiopulmonary bypass,
• use of transfusions for blood loss,
• Aggressive fluid therapy,
• patient age, and
• rate of diffusion into the wound.

Selection of Drugs for Prophylaxis
• based on having effective levels of the antimicrobial present throughout the operative period from skin incision to closure, and in some settings, one or two postoperative doses.
• Clindamycin and Vancomycin

WOUND CLASSIFICATION
ANTIBIOTIC PENICILLIN ALLERGY
I 1ST GENERATIONCEPHALOSPORIN
VANCOMYCIN CLINDAMYCIN
II – BILIARY, GU, UPPER GI
1ST GENERATIONCEPHALOSPORIN
VANCOMYCIN CLINDAMYCIN
II – LOWER GI 2ND GENERATION CEPHALOSPORIN
AZTREONAM CLINDAMYCIN/FLAGYL
III/IV GENERALLY THERAPEUTIC
• Once the incision is made, antibiotic delivery to the wound is impaired.
Must give before incision!
IMPROVEMENT OF HOST DEFENSE
INFLUENCE OF BODY TEMPERATURE• Mild hypothermia in the range of 34 to 36◦C -
large
number of adverse effects
• increased blood loss and transfusion requirements
• prolonged pos-tanesthesia recovery
• prolonged hospitalization
• morbid myocardial events
• increase in wound infections

• local warming with radiant heat was as good as systemic warming in preventing SSI
• Hypothermia -> SSI (RR 6.3)

WHY..??
• Generalized vasoconstriction
• Dec. subcutaneous blood flow and oxygen
• Antibody & Cell-mediated immune defenses

GLUCOSE CONTROL
• Surgical patients with Diabetes > increased incidence of major complications
0.00%
2.00%

• Protocols to keep blood glucose levels between 120 and 160 mg/dL for the first 2 - 3 days postoperatively have resulted in a reduction of DSWI to levels comparable to non-diabetic patients

WHY..??
• Hyperglycemia leads to
• disturbances of microvascularresponses• inhibition of complement function• Increase in proinflammatory cytokine levels and
some chemokines• Inhibition of chemotaxins• impaired phagocytosis and intracellular killing
(especially by PMNs)• disturbances in reactive oxygen species• decrease in T and B cell responses

• Catecholamines,
• growth hormones, and
• corticosteroids
are all increased by hyperglycemia,
all inhibiting O2 delivery to wounds.

DELAYED PRIMARY CLOSURE
• strong indication for delayed primary closure was in wounds involving the intestine
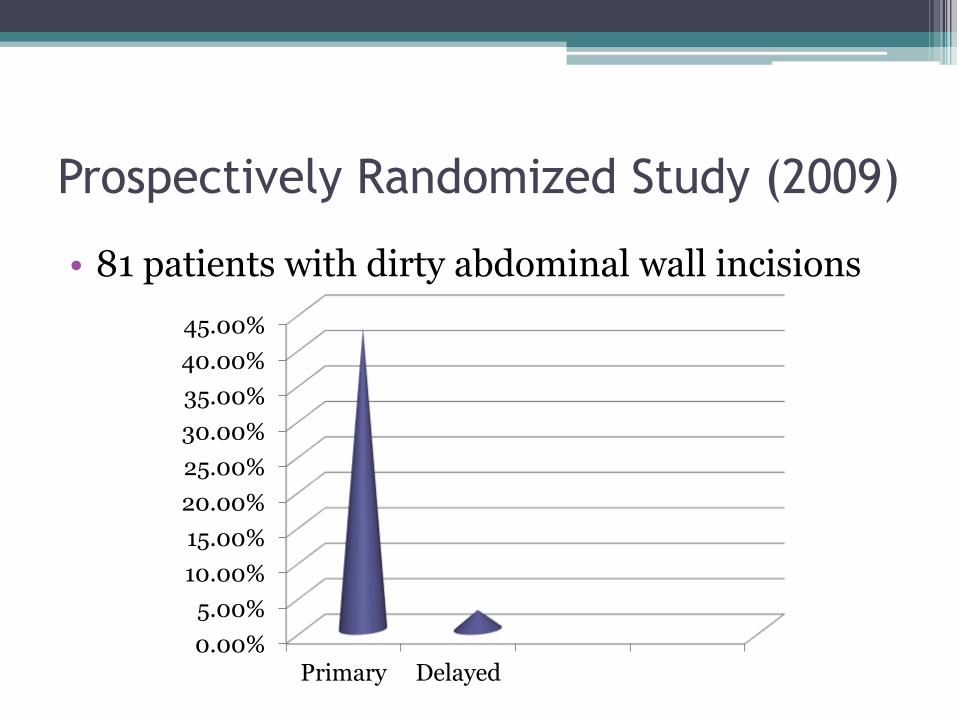
Prospectively Randomized Study (2009)
• 81 patients with dirty abdominal wall incisions
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
40.00%
45.00%
Primary Delayed

THANK YOU FOR YOUR PATIENCE