
Update su terapie targeted e immunologiche del melanoma
49
Update su terapie targeted e immunologiche del melanoma Francesco Spagnolo IRCCS Ospedale Policlinico San Martino
Transcript of Update su terapie targeted e immunologiche del melanoma

Update su terapie targeted e
immunologiche del melanoma
Francesco Spagnolo
IRCCS Ospedale Policlinico San Martino

Melanoma avanzato oggi (pratica clinica)
• Espressione PD-L1 non richiesta per trattamento con anti-PD-1
• Indicazione al trattamento fino a progressione o tossicità inaccettabile
• Ritrattamento/Rechallenge non rimborsabile
• Nivolumab+ipilimumab non rimborsabile
Genomic Classification of Cutaneous Melanoma The Cancer Genome Atlas Network. Cell 2015 Biomarkers

Robert et al. NEJM 2019

Robert et al. NEJM 2019

Robert et al. NEJM 2019


COLUMBUS PHASE 3 TRIAL: UPDATED OVERALL SURVIVAL
ASCO 2019
39%
25%
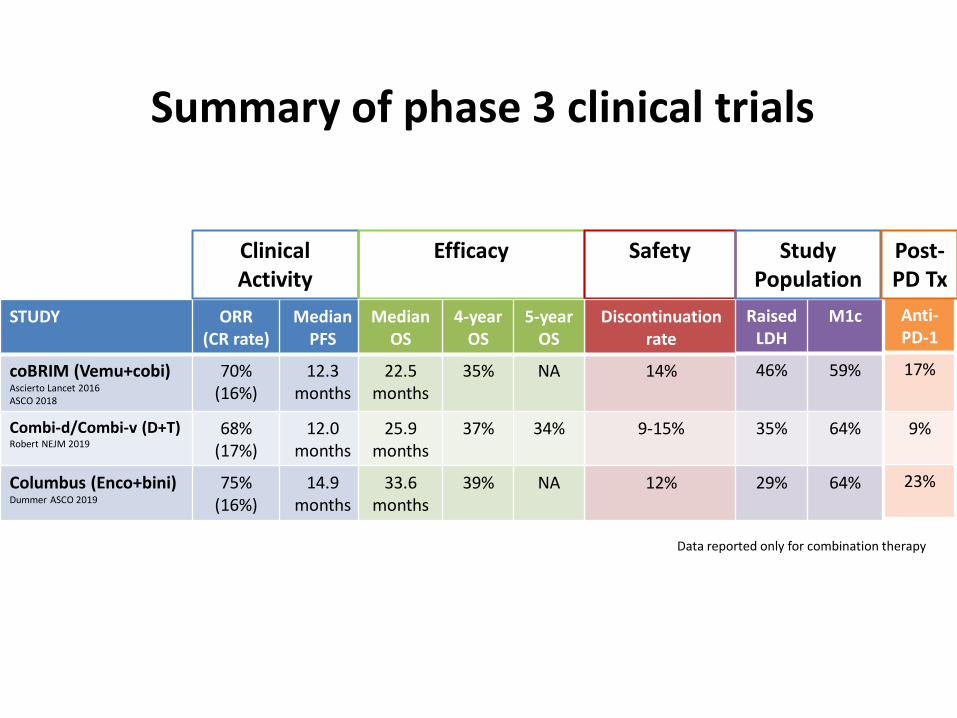
STUDY ORR (CR rate)
Median PFS
coBRIM (Vemu+cobi) Ascierto Lancet 2016 ASCO 2018
70% (16%)
12.3 months
Combi-d/Combi-v (D+T) Robert NEJM 2019
68% (17%)
12.0 months
Columbus (Enco+bini) Dummer ASCO 2019
75% (16%)
14.9 months
Data reported only for combination therapy
Summary of phase 3 clinical trials
Clinical Activity
Efficacy
Safety
Discontinuation rate
14%
9-15%
12%
Median OS
4-year OS
5-year OS
22.5 months
35% NA
25.9 months
37% 34%
33.6 months
39% NA
Raised LDH
M1c
46%
59%
35%
64%
29% 64%
Study Population
Anti-PD-1
17%
9%
23%
Post-PD Tx

Most Frequent adverse events - Summary
Drug Adverse Event
Dabrafenib+Trametinib (Combi-d)
Fever (51%)
Fatigue (35%)
Headache (30%)
Nausea (30%)
Chills (30%)
Vemurafenib+Cobimetinib (CoBrim)
Diarrhea (56%)
Nausea (40%)
Rash (38%)
Photosensitivity (28%)
Vomiting (21%)
Encorafenib+Binimetinib (Columbus)
Nausea (42%)
Diarrhea (37%)
Vomiting (30%)
Arthralgia (26%)
CPK increased
(23%)
• Some toxicities are common to all BRAF+MEK inhibitors combos • Photosensitivity and diarrhea are common with
vemurafenib+cobimetinib but rare with dabrafenib+trametinib, while fever and chills are common with dabrafenib+trametinib
The type and severity of these toxicities vary considerably and may influence choice of drug

Robert et al. Lancet Oncol
2019
5 y OS: 39%
4 y PFS: 23%
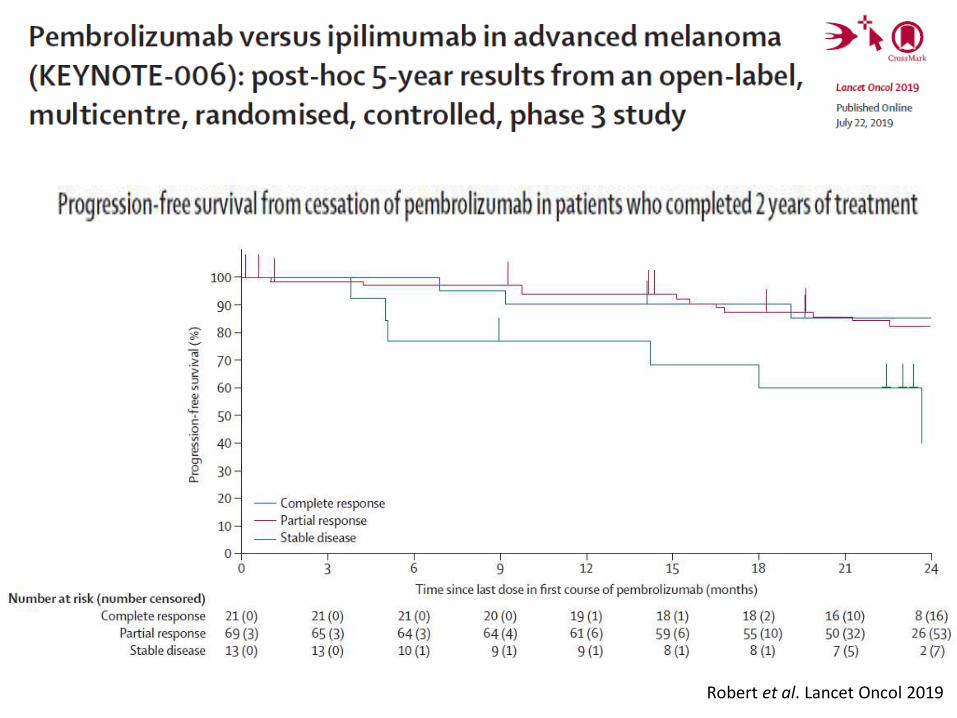
Robert et al. Lancet Oncol 2019
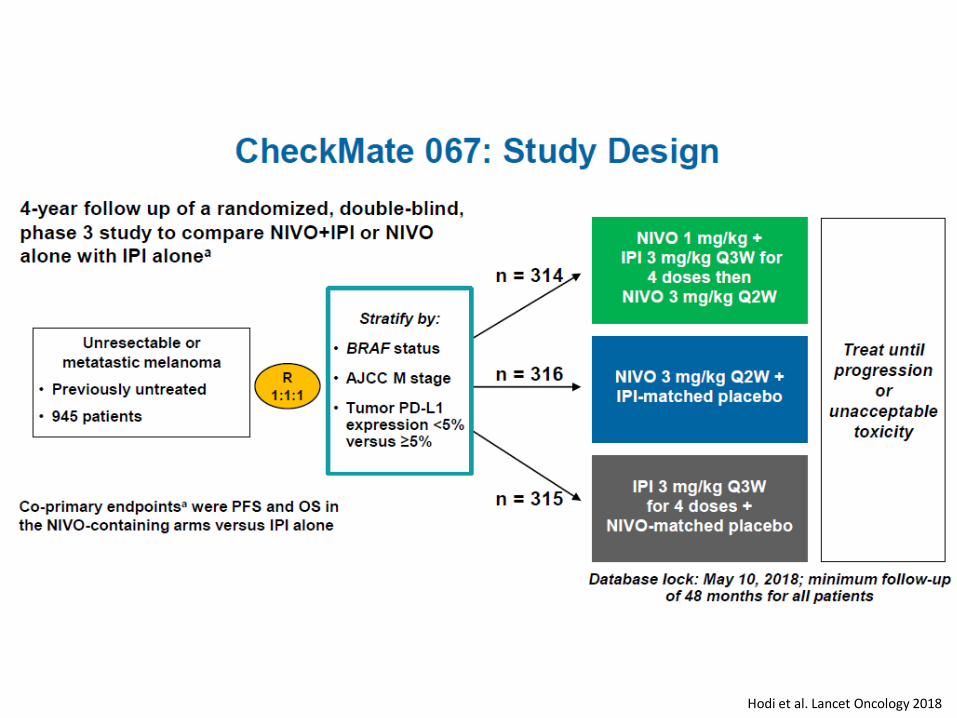
Hodi et al. Lancet Oncology 2018

53%
46%
30%
58%
51%
34%
37%
31%
9%
39%
32%
10%
Hodi et al. Lancet Oncology 2018

Lebbè et al. JCO 2019

Lebbè et al. JCO 2019

CheckMate-067 Higher survival plateau
Targeted therapy Higher early benefit
53%
46%
30%
Hodi et al. Lancet Oncology 2018
58%
51%
34%

Ascierto et al. Nature Medicine 2019

• More patients had grade 3-4 treatment-related AE
• ORR was similar in the two arms, but more CR were observed in the experimental arm
• The duration of response was longer
• PFS did not reach statistical significance due to the small sample size (i.e. study was underpowered)
• In terms of PFS, triplet combination did better compared to targeted therapy alone in patients with poor prognostic features
• At a median follow-up of 9.6 months, no significant differences in OS were noted
WHAT WE HAVE LEARNT FROM KEYNOTE-022 TRIAL
Ascierto et al. Nature Medicine 2019

ONGOING PHASE III
TRIALS WITH «TRIPLETS»
IN BRAF-MUTANT PATIENTS
COMBI-I
TRILOGY

Sequential Combo Immuno and Target Therapy Study (SECOMBIT)
EORTC-1612-MG: Immunotherapy With Ipilimumab and Nivolumab Preceded or Not by a Targeted Therapy With
Encorafenib and Binimetinib (EBIN)
Patients with BRAF-
Mutant Melanoma
n=270
Primary endpoint: OS
Primary endpoint: PFS
Randomization
Nivolumab + low-dose ipilimumab q3w for 4 injections
Nivolumab 480 mg q4w for 2 years or until PD
Encorafenib 450 mg QD + binimetinib 45 mg BID for 12 weeks
Nivolumab + low-dose ipilimumab q3w for 4 injections
1 week
Nivolumab 480 mg q4w for 2 years or until PD
EVALUATION OF TARGETED
THERAPY IN SEQUENCES WITH IMMUNOTHERAPY

Targeted therapy plus immunotherapy in patients with brain metastases
TRICOTEL Trial: Study design

Overview of recent adjuvant trials
Study
Patients
N
Stage
Primary
Endpoint
Treatment
Experimental
arm
Control Duration
CA184-029/
EORTC 18071
1211 IIIA (>1
mm)/IIIB/IIIC
RFS Ipilimumab Placebo 3 years
COMBI-AD 852 IIIA (>1
mm)/IIIB/IIIC
RFS Dabrafenib +
trametinib
Placebo 1 year
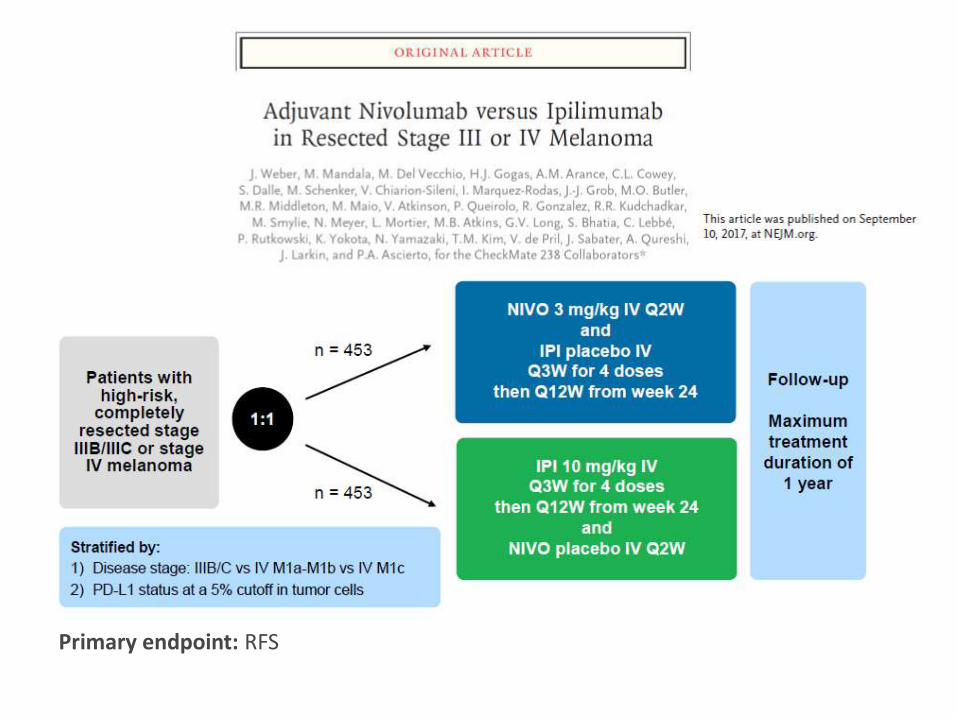
CA209-238 800 IIIB/IIIC/
resected IV
RFS Nivolumab Ipilimumab 1 year
KEYNOTE-054 900 IIIA (>1
mm)/IIIB/IIIC
RFS Pembrolizumab Placebo 1 year
Approved by the FDA in 2017 and EMA in 2018
Approved by EMA in 2018 and the FDA in 2019
Approved by the FDA in 2015
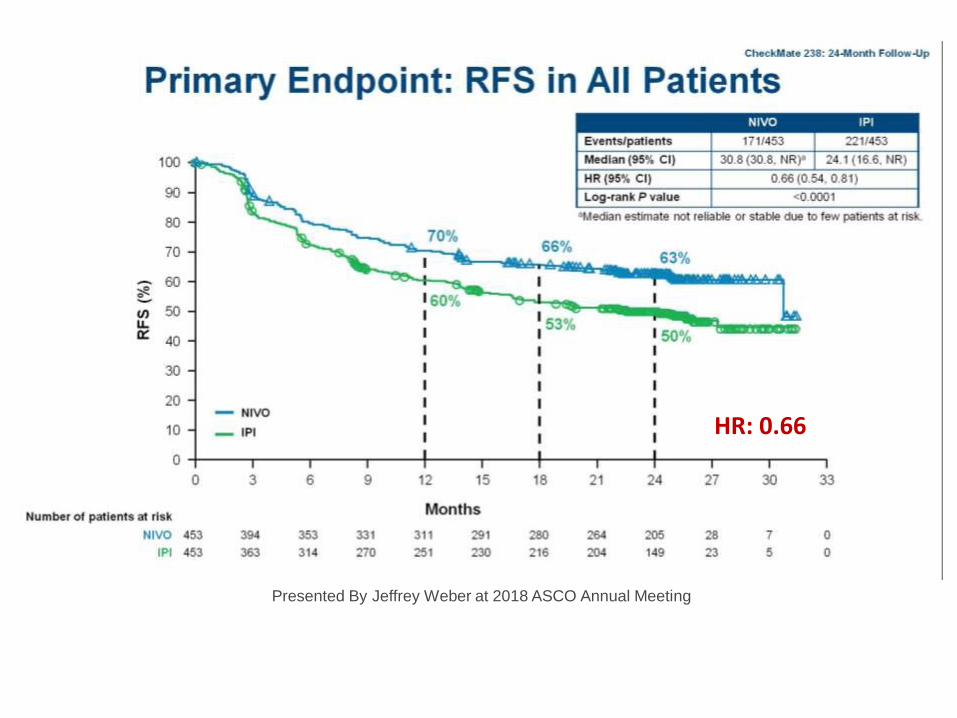
Primary endpoint: RFS
Slide 7
Presented By Jeffrey Weber at 2018 ASCO Annual Meeting
HR: 0.66

Subgroup Analysis of RFS: 5% PD-L1 Expression Level
Presented By Jeffrey Weber at 2018 ASCO Annual Meeting

Subgroup Analysis of RFS: BRAF Mutation Status
Presented By Jeffrey Weber at 2018 ASCO Annual Meeting

Subgroup Analysis of RFS: Disease Stage III and IV
Presented By Jeffrey Weber at 2018 ASCO Annual Meeting

Keynote 054: Pembrolizumab vs Placebo

Eggermont et al. NEJM 2018
75.4%
61.0%
71.4%
53.2%
RFS HR: 0.57

Eggermont et al. NEJM 2018
DMFS HR: 0.53

Checkmate-915
Primary Endpoint: DFS Emendamento per sample size fino a 2000 pazienti

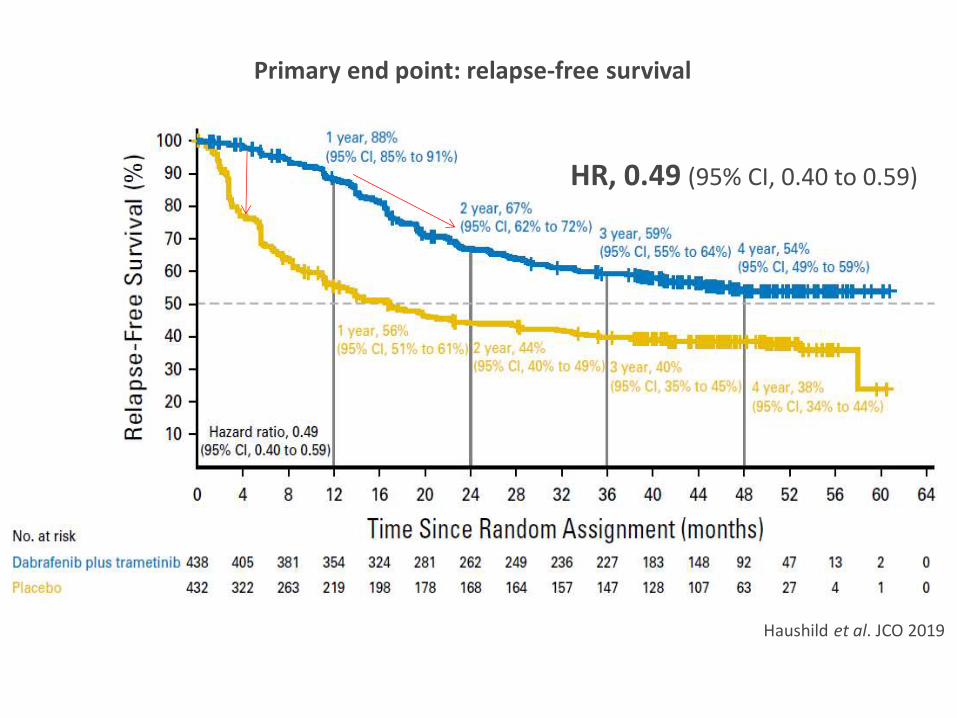
Primary end point: relapse-free survival
Haushild et al. JCO 2019
HR, 0.49 (95% CI, 0.40 to 0.59)

Stage IIIA Stage IIIB
Stage IIIC Stage IIID
Haushild et al. JCO 2019 Relapse-free survival by stage (8th ed.)

Secondary end point: overall survival
Long et al. NEJM 2017
86%
77%
91%
83%
97%
94%
Δ=3% Δ=8%
Δ=9%

Adjuvant setting: summary
Study Treatment Stage HR for RFS HR for OS
Interferon meta-analysis
Interferon different regimens
IIB -> IIIC 0.82 vs placebo
0.89
CheckMate-029
Ipilimumab Placebo
IIIA (>1 mm)/IIIB/IIIC
0.76 vs placebo
0.72
CheckMate-238
Nivolumab Ipilimumab
IIIB/IIIC/resected IV 0.65 vs ipilimumab
Not available
Keynote-054 Pembrolizumab Placebo
IIIA (>1 mm)/ IIIB/IIIC
0.57 vs placebo
Not available
Combi-AD Dabrafenib+trametinib Placebo
IIIA (>1 mm)/ IIIB/IIIC
0.49 vs placebo
0.57

Eggermon et al. Nature Reviews Clinical Oncology 2018
Kaplan–Meier curves of estimated RFS in key trials of adjuvant therapies
for melanoma

Melanoma adjuvant setting
Stage IIB/C
Ulcerated primary
Non-ulcerated primary
Interferon Observation

Efficacy of interferon by ulceration
Ives et al. European Journal of Cancer 2017
HR: 1.02 (CI 0.87-1.20)
HR: 0.77 (CI 0.64-0.92)


Melanoma adjuvant treatment
Stage IIB/C
Ulcerated primary
Non-ulcerated primary
Interferon Observation
Stage III
BRAF V600 BRAF wild-
type
BRAF+MEKi Anti-PD-1
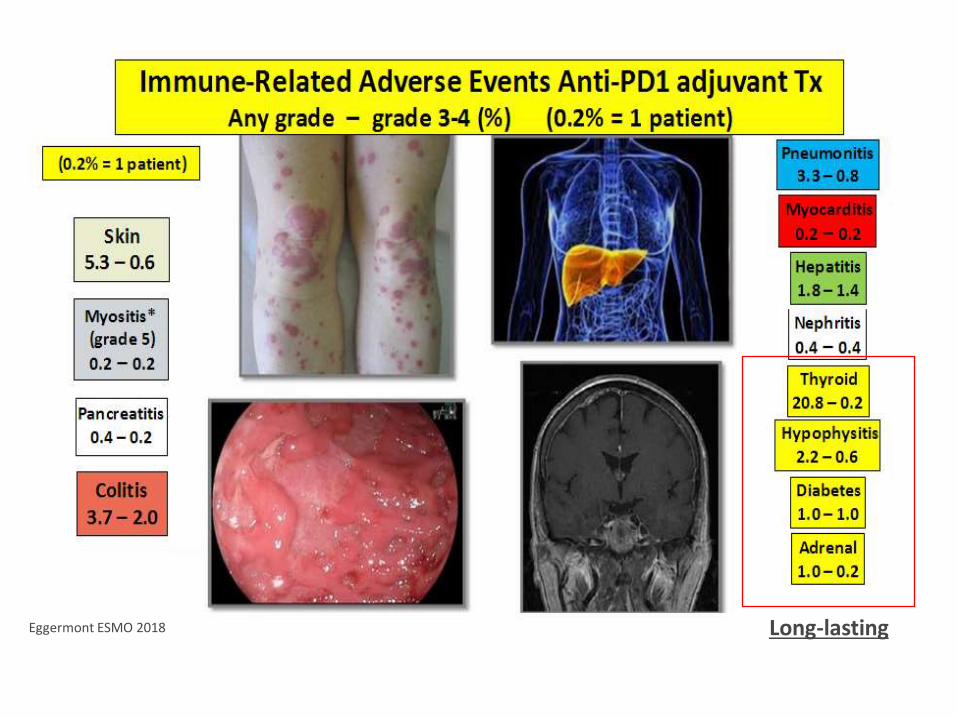
Long-lasting Eggermont ESMO 2018

Verver et al. EJC 2018 Van Akkoi et al. Ann Surg 2008
Low burden stage III disease

Melanoma adjuvant treatment
Resected Stage IV
Anti-PD-1
Stage IIB/C
Ulcerated primary
Non-ulcerated primary
Interferon Observation
Stage III
BRAF V600 BRAF wild-
type
BRAF+MEKi Anti-PD-1

Why shall we go for neoadjuvant therapy?
1) Therapy efficacy can de determined within the individual patient for possible additional adjuvant therapy
2) Reduce tumor burden before surgery
3) Utilize pathological response data as surrogate outcome
markers for relapse free and overall survival 4) In the case of T cell checkpoint blockade neoadjuvant therapy
could induce stronger and broader tumor-specific T cell response


Amaria et al. Lancet Oncology 2018
Relapse-free survival
Distant metastasis-free survival
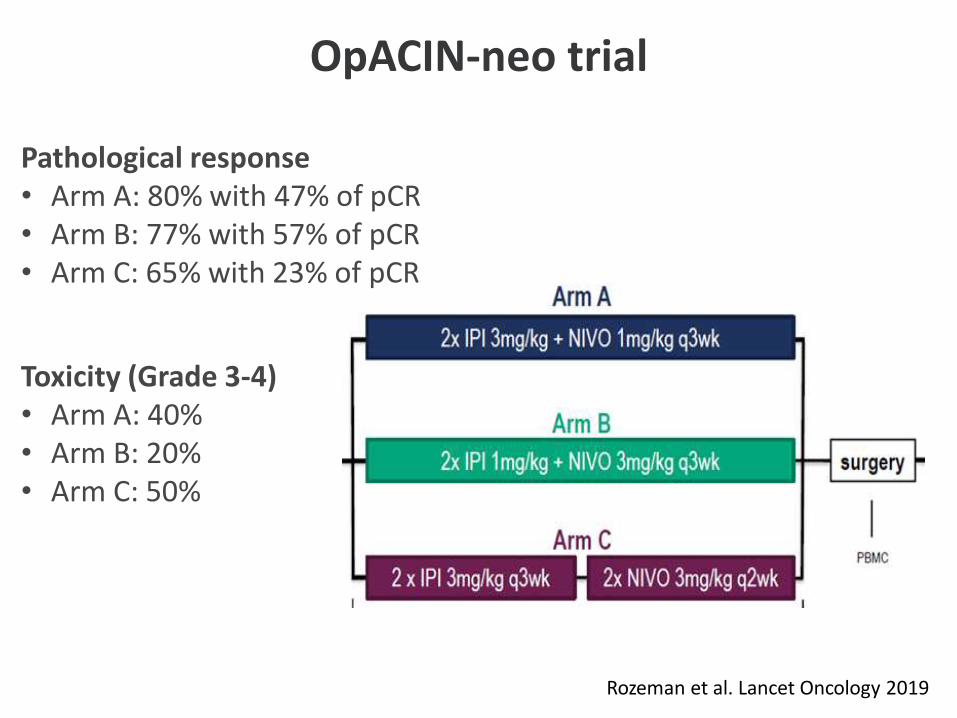
OpACIN-neo trial
Pathological response • Arm A: 80% with 47% of pCR • Arm B: 77% with 57% of pCR • Arm C: 65% with 23% of pCR
Toxicity (Grade 3-4) • Arm A: 40% • Arm B: 20% • Arm C: 50%
Rozeman et al. Lancet Oncology 2019

• IPI+NIVO: ORR 73%, pCR 45%, toxicity 73% grade 3 trAEs)
• NIVO: ORR 25%, pCR 25%, toxicity 8% grade 3 trAEs.
Neoadjuvant and Adjuvant Checkpoint Blockade in Patients With Clinical Stage III or Oligometastatic Stage IV Melanoma
Amaria et al. Nat Med 2019


















