Constanza Carolina Carrillo Ballesteros - Universidad de Chile
Upload
shaylee-fairchildCategory
view
213download
0
Update on HIV and infant feeding
Update on HIV and infant feeding
Peggy Henderson and Constanza Vallenas
Department of Child and Adolescent Health and Development, WHO
Rome, 25 February 2007

2 |
UN RecommendationsUN Recommendations
HIV- women or HIV status unknown
Exclusive breastfeeding for 6 months and continued breastfeeding for 2 years or beyond
HIV+ women
Most appropriate infant feeding option for HIV-exposed infant depends on individual circumstances, including consideration of health services, counselling and support

3 |
Selecting an option:AFASS
Selecting an option:AFASS
To be a better option for the individual than exclusive breastfeeding, replacement feeding has to be AFASS:
Acceptable
Feasible
Affordable
Sustainable AND
Safe
For the mother and baby

4 |
Balancing risksfor HIV-positive women
Balancing risksfor HIV-positive women
HIV transmission
IF BREASTFEEDING
Mortality Infectious diseasesMalnutrition
IF NOT BREASTFEEDING

5 |
Balancing risks - 1 HIV transmission
Balancing risks - 1 HIV transmission
Risk of HIV transmission with full package of MTCT prevention Interventions (HAART, replacement feeding, caesarean section) < 2%
Risk of HIV transmission through breastfeeding:
Exclusive breastfeeding (6 weeks – 6 months) ~ 4%
Breastfeeding as usual (varying duration) 5 to 20%

6 |
1
2
3
4
5
6
7
<2 m 2 - 3 m 4 - 5 m 6 - 8 m 9 - 11 m
Rela
tive r
isk
Age (months)
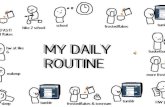
WHO Collaborative Study Team, Lancet, 2000
Balancing risks – 2Relative risk of infectious disease mortality
among non-breastfed infants
5.8
4.1
2.6
1.81.4

7 |
1
3
5
7
9
11
13
BF+formula BF+solids EBF
Haz
ard
rat
io
Coovadia et al., Lancet, in press
Balancing risks – 3Mixed feeding carries higher risk of HIV transmission
than exclusive breastfeeding

8 |
Balancing Risks - 4No Difference in 18-Month mortality/HIV infection
between Formula and Breastfed Infants
Balancing Risks - 4No Difference in 18-Month mortality/HIV infection
between Formula and Breastfed Infants
13.9%12.5%8.9%
15.1%12.9%
6.1%
0%
10%
20%
30%
1 Month 7 Months 18 MonthsInfant age
Formula Breast + AZT
p=0.60p=0.86
p=0.08
FF: 33 infected, 62 deathsBF: 53 infected, 48 deaths
% H
IV-I
nfe
cte
d o
r D
ea
d
Thior et al., JAMA, 2006

9 |
Supporting a mother to choose and implementan option:
Before delivery and in the first months
Supporting a mother to choose and implementan option:
Before delivery and in the first months
Counselling based on broad definition of AFASS for her and her baby
2 main options (replacement feeding and exclusive breastfeeding for 6 months), with other local options discussed only if mother interested
Support for choice

10 |
High EXCLUSIVE breastfeeding rates achievable with good quality counselling and support
High EXCLUSIVE breastfeeding rates achievable with good quality counselling and support
66.50%
40.10%
81.90%
0
20
40
60
80
100
6 weeks ≥ 3 months 6 monthsAge
% e
xclu
sive
ly b
reas
tfed
Median duration of EBF = 159 days
Coovadia et al., Lancet, in press

13 |
Emerging evidenceEmerging evidence
Early BF cessation associated with increased morbidity and mortality in HIV-exposed infants
Providing free infant formula from birth does not necessarily lead to better HIV-free survival compared to EBF

14 |
Infant infections by feeding modeInfant infections by feeding mode
HRp95% CI
EBF1.0
BM + fluid1.56 0.308 0.66-3.69
BM + solids10.870.0181.51-78.00
BM+FF (@12wks)1.820.0570.98-3.36
EBF1.0
MBF pre-3/121.54 0.011 1.10-2.15
MBF post-3/121.53 0.021 1.07-2.20
Vertical Transmission Study, in Press

15 |
Emerging evidenceEmerging evidence
HIV-positive infants benefit from continued BF
Availability of health system support important in assessing AFASS
Severity of disease in mother important, but AFASS criteria still more critical

16 |
Emerging evidenceEmerging evidence
● Improved adherence, longer duration of exclusive breastfeeding achieved in HIV-infected and HIV-uninfected mothers given consistent messages and frequent, high quality counselling
● Not enough evidence re ARVs and breastfeeding to draw firm conclusions, but HIV-infected mothers who need ARVs should have them

17 |
Supporting a mother at key decision points in first months
Supporting a mother at key decision points in first months
If mother breastfeeding: Early testing (PCR):
Baby HIV-negative: replacement feeding if AFASS Baby HIV-positive: continue breastfeeding
Improvement in financial/social/support situation: re-assess AFASS to consider replacement feeding
Mother on ARVs: Risk of transmission low, but replacement feeding if AFASS
Continued support for choice for all mothers

18 |
Supporting a mother when practiceschange at 6 months
Supporting a mother when practiceschange at 6 months
If still breastfeeding: if other milks, animal source-foods available – cease all breastfeeding
and give other foods no such foods available – risk of mixed feeding for a few months
probably less than risk of severe malnutrition
If breastfeeding already stopped: Continue with milk of some kind and complementary foods
Continued support for choice

19 |
Implications for scaling-up in countriesImplications for scaling-up in countries
Good quality infant feeding counselling and support for mothers (training, motivation, supervision)
Protection, promotion and support for infant feeding for all women to help HIV-positive women who breastfeed
Where breast-milk substitutes provided, safe and appropriate use and prevention of spillover
Link infant feeding with effective reproductive and child health services

20 |
Updating guidanceUpdating guidance
Consensus Statement from 2006 Technical Consultation (new evidence and experience, updated recommendations
Full consultation report (1st quarter 2007)
Update of Review of transmission (1st quarter 2007)
Technical update (2nd quarter 2007)
Minimal revision of existing tools (as reprinted)
Complete revisions when more evidence on ARVs and breastfeeding available (~2008-9)

21 |
THANK YOUTHANK YOU