Update from the WHO Global Malaria Programme Update from the WHO Global Malaria Programme Silvia...
18
1 Global Malaria Programme IPC Meeting | 30-31 May 2013 Update from the WHO Global Malaria Programme ilvia Schwarte iagnosis, Treatment and Vaccines (DTV) lobal Malaria Programme (GMP) -mail: [email protected] Interagency Pharmaceutical Coordination Group Meeting 16-17 December 2014 World Bank, Washington, USA
-
Upload
godwin-cunningham -
Category
Documents
-
view
217 -
download
2
Transcript of Update from the WHO Global Malaria Programme Update from the WHO Global Malaria Programme Silvia...
Update from the
WHO Global Malaria Programme
Update from the
WHO Global Malaria Programme
Silvia SchwarteDiagnosis, Treatment and Vaccines (DTV) Global Malaria Programme (GMP)e-mail: [email protected]
Interagency Pharmaceutical Coordination Group Meeting16-17 December 2014World Bank, Washington, USA
2 Global Malaria Programme
IPC Meeting – Washington – 16-17 December 2014
Outline
Rapid diagnostics tests (RDTs) for malaria - WHO/FIND Malaria RDT Product Testing Programme and WHO Information note on recommended selection criteria for procurement of malaria RDTs
Antimalarial medicines - WHO Prequalification - Stringent Regulatory Authorities
Temporary malaria control measures in ebola- affected countries

3 Global Malaria Programme
IPC Meeting – Washington – 16-17 December 2014
WHO/FIND/CDC Malaria RDT Product Testing Programme
Round 1 Round 2 Round 3 Round 4 Round 5
Number of products 41 29 50 48 42
Number of manufacturers 21 13 23 27 34
Resubmissions - 1 23 13 23
Invalid Rate False Positive Rate
PDS at 200 parasites/μl
PDS at 2000 parasites/μl
PDS = 75%
Round 5 report published July 2014
http://apps.who.int/iris/bitstream/10665/128678/1/9789241507554_eng.pdf?ua=1&ua=1
WHO Information Note on recommended selection
criteria for procurement of malaria RDTs updated
September 2014
English: http://
www.who.int/entity/malaria/publications/atoz/rdt-selection-criteria-sept2014.pdf?ua=1
French: http://www.who.int/entity/malaria/publications/atoz/rdt-selection-criteria-sept2014-fr.pdf?ua=1
4 Global Malaria Programme
IPC Meeting – Washington – 16-17 December 2014
WHO-prequalified medicines(last updated 11 November 2014)
Fixed-dose combinations - AL, 20mg/120mg: Ajanta, Cipla, Ipca, Macleods, Mylan,
Novartis, Strides
- AL, 20mg/120mg, dispersibles: Ajanta, Novartis
- AL, 40mg/240mg: Mylan
- ASAQ: Ajanta, Cipla, Guilin, Ipca, Sanofi
- ASMQ: DNDi/Cipla
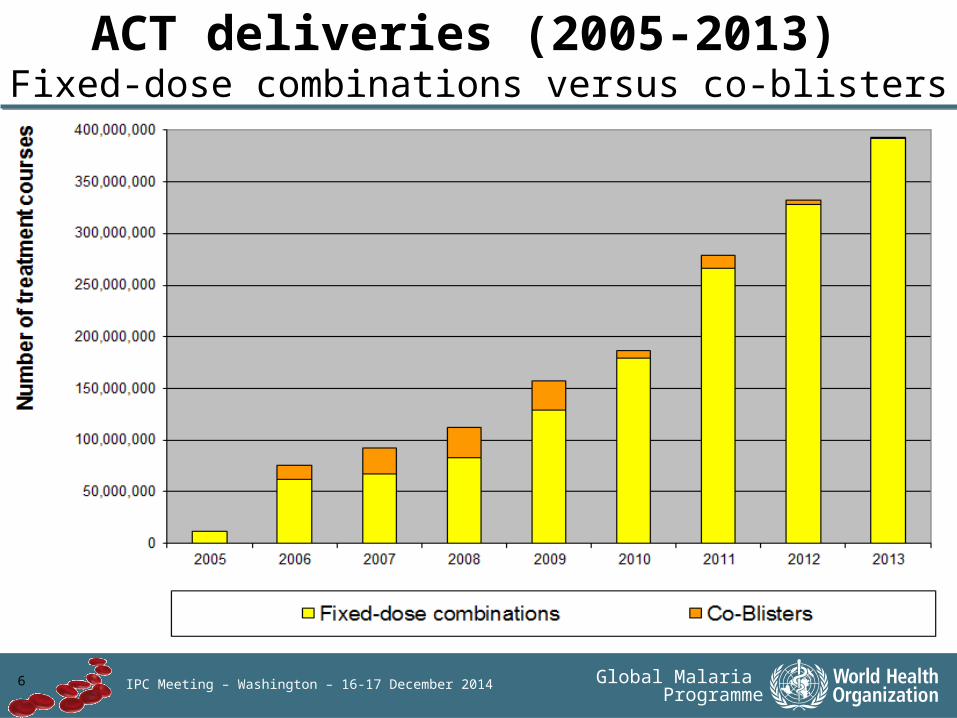
Co-Blisters (Co-B) - AS + AQ: Cipla, Guilin, Ipca, Strides
- AS + SP: Guilin
Injectables - AS powder for injection (30mg, 60mg, 120mg): Guilin
Full list of WHO-prequalifed medicines available at: http://apps.who.int/prequal/
-----------------------------------------------------------------------------------------------------------------------------AL: artemether/lumefantrine; AS: artesunate; AQ: amodiaquine; MQ: mefloquine; SP: sulfadoxine /
pyrimethamine

5 Global Malaria Programme
IPC Meeting – Washington – 16-17 December 2014
ACT deliveries (2005-2013) by combination
6 Global Malaria Programme
IPC Meeting – Washington – 16-17 December 2014
ACT deliveries (2005-2013) Fixed-dose combinations versus co-blisters
7 Global Malaria Programme
IPC Meeting – Washington – 16-17 December 2014
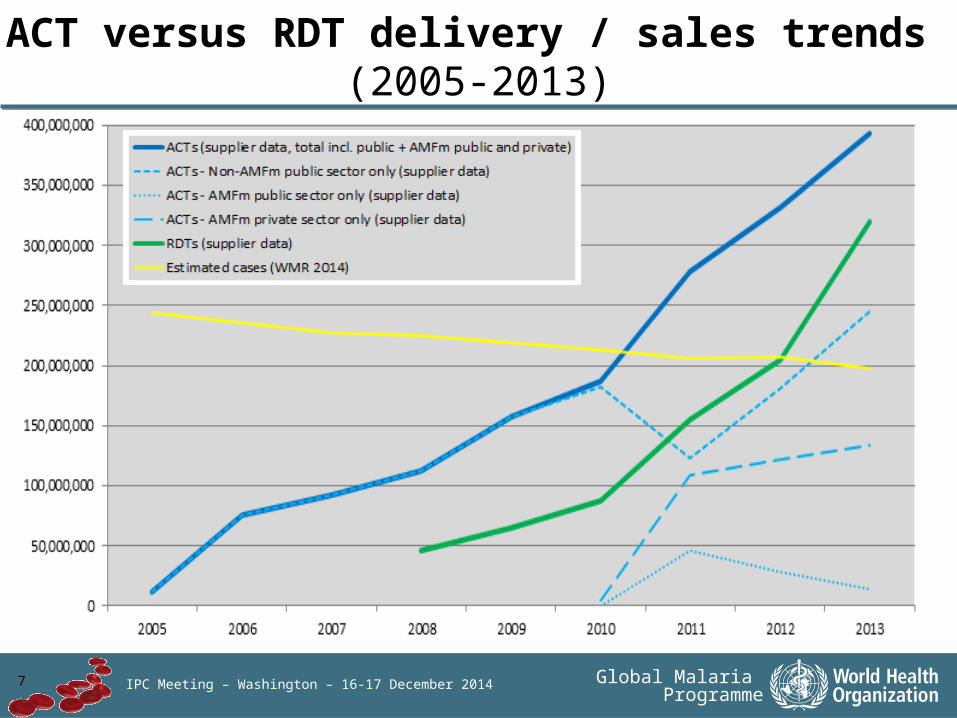
ACT versus RDT delivery / sales trends (2005-2013)

8 Global Malaria Programme
IPC Meeting – Washington – 16-17 December 2014
European Medicines Agency (EMA) reviewed
EMA approval: Eurartesim (dihydro-artemisinin + piperaquine) Prolonged QTc intervals: max 2 doses / year => further studies are ongoing, results expected soon
EMA Article 58 – Positive Scientific Opinion:
Pyramax (artesunate + pyronaridine) Hepatotoxicity: max single dose => further studies on repeated exposure are ongoing, results expected soon
9 Global Malaria Programme
IPC Meeting – Washington – 16-17 December 2014
Single-dose primaquine as gametocytocide in
Plasmodium falciparum malariaSingle dose of primaquine at 0.25mg base/kg:
is effective in transmission blocking is unlikely to cause serious toxicity in subjects with any of the
G6PD variants
MPAC recommendation => WHO treatment guidelines , 3rd Edition, Q1/2015:
In low transmission areas,
a single 0.25 mg base/kg primaquine dose should be given to all patients with parasitologically-confirmed P. falciparum
malaria on the first day of treatment in addition to an ACT,
except for pregnant women, breastfeeding women in the first six months and children less than six months of age
due to insufficient data on the safety of its use in these categories. G6PD testing is not required.
http://
www.who.int/malaria/pq_updated_policy_recommendation_en_102012.pdf?ua=1

10 Global Malaria Programme
IPC Meeting – Washington – 16-17 December 2014
Primaquine sourcing for procurement
LIST OF MALARIA PHARMACEUTICAL PRODUCTS classified according to the Global Fund Quality Assurance Policy, accessible via the
following link: http://www.theglobalfund.org/documents/psm/PSM_ProductsMALARIA_List_en/
11 Global Malaria Programme
IPC Meeting – Washington – 16-17 December 2014
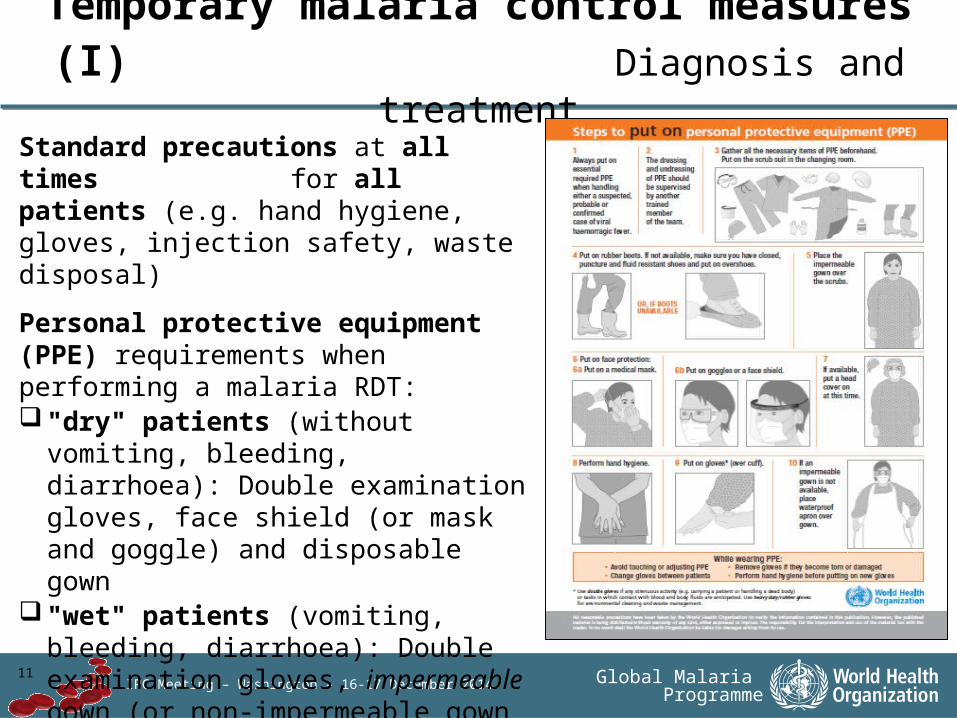
Temporary malaria control measures (I) Diagnosis and treatment
Standard precautions at all times for all patients (e.g. hand hygiene, gloves, injection safety, waste disposal)
Personal protective equipment (PPE) requirements when performing a malaria RDT:"dry" patients (without vomiting,
bleeding, diarrhoea): Double examination gloves, face shield (or mask and goggle) and disposable gown
"wet" patients (vomiting, bleeding, diarrhoea): Double examination gloves, impermeable gown (or non-impermeable gown and rubber apron), medical mask, face shield or goggles, head cover, boots

12 Global Malaria Programme
IPC Meeting – Washington – 16-17 December 2014
Where PPE requirements cannot be met: Temporary suspension of RDT performance Presumptive treatment of suspected malaria cases
with full ACT dose – clinical response expected within 48hrs – if no fever clearance in this time, this virtually excludes malaria as a cause of fever and strengthens the likelihood of other febrile illnesses, including ebola
Integrated community case management (iCCM) programmes:CHWs should be instructed / trained to diagnose malaria cases
only on the basis of history of fever (without performing RDTs)Presumptive malaria treatment until the epidemic is officially
declared overPneumonia and diarrhoea: iCCM guidelines – referral of suspected
ebola cases
Temporary malaria control measures (II) Diagnosis and treatment

13 Global Malaria Programme
IPC Meeting – Washington – 16-17 December 2014
Temporary malaria control measures (III)
Distribution of long-lasting insecticidal nets (LLINs)Precautions at all times:
personal protective equipement (PPE) is not required no-touch
– avoid hand-shaking; – no touching or providing care to sick people; – no touching of personal items (i.e. plates, cup, utensils) and surfaces in the household, in particular if anyone is sick in the house);
frequent hand hygiene (alcohol-based hand-rub solution or, if not available, with water and soap);
maintaining a 1 meter distance when interacting with people

14 Global Malaria Programme
IPC Meeting – Washington – 16-17 December 2014
Temporary malaria control measures (IV)
Mass administration of ACTs Where? Recommended in areas
– heavily affected by ebola – with high malaria transmission and – low access to malaria treatment
Why? Expected benefits: – rapid reduction in malaria morbidity and mortality; – decreased incidence of febrile illnesses due to malaria => reduced presentation of febrile patients at ebola evaluation facilities => lower risk of ebola transmission to malaria patients; reduced workload – improve the credibility of health service delivery, including community
outreach; – possible delivery in combination with other interventions How?
– Ideally long-lasting ACTs not used as first-line treatment (e.g. DHA-PPQ); – however, ASAQ (first-line treatment in affected countries) may be
preferable given its immediate availability and acceptability Who? Health workers and general population
15 Global Malaria Programme
IPC Meeting | 30-31 May 2013
Thank you
16 Global Malaria Programme
IPC Meeting | 30-31 May 2013
Backup slides

17 Global Malaria Programme
IPC Meeting – Washington – 16-17 December 2014
Temporary malaria control measuresDistribution of long-lasting insecticidal nets (LLINs)
Further considerations for distribution campaigns avoid creation of large crowds communication and social mobilization campaigns simple recording / pragmatic approach (e.g. standard
number of LLINs per household based on average household size if this will ensure universal coverage in target areas)
door-to-door distribution of nets (including nails and strings to limit population movement)
door-to-door distribution of vouchers (reduce logistical requirements; voucher information: (i.) number of LLINs to be given per voucher; (ii.) point of distribution where LLINs can be collected; (iii.) recommended time periods for collecting LLINs and hanging materials; and (iv.) ideally message on appropriate behaviours to prevent malaria and ebola transmission – net no role in ebola transmission blocking)
inclusion of health centres with inpatient facilities including ebola referral and ebola treatment centres to replace used nets (incinerate; PPE!)
18 Global Malaria Programme
IPC Meeting – Washington – 16-17 December 2014
Temporary malaria control measuresMass administration of ACTs
Communication and social mobilization campaign (e.g. expected benefits, full adherence to treatment, management of adverse events)
MDA door-to-door; administering health workers: "precautions at all times" (see above). Ideally, 1st ASAQ dose: directly observed treatment; 2nd and 3rd doses self-administered at home.
ASAQ can be given to the entire population (exceptions: pregnant women during the first trimester, infants weighting less than 5 kg, people who received ASAQ during the past month, and patients taking zidovudine, efavirenz or co-trimoxazole)
MDA should be provided at monthly intervals. After 2-3 rounds need for continuing MDA should be assessed.
Ideally, combine MDA with distribution of other commodities (e.g. LLINs, soaps, oral rehydration salts)