
Untying the elderly: Response to quality-of-life issues: A multifaceted approach is necessary to...
5
Untying the Elderly: Response to Quality-of-Life Issues A multifaceted approach nursing practice. is necessary to effect change in BY ROSE MASON/MARJORIE O'CONNOR/SUSAN KEMBLE B efore 1991, nurses at the FDR VA were respon- sible for initiating the use of "soft" restraints, and this practice was not monitored.1 "Protective de- vices" were among the euphemisms for gerichairs, vests, and wheelchair belts, which were commonly used. These were, of course, types of restraints. This practice agreed with past thinking, which emphasized an active or pro- active approach to patient safety to avoid falls and injury during hospital stays. Three separate, but related, trends called such thinking into question: a growing emphasis on the importance of patients' rights, 2 changes in JCAHO and OBRA standards, 3-5 and evidence from research that questioned the efficacy of restraints for patient safety. 6, 7 Restraints came to be seen as being counterproductive to the patient's quality of life and safety) The standard for geriatric, as well as psychiatric, care has evolved to one of providing care in the least restrictive environment possible.9, 10 Purpose These policy and social changes led to our becoming actively involved in a program to "untie the elderly." The program required shifts in philosophy and practice to pre- pare staff and families for an increase in falls. However, the literature told us that an increased number of falls did not correlate with an increased number of injuries. 11 This led to our conducting a descriptive correlational study to examine nurses' use of soft restraints on eight nonpsychiatric units at our VA hospital. ROSE MASON, RN, BSN, is an associatechief nurse/extendedcare, MARJORIE O'CONNOR, RN, MS, is chief of the Nursing Service, and SUSAN KEMBLE,RN, MS, is a nurse researcherat the FDR VA Hospital, in Montrose, N.Y. GERIATR NURS1995; 16:68-72. Copyright 1995 by Mosby-Year Book, Inc. 0197-4572/95/$3.00 + 0 34/1/53697 The question that we sought to answer was: What would be the change in nursing staff's use of soft re- straints over a 12-month period on eight nonpsychiatric units in our VA hospital under conditions of multiple re- inforcement versus conditions of no reinforcement? Operational definitions were as follows: Change: (1) change by unit (2) change by type of restraining device Soft restraints: garments or devices (excluding locked leather restraints) that inhibit a patient's voluntary movement This definition meant that some devices (e.g., wheel- chair belts) were restraints for some patients but not for others, and for some patients at some times but not at others, depending on the patient's ability to release the restraint. The definition also meant that the same devices may or may not have been restraints, depending on how they were used. For example, gerichairs were restraints if the trays were down and the patients could not get out of them, but not if the trays were up. Nursing staff: registered nurses, licensed practical nurses, and nursing assistants Multiple reinforcement: continuing education, in- services, memoranda, policy change, and discussions in committees, on rounds, and informally No reinforcement: none of the above Methodology The FDR VA Hospital is a 650-bed geropsychiatric fa- cility located approximately 60 miles north of New York City. The units involved in this study included three nurs- ing home care units, four intermediate care units, and one acute medical unit, which was included because our pop- ulation is predominantly geriatric. A tool designed by the first author was used to survey the eight units included in the sample. In addition to in- dicating the individual patient who was restrained and 68 Mason, O'Connor,and Kemble March/April 1995 GERIATRIC NURSING
-
Upload
rose-mason -
Category
Documents
-
view
214 -
download
0
Transcript of Untying the elderly: Response to quality-of-life issues: A multifaceted approach is necessary to...

Untying the Elderly: Response to Quality-of-Life Issues A multifaceted approach nursing practice.
is necessary to effect change in
B Y R O S E M A S O N / M A R J O R I E O ' C O N N O R / S U S A N K E M B L E
B efore 1991, nurses at the FDR VA were respon- sible for initiating the use of "soft" restraints, and this practice was not monitored.1 "Protective de-
vices" were among the euphemisms for gerichairs, vests, and wheelchair belts, which were commonly used. These were, of course, types of restraints. This practice agreed with past thinking, which emphasized an active or pro- active approach to patient safety to avoid falls and injury during hospital stays. Three separate, but related, trends called such thinking into question: a growing emphasis on the importance of patients' rights, 2 changes in JCAHO and OBRA standards, 3-5 and evidence from research that questioned the efficacy of restraints for patient safety. 6, 7 Restraints came to be seen as being counterproductive to the patient 's quality of life and sa fe ty ) The standard for geriatric, as well as psychiatric, care has evolved to one of providing care in the least restrictive environment possible.9, 10
Purpose
These policy and social changes led to our becoming actively involved in a program to "untie the elderly." The program required shifts in philosophy and practice to pre- pare staff and families for an increase in falls. However, the literature told us that an increased number o f fal ls did not correlate with an increased number o f injuries. 11 This led to our conducting a descriptive correlational study to examine nurses' use of soft restraints on eight nonpsychiatric units at our VA hospital.
ROSE MASON, RN, BSN, is an associate chief nurse/extended care, MARJORIE O'CONNOR, RN, MS, is chief of the Nursing Service, and SUSAN KEMBLE, RN, MS, is a nurse researcher at the FDR VA Hospital, in Montrose, N.Y. GERIATR NURS 1995; 16:68-72. Copyright �9 1995 by Mosby-Year Book, Inc. 0197-4572/95/$3.00 + 0 34/1/53697
The question that we sought to answer was: What would be the change in nursing staff's use of soft re- straints over a 12-month period on eight nonpsychiatric units in our VA hospital under conditions of multiple re- inforcement versus conditions of no reinforcement?
Operational definitions were as follows: �9 Change: (1) change by unit
(2) change by type of restraining device �9 Soft restraints: garments or devices (excluding locked
leather restraints) that inhibit a patient 's voluntary movement This definition meant that some devices (e.g., wheel-
chair belts) were restraints for some patients but not for others, and for some patients at some times but not at others, depending on the patient's ability to release the restraint. The definition also meant that the same devices may or may not have been restraints, depending on how they were used. For example, gerichairs were restraints if the trays were down and the patients could not get out of them, but not if the trays were up. �9 Nursing staff: registered nurses, licensed practical
nurses, and nursing assistants �9 Mul t i p l e reinforcement: continuing education, in-
services, memoranda, policy change, and discussions in committees, on rounds, and informally
�9 No reinforcement: none of the above
Methodology
The FDR VA Hospital is a 650-bed geropsychiatric fa- cility located approximately 60 miles north of New York City. The units involved in this study included three nurs- ing home care units, four intermediate care units, and one acute medical unit, which was included because our pop- ulation is predominantly geriatric.
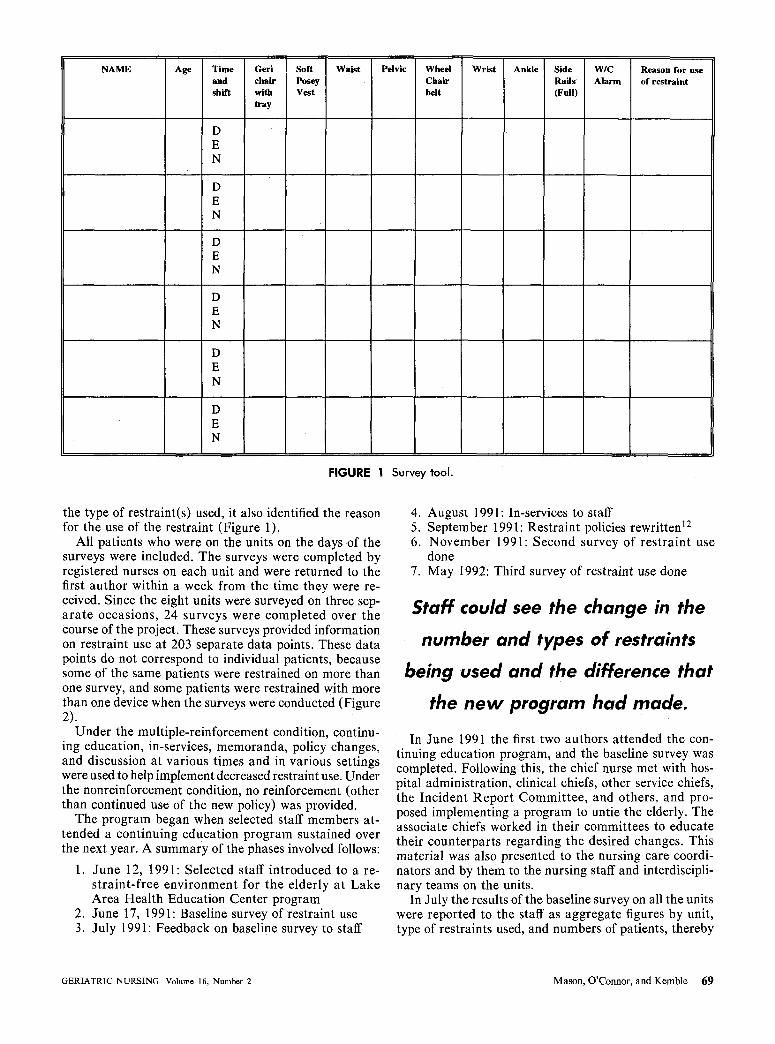
A tool designed by the first author was used to survey the eight units included in the sample. In addition to in- dicating the individual patient who was restrained and
68 Mason, O'Connor, and Kemble March/April 1995 GERIATRIC NURSING
NAME Age Time and shift
D E N
D E N
D E N
D E N
D E N
D E N
Geri chair with tray
Soft Posey Vest
Waist Pelvic Whed Chair belt
Wrist An~e Side Rails (Full)
W/C Alarm
Reason for use of restraint
FIGURE 1 Survey tool.
the type of restraint(s) used, it also identified the reason for the use of the restraint (Figure 1).
All patients who were on the units on the days of the surveys were included. The surveys were completed by registered nurses on each unit and were returned to the first author within a week from the time they were re- ceived. Since the eight units were surveyed on three sep- ara te occasions, 24 surveys were completed over the course of the project. These surveys provided information on restraint use at 203 separate data points. These data points do not correspond to individual patients, because some of the same patients were restrained on more than one survey, and some patients were restrained with more than one device when the surveys were conducted (Figure 2).
Under the multiple-reinforcement condition, continu- ing education, in-services, memoranda, policy changes, and discussion at various times and in various settings were used to help implement decreased restraint use. Under the nonreinforcement condition, no reinforcement (other than continued use of the new policy) was provided.
The program began when selected staff members at- tended a continuing education program sustained over the next year. A summary of the phases involved follows:
1. June 12, 1991: Selected staff introduced to a re- s traint-free environment for the elderly at Lake Area Health Education Center program
2. June 17, 1991: Baseline survey of restraint use 3. July 1991: Feedback on baseline survey to staff
4. August 1991: In-services to staff 5. September 1991: Restraint policies rewritten 12 6. November 1991: Second survey of restraint use
done 7. May 1992: Third survey of restraint use done
Staff could see the change in the
number and types of restraints
being used and the difference that
the new program had made.
In June 1991 the first two authors attended the con- tinuing education program, and the baseline survey was completed. Following this, the chief nurse met with hos- pital administration, clinical chiefs, other service chiefs, the Incident Report Committee, and others, and pro- posed implementing a program to untie the elderly. The associate chiefs worked in their committees to educate their counterparts regarding the desired changes. This material was also presented to the nursing care coordi- nators and by them to the nursing staff and interdiscipli- nary teams on the units.
In July the results of the baseline survey on all the units were reported to the staff as aggregate figures by unit, type of restraints used, and numbers of patients, thereby
GERIATRIC NURSING Volume 16, Number 2 Mason, O'Connor, and Kemble 69

FIGURE 2 Patients in restraints by type of restraint.
facilitating comparisons between the units. Staff were in- structed to review and document continued need or to dis- continue using restraints. They were also told that their practice would be resurveyed in the future.
In September the policy on the use of soft restraints was rewritten. Although initiating the use of and main- taining these restraints had been a nursing function, it was changed to a hospital policy requiring a physician's order, which required renewal every 30 days on the acute and intermediate medical units and every 90 days on the nursing home care units. The nursing policy was rewrit- ten to be consistent with this, and a flow sheet was de- veloped to document the outcome. The new policies were in t roduced and pract ice re inforced with in-services, rounds, committee meetings, and informal interaction.
In November a second survey on res t ra in t use was done. During this interval, no additional in-service train- ing was provided, but f rom the staff feedback one could see the change in the number and types of restraints being used and the difference that the new program had made.
In May 1992, the survey on restraint use was repeated for the third time. At this point there was no further re- inforcement with in-services, and the new policies regard- ing restraints had been in effect for 8 months (Figures 2, 3, and 4).
Discussion
The results of our surveys showed the changes that we expected. Res t ra in t use decreased between the first (baseline) and second (multiple reinforcement condition) survey for both types of change, units, and types of re- straining devices. Restraint use increased somewhat be- tween the second and third surveys (no reinforcement condition). Restraint use remained, however, far below what it had been at baseline.
Without a control group and randomization, our re- suits cannot be generalized. In addition, our numbers are very small: some of our data points could not be used for any kind of analysis.
Still, our findings are consistent with the literature, which shows that a discrepancy between awareness and behavior makes multiple reinforcement important for successful change in practice. We believe that this also applied to our restraint-reduction program.
The long-term consequence of
maintaining a patient in a restraint
is a negative one.
Successful change in nursing practice seems to require a multifaceted approach, but once in place, it can be sus- tained at an acceptable level without the intensity of ef- fort required to initiate it.
Removingrestraints from patients, as noted by the sur- vey, does not increase their potential for injury. The pa- tient's short-term safety would be ensured if the patient were to be maintained in the restraint. However, re- straints foster a dependent attitude, potentiate contrac- tures and skin breakdown, and increase nursing time in turning and releasing the restraints. Therefore the long- term consequences of maintaining a patient in a restraint is a negative one. This argues for decreasing the use of re- straints. The survey did support the findings in the liter- ature that removing restraints from patients will result in an increased number of falls, but, as noted, there would be few serious injuries. Nursing is a dynamic profession that changes its practice on the basis of scientific facts and data; the use of restraints would be curtailed on the basis of facts. With the advent of patient rights, quality care issues, and increased focus on the treatment of the
70 Mason, O'Connor, and Kemble March/April t995 GERIATRIC NURSING

2 5
~ r
O
~ 5 E z
0
25 W
P t- o15 r
@
~ 5 E 23 z
0
25
10C0 10AB gAB 9CD 7AB 7CD 6CD 6AB
June I g91
10CD 10AB gAB 9CD 7AB 7CD 6CD 6AB
November 1991
I~ 2o
C
~ t ' -
o
"6
-Q 5 E z
0 10CD 10AB gAB g(2O 7AB 7CD 6CD
May lgg2
FIGURE 3 Patients in restraints per word.
~ B
geriatric patient, the use of restraints has been an area of concern that has stimulated research.
Caretakers have been indoctrinated with the concept that to maintain patient safety--particularly with the ge- riatric pa t ien t - - i t is necessary to use some type of re- straint. Again, past thinking emphasized patient safety to avoid falls and injury. To ensure this, the use of restraints was appropriate, and, in fact, nursing staff would be held liable if the restraint was not in place. Nurses used the eu- phemism "protective device" to enable them to imple- ment the use of restraints with a nursing order, and the
t0CD 10AB gAB 9CD 7AB 7CD 6CD 6AB
I l l June1991]
IOCD IOAB 9AB 9CD TAB 7CD
I I I November 1991 I
6CD 6AB
~ 5
e , -4 o
~3 n "62 .Q E1 z
0 10CD 10AB
FIGURE
gAB 9CD 7AB 7CD 6CD 6AB
f U May lgg2 1
4 Patients in multiple restraints.
staff member either advocated for the initiation, elimina- tion, or maintenance of restraints. The study argues for a decrease in the number of restraints used and represents both a change in nursing pract ice and a philosophic change in the way that caretakers view patient safety and the use of restraints. It also changes the focus from one of merely preventing injury to one of maintaining a patient's
GERIATRIC NURSING Volume 16, Number 2 Mason, O ' C o n n o r , and Kemble 7 1

qua l i ty of l ife and r ights . This represents a change in long- term versus shor t - term gain. The change, however, will enhance not only the dignity of pat ient but will focus on the assessment factors needed if a restraint is imple- mented. It was noted that once a restraint was issued it was easy to lose sight of the reason for the restraint, and so it may become a s tandard of practice, the use not nec- essarily being based on need. When the use of restraints is reviewed on an ongoing basis and when focus on the use of restraints is maintained, the number of restraints being used will decrease. The implicat ion for pract ice involved the par t ic ipat ion of the team, the assessment of the pa- t ient for the need for restraint, a refocusing of the assess- m e n t of the pa t i en t for con t inua t ion of the res t ra in ts . This also places nursing staff in a role they are comfort- able with (by being proact ive as a patient advocate in pa- t ient-r ights issues, t rad i t ional ly a role of nursing). This must also be done in concurrence with an a t t i tude change in the way care takers view the use of restraints. I t is nec- essary to reor ient and reeducate and change the att i tudes of the care takers and hospital adminis t ra tors about be- coming actively involved in quali ty-of-l i fe issues and the main tenance of pat ient 's rights. Thus the significance of this change in prac t ice is great , because nurses are the frontl ine caretakers involved in the use of restraints. This will involve educational , at t i tudinal , and pract ice changes that will all help to support and evolve an env i ronment much more conducive to the patient 's qual i ty of life. •
We acknowledge the assistance of Cecile Sisson, PhD, with the graphs. All views expressed are those of the authors, and do not necessarily re- flect the views and policies of the Franklin Delano Roosevelt Hospital, or the Department of Veterans Affairs.
REFERENCES
1. Department of Veterans Affairs. Supportive protective devices. Nursing Ser- vice Letter ¢26. Montrose, New York: FDR VA Hospital, 1990.
2. Joint Commission on Accreditation of Healthcare Organizations. Accredita- tion manual for long term care standards. Chicago: JCAHO, 1992.
3. Hurley M. What do the new JCAHO standards mean to you? RN 1991;54(6):42-6.
4. US Congress. Omnibus Budget Reconciliation Act of 1987. Public Law 100- 203, sections 4201 (a), 4211 (a). Washington: US Government Printing Office, 1987.
5. Fletcher K. Restraints should be a last resort. RN 1990;53(1):52-6. 6. Lewis L. Toward restraint-free nursing homes. Long-Term Care Currents
1990;13(1):1-6. 7. Cutchins C. Blueprint for restraint-free care. Am J Nurs 1991;91(7):36-42. 8. Stilwell E. Use of physical restraints on older adults. J Gerontol Nurs
1988;14(6):42-3. 9. Conely L, Campbell L. The use of restraints in caring for the elderly: realities,
consequences and alternatives. Nurse Pract 1991;16(12):48-52. 10. Evans L, Strumpf N. Myths about elder restraint. Image J Nurs Sch
1990;22:124-8. 11. Department of Veterans Affairs. Protective restraints. Nursing Service Letter
~26. Montrose, New York: FDR VA Hospital, 1991. 12. Department of Veterans Affairs. Management of disturbed behavior by use of
seclusion room and/or physical restraints. Memorandum 11-108. Montrose, New York: FDR VA Hospital, 1991.
" Q u o t e . . .
The physician of the future will give no medicines,
but will interest pat ients in the care of the human
frame, in nutrition, and in causes and prevention of
i l l n e s s . . . Thomas Edison
. . . E n d q u o t e "
72 Mason, O'Connor, and Kemble March/April 1995 GERIATRIC NURSING


















