
Unpacking the puzzle of Local Healthcare Politics
45
UNPACKING THE PUZZLE OF LOCAL HEALTH CARE POLITICS David Houvenagle, Ph.D. [email protected] August 2010 1
-
Upload
houvenagle -
Category
Documents
-
view
222 -
download
0
Transcript of Unpacking the puzzle of Local Healthcare Politics

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 1/45
UNPACKING THE PUZZLE OF
LOCAL HEALTH CARE POLITICS
David Houvenagle, Ph.D.
August 2010
1

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 2/45
Health care reform has been no little deal since the Obama Administration
took office in January 2009. It has become reality with President Obama signing
into law the “Health Care and Education Reconciliation Act of 2010.” In light of
this milestone, a group of health policy scholars recently recognized that health
care is organized and delivered at the local level and declared the local role to be
key for health care reform success:
The ability of each community and its local health care stakeholders todesign and implement payment reforms will be critical to the success of
those reforms. Payment reform is both a national issue because of the
national payers such as Medicare, and a local issue, because negotiations
at the local level reflect market conditions. (Robert Wood JohnsonFoundation, p.1)
Lennarson-Greer (1997) had already concluded over a decade ago that health care
delivery in the U.S. was a local responsibility. She also observed that both urban
studies and health policy scholars had been ignoring this reality and so little is
known about it in terms of social or governmental theory (p.356). 1 Health policy
scholars are expecting policy outcomes out of a local political apparatus that they
have failed to define.
The scholarly ignorance of the local aspect appears to be a product of
adherence to paradigms. Health policy scholars have been entrenched in their
focus on national and state levels and quantitative research methods. Urban
studies scholars have not considered health care to be a central focus of local
governance. However, urban studies has useful political-economic tools that can
be used in this case starting with the premise that politics consists of a tension
1 For Lennarson-Greer used the term “urban health politics” to describe the local aspect. Her
definition of this was “Urban health politics and policies attempt to define and fulfill the
responsibilities of cities for the health of their population, especially in regard to the hazards and
dangers of urban life and the uneven concentration of disease in cities (p.356).
2

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 3/45
between political structure and agency. In a personified way, structure and
agency tend to give indication about each other. Given that premise, this article
shows the growth machine thesis as a valid explanation of local health care
politics that is consistent with the older structural findings. Using Louisville
Kentucky as a case, Social Network Analysis and field interviews show that the
local growth coalition with its growth agenda is the group of political decision
makers in local health care.
This article will first review the previous relevant literature on local health
care politics and discuss the growth machine thesis. It will then review the social
network analysis (SNA) and interview findings, draw conclusions and make
suggestions for future research.
LITERATURE REVIEW
Previous scholarly writing and research on local health care politics in the
American context is from the schools of health policy, sociology, and urban
studies and goes no further than suggesting political structure at best. The
majority of this work was in the form of older case studies. While later authors
cited referred to the topic they failed to analyze the local aspect. This section will
review this literature.
Sociological Studies
The sociological authors mostly reached elitist political structure
conclusions. Belknap and Steinle (1963) identified that business interests
dominated hospital board membership (pp.122-123), and that facility
development and improvement processes required “a reasonable unity between
3
8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 4/45
formal governmental leadership and community leadership in major civic,
economic, social, and cultural groups” (p.89). Elling (a contemporary of Belknap
and Steinle) co-authored a number of qualitative studies repeatedly identifying
economic elites as central in local health care governance. Starr (1982) observed
that physicians historically depended upon the capital and philanthropy of
influential business elites to establish hospitals (pp.152-153).
Two later doctoral dissertations deserve mention. Morone (1982) studied
a number of the citizen-led local health systems agencies (HSA’s) established by
the National Health Planning and Resource Development Act of 1974 and had
found that territorial local politicians had sabotaged them. Plano (1999) vaguely
identified that some interest groups made decisions about hospital placement
within Toronto Canada and Milwaukee, but he did not produce a picture of the
community power structure making the health care decisions. While these studies
contribute to overall knowledge, no one has expounded on their work.
Health Policy Writings
Contemporary to Elling, Conant, and Wilson were health policy
researchers cited in later works. Conant’s (1968) decision-making study of five
communities found the public to be apathetic and ignorant of health issues and
that planning was ad-hoc versus rational-comprehensive in nature (pp.14-18).
Wilson’s (1968) 21-community study found economic leaders were more
influential than political leaders and professionals in health issues (p.98). Both
Conant and Wilson identified several political tendencies 1) incrementalism; 2) a
4

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 5/45
status quo; 3) no consistent agenda; and 4) ensconced administrators holding
decision-making power with the backing of supportive civic and economic elites.
Alford (1975) focused on New York City’s health system from a political-
economic view. He suggested that health care institutions “must be understood in
terms of a continuing struggle between major structural interests operating within
the context of a market society.” Alford noted that a tension exists between
bureaucratic reformers and market reformers (pp.1-2). He suggested that popular
control of health care is unlikely, because the public is too unorganized to
negotiate with the structural interests (pp.220-222). Alford’s findings were
unique but like the dissertation writers, there was no expounding on his work.
Ginzburg (1977) was more anecdotal in nature and observed that elites
historically controlled the typical nonprofit community hospital. He observed the
norm of multiple generations of affluent local families sitting on the same local
hospital boards (p.3).
Litman and Robins (1984) devoted one-half of a page to political structure
as it pertained to local health care. Litman and Robins use the term “pluralism” to
describe their view of local politics, but their citations are not about the pluralism
of community power. They referred to pluralism in terms of the autonomy of
doctors, while it indicates popular or democratic control by the community in
urban studies. Their political structure discussion seemed incidental with a focus
on a standard of participatory democracy (p.20).
The later public health authors exemplify Lennarson-Greer’s point about
neglect of the local aspect. Tulchinsky and Varavikova (2000) only discuss the
5

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 6/45
local level of health care governance in bureaucratic terms as part of the federal
system (pp.530-532). Gentile-Donnell (2004) related the closing of a
Philadelphia public hospital in terms of formal government but she failed to
discuss community power structure. Bodenheimer and Grumbach (2005)
described local policies in generalities, and only discussed the governance of
community health centers in federal versus local terms (p.60-62). Lastly, Shi and
Singh (2008) declared that “Federal, state, and local governments pursue their
own policies with little coordination of purpose or programs,” but Shi and Singh
failed to give any description of the local governance structure or agency (p.538).
These later health policy authors confirmed Lennarson-Greer’s point.
Urban Studies
A number of urban studies authors produced some relevant work in terms
of this discussion about health care governance. The studies were reflective of the
paradigms of their times evolving from conclusions that were cybernetic to
political-economic in nature.
Swanson’s (1972) “cybernetic” political model consisted of seven
variables where different variable formulations explain government’s
involvement in health care on various levels. His variables are: 1) system output,
2) system stress (political contention, controversy, and conflict), 3) system inputs,
4) power structure, 5) political ideologies, 6) political focus, and 7) system change
processes (pp.443-454). Local health politicians then theoretically utilize
different mixtures of the variables to achieve desired policy results. Swanson
seemed to adapt a general process model to a particular policy realm and did not
6

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 7/45
identify general structural or agency tendencies, and there was no further
expansion upon his work.
Dye (1973) stated, “In nearly every community, decision-making in health
and hospital matters is firmly lodged in the hands of leaders of the local medical
associations” (p.479). Dye did not empirically substantiate this statement and did
not repeat it in later editions of his textbook.
Schussler (1994) explored corporatism in local health care politics through
the process of the state of Kentucky awarding the Humana Corporation the
management contract for the University of Louisville Hospital. In this case, a
locally based proprietary health care corporation and government had a public-
private partnership to deliver indigent care (pp.1-2).
Britton and Ocasio (2007) explored hospital and orphanage location in
Chicago between 1848 and 1916. Britton and Ocasio noted that hospitals were
placed in locations to create greater visibility of the “material and symbolic
benefits provided by these facilities.”
Within the limited body of literature on local health politics in the United
States, an elitist political structure is the most consistent theme, but this is still an
incomplete picture of the local situation. More recent urban studies findings have
evolved with the discipline to a political economic framework asking the question
“for what are the actors motivated,” which suggests agency in addition to political
structure (See Vogel, 1992 for a further discussion of urban political economy).
THE GROWTH MACHINE THESIS
7
8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 8/45
As noted earlier, the growth machine thesis is an established urban
political economy theory of urban governance. Molotch (1976) asserts in his
theory “that the political and economic essence of virtually any given locality in
the present American context is growth.” Growth unifies categorically defined
local elite stakeholders in their quest for constant expansion of the city in the
areas of population, land development and commerce (1976, pp.309-310). These
elites informally comprise a growth coalition to make political decisions for the
city. The local public only weighs in on local issues when the local elites have
agreed to disagree on those particular issues (Logan and Molotch, 2007, p.51).
The three categories of growth coalition stakeholders are listed in table 1.
They have the most to lose or gain from land-use decision-making (1976, p. 314).
The first category consists of parochial/local businesspeople (especially property
owners) and those in “locally-oriented financial institutions who need local
government in their daily money-making routines.” The second category of
stakeholders includes lawyers, syndicators and realtors who make their incomes
and revenues servicing the property owners and investors. The third category of
stakeholders consists of parties whose fortunes are tied to the overall growth of a
metropolitan area (i.e., the daily newspaper, universities and utilities). Molotch
observes that these stakeholders mobilize, legitimize and sustain local pride and
growth momentum into “particular kinds of policy decisions” (1976, pp.314-316).
Since the growth machine thesis suggests central or key relationships
within a community, testing for its presence is a matter of measuring and
evaluating relationships. The
8

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 9/45
(Table 1 about here)
growth machine thesis offers a set of nominal variables for social network
analysis (SNA) by which relationships in a local network can be interpreted.
METHOD
Research Questions
Given that the previous literature stopped at identifying political structure
and did not make any conclusions about agency, the latter was left open for
exploration. Given that the urban political economy view holds that there is a
tension between structure and agency, the question became: does the structure tell
something about the agency? Initial research indicated a growth machine
hegemony on all of the local hospital boards in Louisville, so the general question
became does the growth machine thesis explain both the structure and agency of
health care politics for the community as a whole? Evolving out of this were at
least two overall research questions:
1) Is there a growth machine in Louisville?
2) Does it shape local health care decision-making?
For all practical purposes, the question about the existence of a growth machine in
Louisville, Kentucky had been answered. Three previous studies (Whitt 1988),
(Savitch and Vogel, 2004), (Savitch et al 2008) had identified the existence of a
growth machine in Louisville.
9

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 10/45
The research design for answering the questions was a disciplined-
configurative case study that used Social Network Analysis (SNA)2 3 and elite
interviewing of individuals. This case study design applies a specific theory as a
test and compares the test results with the theoretical propositions Otherwise this
study is similar in design to one by Moore and Whitt (2000) that also combined
SNA and interviews to explore gender in community leadership roles in
Louisville, KY.
SNA is a formalized, quantitative approach for studying networks (Adam
and Kriesi 2007, p.130). It “is useful for investigations of kinship patterns,
community structure, interlocking directorships and so forth” (Scott, 1991, p.2).
Knoke and Kuklinski (1982) define a network “as a specific type of relation
linking a defined set of persons, objects or events” (p.12). SNA results are both
graphical and numerical in form to show connections and strengths or relationship
respectively.
Whitt (1989) first suggested the use of SNA to study questions suggested
by the growth machine thesis. He proposed that it could identify structural
channels and connections (pp.104-105). In light of that suggestion, SNA methods
were used to explore necessary subsidiary questions of the structural aspects that
included:
• Is there a coherent network in Louisville health care?
2 The SNA results were generated from an initial dataset of 8240 cases from a snowball sample of
board members and officer rosters of hospital and other organizations in the Louisville area
between 2005 and 2006. It is assumed that the sample used to create the dataset is representative
of the community and the health care actors.3 The centrality rankings of individuals and organizations were the same whether n= 7515 or
n=4438. The dataset likely could have been reduced further with similar ranking results.
10
8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 11/45
• If there is a coherent network, then what individuals are central in the
network and thus more powerful?
• What organizations are central in the network?
• Is there any detectable elite clique/inner circle that has high centrality?
• Where do the sectors of the growth coalition fit in relation to the whole
network?
These questions should answer the structural matter of whether health care
governance is connected to the growth machine and to what extent.
The use of SNA to determine a community-wide structure has been
conducted on a limited basis. There are two prior, known examples of the SNA
analysis of Multi-Dimensional Scaling (MDS) used to study community elites.
Laumann and Pappi (1973) used MDS to identify the network of a German city’s
elites and followed up with interviews. Galaskiewicz (1979) used MDS to
analyze the organizational networks in a Midwestern city. So, there has been a
track record for SNA to examine networks at the community level.
Whitt (1989) suggested that network analysis of a community can identify
organizational connections, but field interviews are needed to uncover intentions
(pp.104-105). In light of this suggestion—and given the SNA results, the specific
interview topics were:
1) Can the validity of the SNA results be affirmed?
2) Is there a growth agenda?
3) Is there a particular political mode of operation?
11

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 12/45
4) Why was there a disconnect between local public and private health
care organizations shown in the SNA results?
SNA Dataset
The dataset for the SNA was a snowball sample collected in 2005-2006.
The sample starting point was the hospital organizations, and the collection
spanned out into the metropolitan area to have a clear representation of the major
public and private organizations in Louisville-Jefferson County and the adjacent
Indiana and Kentucky Counties. The sample was inclusive of board and officer
rosters taken from a variety of publicly available sources based on published
rankings, organization websites, federal income tax statements, annual reports,
business databases, and the Kentucky Secretary of State business services
database.4 The data was cleaned and encoded into a form readable by the
UCINET 6 software package. The initial database had 8240 cases, which was
pared down to 4438 after initial centrality results rendered a large number of cases
to be insignificant with a Bonacich eigenvector score of 0.
Field Interviews
Interviews were conducted with 22 central individuals. These individuals
had high centrality scores, which meant that they were structurally in positions of
power. The object was to interview all the top informants as substantiated by the
SNA analyses, but not all were available or willing. The reality was that the
informants ended up being some of the most central, but also others were selected
4 The paper Business First runs a ranking of leading Louisville area firms and organizations every
week by size of business or volume of business. The paper runs a different sector every week.
12

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 13/45
based on having been identified by earlier informants as authoritative and
knowledgeable.
SNA RESULTS
The pertinent SNA analyses were 1) clique analysis (several values of N)
on the adjusted dataset of 4438 cases,5 2) Bonacich centrality of organizations and
individuals, and 3) Multi-dimensional scaling (MDS) (non-metric) of the
relationships among the different growth coalition interest groups. Graphical
analyses of individuals and organizations in Louisville using UCINET were not
meaningful due to the large dataset size.
Centrality Analysis Results
In SNA, centrality is a relational matter, and the most central individual or
individuals in a network holds the most power. Hanneman and Riddle (2005)
state, “An individual does not have power in the abstract, they have power
because they can dominate others—ego’s power is alter’s dependence”(chapter
13). There are two centrality metrics that are used in SNA: “Freeman Degree”
and “Bonacich Power.” The Bonacich measure is more precise than the Freeman
measure and was selected.6 The Bonacich power measure of centrality is
mathematically stated as cj = Σ jr ij(α +β c j) and accounts for the number of
connections an actor has and the numbers of connections the connections have.
Bonacich’s equation gives “each actor an estimated centrality equal to their own
degree plus a weighted function of the degrees of the actors to whom they were
connected” (Hanneman and Riddle, chapter 13). The values of Bonacich’s
5 UCINET 6 can be instructed to look for cliques of different sizes.6 The Freeman Degree measure merely counts the number of connections of a point and says
nothing about how significant a point’s connections are. The Bonacich measure does.
13
8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 14/45
measure are called “eigenvalues” have a nature similar to eigenvectors in factor
analysis but are interpreted in a basic fashion (higher score = more centrality).
Centrality Rankings of Organizations in Louisville
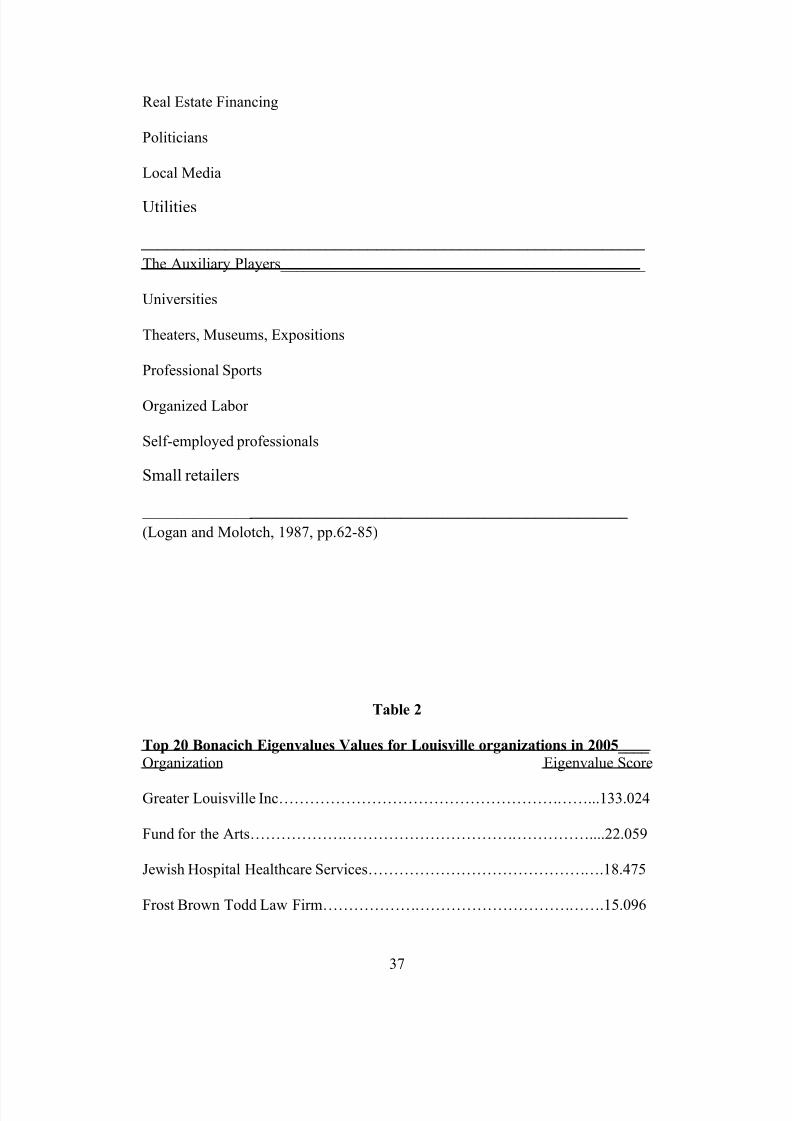
Table 2 displays the gradient of Bonacich rankings of Louisville
organizations. The development sector has hegemony. The most central “Greater
Louisville Inc,” (GLI) the local chamber of commerce is an extreme outlier as it is
603 % more central than the next most central entity. 7 Louisville Metro
Government was ninth on the list. The Metro United Way and the now-defunct
“getCare Health Network” were anomalies in the list as charitable concerns.8 The
health care organizations and typical growth coalition entities ranked high in
centrality.
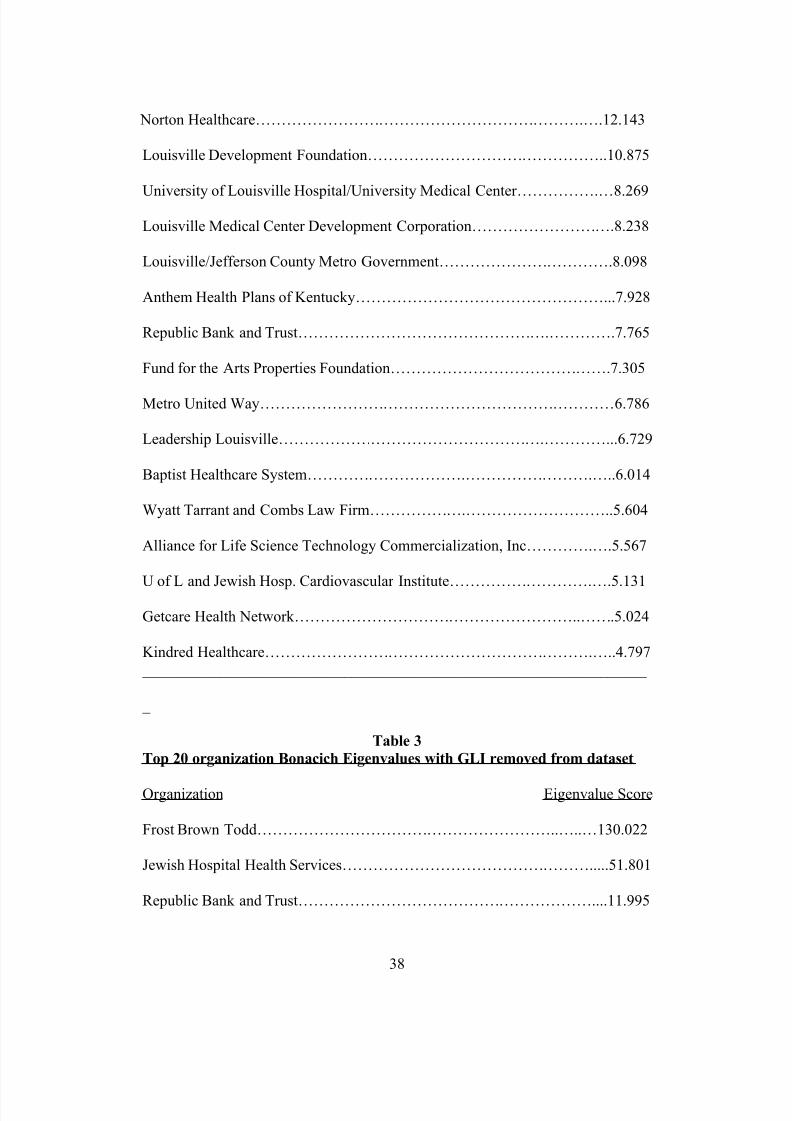
To correct the skewness, the GLI cases were removed from the dataset.
Table 3 displays that eight entities dropped out of the rankings, including
Louisville Metro Government and Norton Healthcare. However, the Frost Todd
Brown law firm (FBT) and Jewish Hospital Health Services (JHHS) increased in
centrality and became the outliers,9 which indicated inherent centrality and
organizational interlock. The now-defunct getCare Network stayed in the top 20,
suggesting participation by highly central individuals. The changes indicate that
GLI is a “knot” or “cut-point” (Scott, pp.110-111) or central exchange connecting
numerous entities in the network. This adds support to the existence of growth
coalition interests and their hegemony.
7 Mean = 1.799 Std Deviation = 8.6548 They are redistributive or charitable organizations and of a different nature than the rest. The
getCare Network was an organization spear-headed by the Louisville-Metro Health Department
and primarily funded by a Robert-Wood-Johnson Foundation “Communities in Charge” grant to
provide free or reduced medical services to uninsured individuals.9 Mean =0.488, Standard Deviation = 5.827
14

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 15/45
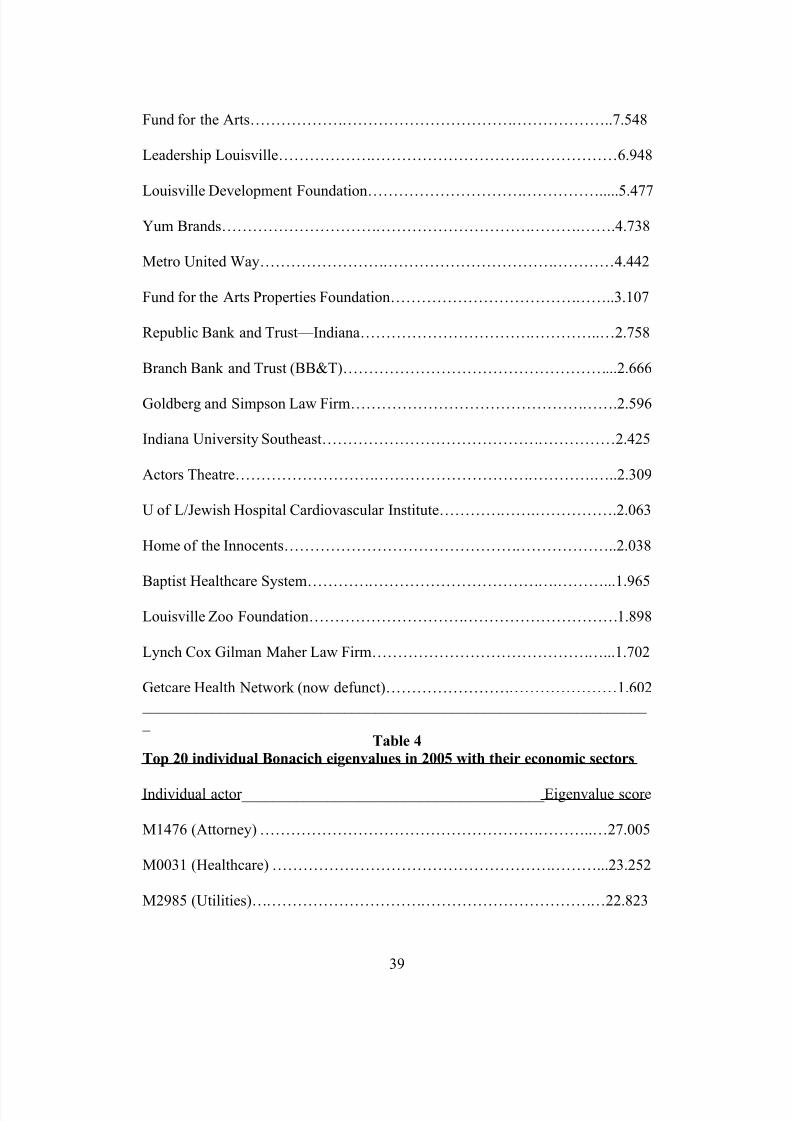
Centrality Rankings of Individuals
The Bonacich centrality for individuals further strengthened the picture of
hegemony of the growth coalition as attorneys, and individuals from utilities,
finance and education dominate the top 20 as shown in Table 4. The highest-
ranking elected politician is ranked sixth.
(Table 2 about here)
(Table 3 about here)
Like the organization scores, the individual Bonacich scores evidenced
positive skewing of the data, but with a less steep gradient .
10
There thus appears
to be correlation between membership or leadership in GLI and membership on a
hospital board.
With the GLI cases removed from the dataset, the individual rankings
displayed in table 4 followed the organization ranking patterns. M1476 gained in
value and 18 of the 20 in this second list are attorneys at the Frost Brown Todd
(FBT) law firm. While GLI is most central in the network, many FBT members
have centrality by firm membership. The more central FBT members have more
known civic involvement. GLI proved to be a central knot or cut-point connection
in the network.
Clique Analysis
In SNA, a clique is a group of individuals who are not a sub-group of any
other group. In graphical terms it is also “a sub-set of points in which every
possible pair of points is directly connected by a line and the clique is not
contacted in any other clique” (Scott, 117). The point of clique analysis in this
10 Mean =1.799, Standard Deviation = 8.654
15

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 16/45
research was to identify whether the most central and powerful individuals in the
database had any evident, exclusive associations with each other.
Clique analysis was conducted on the dataset of 4438 cases to determine
social alignment among the most central actors.11 There were 28 cliques with an
average eigenvalue of 12 or higher which was the approximate “floor” of table 4.
Two cliques stood out, the clique listed in table six (average 16.156) and the
second clique listed in table seven (average eigenvalue -15.665). The
predominant clique consisted primarily of health care executives and physicians,
and growth coalition types who had been documented to have sat on hospital
boards. Eight members in the second clique were unique to it from the
predominant clique so there was little redundancy between the two cliques.
(Table 4 about here)
(Table 5 about here)
(Table 6 about here)
(Table 7 about here)
Returning to the construct that a clique is a group of individuals that is not
a sub-group of any other group, we can conclude that there is support for an elite-
group of individuals that relate to each other exclusively within this network. In
both central cliques, growth coalition sectors are present alongside health care
figures, supporting both elite and growth coalition hegemony.
Analyses of the Network in Terms of Sectors
At this point, it has been established that 1) there is a hegemony of growth
machine and healthcare figures in Louisville in terms of centrality scores, and 2)
11 Given the gargantuan size of the network and the fact that it was a snowball sample versus
survey, it cannot be determined whether these cliques were strong cliques or weak cliques (Scott,
p.118).
16

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 17/45
there is evidence that the central growth machine and health care figures have
exclusive relationships amongst themselves in the form of coherent cliques, but
despite the strength of the centrality and clique analysis results, where the growth
coalition fits in the overall picture of the community structure remained a
curiosity. This is because Molotch’s theory is framed in terms of specific interest
groups/sectors. To assess whether different interest groups (especially those of
the growth coalition) relate to each other a dataset of 747012 was modified to
include a classification of each individual person’s livelihood.
This modification reframed the dataset in terms of 28 nominal variables,
which allowed for meaningful Multi Dimensional Scaling analysis.13 Strict
adherence to Logan and Molotch’s list of 12 growth coalition categories would
have meant a large, imprecise “other” category14 and so other livelihood names
were used for precision. 15,16
Bonacich Eigenvalue Results of Sectors.
12 This was the original dataset of n=8240 where non-human beings were removed. (Corporations
as entities were listed as officers in these cases.) Even though it was obvious from previous
analyses that the larger set contained had 41 percent of essentially irrelevant actors, the larger data
set should lend more credibility to such an analysis of the overall community picture. The added
benefit of using the larger dataset also can inform about what sectors are outside of or inside the
center of the community network. 13 For a discussion of network mapping of the sectors see Author (2008). Traditional network
graphing in the form of a map added little meaning to the results other than the growth machine
sectors were in the mainstream but affirmed that public health and health related businesses wereoutliers from the network.14 With a large general “other” category that included all other different entities, much would
likely be missed in analysis. Creating other unique categories seems to be in harmony with the
growth machine thesis as the specific categories appear to be locally dependent.15 There was an initial data problem in that the UCINET DL formatting routine did not read 377
cases. Reducing the sector names to one word reduced the missing cases down to 3.16
The sector names are as follows: Accountants, Advertising, Colleges, Branch (Corporate
Capitalists of Multi-locational firms), Development, Doctors, Elite (Social Organization),
Foundation (Charitable organization), Government, HRB (Health-Related Business), Health care
(other than hospitals), Hospitals, Insurance, Law, Media, MH (Mental Health), National (Home
Office of a Corporation based in Louisville), Nonprofit, Other, Politicians, PI (Property Investing),
Public (Health organizations), Finance (Real Estate Financing), Retailers, Sports, Technology,
Arts (Museums, Theaters, Expositions), Utilities
17

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 18/45
The Bonacich eigenvalues in the sector analysis suggest why FBT
subsumed GLI’s centrality, and why M1476 (an attorney) gained centrality when
GLI cases were removed. The “law” sector had a total eigenvalue score of
141.380 out of a sum or (Σ ) of 149.229, which was 94.7 percent of the value.17
The “development” sector had an eigenvalue of 2.283. The “hospitals” sector was
third with an eigenvalue of 2.208. The distribution of eigenvalues was, positively
skewed given that the mean was 5.330 and the standard deviation was 26.189.
Local attorneys are central in the “development” sector and are the foremost
central sector in the network of health care politics in Louisville, Kentucky.
Multi-Dimensional Scaling (MDS)
MDS has broad applications and is an alternative to factor analysis
(Wasserman and Faust, p.288). Its general goal is “to detect meaningful
underlying dimensions that allow the researcher to explain observed similarities
or dissimilarities (distances) between the investigated objects”
(http://statsoft.com/textbook/stmulsca.html). Borgatti (1997) 18states that the
purpose of MDS is “to provide a visual representation of the pattern of
proximities among a set of objects.” It is used to “provide a visual representation
of a complex set of relationships that can be scanned at a glance”
17 The reader is referred to the idea that the Bonacich measure is akin to Factor Analysis. Only so
much probability is generated and therefore 149.229= 100 percent of the possible value or
probability. It is clear that the lawyers in Louisville as a group are overwhelmingly the most
powerful group of individuals in town.18 Borgatti is also one of the architects of the UCINET software package. There are also two
versions of this page on the Internet. The other is at
http://www.analytictech.com/networks/mds.htm.
18
8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 19/45
(http://www.analytictech.com/borgatti/mds.htm). Therefore, MDS goes one-step
further than factor analysis to give a valued, graphical depiction of a network. 19
Figure 1 is the initial result from the UCINET MDS routine. The result
shows that the public health and health-related business sectors are extreme
outliers in the network—they are distinctly isolated from the other points with no
connection. In contrast, the other sectors are densely compacted or tightly
clustered into a small space.
(Figure 1 about here )
Figure 2 is a magnification of the compacted cluster in Figure 1. The
“neighborhood” of sectors overall are close to each other and could be called a
cluster in and of itself. However, within the MDS results there appears to be a
tighter cluster composed of hospitals, development, law, property-investing, non-
profit, and finance. Mental health, public health and health-related businesses
were extreme outliers.
On the other hand, in the center of the map, hospitals and development
sectors are practically on top of one another with law and finance being the other
closest, adjacent sectors. There are no clean or neat dimensions evidenced in the
19 MDS has both numerical and graphical components that can add additional understanding to the
network of actors. Its output “is a set of estimated distances among pairs of entities, which can beexpressed as coordinates in one-, two-, or higher dimensional space” (Wasserman and Faust,
p.288). Its graphical depiction is a “Shepard’s diagram” similar to a Cartesian plane.
(http://www.statsoft.com/textbook/stmulsca.html)
Borgatti’s guidelines for interpreting a MDS map are as follows. First, “All that matters in an
MDS map is which point is close to which others.” Second, the axes are “meaningless” and “that
the orientation of the picture is arbitrary.” Furthermore, Borgatti notes that the two keys to
interpretation are noting the “clusters” or groups of points that are closer to each other than toother points and the “dimensions” that are “item attributes that seem to order the items in the map
along a continuum”(http://www.analytictech.com/borgatti/mds.htm).
19
8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 20/45
MDS map. At best, the closeness of the law, hospitals, and development sectors
reflect their high Bonacich centrality results.
(Figure 2 about here)
Validity of MDS results
The validity of MDS results is indicated by the “stress” score. Stress is
either an indication of goodness of fit (www.statsoft.com/textbook/stmulsca.html)
or “a measure of badness of fit” (Hanneman and Riddle, chapter 13). The stress
score was 0.002 in 50 iterations. Borgatti noted that a map with “non-zero stress”
is distorted.” Borgatti suggests that any stress score under 0.1 is “excellent and
anything over 0.15 is unacceptable”
(http://www.analytictech.com/borgatti/mds.htm). Therefore, the stress score of
0.002 means that the fit is excellent and the results are valid.
It can be concluded from the MDS results that the “development” and
“hospitals,” “law” and “finance” sectors are closely connected to each other along
the lines of the measures of centrality in the network. There is cohesion among
certain sectors within the network while other sectors are outsiders of the
network. 20
Section Conclusion
Overall, the SNA results support a conclusion that a coherent political
network of elite relationships exists in governing Louisville health care apart from
elected government. The Bonacich centrality results identified growth coalition
20As mentioned above, there have been few studies of a community power structure using MDS.
The above cited studies (Laumann and Pappi and Galaskiewicz) were identified as utilizing this
method at the community level. The MDS results here have similarity to Galaskiewicz’s (1979)
smallest space analysis MDS (SSA-1) on an anonymous Midwestern community which suggests
that these results can be generalized.
20

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 21/45
hegemony both in terms of analysis of individual and organizational networks—
there was no branch plant representation in the elite group of individuals. The
clique analysis buttressed the centrality results by identifying that the two most
central cliques consist of local health care and growth coalition types. In terms of
the overall community network, the MDS results showed hospitals are closely
related to the law firms, and economic development organizations.21 Under the
premises of SNA, a reasonable conclusion is the relatively few elite actors at the
top of a steep eigenvalue gradient are the controlling parties making decisions in
the network.
FIELD INTERVIEWS
As discussed earlier, the SNA results suggested individual informants who
were central in the network of power in health care. Available and willing
central individuals were interviewed as well as other informants who were
identified to be authoritative. The interview questions sought to verify validity of
the SNA results, as well as explore areas of policy and structure. This section will
discuss those issues in addition to examining the role of local government, and the
role of doctors.
Who do the Central Players Say Move and Shake
Individuals
The informants identified health care movers and shakers in Louisville as
coming from one of four groups: health administrators, educational figures,
political figures, and board chairs of hospital organizations. Overall, individuals
21 Furthermore some sectors are distinctively not in this network, and some sectors (especially
doctors) are distinctively on the fringe of the central power.
21
8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 22/45
who were both community elites and executives were identified to be the movers
and shakers.
Organizations 22
There was a short list of key organizations. The leading three leading
hospital organizations (Norton, Jewish, and Baptist) were the most identified
leading organizational actors. The University of Louisville was identified next in
terms of frequency. Informants repeatedly identified the proprietary
organizations: Humana23, Kindred and Rescare24 as a third echelon and not
involved with the top tiers of actors. Given the list, informants saw the hospital
organizations as the main organizational players in local health care politics.
Sectors
Some informants framed answers in terms of sectors and acknowledged
that a great disconnect existed between the public and the private sectors.
Informants most frequently identified the Family Health Centers and the
Louisville Metro Health Department as the main public sector actors. The non-
profit hospital organizations were again identified as the primary movers and
shakers. Informants did not recognize the proprietary actors (Kindred and
Humana)25 as involved in local health care politics. Humana was identified as the
22
One respondent also said “I may be using the wrong term, the unions or the company, Ford,GE, UPS, are major players in this, and then you get into the health care companies themselves . . .
like Humana, Ventas.”23 As noted elsewhere Humana was first a Louisville-based proprietary health care organization
that then evolved into health insurance and then divested itself of hospitals. It is a hometown
company that wields sizeable influence.24 Rescare is a Louisville-based proprietary organization that primarily specializes in running
residential care facilities across the United States. The residential facilities historically have been
called “group homes.”25 Kindred’s home office is in Louisville, and they have one hospital in Louisville.
22

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 23/45
exception when it had owned three Louisville hospitals and had the management
contract for the University of Louisville Hospital for 13 years.
Where are the Doctors?
The informant comments affirmed the MDS results. Informants
consistently did not name doctors and only answered when asked the specific
question: How have you seen the role of doctors in the political realm?
The informants consistently confirmed that the physicians as a group in
Louisville are marginally involved in the local politics and do not wield power or
influence over community health care goals. Despite the existence of the Greater
Louisville Medical Society,26 informants did not recognize strong organization
among physicians at the community level and they are quiet unless they have
strong opinions on a particular issue.
However, informants consistently noted that physicians wield political
power at the institutional level. Physicians are economic drivers as they direct
business to the hospitals. One informant said that doctors did not have a strong
say until it was discovered that hospitals could “construct a lot of profit under the
guise of doctors’ offices” and that doctors are cheerleaders for a hospital getting
new equipment already in use at other hospitals. Another informant said a
specialist making significant revenue for a hospital has more pull and can extract
concessions.27
26 Historically, the Jefferson County/Greater Louisville Medical Society has facilitated a process
whereby a physician can apply for credentials at all the desired facilities in town through its
auspices.27 Informants repeatedly described physicians as independent business people who sell their time
and can influence placement of facilities. However, a change in the trend of doctors as
independent business people was noted by a number of informants as hospital organizations have
been hiring physicians (especially family practice doctors) as employees. The employed
23

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 24/45
On the other hand, some informants noted the Louisville Medical Center
as an exception in terms of physician political power and influence because of the
University of Louisville Medical School. The University of Louisville Medical
School dean is an agenda-setter. Medical school department chairs wield
influence over the placement and operation of indigent care services. However,
the responding informants said the Medical School’s influence stays within the
downtown Medical Center and does not extend to the larger community.28
Where is Greater Louisville Inc?
Like the doctors, Greater Louisville Inc (GLI) was not automatically
identified as a mover and shaker .29 This supports the SNA results when the
dataset was adjusted for skewness.
Most informants saw GLI driving research and economic development
agendas that involved health care but did not see GLI having a consistent role in
health care. Two informants cited the Boyle Report 30 of 1996 (commissioned by
GLI’s predecessor organization) as a source for understanding Louisville’s health
care agenda in economic development terms, but that was the extent of GLI
involvement in health care governance.
physicians are required to refer within the hospital organization and therefore hospital
organizations are controlling the referrals under the guise of an established continuum of care.
One informant declared that this is a ‘de facto’ closed staff system in place in the various hospitals
and the doctors are ceasing to be independent business people with mobility throughout the city to
practice in different hospitals.
28 One respondent suggested that as part of an overall agenda by the University of LouisvilleMedical School to build the “U of L” brand, it is looking to be a full competitor with Jewish,
Norton, and Baptist. There is some news coverage to that extent where U of L is contemplating
outpatient facilities outside the downtown Howington, (2007 July 12), but no other informant
confirmed this.29 Some informants identified the Health Enterprises Network, which is a “network” of GLI, but
few spontaneously mentioned GLI or the Health Enterprises Network as a player.30 The formal title of this was Economic Development Strategy for the Greater Louisville Region.
24

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 25/45
The informant responses reflect SNA indications that GLI as an
organization is a central cut point or juncture of relationships as opposed to a
central actor in health care politics. This is despite the face value evidence that
GLI has members who are active in health care politics including hospital
executives.
Where Are Local Government and the Mayor among the Players?
Like the doctors and GLI, informants did not consistently name the Mayor
of Louisville and Municipal/Metro Government as actors in health care politics.
This also validates the SNA centrality results. The question asked to elicit this
information was usually worded as: In your opinion, what is the Mayor’s and
Metro Government’s31 primary role in the health care system?
The Mayor
Informants generally saw the current Louisville Mayor, Jerry Abramson as
more involved in economic development issues pertaining to health care and not
in redistributive issues. He is a passive, but well informed behind-the scene
player who supports and cheers on development. Some informants said that the
Mayor will talk to executives in an effort to influence, but he does not wield
control over the hospital organization agendas. One informant said that there does
not appear any “mechanism” set up for the Mayor to be involved in identifying
health needs in the community.
Involvement by Metro Government as an Entity32
31 The term “Metro Government” is being used in lieu of the 2003 consolidation of Louisville and
Jefferson County, Kentucky governments.32 Louisville renamed its health department to be the “Department of Health and Wellness.”
25
8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 26/45
Overall, the informants saw that beyond the Mayor and the head of the
health department, Adewale Troutman M.D., the Louisville Metro (Consolidated)
Government is a minor, if not just a passive, player in health care politics. One
informant said,
I don’t think there are even positions established that the designation or
authority to really take that on beyond Dr. Troutman, and if there are positions, they’re relative weak positions, I am not talking individuals; I’m
talking positions that have somewhat perfunctory leadership roles.
A number of informants viewed Dr. Troutman as a credible and influential
opinion leader in the area of health disparities, and that the Mayor backs him.
Informants did not see the Louisville Metro Council as a central player in health
care politics.33 The bottom line is that the municipal government was not a
significant player in local health care politics.
Section Summary
This section reviewed the informants responses regarding the structure of
local health care politics in Louisville. Elected government and local elected
politicians are not the movers and shakers. Overall, the informants confirmed that
local health care politics is not a matter of formal government and controlled by a
small group of actors outside government.
What is the Agenda of the Local Players?
The question about the political agenda of the players did not have to be
asked in every interview, but in many cases the question was: Do you think that
33 Informants saw GLI as being the driver of the 2006 indoor smoking ban ordinance and the
Metro Council as only the official ratifying body. Informants saw the Mayor and the University of
Louisville president as the primary negotiators of the QCCT.
26

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 27/45
there is any particular agenda overall in this political realm? Informants gave a
variety of views.
Some informants saw the city agenda as a combination of the growth
agendas of the different hospital organizations. The different organizations have
their own strategic plans and cooperate when it does did not threaten the
organizational interests.34 A common theme among informants was that the
hospital organizations are competitors first and collaborators second. In this
context, basic market logic appears to determine the political positions. Overall,
a theme from most of the informants with an opinion on this was that the different
organizations do not want the competitors to have an advantage, and will go to
court to maintain parity in the marketplace.
Two examples of this cooperation were the joint venture of Norton Health
care, Jewish Hospital, and the University of Louisville to govern the University of
Louisville Hospital as University Medical Center Inc (UMC), and the formation
of the Louisville Medical Center Development Corporation (LMCDC). Despite
being competitors Norton and Jewish had a mutual desire to see Columbia HCA
leave town and so cooperated on governing a third hospital in the Louisville
Medical Center. The governance agreement lasted from 1996 until 2007 when
the University of Louisville terminated it for what some informants said were
development purposes.35
The LMCDC was formed about the same time that34 One example of this was cooperation by the hospital organizations to make a jointannouncement in May 2007 that all facilities would be smoke-free. Some informants said that this
was a way of preventing turnover and transience of employees from one organization to another in
order to smoke at work.35 Informants said that initially Jewish and Norton spent significant money to revitalize the
infrastructure of University Hospital, and that they could maintain a status quo in the area of
medical specialties. The board of directors had members from Jewish, Norton, and the University
of Louisville. However, University Hospital got stronger over time with the investment, and
27

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 28/45
Norton and Jewish entered into the UMC agreement that and backed away from it
about the same time they left UMC.36 Informants indicated that Norton and
Jewish decided that cooperation in this case stopped being in their interests.37
A third example of the informal cooperation around the development
agenda surrounded the closing of Southwest Hospital by Norton Healthcare and
the moving of the Certificate of Need (CON) to a new hospital that was opened in
a developing area of eastern Louisville in 2009. Informants suggested that
Norton, Jewish, and Baptist Healthcare all agreed on the need for growth and did
not challenge each others plans in front of the pertinent state planning body.
Some informants explicitly identified the health care politics agenda in
Louisville as economic development.38 Some informants also said that the agenda
includes national and international prestige, especially given the Abiocor
Artificial Heart implantation trials and the first hand transplants. Besides the
branding efforts, health care is recognized as a “hot issue” in the Louisville
economy and thus of political importance. One informant said,
conflict started when there was a push to upgrade certain specialty infrastructure that would
compete with the specialties of Norton and Jewish. Some informants reported that in the last
several months that Norton and Jewish participation, the conflict was so great that there was no
quorum so the University Medical Center board of directors could not meet. A dynamic in this
conflict was the University of Louisville has a state mandate to facilitate economic, development
and informants said that it is now the main leader in the health care development agenda.36 Norton and Jewish are still members of the LMCDC now “ Nucleus” but they are neither central
members nor do they give as much money to the organization as they previously did.37 In light of the detachment among the organizations within the Medical Center, a number of
informants questioned whether there was a future in cooperation in Louisville health care.
However, a number of informants saw cooperation as inevitable. The actors are connecting in
other ways. For example, Jewish and the University of Louisville had cooperated in creating a
cardiovascular research institute. One informant said that Norton and the University of Louisville
were looking for other ways to cooperate despite the break-up of the governance consortium of UMC. The organizations operating in the downtown Louisville Medical Center are still working
together in some form.
38 It was interesting that a number of actors acknowledged that this was the agenda, but also voiced
criticism of this agenda as it led to inequities and was not a solid basis for Economic
Development.
28

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 29/45
Health care has been seen not only because of the services it provides, but
as a way to provide lost manufacturing jobs so it is a critical service to the
quality of life to the people, but it’s also an economic cluster that isvalued by our community. So I see that city government and the Mayor
driving that role as well.
One informant said, “Our local government has a vested interest in the healthcare
system continuing to grow.”
The Political Modus Operandi
When it came to the modus operandi of the health care movers and
shakers, the general answer was that hospital executives and not board members
were the primary negotiators in local health care politics.
39
The chief executive
officers (CEO’s) and executive teams are the prime negotiators, because health
care has evolved into a highly complex industry.
The hospital executives talk both formally and informally. Some
informants said the hospital organization executives have conversations under the
auspices of the Kentucky Hospital Association (KHA). The executives of the
different organizations are on various KHA committees and have conversations in
a legal context that cannot be construed as fixing the market. However, other
informants reported that the executives of the different organizations have a
history of talking informally among themselves. The executives of the three
hospital organizations have a history of engaging in quid pro quo with regard to
different facility projects (i.e., we will not challenge you in front of the Certificate
of Need board on your particular project if you do not challenge us on our
project).
39 Informants reported that board members were not involved in outside informal negotiations with
board members from other hospitals on behalf of the respective hospital organizations. One
informant was emphatic that there are no such conversations that take place at “Fund for the Arts”
meetings or at work places.
29

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 30/45
The Lack of Network Connection between the Private and Public Sectors
As noted earlier, the MDS results showed a dramatic disconnect between
public health agencies and the private/non-profit organizations. As illustrated in
figures 1 and 2, the mental health and public health sectors were not part of the
network in the UCINET-generated Multidimensional Scaling (MDS) results in
figures 3 and 4. Why was this? The consistent answer from informants was that
the public sector agencies were required by federal law to be representative of the
community—to include consumers.
DISCUSSIONUpon investigating what constitutes the political structure of health care in
Louisville and talking to available individuals within that structure, the essential
conclusion is that when it comes to the local context the movers and shakers are
elite, locally dependent business interests embedded within the community. The
available informants also consistently confirmed that the agenda of these movers
and shakers is growth. Recognizing that, 1) a U.S. city, as a geopolitical entity is
subject to the political and regulatory structure of the state and national
governments, and 2) if any local health care policy can be locally shaped and
driven in Louisville, it is growth and development driven by the configuration of
actors called a growth machine.
The actors in their political dealings with each other have focused on what
growth and development can occur in terms of the interest of the actors. There
were obvious examples of the actors being united by growth opportunities, and
there was no evidence that the public was part of the discussions. The movers and
shakers in health care in Louisville are not doctors, nor local government nor the
30

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 31/45
general public, but a small, elite group that has the markers of the growth
coalition.
These growth machine findings build upon the older elitist findings on
local health care politics. Congruent with Wilson and Conant’s findings the non-
profit hospital organization executives in Louisville turned out to be the central
actors even though lawyers, developmental, and financial interests were on
hospital boards and appeared to be central in the network of relationships.
These findings also suggest that local non-profit hospitals as a sector could
be added to Molotch’s model of a growth coalition. Like the other growth
coalition livelihoods, hospitals (with a very few exceptions40) are locally
dependent on the area in which they serve for revenue. Local non-profit hospitals
are large employers and serve as an avenue of growth. Hospital organization
executives integrate into the local business community and align with the business
interests of the community. They serve on the boards of banks, charities and
other local institutions and become engage in elite relationships with other elite
business and economic figures.
Given the types of actors and the types of agenda, it appears that the local
responses to health care reform in Louisville within the larger political structure
of the Kentucky and federal levels of government will be along the lines of the
market concepts of growth and development. These elite actors and the agenda of
growth and development will be the political objects for study as to how the local
level responds to health reform. A possible market action in this case is
40 The Mayo Clinic and the Cleveland Clinic are two examples of hospitals that primarily draw
patients from outside their localities and regions, and which would be exceptions.
31

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 32/45
oligopolistic mergers of local non-profit hospital organizations. A related
question to explore pertains to the type of local market condition that engenders
proprietary ownership of former nonprofit hospitals and its relationship to the
local growth machine. (Are local economies where health care is a non-basic
sector more likely to have the presence of proprietary ownership?) More research
is needed to test for generalization of these findings in the United States context.
The results of this study could provide markers for researchers to identify local
health political structures and agendas in other communities to assist health care
payment reform efforts to achieve desired outcomes and impacts.
References
Adam, S. & Kriesi, H. (2007). The network approach. In P.A. Sabatier (ed).
Theories of the policy process (129-154). Boulder, CO: Westview Press.
Author, (2008) Title removed for blind review process
Belknap, I, & Steinle, J.G. (1963). The community and its hospitals: Acomparative analysis. Syracuse, NY: Syracuse University Press.
Blankeship, L.V. & Elling R.H. (1962). Organizational support and community
power structure: The hospital. Journal of Health and Human Behavior,
32

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 33/45
3:257-269. Downloaded from the J-STOR Database on June 9, 2006.
Blankeship, L.V. & Elling R.H.(1971) Effects of community power on hospitalorganization. In M.F. Arnold, L.V. Blankenship & J.M. Hess (Eds.)
Administering health systems: Issues and perspectives. Chicago: Aldine
Atherton.
Bodenheimer T.S. & Grumbach, K (2005). Understanding health policy: A
clinical approach (4ed) New York: Lange Medical Books/McGraw-Hill.
Borgatti, S. (1997) Multidimensional scaling. Retrieved September 8, 2007 from
http://www.analytictech.com/borgatti/mds.htm.
Borgatti, S.P., Everett, M.G. and Freeman, L.C. (2002). Ucinet for Windows:
Software for social network analysis. Harvard, MA: Analytic
Technologies.
Brass, D.J. & Burkhardt, M.E. (1992). Networks and organizations: structure,
form and action. Boston, MA: Harvard Business School Press.
Britton and Octavio (2007). Urban and spatial organization: Hospital and
orphanage location in Chicago, 1848-1916. Social Forces, 85: 1303-1317.
Clark, T.N. (1968).(Ed). Community structure and decision-making.
Comparative analyses. San Francisco: Chandler Publishing Company.
Conant, R.W. (1968) The politics of community health. Washington, D.C.:
Public Affairs Press.
Cox, K.R. & Mair, A. (1988). Locality and community in the politics of local
economic development. Annals of the Association of American
Geographers, 78: 307-325.
Dahl, R.A. (1961). Who Governs? Democracy and power in an American city.
New Haven CT.: Yale University Press.
Elling R.H. & Lee, O.J. (1966). Formal connections of community leadership to
the health system. The milbank memorial fund quarterly, 44:294-306.Retrieved March 3, 2008 from the Proquest database.
Freeman, L.C. (1978). Centrality in social networks conceptual clarification.Social Networks, 1:215-239.
Galaskiewicz, J. (1979). The structure of community organizational networks.
Social Forces, 57:1346-1364. Retrieved February 9, 2008 from the J
33

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 34/45
-STOR database.
Gentile-O’Donnell, D. (2004) An historical analysis of public politics, andhealthcare delivery. (Doctoral dissertation, University of Pennsylvania,
2004).
Ginzburg, E. (1977) Regionalization & health policy. Washington D.C.: U.S.
Department of Health Education and Welfare. Public Health Service
Health Resources Administration. DHEW Publication No. (HRA) 77-623 (Govt. Printing Office.
Green, E. (2007, February 16) LMCDC reorganization will shift control to
university. [Electronic Version] Business First of Louisville.
Hanneman, R. A. & Riddle.M. (2005). Introduction to social network methods.
Riverside, CA: University of California, Riverside. Retrieved February 4,
2007From http://faculty.ucr.edu/~hanneman/ )
Hunter, F. (1953) Community power structure. Chapel Hill NC: The University
of North Carolina Press.
Knoke, D. & Kuklinski, J.H. (1982). Network analysis. Newbury Park, CA:Sage.
Laumann, E.O. & Pappi, F.U. (1973). New directions in the study of communityelites. American Sociological Review, 38:212-230. Downloaded from the
J-STOR database on January 19, 2008.
Laumann, E.O., Galaskiewicz, J., Marsden, P.V. (1978). Community structure as
interorganizational linkages. Annual Review of Sociology, 4: 455-484.
Downloaded from the J-STOR database on February 9, 2008.
Lennarson-Greer A (1997) Urban Health Politics in R.K. Vogel (Ed.) Handbook
of Research on urban politics and policy in the United States. (pp.356-371). Westport, CT: Greenwood Press.
Litman, T.J & Robins, L.S. (1984). Health politics and policy. New York: JohnWiley and Sons.
Logan, J.R. & Molotch, H.L. (1987). Urban fortunes: The political economy of place. Berkley University of California Press.
Logan, J.R. & Molotch, H.L. (2007). Urban fortunes: The political economy of
place with a new preface 20th anniversary edition. Berkley University of
34
8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 35/45
California Press.
Molotch, H. (1976). The city as a growth machine: Toward a political economy of place. American Journal of Sociology, 82:309-332.
Moore,G. & Whitt, J.A. (2000). Gender and networks in a local voluntary-sector elite. Voluntas: International Journal of Voluntary and Nonprofit
Organizations, 11: 309-328.
Morone, J.A. (1982). The dilemma of citizen action: Representation and
bureaucracy in local health politics. (Doctoral Disseration University of
Chicago, 1982).
Multidimensional scaling. Retrieved September 9, 2007 from
http://www.analytictech.com/networks/mds.htm.
Peterson, P.E. (1981). City limits. Chicago: University of Chicago Press.
Plano, J.A. (1999) Communities of interest: Making metropolitan hospitalmarkets in Milwaukee and Toronto 1969-1994. (Doctoral dissertation:
University of Wisconsin-Milwaukee, 1999).
Robert Wood Johnson Foundation (2007, April). Communities in charge:Financing and delivering heath care to the uninsured grant results.
Retrieved October 17, 2007 from
http://www.rwjf.org/reports/npreports/cic.htm
Robert Wood Johnson Foundation (2010, June) Charting a path for healthcare
payment reform: Recommendations from the field. Retrieved July 1, 2010from http://www.rwjf.org/pr/product.jsp?id=64971
Schussler, N.C. (1994) A public-private partnership for providing indigent healthcare through corporatist mediation: A critical evaluation of the Humana
partnership. (Doctoral dissertation, University of Louisville, 1994).
Scott, J. (1991). Social network analysis: A handbook. London: Sage Publications
Ltd.
Starr, P. (1982) The social transformation of American medicine. New York:
Basic Books Inc.
Statsoft Inc. (2003). Multidimensional scaling. Retrieved September 8, 2007 from
http://www.statsoft.com/textbook/stimulsca.html.
Swanson, B.E. (1 972) The politics of health. In H.E. Freeman, S. Levine, & L.G.
Reeder (Eds.), Handbook of Medical Sociology (2nd ed.) (pp. 435-455).
Englewood Cliffs, NJ: Prentice-Hall, Inc.
35

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 36/45
Tulchinsky, T.H. & Varavikova E.A. (2000). The new public health: An
introduction for the 21st century. San Diego: Academic Press.
University Medical Center Incorporated (1996). Affiliation agreement.
Vogel, R.K. (1992). Urban political economy: Broward County, Florida.
Gainesville: University of Florida Press.
Wasserman, S. & Faust, K. (1993) Social network analysis: Methods and
applications. New York: Cambridge University Press.
Wilson, R.N. (1968) Community structure and health action: A report on processanalysis. Washington, D.C.: Public Affairs Press.
Table 1
The political players of the local growth coalition
____________________________________________________________
The major players__________________________________________________
Property Investing
Development
36
8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 37/45
Real Estate Financing
Politicians
Local Media
Utilities
____________________________________________________________
The Auxiliary Players_______________________________________________
Universities
Theaters, Museums, Expositions
Professional Sports
Organized Labor
Self-employed professionals
Small retailers
_____________ _____________________________________________
(Logan and Molotch, 1987, pp.62-85)
Table 2
Top 20 Bonacich Eigenvalues Values for Louisville organizations in 2005____
Organization Eigenvalue Score
Greater Louisville Inc……………………………………………………...133.024
Fund for the Arts…………………………………………………………....22.059
Jewish Hospital Healthcare Services……………………………………….18.475
Frost Brown Todd Law Firm……………………………………………….15.096
37
8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 38/45
Norton Healthcare……………………………………………………….….12.143
Louisville Development Foundation………………………………………..10.875
University of Louisville Hospital/University Medical Center…………….…8.269
Louisville Medical Center Development Corporation……………………….8.238
Louisville/Jefferson County Metro Government…………………………….8.098
Anthem Health Plans of Kentucky…………………………………………...7.928
Republic Bank and Trust………………………………………….………….7.765
Fund for the Arts Properties Foundation…………………………………….7.305
Metro United Way……………………………………………………………6.786
Leadership Louisville…………………………………………….…………...6.729
Baptist Healthcare System………………………….…………………….…..6.014
Wyatt Tarrant and Combs Law Firm……………….………………………..5.604
Alliance for Life Science Technology Commercialization, Inc………….….5.567
U of L and Jewish Hosp. Cardiovascular Institute……………………….….5.131
Getcare Health Network………………………………………………..…….5.024
Kindred Healthcare……………………………………………………….…..4.797 _________________________________________________________________
_
Table 3
Top 20 organization Bonacich Eigenvalues with GLI removed from dataset
Organization Eigenvalue Score
Frost Brown Todd…………………………………………………..…..…130.022
Jewish Hospital Health Services………………………………………….....51.801
Republic Bank and Trust…………………………………………………....11.995
38
8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 39/45
Fund for the Arts……………………………………………………………..7.548
Leadership Louisville…………………………………………………………6.948
Louisville Development Foundation……………………………………….....5.477
Yum Brands…………………………………………………………….…….4.738
Metro United Way……………………………………………………………4.442
Fund for the Arts Properties Foundation……………………………………..3.107
Republic Bank and Trust—Indiana………………………………………..…2.758
Branch Bank and Trust (BB&T)……………………………………………...2.666
Goldberg and Simpson Law Firm…………………………………………….2.596
Indiana University Southeast…………………………………………………2.425
Actors Theatre…………………………………………………………….…..2.309
U of L/Jewish Hospital Cardiovascular Institute……………….…………….2.063
Home of the Innocents………………………………………………………..2.038
Baptist Healthcare System………………………………………….………...1.965
Louisville Zoo Foundation……………………………………………………1.898
Lynch Cox Gilman Maher Law Firm………………………………………...1.702
Getcare Health Network (now defunct)………………………………………1.602
_________________________________________________________________
_
Table 4
Top 20 individual Bonacich eigenvalues in 2005 with their economic sectors
Individual actor_______________________________________Eigenvalue score
M1476 (Attorney) ………………………………………………………..…27.005
M0031 (Healthcare) ………………………………………………………...23.252
M2985 (Utilities)……………………………………………………………22.823
39

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 40/45
M3715 (Healthcare)………………………………………………………....22.777
M2868 (Education)………………………………………………………….22.315
M0044 (Politician)…………………………………………………………..21.642
M3590 (Health Insurance)…………………………………………………..21.392
M1656 (Development)………………………………………………………20.680
W1259 (Healthcare)…………………………………………………………20.654
M3389 (Development)………………………………………………………20.506
M1799 (Finance)…………………………………………………………….19.563
M2919 (Development)………………………………………………………19.115
M3747 (Education)………………………………………………………….19.115
W1084 (Development)……………………………………………………...19.115
M1611 (Attorney)…………………………………………………………...12.925
M0634 (Healthcare)…………………………………………………………12.687
M3559 (Healthcare)…………………………………………………………12.237
M3682 (Healthcare)…………………………………………………………12.156
M2338 (Health-related field)………………………………………………..11.757 _________________________________________________________________
_
Table 5
Individual Bonacich eigenvalues with GLI cases removed from dataset___
Individual actor_______________________________________Eigenvalue score
M1476(Attorney)…………………………………………………….……..29.256
W0497 (Banking)………………………………………………….………..15.593
M0568(Attorney)…………………………………………………………...11.579
40
8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 41/45
M1552 (Charity)……………………………………………………………11.498
W0207 (Attorney)………………………………………………………….11.160
M0242 (Attorney)…………………………………………………………..11.153
M2633 (Attorney)…………………………………………………………..11.148
M1562 (Attorney)…………………………………………………………..11.080
M2822 (Attorney)…………………………………………………………..11.080
M0061 (Attorney)…………………………………………………………..10.984
M0098 (Attorney)…………………………………………………………..10.984
M0119 (Attorney)…………………………………………………………..10.984
M0127 (Attorney)…………………………………………………………..10.984
M0157 (Attorney)…………………………………………………………..10.984
M0176 (Attorney)…………………………………………………………..10.984
M0273 (Attorney)…………………………………………………………..10.984
M0275 (Attorney)…………………………………………………………..10.984
M0282 (Attorney)…………………………………………………………..10.984
M0301 (Attorney)…………………………………………………………..10.984
M0390 (Attorney)…………………………………………………………..10.984
_________________________________________________________________
_
Table 6
Clique with highest average Bonacich eigenvalue score with sectors.
Actor with corresponding sector
1. M0031 (Healthcare)
2. M0634 (Healthcare)
41

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 42/45
3. M1476 (Attorney)
4. M1542 (Physician)
5. M2004 (Physician)
6. M2357 (Development)
7. M2868 (Education)
8. M3065 (Local Business Executive)
9. M3559 (Healthcare)
10. M3634 (Healthcare)
11. M3682 (Healthcare)
12. M3715 (Healthcare) _________________________________________________________________
_
Table 7
Clique#106 with second highest average eigenvalue score with sectors.
Actor and economic sector
1. M0031 (Health care)
2. M0044 (Politician)
42

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 43/45
3. M0093 (Local Professional)
4. M0465 (Local Business Executive)
5. M0669 (Health care)
6. M0997 (Health care)
7. M2868 (Education)
8. M3081 (Health care)
9. M3389 (Development)
10. M3559 (Health care)
11. M3715 (Health care)
12. W1259 (Health care) _________________________________________________________________
_
43

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 44/45
Figure 1: Initial MDS result of sectors in the Louisville, KY Metropolitan
Area
5
4
3
2
1
0
- 1
- 2
A ccountantsA dvert isingA rtsB r a n c hCollegesDeve lopmentDoctorsEliteFinanceFoundationG o v e r n m e n t
HR B
Heal thcareHospitalsInsuranceLa wMHMediaNationalNonprof i tOther PIPoliticians
Public
RetailersSportsTechno logyUtilities
44

8/7/2019 Unpacking the puzzle of Local Healthcare Politics
http://slidepdf.com/reader/full/unpacking-the-puzzle-of-local-healthcare-politics 45/45
Figure 2: magnification of the cluster of sectors in the Louisville KY area
0.066
0.065
0.064
0.063
0.062
0.061
0.06
0.059
0.058
0.057
0.056
0.055
0.054
0.053
0.052
0.051
0.05
0.049
0.048
0.047
0.046
0.045
0.044
0.043
0.042
0.041
0.04
0.039
0.038
Accountants
Advertising
Arts
Branch
Colleges
Development
Doctors
Elite
Finance
Foundation
Government
Healthcare
Hospitals
Insurance
Law
MH
Media
National
Nonprofit
Other
PI
Politicians
Retailers
Sports
Technology
Utilities


















