
University of Groningen Essential fatty acid deficiency ...
19
University of Groningen Essential fatty acid deficiency and the small intestine Lukovac, Sabina IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document version below. Document Version Publisher's PDF, also known as Version of record Publication date: 2010 Link to publication in University of Groningen/UMCG research database Citation for published version (APA): Lukovac, S. (2010). Essential fatty acid deficiency and the small intestine. s.n. Copyright Other than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons). The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license. More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne- amendment. Take-down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons the number of authors shown on this cover page is limited to 10 maximum. Download date: 14-10-2021
Transcript of University of Groningen Essential fatty acid deficiency ...
University of Groningen
Essential fatty acid deficiency and the small intestineLukovac, Sabina
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2010
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Lukovac, S. (2010). Essential fatty acid deficiency and the small intestine. s.n.
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license.More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne-amendment.
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 14-10-2021
CHAPTER 6
GELUCIRE®44/14 IMPROVES FAT ABSORPTION IN RATS WITH
IMPAIRED LIPOLYSIS
S. Lukovac1, K.E.G. Gooijert
1, P.C. Gregory
2, G. Shlieout
2, F. Stellaard
1, E.H.H.M.
Rings1, H.J. Verkade
1
(1) Pediatric Gastroenterology, Department of Pediatrics, Beatrix Children’s Hospital,
Groningen University Institute for Drug Exploration (GUIDE), Center for Liver, Digestive
and Metabolic Diseases, University of Groningen, University Medical Center Groningen,
Groningen, The Netherlands.
(2) Solvay Pharmaceuticals GmbH, Hannover, Germany.
Manuscript conditionally accepted for publication in Biochimica et Biophysica
Acta (BBA) Molecular and Cell biology of lipids

CHAPTER 6
112
ABSTRACT
Clinically relevant fat malabsorption is usually due to impaired intestinal fat digestion
(lipolysis) and/or to impaired solubilization of the lipolytic metabolites. We hypothesized
that Gelucire®44/14 –a semi-solid self-micro-emulsifying excipient– could increase fat
absorption. In relevant rat models for impaired lipolysis or for impaired solubilization we
tested whether administration of Gelucire®44/14
enhanced fat absorption. Rats with
impaired lipolysis (lipase inhibitor Orlistat-diet) and rats with reduced solubilization
(permanent bile diversion) underwent a 72h fat balance test to assess fat absorption.
The absorption kinetics of a stable isotope-labeled fatty acid was assessed in rats with
reduced solubilization, in the presence or absence of Gelucire®44/14. Gelucire
®44/14
improved fat absorption in rats with impaired lipolysis (from 70% to 82%, p<0.001). In
rats with reduced solubilization, Gelucire®44/14 did not increase fat absorption nor did it
reconstitute the absorption kinetics of 13
C-labeled palmitate, compared with control rats
administered buffer without Gelucire®44/14.
The present data show that Gelucire®44/14 might enhance fat absorption under
conditions of impaired lipolysis, but not during impaired solubilization. We speculate that,
due to its self-micro-emulsification properties, Gelucire®44/14 stabilizes and improves
residual lipolytic enzyme activity in vivo, which could be of therapeutic value in clinical
conditions of fat malabsorption due to impaired lipolysis.
GELUCIRE®44/14 AND FAT ABSORPTION
113
6
CH
AP
TE
R
INTRODUCTION
Dietary fat is mainly composed of triglycerides, which undergo several intraluminal
processes before their absorption in the form of fatty acids and monoacylglycerides by
the small intestinal enterocytes.1 The first step of fat absorption involves emulsification
and hydrolysis by gastric lipase, which results in partial hydrolysis of triglycerides into
free fatty acids and diglycerides. The remaining partially digested and undigested,
triglycerides are digested by pancreatic lipases in the small intestine, which leads to
lipolysis into free fatty acids and monoglycerides. Subsequent steps involve micellar
solubilization with bile salts, phospholipids and cholesterol, transport to the enterocytes,
and translocation of the fatty acids and monoacylglycerides across the apical brush
border of the enterocytes. Under physiological conditions the pancreas produces
sufficient amounts of pancreatic lipases. However, under conditions of severe pancreatic
insufficiency, lipolysis may be incomplete and fat malabsorption occurs.2
Cystic fibrosis (CF), a common autosomal recessive disorder, is a condition in which
pancreatic secretory function is frequently affected.3 On top of impaired lipolysis, CF
patients often have solubilization defects, which may be due to changes in bile
production and composition, impaired pancreatic and intestinal bicarbonate secretion,
and/or changes in the intestinal microclimate.4,5,6
The combination of impaired lipolysis
and solubilization in CF patients can lead to severely reduced absorption of dietary fats
and to essential fatty acid deficiency.7,8
Several attempts to correct for low fat absorption,
for example with pancreatic enzyme replacement therapies and linoleic acid
supplementations, have shown variable effects in CF patients.9,10,11,12
Gelucire®44/14 is a semi-solid, self-emulsifying excipient frequently used in the
pharmaceutical industry as an enhancer of absorption of poorly soluble and poorly
bioavailable drugs.13,14
Gelucire®44/14 is composed of surfactants (mono- and diesters
of polyethylene glycol), co-surfactants (monoglycerides), and an oily phase (di- and
triglycerides). In vitro, Gelucire®44/14 has been shown to maintain the activity of
pancreatic enzymes under unfavorable conditions at low pH (Patent WO 2005/092370).
Moreover, Fernandez et al. have demonstrated that Gelucire®44/14 is a good substrate
for digestive enzymes.15
However, it remains unclear whether the efficacy of
Gelucire®44/14 is exclusively related to increasing the acid stability of pancreatic lipase,
and thereby to increasing lipolysis of dietary lipids. Alternatively, the mechanism of fat
malabsorption in CF is not exclusively related to impaired lipolysis. Thus it seems
feasible that Gelucire®44/14 might enhance net fat absorption by increasing the
solubilization of the lipolytic metabolites (free fatty acids and monoglycerides) and
thereby improve present CF therapy. Therefore, studies have been performed to test the
effects of Gelucire®44/14 on fat absorption in animals with induced fat malabsorption. In
order to address the potential, specific roles of Gelucire®44/14 in lipolysis and
solubilization of fat in vivo, we used validated rat models for either impaired lipolysis or
for severely reduced solubilization. Rats fed the lipase-inhibitor Orlistat (Xenical®) have a
selectively inhibited hydrolysis of dietary triglycerides, but unaffected
solubilization.16,17,18,19
On the other hand, rats with permanent bile diversion (BDD rats)
are a well characterized model to assess fatty acid uptake under condition of
(exclusively) reduced solubilization.18,20
CHAPTER 6
114
MATERIAL AND METHODS
Compounds
Taurocholate, phosphatidylcholine and cholesterol were purchased by Sigma Chemical
(St. Louis, USA). 13
C-labeled palmitic acid (C16:0) was purchased from Isotec Inc.
(Matheson, USA). Gelucire®44/14 was a generous gift from Solvay Pharmaceuticals
GmbH (Hannover, Germany). Orlistat (tetrahydrolipstatin, Xenical®) was obtained as
capsules containing 120 mg active compound from Roche Nederland B.V. (Mijndrecht,
The Netherlands).
Animals and diets
Male Wistar rats (Harlan, Zeist, The Netherlands), weighing 300-350 g, were housed in a
light-controlled (lights on 7 AM - 7 PM) and temperature-controlled facility with free
access to food and tap water, and, in the case of bile-diverted rats, saline (0.9% NaCl
w/v). The experimental protocol was approved by the Ethics Committee for Animal
Experiments, Faculty of Medical Sciences, University of Groningen, The Netherlands.
A semi-synthetic high-fat diet containing 16 weight% fat (4141.07) and the same diet
containing Orlistat (4141.07 + 200 mg/kg Orlistat) were produced by Arie Blok BV
(Woerden, The Netherlands). The diet contained 35 energy% fat and 16.2 wt% long-
chain fatty acids (fatty acid composition (in mol%): palmitic acid (C16:0), 39.0%; stearic
acid (C18:0), 4.0%; oleic acid (C18:1n-9), 31.7%; linoleic acid (C18:2n-6), 22.9%).
Gelucire®44/14 (1 wt% or 2 wt%) was mixed into the semi-synthetic high-fat diet or into
the semi-synthetic high-fat diet containing Orlistat.
Infusates and intraduodenal infusions
Infusates and bolus were prepared as described previously.20
Buffer contained 10 mM
HEPES and 135 mM NaCl (negative control). Model bile contained 60 mM taurocholate,
8 mM phosphatidyl choline and 1 mM cholesterol (positive control). Gelucire®44/14-
infusates contained buffer with 0.1% or 0.5% Gelucire®44/14.
Bolus (500 μl) was administered intraduodenally and composed of olive oil (25%),
medium chain triglyceride oil (75%; (composed of extracted coconut oil and synthetic
triglycerides; fatty acid composition: 6:0, 2%; 8:0, 50-65% max.;10:0, 30-45%; 12:0, 3%
max.) and 10 mg of 13
C-labeled palmitic acid (> 99% enriched) per 300 g body.20,18
Fat balance study in rats with impaired lipolysis
After a run-in period of two weeks on the semi-synthetic high-fat diet (4141.07) the fat
absorption was assessed during a 72 hours period in individually housed rats.
Subsequently, the rats fed the Orlistat containing diet for two weeks. At the end of the
two weeks, fat absorption test was performed again. Consistent with previous studies
with Orlistat feeding in rats, two weeks of Orlistat-diet (200 mg/kg) was sufficient to
decrease the net fat absorption.17
Next, one group of rats received the Orlistat-diet with
additional 1 wt% Gelucire®44/14 and another group of rats received the Orlistat-diet with
2 wt% Gelucire®44/14 for one additional week. At the end of the experimental week food
intake was determined and feces were collected for the assessment of the fat absorption
upon Gelucire®44/14 feeding. Net fat absorption was determined by measuring the fatty
GELUCIRE®44/14 AND FAT ABSORPTION
115
6
CH
AP
TE
R
acid intake and excretion by fatty acid methylation as described in section “Analytical
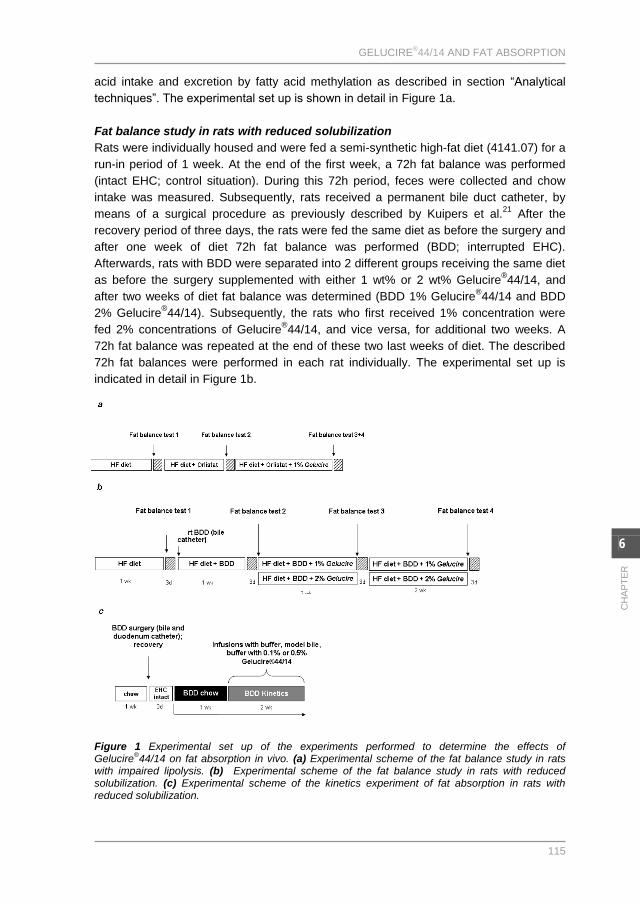
techniques”. The experimental set up is shown in detail in Figure 1a.
Fat balance study in rats with reduced solubilization
Rats were individually housed and were fed a semi-synthetic high-fat diet (4141.07) for a
run-in period of 1 week. At the end of the first week, a 72h fat balance was performed
(intact EHC; control situation). During this 72h period, feces were collected and chow
intake was measured. Subsequently, rats received a permanent bile duct catheter, by
means of a surgical procedure as previously described by Kuipers et al.21
After the
recovery period of three days, the rats were fed the same diet as before the surgery and
after one week of diet 72h fat balance was performed (BDD; interrupted EHC).
Afterwards, rats with BDD were separated into 2 different groups receiving the same diet
as before the surgery supplemented with either 1 wt% or 2 wt% Gelucire®44/14, and
after two weeks of diet fat balance was determined (BDD 1% Gelucire®44/14 and BDD
2% Gelucire®44/14). Subsequently, the rats who first received 1% concentration were
fed 2% concentrations of Gelucire®44/14, and vice versa, for additional two weeks. A
72h fat balance was repeated at the end of these two last weeks of diet. The described
72h fat balances were performed in each rat individually. The experimental set up is
indicated in detail in Figure 1b.
Figure 1 Experimental set up of the experiments performed to determine the effects of Gelucire
®44/14 on fat absorption in vivo. (a) Experimental scheme of the fat balance study in rats
with impaired lipolysis. (b) Experimental scheme of the fat balance study in rats with reduced solubilization. (c) Experimental scheme of the kinetics experiment of fat absorption in rats with reduced solubilization.

CHAPTER 6
116
Kinetics of fat absorption in rats with reduced solubilization
Rats were fed standard chow and received permanent catheters in bile duct and
duodenum as previously described by Kuipers et al.21
After the surgery, bile duct and
duodenum catheters were connected with each other at the skull of the rat for at least
three days to restore the enterohepatic circulation, in order to allow the rats to recover
from surgery. Subsequently, catheters of bile duct and duodenum were chronically
interrupted, resulting in permanent intestinal bile-deficiency. On the day of the
experiment, rats were infused intraduodenally for 7 hours (flow rate 1.5 ml/h) with buffer
(negative control), model bile (positive control), and with Gelucire®44/14-buffer
containing 0.1% or 0.5% Gelucire®44/14. The infusion rate and concentrations of bile
components were selected to reflect the physiological rates of bile flow and of the
intestinal delivery of specific bile components in adult Wistar rats. After starting the
intraduodenal infusion, 500 μl of fat per 300 gram body weight was administered slowly
as a bolus (olive oil, medium chain triglyceride oil and 13
C-labeled palmitic acid) via the
intraduodenal catheter. Medium chain triglyceride oil was included in the bolus in order to
obtain a reliable, reproducible vehicle for the quantitative administration of the labelled
compound, without introducing a profound increase in the intake of long-chain fatty
acids.22
The fat bolus represented approximately 15% of the daily fat intake of the semi-
synthetic high-fat diet. Blood samples (approximately 200 μl) were taken from the tail
vein at base line and every hour for 6 hours after administration of the fat bolus. The
baseline sample was taken prior to the administration of the fat bolus. Plasma and
erythrocytes were separated by centrifugation (2000 rpm, 10 min at 4˚C) and afterwards
stored at -20˚C until further analysis. Rats were used as their own controls during the
experiment, which was performed four times during the two weeks subsequent to the
chronic interruption of the bile duct (with different infusates); the above described
intraduodenal infusion conditions were performed in each rat individually. The
experimental set up is shown in detail in Figure 1c.
Analytical methods
Fatty acid analysis in chow and feces
Feces and chow were freeze-dried and homogenized mechanically. From aliquots of
feces and chow, lipids were extracted, hydrolyzed and methylated according to Muskiet
et al.23
Resulting fatty acid methyl esters were analyzed by gas chromatography to
calculate ingestion and fecal excretion of major fatty acids. Fatty acids were quantified
using heptadecanoic acid (C17:0) as internal standard. Total fecal fat excretion was
calculated from the daily fat intake and the daily fecal fat excretion and expressed as a
percentage of the daily fat intake as indicated in the following formula:
Fat intake (g day-1
) – Fecal fat output (g day-1
)
Percentage of total fat absorption = x100%
Fat intake (g day-1
)
Plasma lipids
Total lipids of plasma samples were extracted, hydrolyzed and methylated for gas-
chromatographic analysis of fatty acid profile as described by Muskiet et al.23
13
C
enrichment of fatty acid methyl esters was determined on a gas chromatography
GELUCIRE®44/14 AND FAT ABSORPTION
117
6
CH
AP
TE
R
combustion isotope ratio mass spectrometer (GC-C-IRMS). The concentration of 13
C
fatty acid in plasma at each time point was calculated from the fatty acid concentration
and 13
C enrichment and expressed as the percentage of the dose administered per ml
plasma (%dose/ml).20
Statistical analysis
Statistical analyses were performed using analysis of variance (One-Way ANOVA)
followed by post-hoc analysis (Bonferroni) using the SPSS version 12.0.2 software
(Chicago, IL, USA). For all experiments, p-values below 0.05 were considered
statistically significant.
RESULTS
After bile diversion, rats transiently lost up to 10% of their body weight. However, body
weights returned to normal within days (data not shown). There was no significant
difference in body weight between rats fed Orlistat and rats fed control high fat diet, or
between rats fed Orlistat and rats fed Orlistat with additional Gelucire®44/14 (data not
shown).
Dietary Gelucire®44/14 increases food intake in rats with reduced lipolysis and
solubilization, but increases fecal fat excretion exclusively in rats with reduced
solubilization
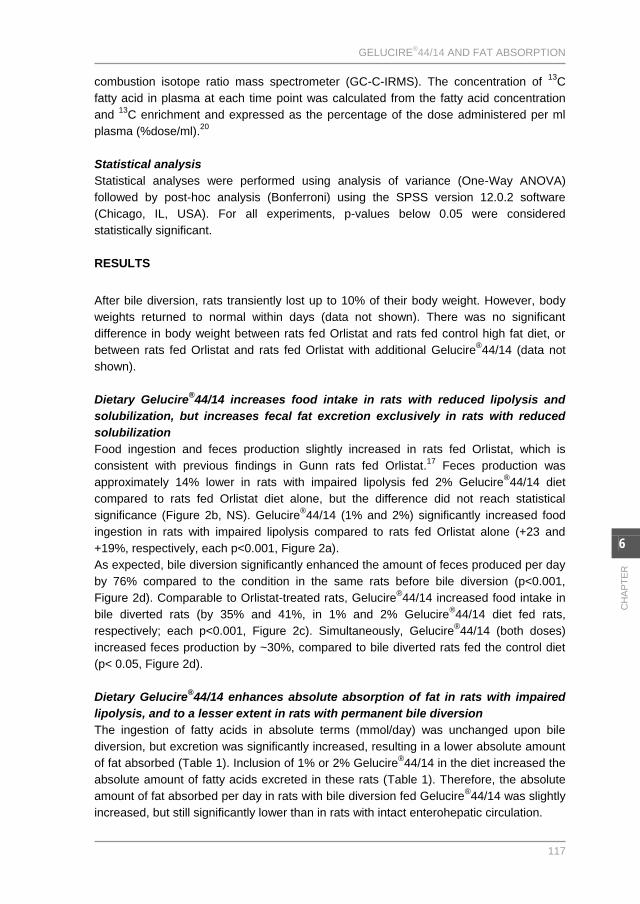
Food ingestion and feces production slightly increased in rats fed Orlistat, which is
consistent with previous findings in Gunn rats fed Orlistat.17
Feces production was
approximately 14% lower in rats with impaired lipolysis fed 2% Gelucire®44/14 diet
compared to rats fed Orlistat diet alone, but the difference did not reach statistical
significance (Figure 2b, NS). Gelucire®44/14 (1% and 2%) significantly increased food
ingestion in rats with impaired lipolysis compared to rats fed Orlistat alone (+23 and
+19%, respectively, each p<0.001, Figure 2a).
As expected, bile diversion significantly enhanced the amount of feces produced per day
by 76% compared to the condition in the same rats before bile diversion (p<0.001,
Figure 2d). Comparable to Orlistat-treated rats, Gelucire®44/14 increased food intake in
bile diverted rats (by 35% and 41%, in 1% and 2% Gelucire®44/14 diet fed rats,
respectively; each p<0.001, Figure 2c). Simultaneously, Gelucire®44/14 (both doses)
increased feces production by ~30%, compared to bile diverted rats fed the control diet
(p< 0.05, Figure 2d).
Dietary Gelucire®44/14 enhances absolute absorption of fat in rats with impaired
lipolysis, and to a lesser extent in rats with permanent bile diversion
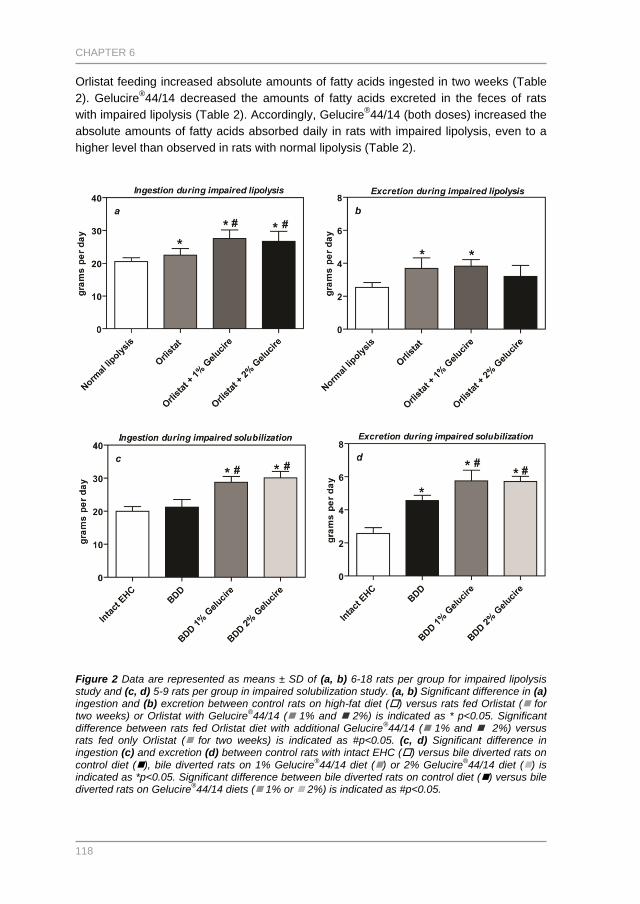
The ingestion of fatty acids in absolute terms (mmol/day) was unchanged upon bile
diversion, but excretion was significantly increased, resulting in a lower absolute amount
of fat absorbed (Table 1). Inclusion of 1% or 2% Gelucire®44/14 in the diet increased the
absolute amount of fatty acids excreted in these rats (Table 1). Therefore, the absolute
amount of fat absorbed per day in rats with bile diversion fed Gelucire®44/14 was slightly
increased, but still significantly lower than in rats with intact enterohepatic circulation.
CHAPTER 6
118
Orlistat feeding increased absolute amounts of fatty acids ingested in two weeks (Table
2). Gelucire®44/14 decreased the amounts of fatty acids excreted in the feces of rats
with impaired lipolysis (Table 2). Accordingly, Gelucire®44/14 (both doses) increased the
absolute amounts of fatty acids absorbed daily in rats with impaired lipolysis, even to a
higher level than observed in rats with normal lipolysis (Table 2).
Figure 2 Data are represented as means ± SD of (a, b) 6-18 rats per group for impaired lipolysis study and (c, d) 5-9 rats per group in impaired solubilization study. (a, b) Significant difference in (a) ingestion and (b) excretion between control rats on high-fat diet () versus rats fed Orlistat ( for two weeks) or Orlistat with Gelucire
®44/14 ( 1% and 2%) is indicated as * p<0.05. Significant
difference between rats fed Orlistat diet with additional Gelucire®44/14 ( 1% and 2%) versus
rats fed only Orlistat ( for two weeks) is indicated as #p<0.05. (c, d) Significant difference in ingestion (c) and excretion (d) between control rats with intact EHC () versus bile diverted rats on control diet (), bile diverted rats on 1% Gelucire
®44/14 diet () or 2% Gelucire
®44/14 diet () is
indicated as *p<0.05. Significant difference between bile diverted rats on control diet () versus bile diverted rats on Gelucire
®44/14 diets ( 1% or 2%) is indicated as #p<0.05.
GELUCIRE®44/14 AND FAT ABSORPTION
119
6
CH
AP
TE
R
Gelucire®44/14 (2%) increases net fat absorption in rats with impaired lipolysis,
but has no effect on net fat absorption in rats with permanent bile diversion
We analyzed the relative fat absorption from the fat balance. Orlistat administration significantly decreased net fat absorption in rats already after one week from 88% in control rats to approximately 70%, attributed to reduced lipolytic activity of lipases (data not shown). An additional week of Orlistat feeding did not further reduce net fat absorption (Figure 3a), neither did an additional 2 weeks (data not shown). This was in agreement with previous findings in Gunn rats.
17
Table 1 Absolute dietary fat ingestion, excretion and absorption in rats with intact EHC (control), bile diverted rats on control diet (BDD) and bile diverted rats on diet supplemented with 1% or 2% Gelucire
®44/14 (BDD 1% Gelucire
®44/14 and BDD 2% Gelucire
®44/14, respectively). Data are
means ± SD of 5-9 rats per group. Mean values represent the average of 72h per rat. *p<0.05 versus control rats with intact EHC. #p<0.05 versus BDD rats on control diet.
The 1% dose of Gelucire®44/14 did not significantly affect net fat absorption in rats fed
Orlistat (72%, NS), but 2% Gelucire®44/14 significantly increased the net fat absorption
reaching close to physiological values (82%, p<0.001, Figure 3a). In accordance with
previous observations, bile diversion lowered net fat absorption to 45% (Figure 3b).22
However, in these rats net fat absorption was not significantly altered by either dosage of
Gelucire®44/14 compared to fat absorption in the same rats on control diet without
Gelucire®44/14 (both 52%, NS, Figure 3b).
Table 2 Absolute dietary fat ingestion, excretion and absorption in control rats, rats fed control diet with Orlistat for one week or two weeks, and rats fed control diet with Orlistat for three weeks with additional Gelucire
®44/14 during the last week of treatment. Data are means ± SD of 6-18 rats per
group. Mean values represent the average of 72h per rat. *p<0.05 versus rats on control diet. #p<0.05 versus rats on Orlistat diet for two weeks.
CHAPTER 6
120
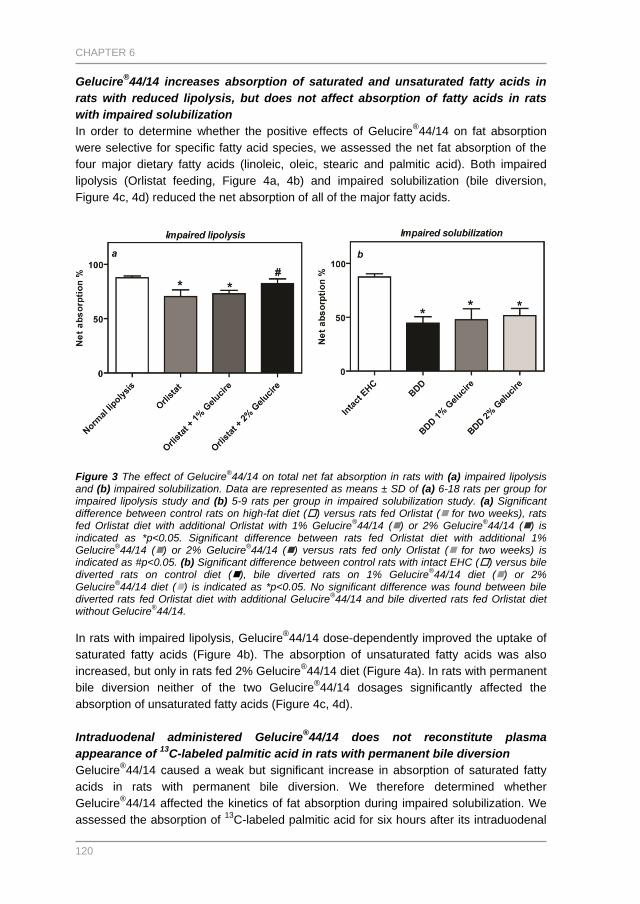
Gelucire®44/14 increases absorption of saturated and unsaturated fatty acids in
rats with reduced lipolysis, but does not affect absorption of fatty acids in rats
with impaired solubilization
In order to determine whether the positive effects of Gelucire®44/14 on fat absorption
were selective for specific fatty acid species, we assessed the net fat absorption of the
four major dietary fatty acids (linoleic, oleic, stearic and palmitic acid). Both impaired
lipolysis (Orlistat feeding, Figure 4a, 4b) and impaired solubilization (bile diversion,
Figure 4c, 4d) reduced the net absorption of all of the major fatty acids.
Figure 3 The effect of Gelucire
®44/14 on total net fat absorption in rats with (a) impaired lipolysis
and (b) impaired solubilization. Data are represented as means ± SD of (a) 6-18 rats per group for impaired lipolysis study and (b) 5-9 rats per group in impaired solubilization study. (a) Significant difference between control rats on high-fat diet () versus rats fed Orlistat ( for two weeks), rats fed Orlistat diet with additional Orlistat with 1% Gelucire
®44/14 () or 2% Gelucire
®44/14 () is
indicated as *p<0.05. Significant difference between rats fed Orlistat diet with additional 1% Gelucire
®44/14 () or 2% Gelucire
®44/14 () versus rats fed only Orlistat ( for two weeks) is
indicated as #p<0.05. (b) Significant difference between control rats with intact EHC () versus bile diverted rats on control diet (), bile diverted rats on 1% Gelucire
®44/14 diet () or 2%
Gelucire®44/14 diet () is indicated as *p<0.05. No significant difference was found between bile
diverted rats fed Orlistat diet with additional Gelucire®44/14 and bile diverted rats fed Orlistat diet
without Gelucire®44/14.
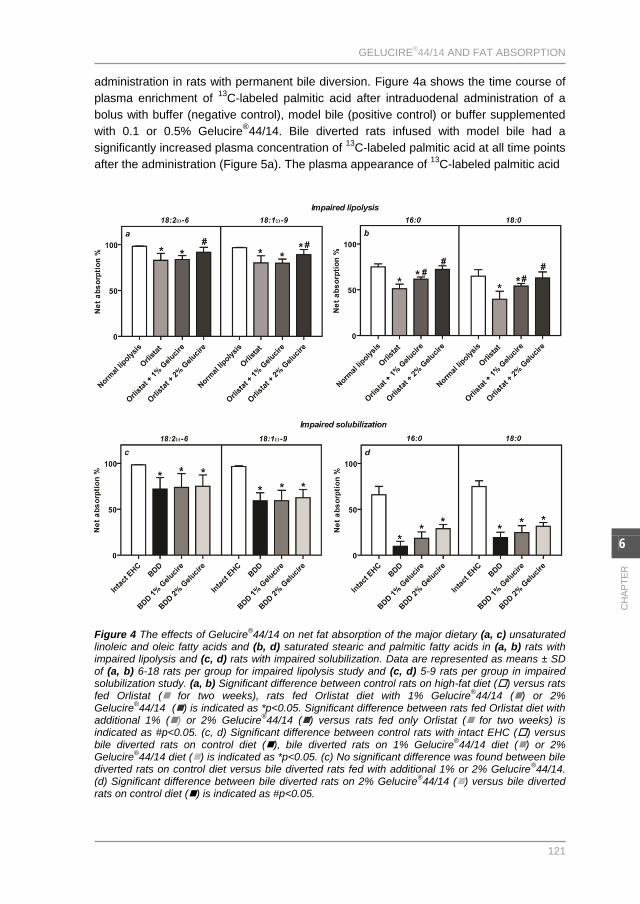
In rats with impaired lipolysis, Gelucire
®44/14 dose-dependently improved the uptake of
saturated fatty acids (Figure 4b). The absorption of unsaturated fatty acids was also
increased, but only in rats fed 2% Gelucire®44/14 diet (Figure 4a). In rats with permanent
bile diversion neither of the two Gelucire®44/14 dosages significantly affected the
absorption of unsaturated fatty acids (Figure 4c, 4d).
Intraduodenal administered Gelucire®44/14 does not reconstitute plasma
appearance of 13
C-labeled palmitic acid in rats with permanent bile diversion
Gelucire®44/14 caused a weak but significant increase in absorption of saturated fatty
acids in rats with permanent bile diversion. We therefore determined whether
Gelucire®44/14 affected the kinetics of fat absorption during impaired solubilization. We
assessed the absorption of 13
C-labeled palmitic acid for six hours after its intraduodenal
GELUCIRE®44/14 AND FAT ABSORPTION
121
6
CH
AP
TE
R
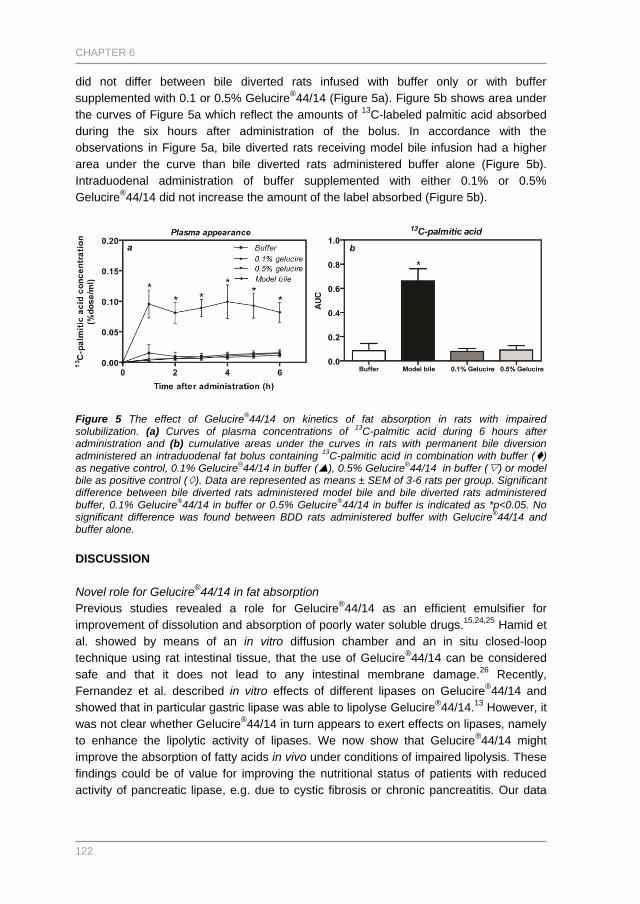
administration in rats with permanent bile diversion. Figure 4a shows the time course of
plasma enrichment of 13
C-labeled palmitic acid after intraduodenal administration of a
bolus with buffer (negative control), model bile (positive control) or buffer supplemented
with 0.1 or 0.5% Gelucire®44/14. Bile diverted rats infused with model bile had a
significantly increased plasma concentration of 13
C-labeled palmitic acid at all time points
after the administration (Figure 5a). The plasma appearance of 13
C-labeled palmitic acid
Figure 4 The effects of Gelucire
®44/14 on net fat absorption of the major dietary (a, c) unsaturated
linoleic and oleic fatty acids and (b, d) saturated stearic and palmitic fatty acids in (a, b) rats with impaired lipolysis and (c, d) rats with impaired solubilization. Data are represented as means ± SD of (a, b) 6-18 rats per group for impaired lipolysis study and (c, d) 5-9 rats per group in impaired solubilization study. (a, b) Significant difference between control rats on high-fat diet () versus rats fed Orlistat ( for two weeks), rats fed Orlistat diet with 1% Gelucire
®44/14 () or 2%
Gelucire®44/14 () is indicated as *p<0.05. Significant difference between rats fed Orlistat diet with
additional 1% () or 2% Gelucire®44/14 () versus rats fed only Orlistat ( for two weeks) is
indicated as #p<0.05. (c, d) Significant difference between control rats with intact EHC () versus bile diverted rats on control diet (), bile diverted rats on 1% Gelucire
®44/14 diet () or 2%
Gelucire®44/14 diet () is indicated as *p<0.05. (c) No significant difference was found between bile
diverted rats on control diet versus bile diverted rats fed with additional 1% or 2% Gelucire®44/14.
(d) Significant difference between bile diverted rats on 2% Gelucire®44/14 () versus bile diverted
rats on control diet () is indicated as #p<0.05.
CHAPTER 6
122
did not differ between bile diverted rats infused with buffer only or with buffer
supplemented with 0.1 or 0.5% Gelucire®44/14 (Figure 5a). Figure 5b shows area under
the curves of Figure 5a which reflect the amounts of 13
C-labeled palmitic acid absorbed
during the six hours after administration of the bolus. In accordance with the
observations in Figure 5a, bile diverted rats receiving model bile infusion had a higher
area under the curve than bile diverted rats administered buffer alone (Figure 5b).
Intraduodenal administration of buffer supplemented with either 0.1% or 0.5%
Gelucire®44/14 did not increase the amount of the label absorbed (Figure 5b).
Figure 5 The effect of Gelucire
®44/14 on kinetics of fat absorption in rats with impaired
solubilization. (a) Curves of plasma concentrations of 13
C-palmitic acid during 6 hours after administration and (b) cumulative areas under the curves in rats with permanent bile diversion administered an intraduodenal fat bolus containing
13C-palmitic acid in combination with buffer ()
as negative control, 0.1% Gelucire®44/14 in buffer (), 0.5% Gelucire
®44/14 in buffer () or model
bile as positive control (). Data are represented as means ± SEM of 3-6 rats per group. Significant difference between bile diverted rats administered model bile and bile diverted rats administered buffer, 0.1% Gelucire
®44/14 in buffer or 0.5% Gelucire
®44/14 in buffer is indicated as *p<0.05. No
significant difference was found between BDD rats administered buffer with Gelucire®44/14 and
buffer alone.
DISCUSSION
Novel role for Gelucire®44/14 in fat absorption
Previous studies revealed a role for Gelucire®44/14 as an efficient emulsifier for
improvement of dissolution and absorption of poorly water soluble drugs.15,24,25
Hamid et
al. showed by means of an in vitro diffusion chamber and an in situ closed-loop
technique using rat intestinal tissue, that the use of Gelucire®44/14 can be considered
safe and that it does not lead to any intestinal membrane damage.26
Recently,
Fernandez et al. described in vitro effects of different lipases on Gelucire®44/14 and
showed that in particular gastric lipase was able to lipolyse Gelucire®44/14.
13 However, it
was not clear whether Gelucire®44/14 in turn appears to exert effects on lipases, namely
to enhance the lipolytic activity of lipases. We now show that Gelucire®44/14 might
improve the absorption of fatty acids in vivo under conditions of impaired lipolysis. These
findings could be of value for improving the nutritional status of patients with reduced
activity of pancreatic lipase, e.g. due to cystic fibrosis or chronic pancreatitis. Our data
GELUCIRE®44/14 AND FAT ABSORPTION
123
6
CH
AP
TE
R
show that Gelucire®44/14 might act as an enhancer of lipolysis, rather than a solubilizer
under conditions of impaired fat malabsorption.
Dietary Gelucire®44/14 as enhancer of impaired lipolysis
In accordance with previous studies, our rat models of impaired lipolysis and impaired
solubilization show signs of fat malabsorption.17,18,22
Rats fed Orlistat show more
preserved fat absorption (71% after one week and 70% after two weeks of Orlistat
feeding) compared with rats with reduced solubilization (45% two weeks after the
operation). These percentages of net absorption coefficients are in agreement with
previously published data in similar rat models.17,18,27
However, rats fed Orlistat show
lower levels of inhibition of fat absorption (20% reduction) compared with human subject
who received lower amount of Orlistat (120 mg per meal; 30-40% reduction in fat
absorption).28,29,30
It appears that human subject received 0.59% of Orlistat per grams of
fat ingested, while the rats in our study received 0.89% of Orlistat per gram of fat
ingested. Present and other studies performed in rats fed Orlistat show that rats seem to
compensate the fecal fat loss by increasing their food intake during Orlistat feeding.17,19
To our knowledge human subjects fed Orlistat do not compensate for fecal fat loss by
increased food intake and, therefore, these observations might explain the discrepancy
between the effects of Orlistat fat absorption in rats and humans.
In vitro studies of Subramanian and Wasan suggested that Gelucire®44/14 might inhibit,
rather than improve, lipolytic activity.31
However, these data are not conclusive since no
significant difference was found in lipolytic activity between untreated lipases and lipases
treated with increasing concentrations of Gelucire®44/14.
31
One could have anticipated that Gelucire®44/14 would have had the largest effect on fat
absorption in bile diverted rats in which the fat malabsorption was most severely
affected. However, this would only be the case if the effects of Gelucire®44/14 could
restore (to some extent) the solubilization. Our data show that Gelucire®44/14 improves
total net fat absorption to a much larger extent in rats with impaired lipolysis; indeed, the
coefficient of fat absorption returned to almost normal values after one week of 2%
Gelucire®44/14 diet in Orlistat fed rats. In contrast, there was no effect of Gelucire
®44/14
on the solubilization of unsaturated fatty acids and only a minimal effect on the
solubilization of saturated fatty acids in rats with bile diversion. This suggests that
Gelucire®44/14 has only a slight effect on fat absorption under conditions of fat
malabsorption exclusively due to impaired solubilization.
Both rat models showed increased food ingestion of Gelucire®44/14 diets, while rats with
bile diversion also showed increased feces production upon Gelucire®44/14 feeding. The
underlying mechanism of the increased food intake by Gelucire®44/14 in these ad libitum
fed rats remains to be elucidated. We cannot exclude the possibility that difference in the
texture of the granules (which were manually made for Gelucire®44/14 diets and custom
made for the other diets) contribute to increased food ingestion in rats fed
Gelucire®44/14 diets. It has been described previously by Sako et al. that texture of food
plays an important role in food selection behavior in rats.32
Another possibility would be
that pre-digested lipolysis products (monoglycerides) directly derived from the ingested
Gelucire®44/14 might have a positive effect on food intake in these animals. The
elucidation is relevant for several reasons, including an explanation for the observed
CHAPTER 6
124
increase in net absorption of fatty acids by Gelucire®44/14. Gelucire
®44/14 may directly
enhance the activity of pancreatic lipases on fat digestion in the small intestine or retard
their degradation, for example by pancreatic proteases. However, it is unlikely that an
increase in food ingestion due to softer food pellets is the main cause of increased fat
absorption. Food intake was similarly increased during impaired lipolysis and reduced
solubilization, while the net absorption of fat was only enhanced under conditions of
impaired lipolysis and moreover was not improved in rats fed Orlistat with 1%
Gelucire®44/14. Therefore other factors must be responsible for enhanced absorption of
fat in rats with impaired lipolysis. It is possible that due to the emulsification properties of
Gelucire®44/14 an increase in the specific surface area of the fat could enable the lipase
to be more effective in vivo.
To expand our insights in the (possible) effects of Gelucire®44/14 on the kinetics of fat
absorption, we additionally measured the absorption kinetics of the saturated fatty acid
palmitate. Direct duodenal infusion of Gelucire®44/14 did not result in increased plasma
appearance of 13
C-labelled palmitate, indicating that there is no significant effect of the
compound on the kinetics of palmitate absorption. The ratio of Gelucire®44/14 to the total
amount of fat administered was equivalent to the ratio of Gelucire®44/14 to the total
amount of fat ingested in diet so that it is unlikely that the concentration of
Gelucire®44/14 infused was too low to exert an effect. The possibility remains however,
that by intraduodenal administration of the bolus, preduodenal lipolysis of Gelucire®44/14
is bypassed and that this limited its biological activity.
The exact reason for the higher specificity of Gelucire®44/14 on saturated fat compared
to unsaturated fatty acid absorption remains to be elucidated, but it seems that there
could be an effect on both solubilization and lipolysis with saturated fats but only an
effect on lipolysis for unsaturated fats. We cannot exclude, however, that some of the
absorbed palmitate and stearate in rats fed Orlistat with additional Gelucire®44/14 are
derived directly from Gelucire®44/14 itself. Fatty acids within Gelucire
®44/14 are mainly
incorporated within monoglycerides and are absorbed independently by the lipase
activity. Since absolute absorption rates of palmitic and stearic fatty acids in rats fed
Orlistat and Gelucire®44/14 exceed the amount of fatty acids that is present within
Gelucire®44/14 (data not shown), we expect that the contribution of increased fatty acid
absorption directly by fatty acids derived from Gelucire®44/14 is very low.
Future studies on the effects of Gelucire®44/14 on fat absorption
The main focus of the present study was to determine whether dietary supplementation
of Gelucire®44/14 enhances the absorption of fatty acids in vivo in relevant rat models for
different types of fat malabsorption. The underlying mechanisms might include direct
effect on lipolysis leading to increased fat absorption or indirect improvement of fat
absorption by means of enhanced emulsification properties of fat absorption. Our
findings support the concept that Gelucire®44/14 indeed enhances fat absorption in rats
in vivo. Concerning the improved absorption of saturated palmitic (C16:0) and stearic
(C18:0) acids, it would be interesting to measure the solubility of saturated and
unsaturated fatty acids in Gelucire®44/14. It is possible that saturated fatty acid have a
better solubility in a hydrogenated vegetable oil, which is the excipient in Gelucire®44/14.
Furthermore, it would be interesting to perform similar studies as presented here in a
GELUCIRE®44/14 AND FAT ABSORPTION
125
6
CH
AP
TE
R
mouse model for cystic fibrosis, where both lipolysis and solubilization are impaired and
lead to fat malabsorption. We have shown that there seems to be a dose dependent
effect of Gelucire®44/14 on fat absorption in rats with impaired lipolysis. It would be
interesting to further characterize this dose dependency using different diets and animal
models. Moreover, since unsaturated fatty acids may undergo microbial hydrogenation in
the large intestine,33
future studies would also measure absorption of fatty acids at the
level of the terminal ileum to clarify the differential effects of Gelucire®44/14 on
absorption of saturated and unsaturated fatty acids.
Overall conclusion
Dietary supplementation of Gelucire®44/14 to rats with impaired lipolytic activity corrects
the net total fat absorption. If Gelucire®44/14 would similarly improve fat absorption in
patients with impaired lipolysis, such as in CF patients or patients with chronic
pancreatitis, it could constitute a major improvement in the current therapy. However,
essential fatty acid deficiency during CF may remain prominent, even under dietary
Gelucire®44/14 supplementation, since this compound mainly improves the absorption of
saturated fatty acids. Studies in e.g. a mouse model of CF should reveal if
Gelucire®44/14 can normalize fat absorption and can be used in combination with other
compounds to improve the absorption of saturated, but also of essential fatty acids in
clinical conditions of pancreas insufficiency.
ACKNOWLEDGEMENTS
The authors would like to thank Rick Havinga for his excellent technical assistance
during the studies in bile diverted rats. Furthermore, we would like to thank Theo Boer
for his technical assistance during GC-C-IRMS measurements.
GRANTS
Part of this study was supported by an unrestricted grant of Solvay Pharmaceuticals
GmbH (Hannover, Germany) and by the Dutch Digestive Foundation.
REFERENCES
1 Carey MC, Small DM, and Bliss CM. Annu Rev Physiol 1983; 45: 651-677.
2 Bliss CM. Arch Intern Med 1981; 141(1213): 1215.
3 Quinton PM. Lancet 2008; 372(9636): 415-417.
4 Strandvik B, Einarsson K, Lindblad A, and Angelin B. J Hepatol 1996; 25(1): 43-48.
5 Roy CC, Weber AM, Morin CL, Combes JC, Nussle D, Megevand A, and Lasalle R. N Engl J Med 1977;
297(24): 1301-1305.
6 Shumaker H, Amlal H, Frizzell R, Ulrich CD, and Soleimani M. Am J Physiol 1999; 276(1 Pt 1): C16-C25.
7 Rivers JP and Hassam AG. Lancet 1975; 2(7936): 642-643.
8 Innis SM and Davidson AG. Annu Rev Nutr 2008; 28: 55-72.
9 Symonds EL, Omari TI, Webster JM, Davidson GP, and Butler RN. J Pediatr 2003; 143(6): 772-775.
10 Meyer JH, Elashoff JD, and Lake R. Dig Dis Sci 1999; 44(6): 1076-1082.
11 Kusoffsky E, Strandvik B, and Troell S. J Pediatr Gastroenterol Nutr 1983; 2(3): 434-438.
CHAPTER 6
126
12 Bronstein MN, Sokol RJ, Abman SH, Chatfield BA, Hammond KB, Hambidge KM, Stall CD, and Accurso FJ.
J Pediatr 1992; 120(4 Pt 1): 533-540.
13 Fernandez S, Rodier JD, Ritter N, Mahler B, Demarne F, Carriere F, and Jannin V. Biochim Biophys Acta
2008; 1781(8): 367-375.
14 Yuksel N, Karatas A, Ozkan Y, Savaser A, Ozkan SA, and Baykara T. Eur J Pharm Biopharm 2003; 56(3):
453-459.
15 Fernandez S, Chevrier S, Ritter N, Mahler B, Demarne F, Carriere F, and Jannin V. Pharm Res 2009; 26(8):
1901-1910.
16 Henness S and Perry CM. Drugs 2006; 66(12): 1625-1656.
17 Nishioka T, Hafkamp AM, Havinga R, vn Lierop PP, Velvis H, and Verkade HJ. J Pediatr 2003; 143(3): 327-
334.
18 Kalivianakis M, Minich DM, Havinga R, Kuipers F, Stellaard F, Vonk RJ, and Verkade HJ. Am J Clin Nutr
2000; 72(1): 174-180.
19 Hafkamp AM, Havinga R, Ostrow JD, Tiribelli C, Pascolo L, Sinaasappel M, and Verkade HJ. Pediatr Res
2006; 59(4 Pt 1): 506-512.
20 Nishioka T, Having R, Tazuma S, Stellaard F, Kuipers F, and Verkade HJ. Biochim Biophys Acta 2004;
1636(2-3): 90-98.
21 Kuipers F, Havinga R, Bosschieter H, Toorop GP, Hindriks FR, and Vonk RJ. Gastroenterology 1985; 88(2):
403-411.
22 Minich DM, Kalivianakis M, Havinga R, Van GH, Stellaard F, Vonk RJ, Kuipers F, and Verkade HJ. Biochim
Biophys Acta 1999; 1438(1): 111-119.
23 Muskiet FA, van Doormaal JJ, Martini IA, Wolthers BG, and van der Slik W. J Chromatogr 1983; 278(2):
231-244.
24 Damian F, Blaton N, Naesens L, Balzarini J, Kinget R, Augustijns P, and Van den Mooter G. Eur J Pharm
Sci 2000; 10(4): 311-322.
25 Barker SA, Yap SP, Yuen KH, McCoy CP, Murphy JR, and Craig DQ. J Control Release 2003; 91(3): 477-
488.
26 Hamid KA, Katsumi H, Sakane T, and Yamamoto A. Int J Pharm 2009; 379(1): 100-108.
27 Ferraz RR, Tiselius HG, and Heilberg IP. Kidney Int 2004; 66(2): 676-682.
28 Drent ML, Larsson I, William-Olsson T, Quaade F, Czubayko F, von BK, Strobel W, Sjostrom L, and van der
Veen EA. Int J Obes Relat Metab Disord 1995; 19(4): 221-226.
29 Davidson MH, Hauptman J, DiGirolamo M, Foreyt JP, Halsted CH, Heber D, Heimburger DC, Lucas CP,
Robbins DC, Chung J, and Heymsfield SB. JAMA 1999; 281(3): 235-242.
30 Carriere F, Renou C, Ransac S, Lopez V, De CJ, Ferrato F, De CA, Fleury A, Sanwald-Ducray P, Lengsfeld
H, Beglinger C, Hadvary P, Verger R, and Laugier R. Am J Physiol Gastrointest Liver Physiol 2001; 281(1):
G16-G28.
31 Subramanian R and Wasan KM. Drug Dev Ind Pharm 2003; 29(8): 885-890.
32 Sako N, Okamoto K, Mori T, and Yamamoto T. Behav Brain Res 2002; 133(2): 377-382.
33 Jorgensen H, Gabert VM, Hedemann MS, and Jensen SK. J Nutr 2000; 130(4): 852-857.




![University of Groningen Transcriptional response of ......homeostasis of other metal ions. In S. pneumoniae, Zn2+ and Cd2+ have been shown to cause intracellular Mn2+ deficiency [57,248].](https://static.fdocuments.us/doc/165x107/5f4db373def3875b8039ca4a/university-of-groningen-transcriptional-response-of-homeostasis-of-other.jpg)















