Unit9 cognitive lecture3(1)
57
Dementia & Alzheimer’s Disease Dementia syndrome of progressive change in cognitive function memory loss and at least one other type of cognitive deficit. Senile Dementia of the Alzheimer’s Type one cause of dementia insidious onset
-
Upload
university-of-miami -
Category
Health & Medicine
-
view
547 -
download
1
Transcript of Unit9 cognitive lecture3(1)

Dementia & Alzheimer’s Disease
Dementia syndrome of progressive change in cognitive function
memory loss and at
least one other type of cognitive deficit.
Senile Dementia of the Alzheimer’s Type
one cause of dementiainsidious onset

Cognitive Impairment
a range of disturbances in cognitive functioning. diagnosis depends on assessment of cognitive function
and a complete mental status examination
Dementia, Delirium, Depression

Cognitive Impairment Problem Areas
Attention spanConcentrationIntelligenceJudgmentLearning abilityMemory Orientation
PerceptionProblem solvingPsychomotor abilityReaction timeSocial intactness

Confusion
Non clinical term to describe acute onset of inability to understand cir cumstances without loss of consciousness.
Acute onset is over hours or days.

Normal Aging vs Dementia
Characteristics
Normal aging Alzheimer’s/Dementia
Memory loss Mild forgetfulness (able to use reminders)
Progressive memory loss (gradually unable to use reminders, eventually no ability to learn or recall information)
Thinking (cognitive impairment)
None Progressive loss in thinking skills (the ability to make decisions, to judge, to follow directions)
Paranoia, hallucinations
Some paranoia related to vision & hearing loss (may think others are talking about them)
Function of the illness although symptoms will vary among individuals. Paranoia and hallucinations are more prevalent, especially in the middle stage.
Self-care capacity Usually able to perform all self-care tasks
Progressively unable to care for themselves (eventually requires total assistance)

Dementia
Causes Reversible Irreversible

Dementia
Reversible causes nutritional deficiencies endocrine disorders trauma depression sensory deficits

Reversible Cause Normal Pressure Hydrocephalus
accumulation of cerebrospinal fluid in brain
symptoms mild dementia gait disturbance urinary incontinence
diagnosis: CT scan, ventricular enlargement
treatment: ventriculoperotonial or ventriculoatrial shunting

Irreversible Causes
Arteriosclerosis changes Multiple infarctions Alzheimer’s disease Pick’s disease Parkinson’s disease Huntington’s disease Alcohol abuse

What is Alzheimer’s Disease?
amyloid ß peptide (Aß) that accumulates in the AD brain is deposited within senile plaques and cerebral vessels
Aß accumulation initiates AD pathology

Classic triad of AD pathology
senile plaques containing Aß neurofibrillary tangles (NFTs) widespread neuronal loss in the hippocampus and
select cortical and subcortical areas

Alzheimer’s Disease
Characteristics Memory problems the first sign Language difficulties early in the
illness Attention intact for most of illness Motor and seizure disorders occur late
if at all Slowly but steadily progressive over
10-15 years

Early Warning Signs of AD
Developing memory lossLosing things, repetitive questionsSuspiciousness of othersLess activeTrouble drivingDifficulty with financesSelf-neglects —not eating, bathingIrritability, stubbornness, anxiety

Importance of Early Detection of Alzheimer’s Disease
SafetyFamily understandingEarly education of caregiverAdvanced planningPatient’s family right to knowStabilizing treatments now available

The Challenges
Patients with dementia do not recognize that they need help.
If a patient suspects he/she has a problem can go to great lengths to try and hide it.
Social skills are often preserved in early stages.

Diffuse Lewy Body Dementia
Second most common cause of dementiaName comes from the presence of abnormal lumps which
develop inside nerve cells called Lewy bodies.
Lewy Body Disease

Diffuse Lewy Body Disease Dementia
Early problems with attention, executive function, and visuospacial abilities even preceding memory impairment
Fluctuating cognitive ability (day to day changes)
Visual (93%) and auditory (50%) hallucinations are common and not always troubling to patients
Early Parkinson-like motor abnormalities and falls

Diffuse Lewy Body Disease Dementia
At risk for exaggerated Parkinsonian drug side effects from haloperidol and risperidone
psychosis with dopaminergic drugs

Vascular Dementia
Dementia related to strokesVariety of presenting signs with attention disturbances,
memory loss and changes in social behavior being common
Course is progressive, commonly with a step-wise decline being related to each new stroke
Focal neurologic signs are often presentPatients have other vascular diseases such as DM,
HTN, High Cholesterol and a history of smokingCommonly occurs with Alzheimer’s Disease (10-15%)

Frontotemporal Dementia & Pick’s Disease
Early Behavioral changes: lack of social skills, poor hygiene, sexual disinhibition, constant touching and rearranging objects, putting objects in mouthAge of onset earlier than Alzheimer’sCalculation and visuospacial skills intact until late in illnessSlow and steady progression

Parkinson’s Dementia
Dementia occurs late in the history of Parkinson’s Disease (different pattern than DLBD)
Steadily progressive

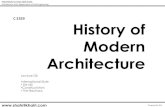
Memory Memory problemsproblems
AttentionAttention
CognitionCognitionHallucinatioHallucinationsns
Distress Distress BehaviorBehavior
MotorMotor
ProblemsProblems
AD Early Hallmark
Early Intact attention
Late or never
Late occurring
DLBD Not first symptoms
Early Fluctuating cognition
Early and Common
Parkinson-like Early
VAS Early attention problems
Common Early
PD Precedes dementia by years
Characteristics of Common DementiasCharacteristics of Common Dementias

Stages of Dementia
EarlyEarlyLoss of Recent memoryMild ConfusionMild Communication DifficultiesImpaired JudgmentPersonality and Behavior Changes (e.g., anxious,
withdrawn, depressed, irritable, mellow, sensitive, frustrated, inconsiderate)
Mild Difficulties with ADLs and advanced activities (e.g., driving, managing finances, telephoning, cooking)

The Stages of DementiaMiddleMiddle
Increased Memory Loss
Significant Confusion
Frustration
Moderate to severe communication difficulties
“When do we eat?”
anger and anxiety if unable to express needs
verbal or physical outbursts, such as yelling or throwing furniture
major word finding problems; sentences may not make sense; it may be difficult to understand others; speech may be slow

Stages of Dementia MiddleMiddle
Poor Judgment
Increased personality and behavior problems
Difficulty in completing activities of daily living
inappropriate comments to friends, questions to strangers, or an attempt to undress in a public place
restlessness, fidgeting, pacing, aimless wandering, hallucinations or delusions
bathing, toileting, grooming, dressing.

Symptoms of DementiaMiddleMiddle
loss of impulse control
agnosia
apraxia
perceptual disturbances
yells out when disturbed or strikes out when awoken
unable to recognize a fork
forgets how to use a fork
thinks the person in the mirror is someone else

Stages of DementiaLateLate
Limited memory
Extremely limited ability to perform any activities of daily living including feeding. Loss of bowel and/or bladder control
Limited communication
Increasing vulnerability and frailty
May not recognize family or friends;
May not recognize self in the mirror;
may think spouse is a stranger
Dependent on 24 hour assistance. Often no longer ambulatory.
May be mute or unable to understand words
More susceptible to infections, physical illnesses
More nutritional problems

Stages of DementiaStages of DementiaLateLate
urinary incontinence delusions
hallucinations
inability to control bladder functions
mistakenly accuses a spouse of affairs
sees people or things that are not there

Dementia Diagnostic Criteria
Characterized by multiple cognitive deficits orientation memory judgment abstract thinking problem solving
Fluctuations in moodShallowness of affective range

Dementia Diagnostic Criteria
loss of intellectual abilities-interference with functioning
at least one: impaired abstract thinking impaired judgment personality change disturbed cortical functioning

Dementia Diagnostic Criteria
disturbed cortical functioning aphasia: impaired language apraxia: impaired motor activity agnosia: failure to recognize constructional difficulty
no clouded consciousness

Diagnostic Workup
History: from patient and familyPhysical exam & vital signsMental status examNeurological examCT scan & EEGThyroid function tests

Diagnostic Workup
Serum B12 and folic acidChest Xray, ECGCBC, Urinalysis, Glucose, BUN, serum
albumin, electrolytes, VDRL

Diagnostic Work up
Rule outtreatable causes of cognitive impairmentcommon co-occuring conditions
Brain imaging studies can rule out vascular disease tumor subdural hematoma normal pressure hydrocephalus

Delirium
Diffuse disruption of cognitive statePrevalence
10-30% in the hospitalized medically ill 10-15% hospitalized elders on admission 10-40% elders while in the hospital 60% of nursing home residents over 75 experience
delirium 80% with terminal illness

Delirium
Causes drugs fever dehydration anesthesia sleep deprivation medical problems: CHF, CVA, renal failure,
anemia psychosis tumors

Delirium
Suspect delirium when Prodromal symptoms develop
Anxiety Restlessness Irritability Disorientaion Distractibility Sleep disturbance
Condition changes throughout the day Familiar figures unable to soothe

Delirium
May progress to Stupor Coma Seizures Death

Delirium Diagnostic Criteria
Disturbance of consciousness Reduced clarity of awareness of the environment Reduced ability to focus, sustain, or shift
attention

Delirium Diagnostic Criteria
At least two of the following:1. Perceptual disturbances
Misinterpretations Illusions Hallucinations-usually visual

Delirium Diagnostic Criteria
At least two of the following:1. Speech
Rambling Irrelevant Pressured Incoherent Switching from subject to subject

Delirium Diagnostic Criteria
2. Disorientation3. Short onset-hours to days

Delirium Associated Features
Sleep disturbance Daytime sleepiness Night time agitation Difficulty falling asleep Wakefulness during the night Reversal of day-night sleep cycle

Delirium Associated Features
Disturbed psychomotor behavior Restless Hyperactive Picking at bed clothes Attempting to get out of bed when it is unsafe to do so

Delirium Associated Features
Disturbed psychomotor behavior Sluggishness Lethargy

Delirium Associated Features
Emotional disturbance Anxiety Fear Depression Irritability Anger Euphoria Apathy

Delirium Associated Features
Behaviors accompanying emotional disturbance Screaming Cursing Muttering Moaning

Delirium Treatment
Manage the causative e.g. hypoxia and pain
Comfort measures to calm patient Antipsychotics for psychotic behaviorAtivan for excessive anxiety

Mini Mental State Exam
Standardized, widely used
Assesses orientation, memory and cognitive skills
Scoring 0-30 0 rating- severe
impairment 24-30 rating- normal
rangeUntreated patients
with dementia have an annual decline of 10%

Secondary Dementia
AlcoholismParkinson’s diseaseHuntington’s disease

Depression in Dementia
Harder to diagnose in the older adults especially with dementia.
May not exhibit sadness

Depression in Dementia
Harder to diagnose in the older adults especially with dementia.
May not exhibit sadness

Causes of Depression in Dementia
Psychosocial factors inability to communicate loss of function loss of pleasurable activities loss of home loss of independence loss of relationships
Biological factors

Consequences of Depression in Dementia
Accelerates decline increases memory loss causes delusions causes agitation causes giving up
Excessive disability loss of functional abilities

Clinical Cues of Depression in Dementia
irritability somatic complaints no tears ruminating critical refusing to eat low self-esteem

Supportive Therapy
One to one very helpful Conversation to reduce isolation Exercise
Group approaches can also be effectiveCombination of support and drugs most
effective for major depression

Primary Prevention
Healthy lifestyle preserves cardiovascular health and subsequently brain health