UNDRR GETI and WHO Webinar
29
UNDRR GETI and WHO Webinar Speakers: • Dr. Peter Williams, IBM Distinguished Engineer, Retd • Dr. Benjamin Ryan, Clinical Associate Professor, Baylor University, United States Commentator: • Dr. Rajib Shaw, Professor Graduate School of Media and Governance, Keio University, Japan. Resilience of local governments: A multi- sectoral approach to integrate public health and disaster risk management in partnership with 07 April 2020
Transcript of UNDRR GETI and WHO Webinar

1
UNDRR GETI and WHO Webinar
Speakers:• Dr. Peter Williams, IBM Distinguished Engineer, Retd• Dr. Benjamin Ryan, Clinical Associate Professor, Baylor University,
United States
Commentator:• Dr. Rajib Shaw, Professor Graduate School of Media and Governance, Keio University, Japan.
Resilience of local governments: A multi-sectoral approach to integrate public health and disaster risk management
in partnership with
07 April 2020

2
Resilience of Local Governments: A Multi-sectoral Approach to Integrating Public Health and Disaster Management
Tuesday April 7th, 2020
Dr Peter Williams, IBM Distinguished Engineer, Retd., USADr Benjamin Ryan, Clinical Associate Professor, Baylor University, USACommentator: Dr Rajib Shaw, Professor, Graduate School of Media and Governance, Keio University, Japan

3
Introduction and Contents
The “Public Health Addendum” is a supplement to the UNDRR’s original Disaster Resilience Scorecard for Cities , written to help address the public health implications of major disaster such as floods, earthquakes and the like.
Pandemics share depth and breadth of impact with other disasters. An instrument that deals with those impacts across all relevant city systems may therefore prove useful in formulating a more effective response to the wider issues and implications posed by Corona Virus - and other pandemics that may arise in the future.
This presentation introduces the City Scorecard very briefly to provide context for the Public Health Addendum. It then discusses the Addendum itself. It contains the following sections:
– The Disaster Resilience Scorecard for Cities – The Public Health Addendum– Using the Scorecard – Resilience Planning
4
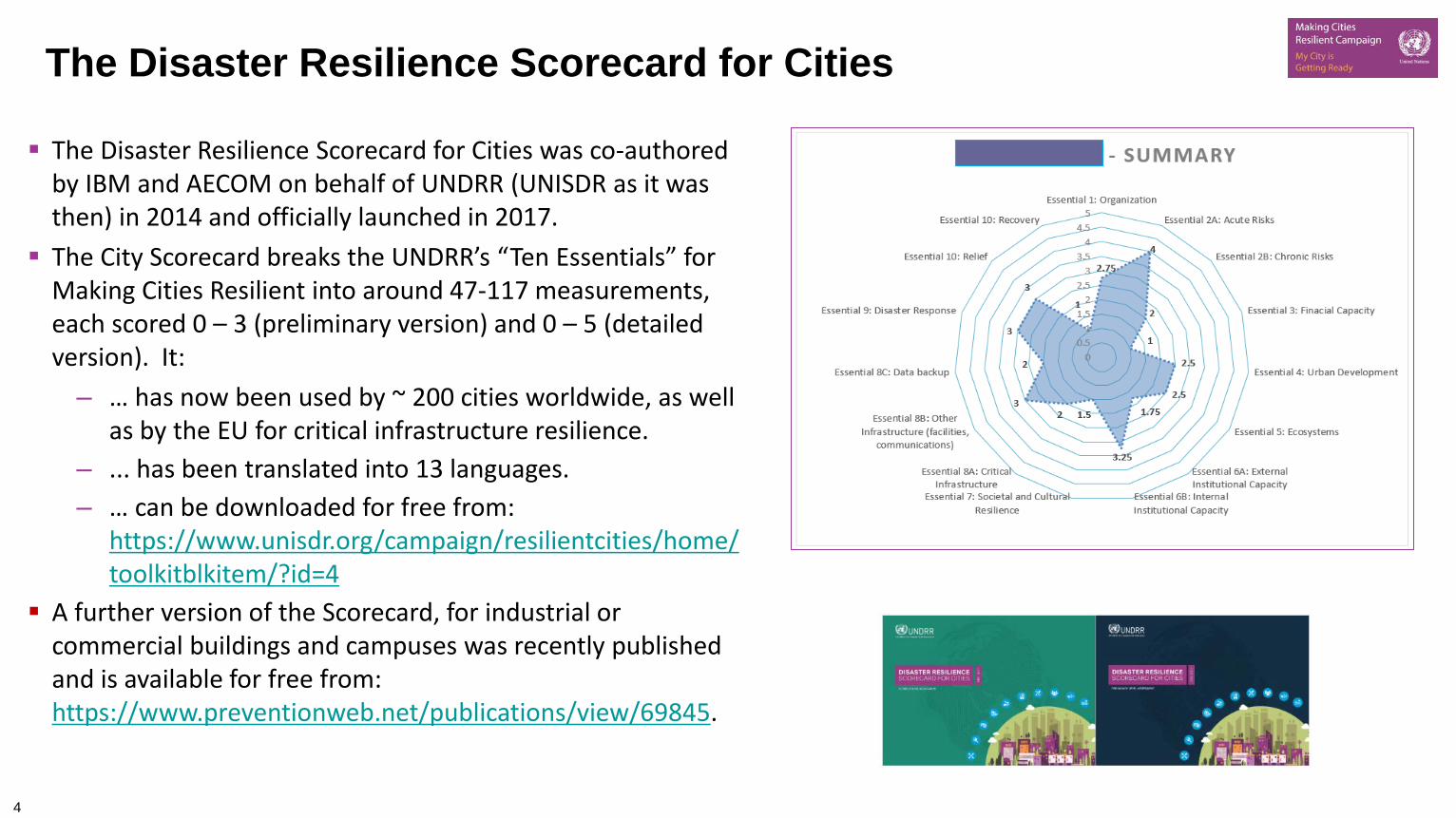
The Disaster Resilience Scorecard for Cities was co-authored by IBM and AECOM on behalf of UNDRR (UNISDR as it was then) in 2014 and officially launched in 2017. The City Scorecard breaks the UNDRR’s “Ten Essentials” for
Making Cities Resilient into around 47-117 measurements, each scored 0 – 3 (preliminary version) and 0 – 5 (detailed version). It:
– … has now been used by ~ 200 cities worldwide, as well as by the EU for critical infrastructure resilience.
– ... has been translated into 13 languages.– … can be downloaded for free from:
https://www.unisdr.org/campaign/resilientcities/home/toolkitblkitem/?id=4
A further version of the Scorecard, for industrial or commercial buildings and campuses was recently published and is available for free from: https://www.preventionweb.net/publications/view/69845.
The Disaster Resilience Scorecard for Cities

5
The Frame of Reference: Chronic and Acute Stresses
Chronic stresses Environmental Economic Social Cultural
Acute events Earthquakes Floods Storms Heat Pandemics.
(After work by Prof. Joseph Fiksel)
Interactions
May predispose to, or worsen acute eventsMay hinder recovery
May exacerbate chronic stresses

6
The UNDRR’s Original “Ten Essentials” For Making Cities Resilient
Pros:– Relatively holistic, complete coverage of the field – both by subject and by different timescales.– Allows “systems of systems” (technological, social, economic) to be addressed – great for making
connections between these. Con: public health issues don’t emerge clearly from this structure.

7
The City Scorecard – Structure. Example from Essential 1

8
Making Cities Resilient Report 2019 – Essentials 3, 7 and 10 lagging
Other trends:
• The full economic impact of a disaster is rarely understood (until you have been in one).
• “Tactically strong, strategically weak”
• Community engagement needs to include business
• Critical asset management is the “forgotten hero” (or villain!) of disaster management.
• Too much reinvention - not enough attention paid to learning from elsewhere.
• The discussion is ALWAYS as important as the score.

9
The Public Health Addendum
• Hospitals – local, regional;
• Isolation facilities;
• Residential facilities, nursing homes, assisted living facilities;
• Community health clinics, doctors’ offices, outpatient care facilities;
• EMS systems;
• Mental health facilities;
• Health laboratory and testing facilities;
• Public sector health departments.
• Water and sanitation systems;
• Food distribution systems;
• Pharmaceutical and medical supply distribution systems, drug stores;
• Environmental health systems;
• Community information, engagement and outreach processes and facilities;
• Skills, staff, assets, facilities and equipment required to function –availability post-disaster.
• Tele-medicine/tele-health systems.
• Created to address the one obvious weakness in the “Ten Essentials”.
• Uses the same “Ten Essentials” structure as the City scorecard – in the context of a pandemic, focuses on the wider issues of management and recovery
• It is NOT a medical or epidemiological tool, although these disciplines will inform answers given.
10
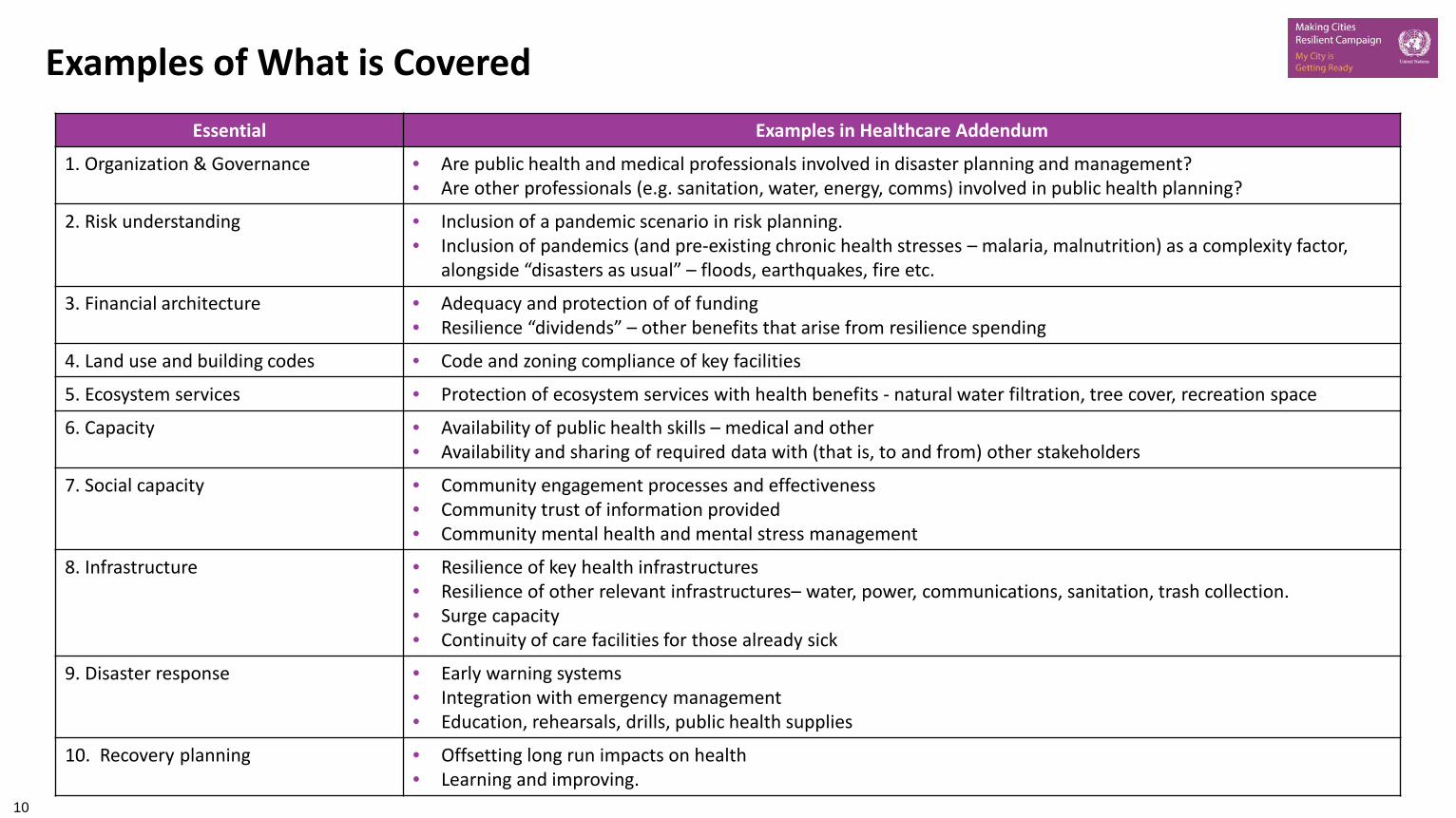
Examples of What is CoveredEssential Examples in Healthcare Addendum
1. Organization & Governance • Are public health and medical professionals involved in disaster planning and management?• Are other professionals (e.g. sanitation, water, energy, comms) involved in public health planning?
2. Risk understanding • Inclusion of a pandemic scenario in risk planning.• Inclusion of pandemics (and pre-existing chronic health stresses – malaria, malnutrition) as a complexity factor,
alongside “disasters as usual” – floods, earthquakes, fire etc.
3. Financial architecture • Adequacy and protection of of funding• Resilience “dividends” – other benefits that arise from resilience spending
4. Land use and building codes • Code and zoning compliance of key facilities
5. Ecosystem services • Protection of ecosystem services with health benefits - natural water filtration, tree cover, recreation space
6. Capacity • Availability of public health skills – medical and other• Availability and sharing of required data with (that is, to and from) other stakeholders
7. Social capacity • Community engagement processes and effectiveness• Community trust of information provided• Community mental health and mental stress management
8. Infrastructure • Resilience of key health infrastructures• Resilience of other relevant infrastructures– water, power, communications, sanitation, trash collection.• Surge capacity• Continuity of care facilities for those already sick
9. Disaster response • Early warning systems• Integration with emergency management• Education, rehearsals, drills, public health supplies
10. Recovery planning • Offsetting long run impacts on health• Learning and improving.

11
Linked – WHO Emergency and Disaster Management Risk Framework
Core principles:
Risk-based approach.
Comprehensive emergency management across prevention, preparedness, readiness, response and recovery.
All-hazards approach.
Inclusive, people- and community-centred approach.
Multisectoral and multidisciplinary collaboration.
Whole-of-health system-based.
Ethical considerations.
12
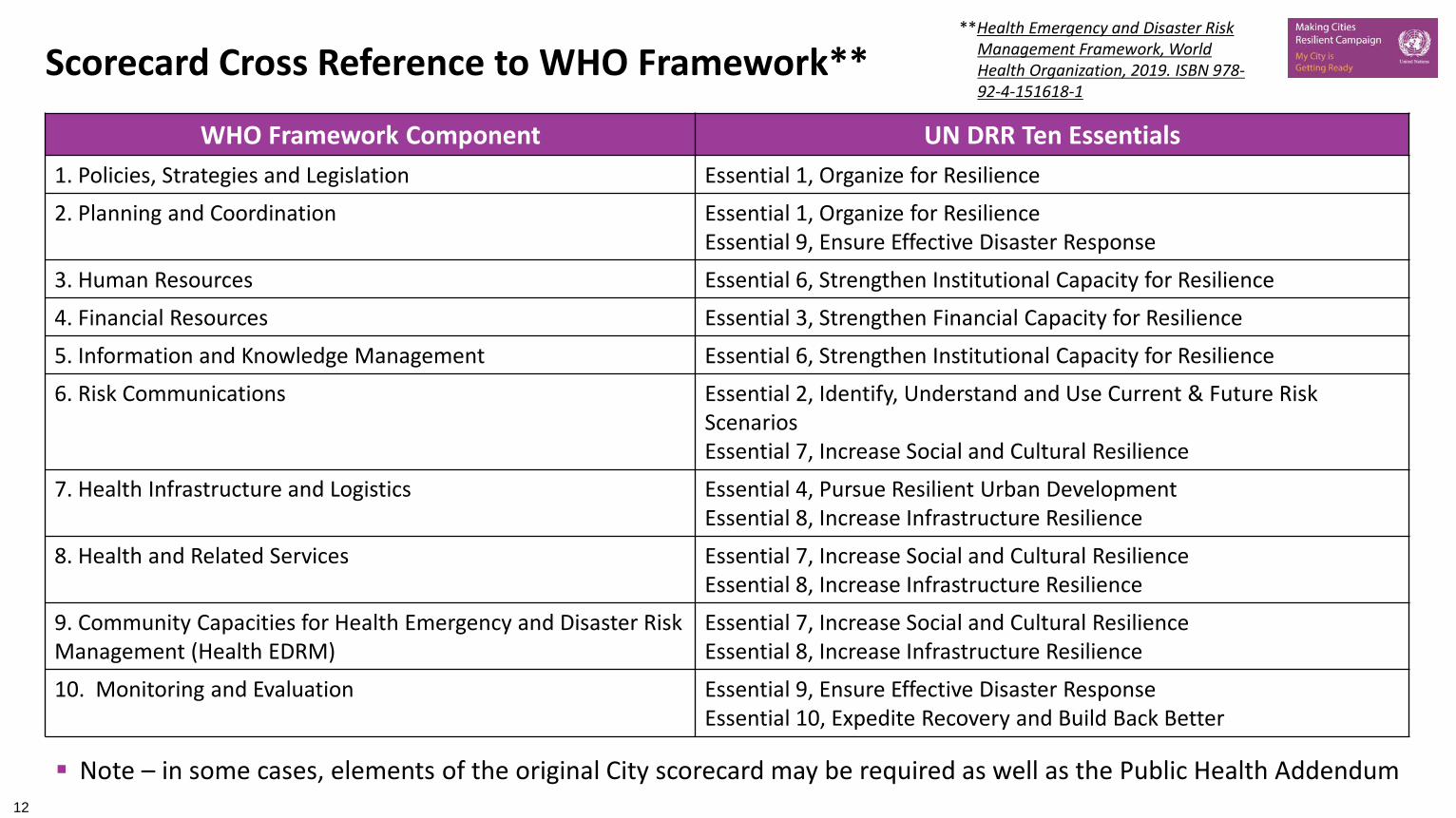
Scorecard Cross Reference to WHO Framework****Health Emergency and Disaster Risk
Management Framework, World Health Organization, 2019. ISBN 978-92-4-151618-1
WHO Framework Component UN DRR Ten Essentials1. Policies, Strategies and Legislation Essential 1, Organize for Resilience
2. Planning and Coordination Essential 1, Organize for ResilienceEssential 9, Ensure Effective Disaster Response
3. Human Resources Essential 6, Strengthen Institutional Capacity for Resilience
4. Financial Resources Essential 3, Strengthen Financial Capacity for Resilience
5. Information and Knowledge Management Essential 6, Strengthen Institutional Capacity for Resilience
6. Risk Communications Essential 2, Identify, Understand and Use Current & Future Risk ScenariosEssential 7, Increase Social and Cultural Resilience
7. Health Infrastructure and Logistics Essential 4, Pursue Resilient Urban DevelopmentEssential 8, Increase Infrastructure Resilience
8. Health and Related Services Essential 7, Increase Social and Cultural ResilienceEssential 8, Increase Infrastructure Resilience
9. Community Capacities for Health Emergency and Disaster Risk Management (Health EDRM)
Essential 7, Increase Social and Cultural ResilienceEssential 8, Increase Infrastructure Resilience
10. Monitoring and Evaluation Essential 9, Ensure Effective Disaster ResponseEssential 10, Expedite Recovery and Build Back Better
Note – in some cases, elements of the original City scorecard may be required as well as the Public Health Addendum

13
Moving towards local resilience that integrates public health and disaster risk management
Local Resilience AssessmentConduct risk assessment (inclusive of
public health risks), understand localized risks, identify vulnerabilities, assess gaps and possible actions to
respond to disaster risks
Development Strategies and Action Plans
Develop and prioritize possible interventions, identify responsible
parties & time frame, establish M&E indicators, obtain political ratification,
identify funding options
Implementation of DRR Strategies
Mobilize resources, implement actions, ensure ownership and
participation
Organizing and Preparing for Disaster Risk Reduction
Raise awareness, plan the process, convene multi- and
diverse stakeholders and relevant actors
Monitoring, Evaluation and Follow up
Monitor, evaluate and report of achievements, document
lessons learned

14
Implementation
Milestone Phases Steps
Phase one Organize and prepare to apply the public health scorecard
1. Prepare institutional setting, raise awareness2. Convene actors, formalize participatory process3. Plan and execute the process
Phase two Assess and diagnose public health system capacity
4. Become familiar with public health system capacity5. Conduct a risk assessment6. Analyze the local environment and actors7. Prepare an assessment report
Phase Three Develop an action plan 8. Define vision, objectives and main actions9. Define programmes and projects10. Institutionalize and sustain the plan
Phase Four Implementation 11. Implementation and resource mobilization12. Ensure broad participation and ownership
Phase Five Monitoring and follow-up 13. Monitor, follow up and evaluate the plan14. Disseminate and promote the plan
Modified from: The TEN Essentials for Making Cities Resilience. Available: https://www.unisdr.org/campaign/resilientcities/toolkit/article/the-ten-essentials-for-making-cities-resilient

15
What is required to complete the public health scorecard?
Public health system capacity, stakeholders, planning and procedural documentation
Public health infrastructure (see Essential 8)
Data on healthcare outcomes of previous disasters, if available
Demographic data, including for vulnerable populations
Community and professional feedback on system capacity and effectiveness.

16
Case study – Community-driven mainstreaming in the Ha’apai Islands, Tonga
Water scarcity was a persistent problem in the Ha’apai Islands, negatively affecting people’s health, crop yield and livestock productivity. Community consultations identified water supply as the top priority. Site selection, safe access to water at night for women, and accessibility of persons with disabilities and older
persons were among some of the issues. Pooling of technical and financial resources from a wide range of partners increased the purchasing power to
obtain new water tanks. Drawing upon local volunteers and engineers ensured capacity to implement and maintain the project was
kept local. As a result of this bottom-up mainstreaming initiative, the Ministry of Finance and National Planning has
started to make decisions based on the community needs and priorities.
Source: Global Assessment Report on Disaster Risk Reduction 2019
17
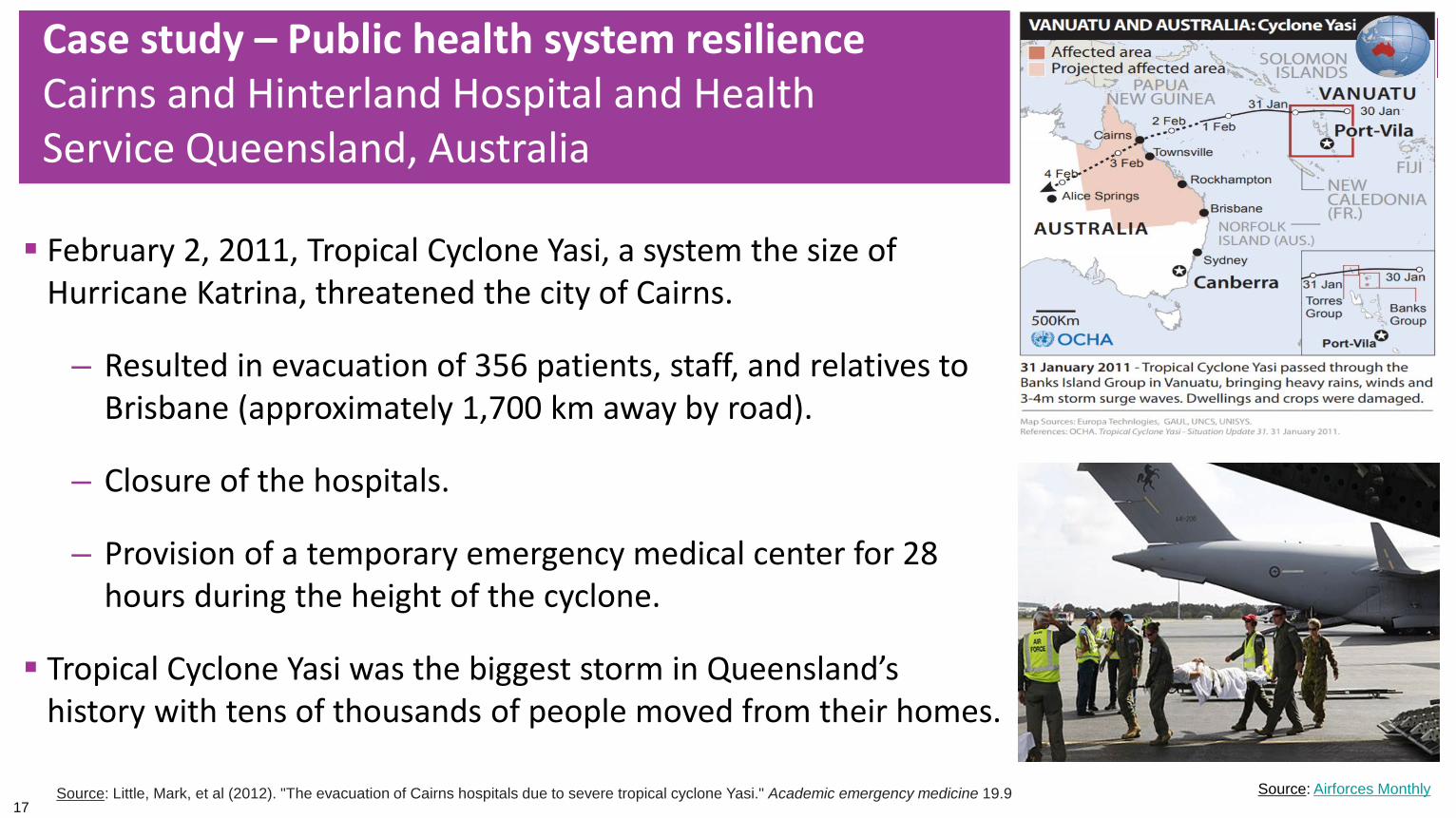
Case study – Public health system resilience Cairns and Hinterland Hospital and Health Service Queensland, Australia
February 2, 2011, Tropical Cyclone Yasi, a system the size of Hurricane Katrina, threatened the city of Cairns.
– Resulted in evacuation of 356 patients, staff, and relatives to Brisbane (approximately 1,700 km away by road).
– Closure of the hospitals.
– Provision of a temporary emergency medical center for 28 hours during the height of the cyclone.
Tropical Cyclone Yasi was the biggest storm in Queensland’s history with tens of thousands of people moved from their homes.
Source: Little, Mark, et al (2012). "The evacuation of Cairns hospitals due to severe tropical cyclone Yasi." Academic emergency medicine 19.9 Source: Airforces Monthly

18
Case study – Public health system resilience Cairns and Hinterland Hospital and Health Service Queensland, Australia Following the event, the then Premier and Minister for Reconstruction
ordered a health review. Multisectoral review of public health systems needs was undertaken. Included leaders and stakeholders from local government, health
department, emergency services, politicians and engineers. A systematic assessment of risks and capabilities identified the need for
alternative site for critical and emergency care during disaster events. Funding provided for the “Cairns South Health Facility”, which will be a
multipurpose facility:– Emergency care in a category five cyclone if the Cairns Hospital Emergency
Department is unable to function
– Site helipad to enable the evacuation of patients and casualties
– Day to day, the facility will provide community health services.
Source: https://www.health.qld.gov.au/cairns_hinterland/south
Cairns South Health Facility
Source: https://www.health.qld.gov.au/cairns_hinterland/south
Cairns Hospital
Source: Advance Cairns

19
Case study – Cox’s Bazar, Bangladesh
The displaced Rohingya people in Cox’s Bazar, Bangladesh, sheltered in makeshift settlements in extremely congested areas. Minimal access to basic infrastructure and services, and are prone to natural hazards, especially cyclones,
floods and landslides. An assessment of medium-term needs and a risk assessment identified priority investments to improve
disaster risk management, healthcare, education and emergency response. A Health Sector Support Project helped to further develop disease surveillance and outbreak response
capacities of the Ministry of Health and Family Welfare. Activities to strengthen disease outbreak response included vaccination campaigns and disease-specific
diagnosis and treatment services. There are now mechanisms for responding to the health impacts of possible disasters, such as the spread of
cholera and diarrhea as well as other water- and vector-borne diseases associated with storms and flooding.
Source: Global Assessment Report on Disaster Risk Reduction 2019
20
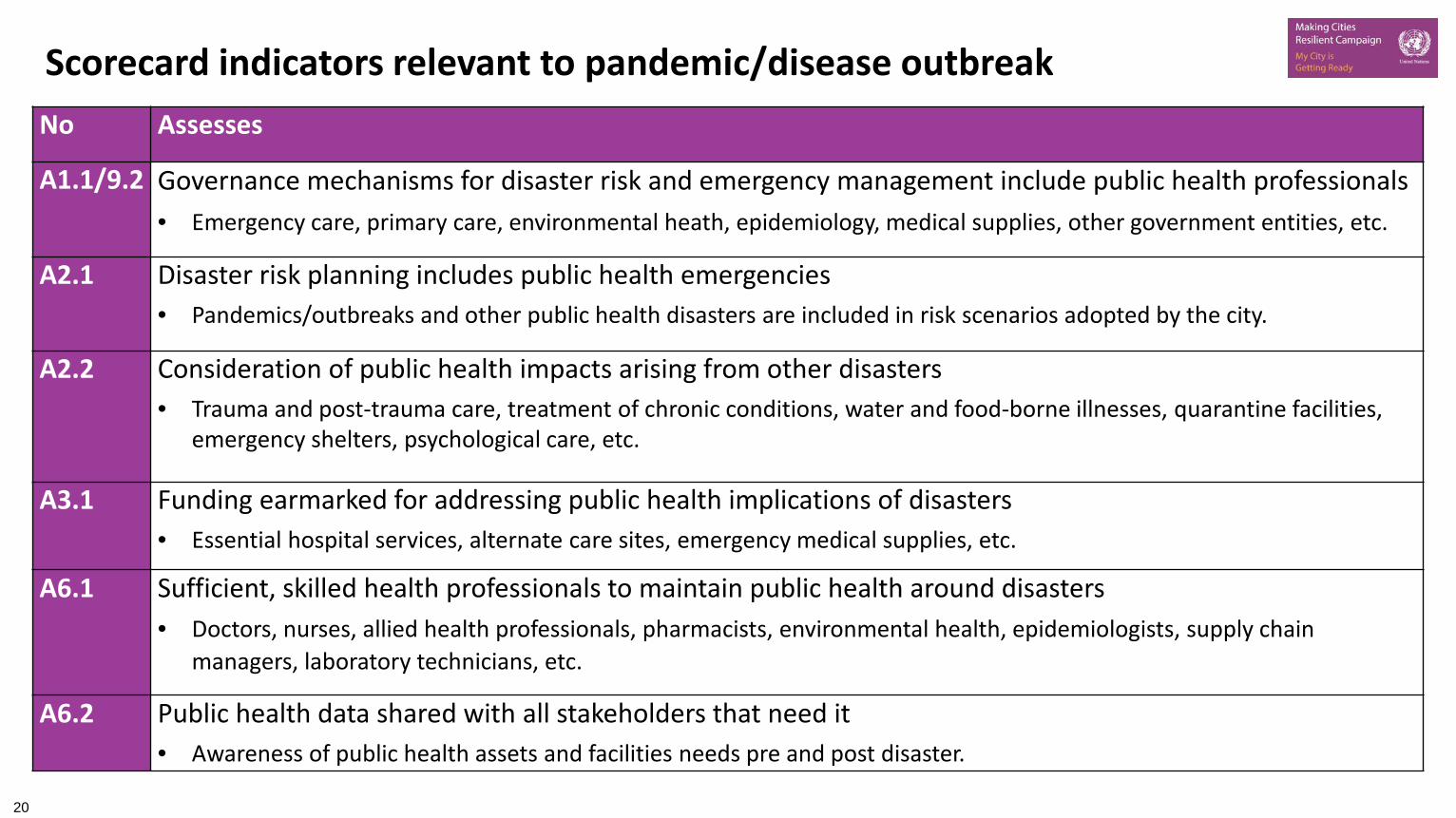
Scorecard indicators relevant to pandemic/disease outbreakNo Assesses
A1.1/9.2 Governance mechanisms for disaster risk and emergency management include public health professionals• Emergency care, primary care, environmental heath, epidemiology, medical supplies, other government entities, etc.
A2.1 Disaster risk planning includes public health emergencies• Pandemics/outbreaks and other public health disasters are included in risk scenarios adopted by the city.
A2.2 Consideration of public health impacts arising from other disasters• Trauma and post-trauma care, treatment of chronic conditions, water and food-borne illnesses, quarantine facilities,
emergency shelters, psychological care, etc.
A3.1 Funding earmarked for addressing public health implications of disasters• Essential hospital services, alternate care sites, emergency medical supplies, etc.
A6.1 Sufficient, skilled health professionals to maintain public health around disasters• Doctors, nurses, allied health professionals, pharmacists, environmental health, epidemiologists, supply chain
managers, laboratory technicians, etc.
A6.2 Public health data shared with all stakeholders that need it• Awareness of public health assets and facilities needs pre and post disaster.

21
Scorecard indicators relevant to pandemic/disease outbreak
No Assesses
A7.1 Communities are prepared to maintain public health levels after a disaster• Infectious diseases monitoring and alerts, air and water quality testing and supporting vulnerable.
A7.1.2 Community can access and trust public health information• Emergency hygiene, disease prevention, support for vulnerable and outbreak information.
A8.1 Existence of health infrastructure besides hospitals• Isolation capabilities, community clinics, nursing homes, laboratories, drugstores, supplies, etc.
A8.2 Health facilities can manage a surge of patients• Estimated loss of critical bed days, urgent medical supplies and health workforce shortages.
A9.1 Early warning systems exist for impending healthcare emergencies• City monitors health trends for the early warning of a healthcare emergency, such as a pandemic and chronic
healthcare stress that is building towards a “tipping point”.
A9.5 Supply items and equipment required to maintain public health after a disaster• PPE, first aid supplies, infection control and sanitation supplies, medications and medical equipment.

22
Multisectoral mechanism for supporting pandemic management
WHO guidance on Health Emergency and Disaster
Risk Management
Disaster Resilience Scorecard for Cities
Public health system resilience scorecard
Pandemic/disaster risk management
Making Cities Resilient Campaign

23
Moving to action
Locally led and developed Help cities establish their public health system resilience baseline
and can help to frame an action plan Cities should ideally move on to develop action plans and assign
responsibilities Further work will inevitably be needed to support project definition
and design, business case, funding, etc Work to complete the public health scorecard will be valuable for
cities participating in the Making Cities Resilience Campaign and other initiatives such as:
– 100 Resilient Cities (100RC) & Global Resilient Cities Network by the Rockefeller Foundation
– C40– UN-Habitat’s City Resilience Profiling Programme – City Resilience Program (CRP) of World Bank amongst others.
Local
District/Region
State/Province
National

24
Moving to action (cont.) – Sample Local Emergency Committee
Completion led by local emergency committee
Ether local emergency preparedness management or health department
Could be completed as part of official meetings
Completed scorecard and action plan should be submitted to state/provincial governments
Completion needs to occur while all stakeholders are present
– This maximizes engagement, understanding, awareness and time
Elected officials
Law enforcement
Fire service
Local health
Emergency medical service
Media
Community groups
Industry
Emergency management
Local Emergency Planning
Committee
Utilities

25
Moving to action (cont.)– Implementation could occur across sectors and disaster systems
Texas disaster districts Requesting assistance
Source: The State of Texas - https://www.dps.texas.gov/dem/documents/planState/state_plan.pdf
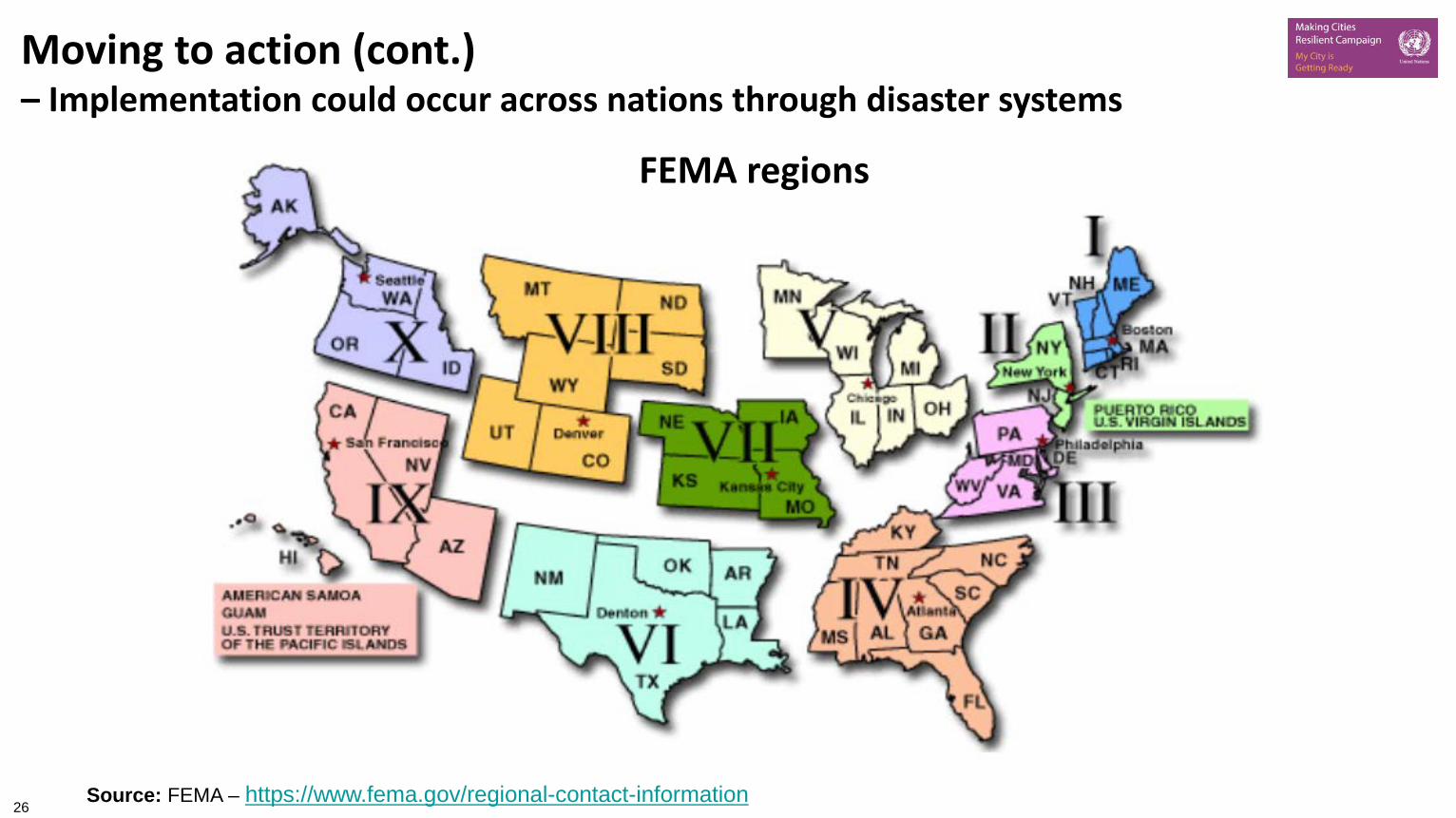
26Source: FEMA – https://www.fema.gov/regional-contact-information
FEMA regions
Moving to action (cont.)– Implementation could occur across nations through disaster systems

27
The benefits of completing extend far beyond reporting.
The conversations the process can generate may even be more important than the scores.
If completed in a collaborative way, cities can:– Establish a baseline measurement of their public health system resilience
– Increase awareness and understanding of resilience challenges
– Enable dialogue between key city stakeholders who may otherwise not collaborate regularly
– Enable discussion of priorities for investment and action, based on a shared understanding of the current situation
– Enable the development of a resilience strategy / action plan that integrates public health issues
– Ultimately lead to actions and implementable projects that deliver increased public health system and overall resilience for the city over time.
Public Health Addendum Benefits
28
Download the Public Health Addendum to the City Disaster Resilience Scorecard
https://www.unisdr.org/campaign/resilientcities/toolkit/article/public-health-system-resilience-scorecard

29
Thank you! Questions?
Dr Benjamin RyanClinical Associate ProfessorBaylor University, Texas, USA [email protected]
Dr Peter WilliamsIBM Distinguished Engineer, Retd.California, [email protected]