Understanding the Costs and Benefits of Colon Cancer Treatment Colorectal Cancer Poster Discussion...
28
Understanding the Costs and Benefits of Colon Cancer Treatment Colorectal Cancer Poster Discussion 2006 Neal J. Meropol, M.D. Director, Gastrointestinal Cancer Program Divisions of Medical Science and Population Science
-
Upload
sophie-francis -
Category
Documents
-
view
216 -
download
0
Transcript of Understanding the Costs and Benefits of Colon Cancer Treatment Colorectal Cancer Poster Discussion...
Understanding the Costs and Benefits of Colon Cancer Treatment
Colorectal Cancer Poster Discussion 2006
Neal J. Meropol, M.D.
Director, Gastrointestinal Cancer Program
Divisions of Medical Science and Population Science
Fox Chase Cancer Center
“Costs” and “Benefits”
Some Costs• Severe toxicity• Symptomatic vs.
laboratory toxicity• Hospitalization• Irreversible toxicity• Quality of life• Death• Dollars, euros, and yen
Some Benefits• Response• Progression free
survival• Relapse free survival• Overall survival• Surgical resection• Cure• Quality of life
Deriving a Treatment Valuation
V = Σ (WnpBn) - Σ (WnpCn)
Implications• There are different types of benefits• There are different types of costs• Various stakeholders evaluate costs/benefits
differently• Individual patients may weigh each cost and
benefit differently, e.g. based upon goals of therapy, decision making “calculus”
What have we learned today?
The triplet combination of irinotecan, oxaliplatin and 5FU/LV (FOLFOXIRI) vs the doublet of irinotecan and 5FU/LV
(FOLFIRI) as first-line treatment of metastatic colorectal cancer (MCRC): Results of a randomized phase III trial by the Gruppo Oncologico Nord Ovest
(G.O.N.O.)
A. Falcone, G. Masi, I. Brunetti, G. Benedetti, O. Bertetto, V. Picone, S. Chiara, M. Merlano,
S. Vitello, S. Ricci
Falcone et al: Is more better? Abstract #3513
• Randomized phase III trial• Unresectable metastatic CRC• Age 18-75• First-line therapy• FOLFIRI vs. FOLFOXIRI• N = 244• Primary endpoint = response rate
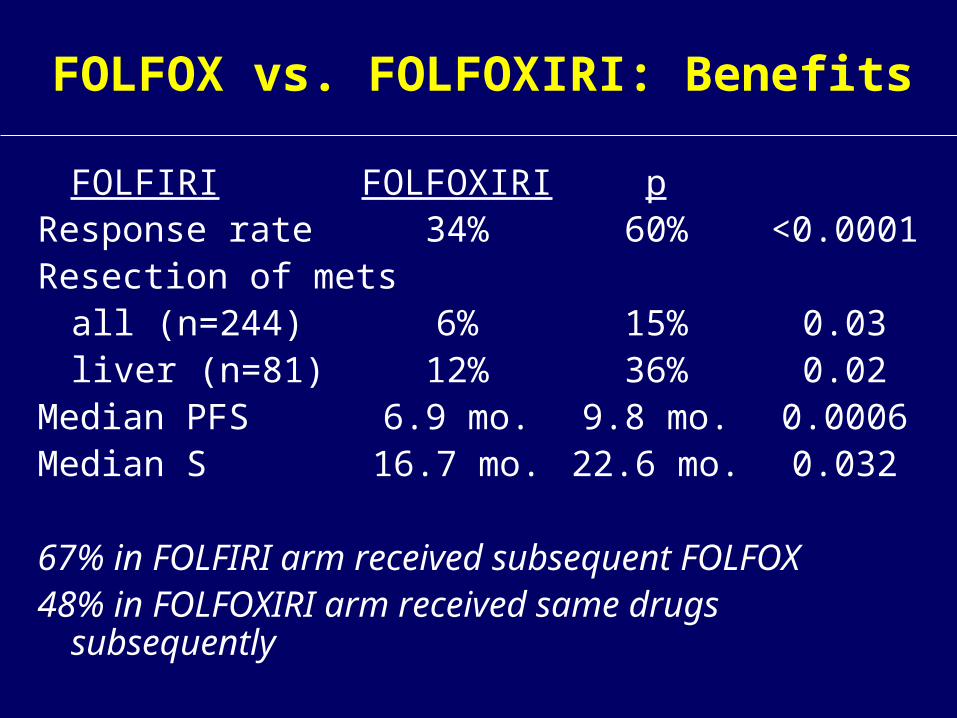
FOLFOX vs. FOLFOXIRI: Benefits
FOLFIRI FOLFOXIRI pResponse rate 34% 60%
<0.0001Resection of mets
all (n=244) 6% 15% 0.03liver (n=81) 12% 36% 0.02
Median PFS 6.9 mo. 9.8 mo. 0.0006Median S 16.7 mo. 22.6 mo. 0.032
67% in FOLFIRI arm received subsequent FOLFOX48% in FOLFOXIRI arm received same drugs
subsequently
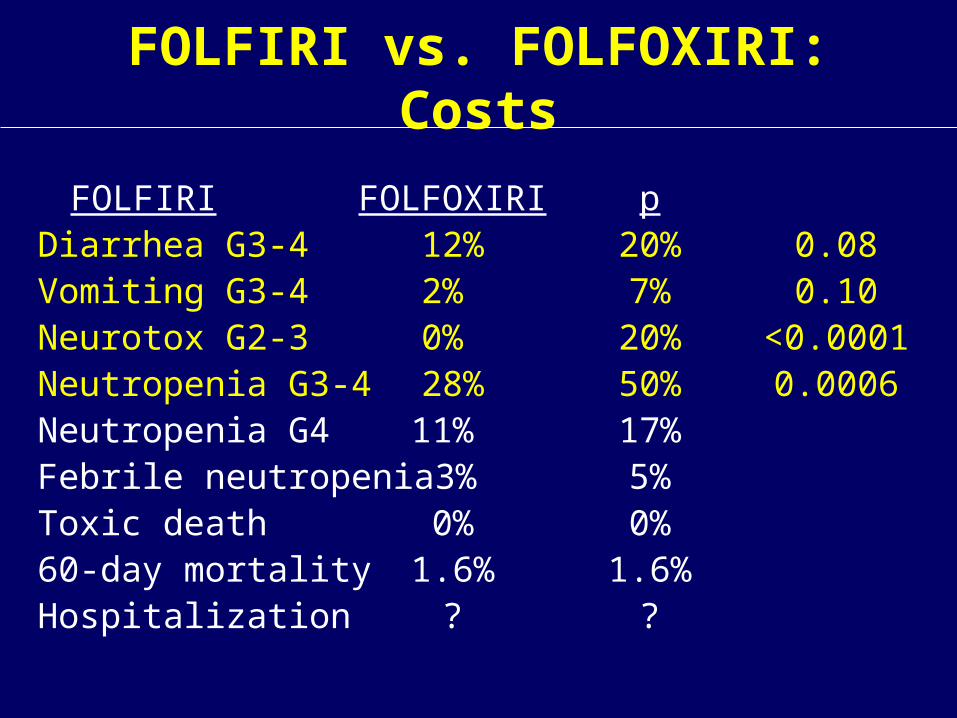
FOLFIRI vs. FOLFOXIRI: Costs
FOLFIRI FOLFOXIRI pDiarrhea G3-4 12% 20% 0.08Vomiting G3-4 2% 7% 0.10Neurotox G2-3 0% 20%
<0.0001Neutropenia G3-4 28% 50% 0.0006Neutropenia G4 11% 17%Febrile neutropenia 3% 5%Toxic death 0% 0%60-day mortality 1.6% 1.6%Hospitalization ? ?
FOLFIRI vs. FOLFOXIRI: Conclusions
• Higher response rate = higher toxicity• Note: EGFR/VEGF antibodies not routinely
available• Resection of mets may account for improvements
in long-term outcome
Identify which patients have the potential for long-term survival and CURE with aggressive surgical management. In this setting, benefits are more
likely to trump costs
Tolerability of fluoropyrimidines appears to
differ by region
D. G. Haller, J. Cassidy, S. Clarke, D. Cunningham, E. Van Cutsem, P. Hoff, M. Rothenberg, L. Saltz, H. J. Schmoll, C.
Twelves
Haller et al: Are there regional variations in fluoropyrimidine toxicity?
Abstract #3514
• Industry databases from phase III studies, international enrollment
• Metastatic– 2 studies, N=1189, capecitabine vs. daily x
5 FU/LV• Adjuvant
– 1 study, N=1861, CAPOX vs. FU/LV• Endpoints: adverse events vs. country
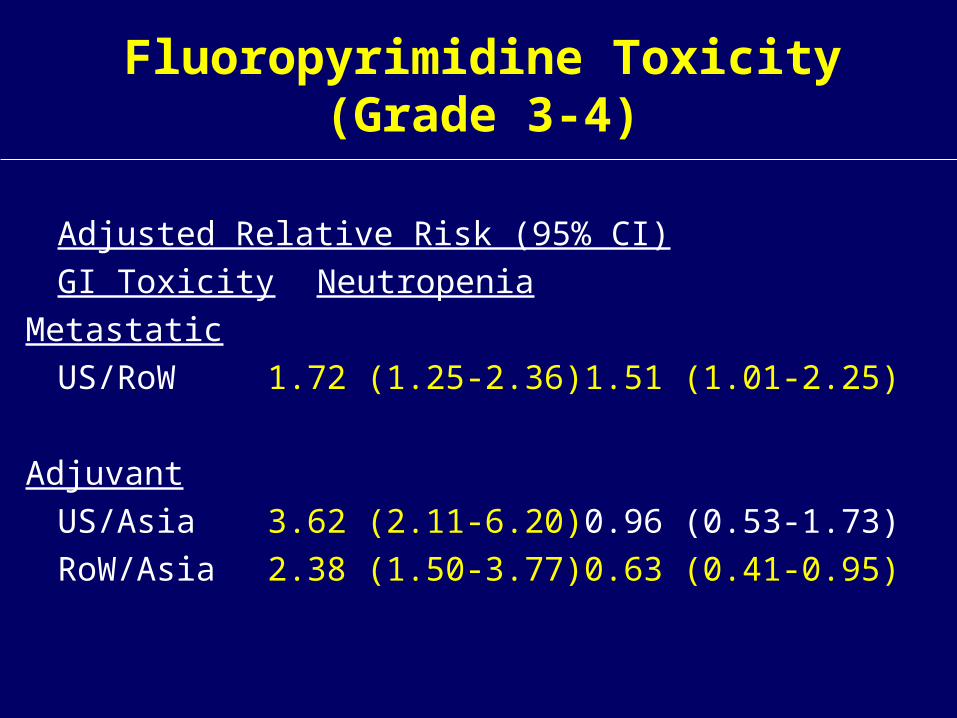
Fluoropyrimidine Toxicity (Grade 3-4)
Adjusted Relative Risk (95% CI)
GI Toxicity Neutropenia
Metastatic
US/RoW 1.72 (1.25-2.36) 1.51 (1.01-2.25)
Adjuvant
US/Asia 3.62 (2.11-6.20) 0.96 (0.53-1.73)
RoW/Asia 2.38 (1.50-3.77) 0.63 (0.41-0.95)
Potential Causes for Regional Variation in Toxicity
• Patient selection (clinical)• Reporting bias• Regional biologic differences• Regional environmental differences• Host-environment interactions• Drug interactions
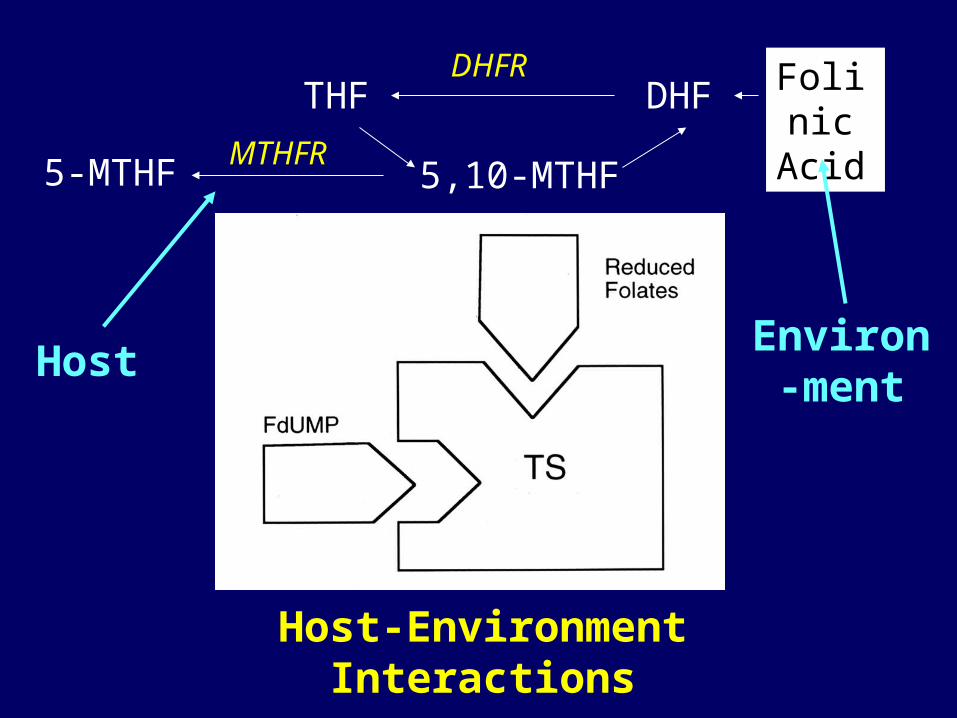
Host-Environment Interactions
DHFR
5,10-MTHF
DHFTHF
5-MTHFMTHFR
Folinic Acid
HostEnviron-
ment
Response rate using conventional criteria is a poor surrogate for
clinical benefit on progression-free (PFS) and overall survival (OS) in
metastatic colorectal cancer (mCRC): A comparative analysis of
N9741 and AVF2107
A. Grothey, E. E. Hedrick, R. D. Mass, S. Sarkar, R. K. Ramanathan, H. Hurwitz, R.
M. Goldberg, D. J. Sargent
Grothey et al: Does benefit require response?
Abstract #3516
• Retrospective analysis of AVF2107g (N=813) and N9741 (N=768)
• Response criteria: RECIST (AVF) and WHO (N9741)
• Hypothesis: Non-responders as well as responders benefit from the superior therapy
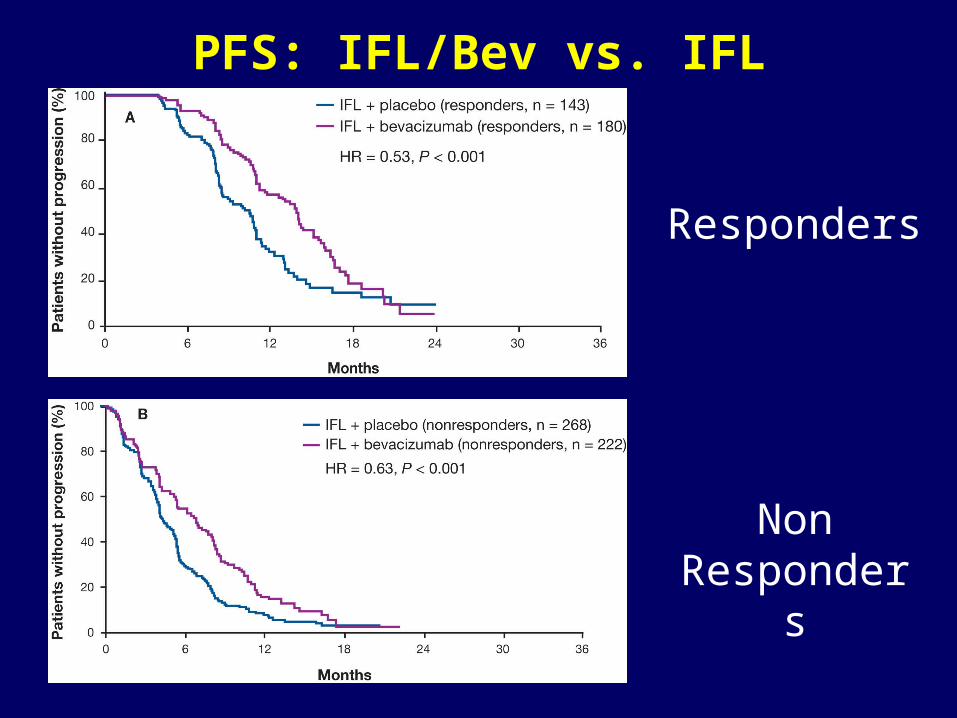
PFS: IFL/Bev vs. IFL
Responders
Non Responders
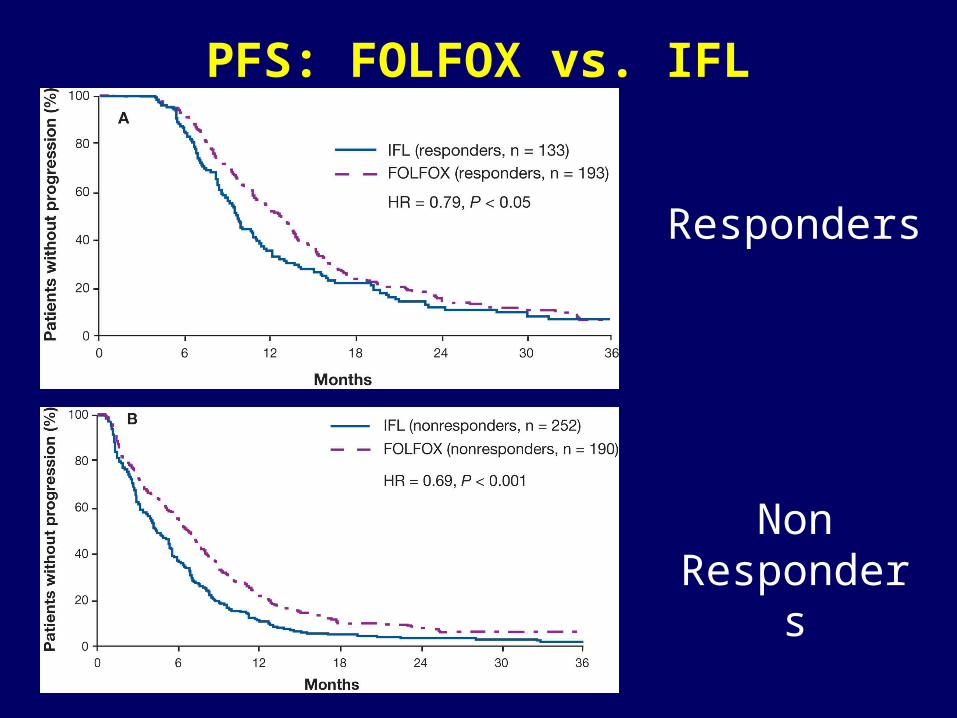
PFS: FOLFOX vs. IFL
Responders
Non Responders
Response Rate is Merely a Surrogate
• Clinical response is not a categorical variable as RECIST/WHO criteria imply
• Grothey et al analysis supports use of other endpoints in randomized trials
• Choice of surrogate should depend on clinical context, goal of study, and treatment mechanism of action (RR, non-progression rate, PFS, tumor marker, in vivo pharmacodynamics…..)
• Endpoints must be validated• Endpoints must permit discrimination of activity
from background; “go – no go” decision
A pooled safety and efficacy analysis of the FOLFOX4
regimen (bi-monthly oxaliplatin plus fluorouracil/leucovorin) in elderly compared to younger
patients with colorectal cancer
D. J. Sargent, R. M. Goldberg, H. Bleiberg, A. De Gramont, C. Tournigand, T. Andre,
M. L. Rothenberg, I. M. Tabah-Fisch
Sargent et al: Does age impact efficacy or toxicity with FOLFOX4?
Abstract #3517
• Pooled efficacy and toxicity analysis of 4 studies with FOLFOX4 (3 metastatic, 1 adjuvant)
• N=3743, 614 at least 70 years old• Analyses: age <>70 (3 studies excluded patients
>75 years old)
• Greater G3-4 neutropenia (49 vs. 43%, p=0.04), thrombocytopenia (5% vs. 2%) in older age group
• No differences in response, survival, dose intensity, neurotox, GI tox, 60 day mortality (2.3 vs. 1.1%, p=0.2)
Questions Remain…..• Other key clinical endpoints:
– What was hospitalization rate?– What was grade 4 neutropenia rate?– What was dehydration rate?
• What was the age distribution in these studies? How many patients were old old (e.g. >80)?
• How representative are these study populations of the general population?
These data highlight the importance of better characterizing key differences in clinical trial and off-
study populations, and maximizing the representativeness of clinical trial populations
Direct cost-survival analysis of therapies for metastatic
colorectal cancer
Y. Wong, N. J. Meropol, D. Sargent, R. Goldberg, J. R. Beck
Wong et al: What is the cost-effectiveness of CRC treatment?
Abstract #3515
• Markov Model comparing cost and effectiveness of up to 3 lines of treatment to base cases of 5-FU/LV or FOLFOX
• Cost = total drug costs (average sales price, 70 kg, BSA 1.7 sq.m.)
• Effectiveness = life expectancy• Aggregate data on progression, survival, and
toxicity from phase II and III published reports, and N9741 unpublished data
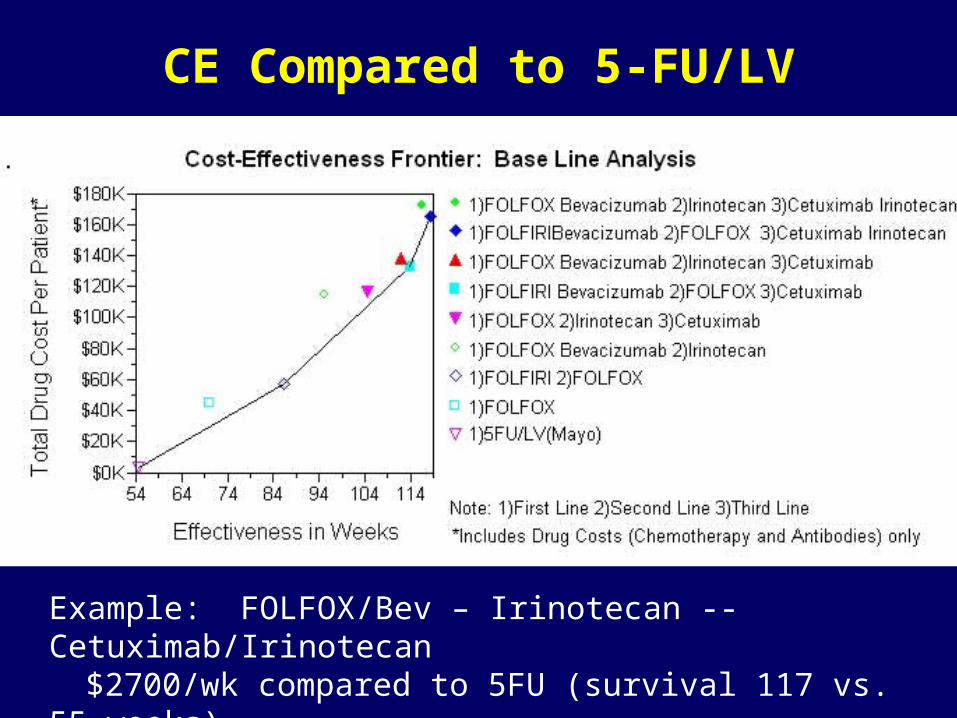
CE Compared to 5-FU/LV
Example: FOLFOX/Bev – Irinotecan -- Cetuximab/Irinotecan$2700/wk compared to 5FU (survival 117 vs. 55 weeks)
Why does this matter?
• New agents for treatment of metastatic colorectal cancer result in meaningful improvements in survival
• Cost is largely driven by drug price• These observations challenge traditional healthcare
cost-effectiveness thresholds• Cost already limits access to care• ASCO must work to ensure:
– development of new cancer therapies (innovation)
– access to high quality care for all cancer patients
– appropriate and optimal use of cancer treatments
Expanding Our Understanding of “Costs” and “Benefits”
• Goals of treatment impact valuation of costs and benefits
• Biologic and/or environmental factors may influence treatment toxicity
• Clinical benefit is not restricted to patients who achieve an objective “response”
• Among clinical trial participants <75 years old, age alone does not confer substantially greater risk of certain toxicities with FOLFOX
• Drugs are expensive. We will ultimately need to address what is an “acceptable” CE ratio, and work with all stakeholders to ensure access of high quality care for all patients