Understanding the Common Elements of Evidence-Based...
6
EVIDENCE-BASED PRACTICE Assistant Editor: John D. Hamilton, MD., M.Sc. Understanding the Common Elements of Evidence-Based Practice: Misconceptions and Clinical Examples BRUCE F. CHORPITA, PH.D., KIMBERLY D. BECKER, PH.D., AND ERIC L. DALEIDEN, PH.D. Science has fostered renewed optimism in mental health practice over the last decade through advances in the development of treatment supported by research (Kazdin and Weisz, 2003; Task Force on Promotion and Dissemination of Psychological Procedures, 1995; Wilson, 1995). The challenge that continues to confront both the scientific and applied domains of psychology and psychiatry is the widespread promotion and implementation of empirically supported treat- ments in general, and in children's mental health in particular (Barlow, 2000; Chorpita et aI., 2002; Schoenwald and Hoagwood, 2001; Weisz et al., 1995). With more than 500 documented treatments available for children and adolescents (Kazdin, 2000), how do practicing clinicians begin to identify the appropriate evidence-based interventions for their clients? On the one hand, it would appear that practitioners could consult the literature to learn more about efficacious interventions for particular problem areas. On the other hand, the increasing proliferation of guidelines, lists, and definitions that has followed has been rather complex (e.g., Chorpita et al., 2002; Lonigan et al., 1998; Schinke et al., 2002; Weisz, 2003), and in some ways has paradoxically increased the Accept.d Dec.mber 4, 2006. All of the authors are with the D.partment of Psychology, Univmity of Hawaii at Manoa, Honolulu. Preparation ofthis articl. was supported in part by awards from the Hawaii D.partments of H.alth and Education to B.P, C. Correspondence to Dr, Bruce F. Chorpita, D.partm.nt of Psychology, Univmity of Hawaii at Manoa. 2430 Campus Road, Honolulu. HI 96822; .-mail: chorpita@hawaii,.du, 0890-8567/07/4605-0647©2007 by the American Academy of Child and Adolescent Psychiatry, 001: 10,1097/chLOb013e318033f!71 j, AM. ACAD. CHILD ADOLESC, PSYCHIATRY, 46:5. MAY 2007 compleXity of identifying "best candidate" interven- tions for treating children's disorders. Contributing to the complexity of identifying evidence-based interventions is ambiguity surrounding the meaning of the term "evidence-based." Tradition- ally, albeit a recent tradition, the term has denoted specific treatment protocols with a particular degree and type of empirical support (e.g., Chambless and Hollon, 1998). Thus, the "manualization" ofinterven- tions (e.g., Coping Cat, Kendall, 1990; Defiant Children, Barkley, 1997) has lent itself to a method of defining evidence-based treatments. At this manual level of analysis, practitioners may choose from a variety of specific treatment programs that have demonstrated their efficacy in research trials. However, evidence- based, manualized treatments often have overlapping strategies, and it is difficult for practitioners to determine the relative appropriateness of one given treatment manual over another for particular clients and situations (Kazdin et aI., 1990). COMMON ELEMENTS Chorpita et al. (2005a) recently introduced a model designed to address some of these issues by employing a new level of analysis. The authors proposed a distillation and matching model (DMM) that describes how evidence-based treatment operations can be conceptualized at a lower order level of analysis than simply by their manuals. Also referred to as the "common elements" approach, this model demon- strates the feasibility of coding and identifying the specific techniques and procedures (e.g., relaxation, exposure, time out) that make up evidence-based protocols for specific problem areas, thereby producing sample aggregate profiles of these procedures. It was 647 Copyright © 2007 American Academy of Child and Adolescent Psychiatry. Unauthorized reproduction of li'I!S article is prollibited,
Transcript of Understanding the Common Elements of Evidence-Based...

EVIDENCE-BASED PRACTICE Assistant Editor: John D. Hamilton, MD., M.Sc.
Understanding the Common Elements ofEvidence-Based Practice: Misconceptions
and Clinical Examples
BRUCE F. CHORPITA, PH.D., KIMBERLY D. BECKER, PH.D., AND ERIC L. DALEIDEN, PH.D.
Science has fostered renewed optimism in mental healthpractice over the last decade through advances in thedevelopment of treatment supported by research(Kazdin and Weisz, 2003; Task Force on Promotionand Dissemination of Psychological Procedures, 1995;Wilson, 1995). The challenge that continues toconfront both the scientific and applied domains ofpsychology and psychiatry is the widespread promotionand implementation of empirically supported treatments in general, and in children's mental health inparticular (Barlow, 2000; Chorpita et aI., 2002;Schoenwald and Hoagwood, 2001; Weisz et al., 1995).
With more than 500 documented treatmentsavailable for children and adolescents (Kazdin, 2000),how do practicing clinicians begin to identify theappropriate evidence-based interventions for theirclients? On the one hand, it would appear thatpractitioners could consult the literature to learn moreabout efficacious interventions for particular problemareas. On the other hand, the increasing proliferation ofguidelines, lists, and definitions that has followed hasbeen rather complex (e.g., Chorpita et al., 2002;Lonigan et al., 1998; Schinke et al., 2002; Weisz,2003), and in some ways has paradoxically increased the
Accept.d Dec.mber 4, 2006.All of the authors are with the D.partment of Psychology, Univmity of
Hawaii at Manoa, Honolulu.Preparation ofthis articl. was supported in part by awards from the Hawaii
D.partments ofH.alth and Education to B.P, C.Correspondence to Dr, Bruce F. Chorpita, D.partm.nt of Psychology,
Univmity ofHawaii at Manoa. 2430 Campus Road, Honolulu. HI 96822;.-mail: chorpita@hawaii,.du,
0890-8567/07/4605-0647©2007 by the American Academy of Childand Adolescent Psychiatry,
001: 10,1097/chLOb013e318033f!71
j, AM. ACAD. CHILD ADOLESC, PSYCHIATRY, 46:5. MAY 2007
compleXity of identifying "best candidate" interventions for treating children's disorders.
Contributing to the complexity of identifyingevidence-based interventions is ambiguity surroundingthe meaning of the term "evidence-based." Traditionally, albeit a recent tradition, the term has denotedspecific treatment protocols with a particular degreeand type of empirical support (e.g., Chambless andHollon, 1998). Thus, the "manualization" ofinterventions (e.g., Coping Cat, Kendall, 1990; DefiantChildren, Barkley, 1997) has lent itself to a method ofdefining evidence-based treatments. At this manuallevel of analysis, practitioners may choose from a varietyof specific treatment programs that have demonstratedtheir efficacy in research trials. However, evidencebased, manualized treatments often have overlappingstrategies, and it is difficult for practitioners to
determine the relative appropriateness of one giventreatment manual over another for particular clientsand situations (Kazdin et aI., 1990).
COMMON ELEMENTS
Chorpita et al. (2005a) recently introduced a modeldesigned to address some of these issues by employing anew level of analysis. The authors proposed adistillation and matching model (DMM) that describeshow evidence-based treatment operations can beconceptualized at a lower order level of analysis thansimply by their manuals. Also referred to as the"common elements" approach, this model demonstrates the feasibility of coding and identifying thespecific techniques and procedures (e.g., relaxation,exposure, time out) that make up evidence-basedprotocols for specific problem areas, thereby producingsample aggregate profiles of these procedures. It was
647
Copyright © 2007 American Academy of Child and Adolescent Psychiatry. Unauthorized reproduction of li'I!S article is prollibited,

CHORPITA ET AL.
shown that evidence-based treatments share themajority of their techniques or "practice elements" incommon with each other (e.g., time out is used inBarkley's Defiant Children and Kazdin's ParentManagement Training manuals), thus suggesting thenotion of "distillation." That is, a large number ofevidence-based protocols can be distilled to a smallernumber of common elements.
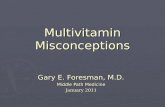
The "matching" part of the model suggests thatfollowing distillation, one can then select those practiceelements that apply to particular client characteristics asreported in the literature. For example, the practiceelements matching "depression" as a client characteristic would be an average of all elements from protocolstested successfully in clinical trials for depression. Moredetailed combinations are also possible; for example,the criteria "depression in girls between the ages of10 and 12" would yield a unique profile of practiceelements from the literature including children withthose characteristics. Figure 1 shows an example of therelative frequency of practice elements for codedevidence-based protocols for depression.
The development of this level of analysis arose to alarge extent out of attempts to promote the use ofevidence-based interventions by practitioners withinHawaii's Department of Health Child and AdolescentMental Health Division (CAMHD). Some potential
Practice Elements
Psychoeducational-ChildCognitive/CopingProblem SolvingActivity SchedulingSkill Building/Behavioral RehearsalSocial Skills TrainingCommunication SkillsMaintenance/Relapse PreventionPsychoeducational-ParentRelaxationSelf-MonitoringSelf-Reward/Self-PraiseTherapist Praise/RewardsModelingPeer Modeling/PairingFamily EngagementCrisis ManagementGuided ImageryInterpretationAssertiveness TrainingRelationship/Rapport BuildingStimulus Control/Antecedent Man.Tangible Rewards
0.00 0.25 0.50 0.75 1.00
Fig. 1 Relative frequency of practice elements from coded evidence-basedprotocols for childhood deptession. man ~ management.
648
barriers to dissemination of evidence-based interventions are listed below, and are followed by brief descriptions of how the DMM attempts to address them.
Potential Barriers to Dissemination
Manuals. Clinicians do not appear to have afavorable attitude toward treatment manuals (e.g.,Addis and Krasnow, 2000). Using the practice elementsapproach, practitioners are encouraged to incorporateelements of manualized treatments into their treatmentplan. Entire manuals can be followed if these appearrelevant or if selected component practices of thesemanuals can be assembled in the context of a particulartreatment plan.
Compatibility. New practices are more easily implemented when they are compatible with the existingorganizational infrastructure (Rogers, 1995). Largesystems rarely have the ability to support servicecontracting, outcome and fidelity monitoring systems,and billing and claims procedures that are compatiblewith more than just a few different treatment protocols.The practice elements approach encourages a standardized approach to contracting, financing, and monitoring a diverse array of services in a large system.CAMHD's example of having all services (manualizedor not) monitored for component practice elementsrelative to those in the evidence base demonstrates thefeasibility of this approach on a large scale.
Complexity. The complexity of new practices canimpede their dissemination (Rogers, 1995). Attemptsto create "evidence-based" practitioners can involvetraining them in more than a dozen different treatmentprotocols, which are not often compatible and consistent in terms of day-to-day management (e.g., variedforms and checklists, manual structures). The practiceelements approach attempts to create evidence-basedpractitioners by training them in the componentelements common to the most effective treatmentprotocols, and these components can then be implemented as needed.
Universal Application. Evidence-based treatmentprotocols are not available for all child disorders(Schiffinan et al., 2006) and hence represent a policyproblem for large systems seeking to adopt themuniversally (Chorpita et aI., 2002). The practiceelements approach is designed to encourage cliniciansto "borrow" strategies and techniques from the best
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 46:5, MAY 2007
Copyright rg 2007 American Academy of Child and Adolescent Psychiatry. Unauthorized reproduction of this article is prohibited.

known treatments, using their judgment and clinicaltheory to adapt the strategies to fit new contexts andproblems for which there is an insufficient evidencebase.
Unavailability. Many evidence-based treatment protocols are not easily obtained (Chorpita et al., 2005a).For example, in the CAMHD ongoing review ofevidence-based protocols, the vast majority (>80%) ofprotocols tested successfully in randomized trials do nothave obtainable descriptions (e.g., manuals, videos)other than what is described in the journal article itself(often no more than a paragraph). Training cliniciansin the best descriptions available and then implementing them according to the collective child treatmentliterature obviates the need for practice developmentand training programs to maintain a library ofhundreds of independent treatment protocols.
Replacement Paradigm. Training in evidence-basedtreatments often represents a "replacement paradigm"for adult learning. That is, regardless of their baselineskill level and use of evidence-based procedures,practitioners are taught to substitute (rather thancomplement) their existing clinical strategies by following a specific protocol and putting aside their existingapproach. Thus, a clinician using cognitive-behavioraltherapy who may only need to adjust the treatmentslightly or add a new technique may be expected toparticipate in the same training as someone who hasnever heard of cognitive-behavioral therapy. A practiceelements approach allows for the examination ofpotentially missing or superfluous elements in atreatment plan, and then calibrates training andsupervision only as needed.
Clinical Applications
For nearly 4 years a version of this practice elementsapproach has been in use in CAMHD. In addition toimplementing specific protocols in the tradition ofspecific manuals (e.g., Multidimensional TreatmentFoster Care, Multisystemic Therapy), CAMHD hasfully implemented monitoring of statewide childservices at the practice element level, and has developedguidelines and policy centered around coded practiceelement profiles specific to different child disorders(Daleiden and Chorpita, 2005; Daleiden et al., 2006).Other variations on this approach are being tested aspart of two independent projects examining large-scaleimplementation of evidence based practices (Integrated
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY. 46:S. MAY 2007
EVIDENCE-BASED PRACTICE
Psychotherapy Consortium, 2005a, b, c and d; and theResearch Network on Youth Mental Health, 2003).Specific clinical applications of the DMM follow.
Selecting the Best Manual jor a Population or SpecialtyClinic. Consider the situation we faced at the Center forCognitive Behavior Therapy at the University ofHawaii in selecting just one of many manuals fortreating youth with depression. DMM addresses the"crowded cell problem" by averaging across interventions that have equivalent evidence for addressing aparticular target. In our situation DMM identifiedelements such as cognitive/coping, child psychoeducation, problem solving, and activity scheduling amongthe most frequent elements used in efficacious interventions for depression. We selected Primary andSecondary Control Enhancement Training (PASCET;Weisz et al., 1999) because it represented well theaverage practice element profile for depression, therebyproviding our clinicians with a single manual that couldtreat depression across a variety of individual characteristics (e.g., age, gender, comorbid problem areas).Moreover, in our clinic PASCET could be used eitherin its entirety as specified by the authors, or, for clientswith comorbid anxiety, particular practice elementsfrom PASCET could be used in conjunction withpractice elements for anxiety (e.g., exposure) to provideindividualized treatment.
Serving a Client .for Whom No Evidence-BasedProtocol Exists. Sometimes no evidence-based protocolexists specifically for the client with certain demographics and target problems, as was the case when a7-year-old boy with depression was referred to ourclinic. DMM handles the "empty cell problem" bycollapsing across characteristics (e.g., age, gender) whensuch factors are not associated with distinct practiceprofiles in the literature. In this case DMM identifiedinterventions with the closest match to our client'scharacteristics based on outcome research for depressionacross all ages (through adolescence). Specifically, weintroduced the practice elements of child psychoeducation and relaxation that arc common in many manualsconcerning depression. However, because of the child'syoung age, we did not deliver cognitive protocols.Instead, we found that working with parents in thedelivery of rewards for successful activity scheduling wasan important treatment component. As in this illustration the practice elements approach is designed toencourage clinicians to borrow strategies and techniques
649
Copyright © 2007 American Academy of Child and Adolescent Psychiatry. Unauthorized reproduction of tnis article is prohibited.

CHORI'ITA ET AL.
from the best known treatments, using their judgmentand clinical theory to adapt the strategies to fit new contexts and problems for which there is an insufficientevidence base. In this way DMM is flexible as well asdynamic in tesponse to the evolving treatment outcomeliterature.
Training an Entire System With Limited Resources. InHawaii CAMHD serves many populations (e.g., child,adolescent) with many target problems (e.g., anxiety,disruptive behavior) in many contexts (e.g., school,outpatient, inpatient). DMM reduced trainingdemands on the CAMHD system by reducing a largenumber of manuals to a smaller number of elements,and then to an even smaller number of elements thathave the highest frequencies in evidence-based protocols. CAMHD practitioners were then trained in thepractice elements common to the most efficacioustreatment protocols, thereby providing them withtreatment strategies that they could incorporate intotheir existing clinical repertoire and apply to a variety ofclient populations.
Using Modular Delivery Based on PracticeComponents. For practitioners, DMM exemplifieshow a modular approach to treatment preserves thebenefits of manualization while allowing flexibilitybased on clinical judgment, and Project LibertyEnhanced Services is instructive in this regard. In thisproject treatment developers (Integrated PsychotherapyConsortium, 2005a, b, c and d) designed four manualsfor children 6 to 18 years old specifically based onaggregate practice elements profiles for particularproblem areas (i.e., anxiety, depression, conductproblems, and traumatic experiences). Each of thefour manuals is composed ofcore practice elements (e.g.,exposure for anxiety) and optional elements (e.g., socialskills for anxiety) that can be introduced on an individualbasis. In this way DMM can inform modular manualsthat promote practitioners' use of clinical judgment toindividualize interventions for children within thecontext of evidence-based treatment.
Misconceptions About Common Elements
Treatment approaches claiming to emanate fromscientific principles are based on many assumptions. Inthe traditional context of treatment manuals, suchassumptions have been raised and discussed in detailelsewhere (e.g., Westen et aI., 2004). The commonelements approach is no different in that regard, and it
650
is best to state these assumptions explicitly and addresspotential misconceptions.
Protocols Are Just the Sum of the Parts, andDecomtructing Them Into Specific Procedures ShouldNot Compromise Outcomes. The common elementsapproach has the potential to suggest that the otheraspects of evidence-based protocols, like sequence, pace,theory, and style, do not matter. As implemented,however (e.g., Daleiden et al., 2006), the approachmakes no assumption about the primacy of treatmentelements over other protocol features. For example,decisions about how to implement cognitive-behavioraltherapy procedures with a Socratic style at a certain paceand in a certain order are given equal considerationwithin the training model.
The Model Dictates Highly Flexible Delivery ofInterventions That Perhaps Should Not Be Flexible. Wehave suggested elsewhere (Chorpita et al., 2005a) thatthe common elements approach is not designed as asubstitute for implementation of manualized treatments. Although the model can allow for flexibility, itdoes not dictate flexibility. A practitioner may, forexample, use a practice element profile to guideselection of a particular treatment manual fromamong several choices, and then implement the manualexactly as specified. In fact, in the current implementations of this model, practitioners are typically encouraged not to mix and match elements (Chorpita et al.,2005b), unless there is highly compelling evidence tosupport such a varied treatment plan (i.e., to challengethe default approach; see for example, Meehl, 1957).
DMM Identifies "Evidence-Based" Components, theEvidence ofWhich Can Be Comidered in Isolation. It ispossible to think that because particular procedures inevidence-based approaches occur with great frequency(e.g., psychoeducation) that they may be necessary oreven sufficient for clinical change. However, noassumptions can be made about the necessity of agiven practice element in a treatment plan (claims ofthat nature represent the logical fallacy of "denying theantecedent," e.g., if A then B, therefore if not A thennot B). It has been shown, however, that most practiceelements are not necessary-there being almost noinstances in which 100% of successful approaches for agiven problem have a single element in common-andthere are just a few demonstrations of practice elementsufficiency in the literature (e.g., exposure for phobias,relaxation for depression).
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY. 46:5, MAY 2007
Copyright «j) 2007 American Academy of Child and Adolescent Psychiatry. Unauthorized reproduction of this article is prohibited.

The Model Identifies What Works for Whom UnderWhich Conditions. Although the matching feature ofthe model allows for users to select the literature thatmost pertains to the child or contextual features at hand(e.g., 10-year-old child, outpatient clinic), the literaturedoes not organize itself in such a way as to answer suchquestions. Rather, the model only allows for theidentification of studies matching those characteristics.The literature does not systematically apply all protocolsto all child characteristics and contexts; thus, theobservation that treatment X works for African American boys with posttraumatic stress disorder may just becoincidence. Other treatments that have not been testedmay also work in that context, and likewise, treatment Xmay work for other children in other contexts. Thus, themodel only yields a "best guess" from the collectivechild treatment literature at any given time.
The Model Shows Us Definitively for Whom thePractices Have Worked. The quality of the inference inthe title is also limited by the literature. For example, aprofile of recommended practice elements for 3-yearolds with disruptive behavior draws from all studies thatsuccessfully treated samples including 3-year-olds withthat target problem. However, just because a successfulstudy included 3-year-olds in the sample does not meanthat it was the 3-year-olds who got better. Perhaps itwas the other children in the sample who got better,thereby bringing up the group average. When suchinteractions are detected and reported in the literature,they can be incorporated into the model. More oftenthat not, however, the vast majority of potentialmoderators cannot and have not been examined inthe child treatment literature (Kazdin, 2005).
In essence, then, what the common elementsapproach really attempts to do is to guide clinicaldecision making by providing a dynamic snapshot ofthe entire treatment literature at a given point in time,and by encouraging a new level of analysis for treatmentmonitoring and implementation that can potentiallyincrease compatibility and utility in certain contexts.This is intended to translate into improved decisionmaking both in selecting and implementing treatments.
CONCLUSIONS
Through the identification of common practiceelements across evidence-based manuals and thesubsequent development of practice element profiles
]. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 46:5, MAY 2007
EVIDENCE-BASED PRACTICE
based on client characteristics, the DMM (Chorpitaet al., 2005a) provides a means by which practicingclinicians can identify evidence-based treatments. TheDMM addresses many potential barriers to dissemination that have hindered the widespread use ofevidencebased treatments by practitioners by encouraging theindividualization of treatments based on the strengthsand needs of the client. At the same time, the DMMdoes not advocate a deconstructionist approach tomanuals, whereby clinicians can provide treatment in apiecemeal fashion; rather, to the extent that thetreatment outcome literature allows, DMM is intendedto provide initial guidance to practitioners who want toknow what works for whom and under whichconditions.
Disclosur~: Dr. Chorpita is president ofPracticeWise, LLC, a privatebehavioral h~alth consulting corporation. Dr. Becker is a consultant toPractis~Wis~, LLe. Dr. Daleiden is 'I consultant to Practis~Wise, LLCand Real Time Engines, LLe.
REFERENCES
Addis ME. Krasnow AD (2000), A national survey of praCtlcmgpsychologists' attitudes toward psychorherapy rreatment manuals.J Consult Gin Psychol 68:331-339
Barkley RA (J 997), Difiant Children: A Clinician's Manual for ASJeJsmwland Parent Training. 2nd ed. New York: Guilford
Barlow DH (2000). Evidence based practice: a world view. Gin Psychol SciPractice 7:241-242
Chambless DL. Hollon SO (1998). Defining empirically supportedtherapies. J Consult Gin PsychoI66:7-18
Chorpita BF, Daleiden E. Weisz lR (2005a), IdentifYing and selecting thecommon elements of evidence based interventions: a distillation andmatching model. Mwt Heallh Sm' Res 7:5-20
Chorpita BF, Daleiden E. Weisz lR (2005b), Modularity in the design andapplication of therapeutic interventions. Appl Prev Psycholll:141-156
Chorpita BF. Yim LM. Donkervoet lC et al. (2002). Toward a large-scaleimplementation of empirically supported treatments for children: areview and observations by the Hawaii empirical basis to services taskforce. Gin Psychol Sci Pract 9: 165-230
Daleiden EL. Chorpita BF (2005). From data to wisdom: qualityimprovement strategies supporting largc~scale implementation ofevidence-based services. Child Adolesl' Psychiatr Clin North Am14:329-349
Daleiden EL. Chorpita BF. Donkervoet C, Arensdorf AM, Brogan M(2006). Getting better", getti ng them bener: health outcomes andevidence-based practice within a sysrem of care. JAm Acad Child AdolescPsychiatry 45:749-756
Integrated Psychotherapy Consortium (2005a). Project Liberty EnhancedServices Program: Anxiety Sympwms InleT/'ention Manual. New York:State Office of Mental Healrh
Integrated Psychotherapy Consortium (2005b), Project Liberty EnhancedStrvices Program: Posl-traumatic Sims Symptoms Intervenlion Manual.New York: State Office of Mental Health
Integrated Psychotherapy Consortium (2005c). Project Liberty EnhancedServices Program: Depression Symptoms InteT/'enlion Manual. New York:Stare Office of Mental Healrh
Inregrated Psychotherapy Consortium (7.005d). Project Liberty Enhanced
651
Copyright © 2007 American Academy of Child and Adolescent Psychiatry. Unauthorized reproduction of this article is prohibited.

CHORI.ITA ET AL.
Servicn Program: DiJruptive 8<hllvior Symptomr 1nt"v"'tion Manual.New Ymk: Sate Office of Mental Health
Kazdin AE (2000), Prychoth"apy for Children and Ar.bJlnunlJ: Di"ctionr forReuarch and Practiu. New York: Oxford University Press
Kazdin AE (2005), Parent Management !"rllining: TrMrmen,for Opporitiona~
Aggrmive, and AntiJocia! 8<hllvior in Children and Adolncentr. NewYork: Oxford University Press
Kazdin AE, Weisz JR (2003). Context and background of evidence-basedpsychotherapies for children and adolescents. In: Evidenu-baudPrychoth"apin For Children and Adolncentr (~20). Kazdin AE, WeiszJR, cds. New York: Guilford
Kazdin AE, Bass D. Ayers WA, Rodger< A (1990), Empirical and clinicalfocus of child and adolescent psychorherapy research. J Consult ClinPrychoI58:729-740
Kendall PC (1990), The Coping Cllt Workbook. Ardmore, PA: WorkbookPublishing
Lonigan CJ. Elbert JC, Johnson SB (1998), Empirically suppottedpsychosocial intervenrions for children: an overview.] elin Child Prychol27:138-145
Meehl PE (1957), When shall we usc our heads instead of rhe fotmula?J Counreling PrychoI4:268-273
Research Nerwork on Youth Menral Healrh (2003). Linlting Scienu andPractiu to 1mprove Youth Mentllllle"'th CIl": 11. Evidence-bared Practiuin Clinier and Syrumr. Research proposal submitted to the John D. andCatherine T. MacArthur Found"rion
Rogers EM (1995), Diffusion of1m/ol'll/ionr, 4th cd. New York: The FreePress
Schiffman J, Becker KD, Daleiden EI. (7.006), Evidence-based services in a
sratewide public mental healrh sysrem: do rhe services fir rhe problems?J elin Child Adolerc PrychoI35:B-19
Schinke S, Brounstein P, Gardner S (2002). Scienu-bared P"ventionProgram! and Principur (DHHS No. SMA 03-3764). Rockville, MD:Center for Subsrance Abuse Prevenrion, Subsrance Abuse and MentalHealrh
Schoenwald SK, Hoagwood K (2001), Effectiveness, transportability. anddisseminarion of inrerventions: Whar matters when? Prychiatr Serv52:1190-1197
Task Force on Promotion and Dissemination of Psychological Procedures(1995), Training in and dissemination of empirically validaredrreatments: repon and recommendations. elin Prychologirt 48:3--23
Weisz JR. Donenberg GR. Han SS. Weiss B (1995), Bridging rhe gapbetween laborarory and clinic in child and adolescent psychotherapy.J Comult Clin PrychoI63:688-701
Weisz JR. Moore PS. Southam-Gerow M, Weersing YR, Yaleri SM,McCarty CA (1999). Th"apiJt' r Manual: Primary and Secondary ControlEnhanum",t Training Program. Available ar: [email protected]
Weisz JR (2003), Prychotherapy for Children and Adolerccntr: Evidenu-baredTrcarm",/S and Care Exampln. Cambridge, UK: Cambridge UniversityPress
Wesren 0, Novotny CM. Thompson-Brenner H (2004), The empiricalstatus of empirically supported psychotherapies: assumprions, findings,and reporting in conrrolled clinical rrials. Psychol Bull 130:631-663
Wilson GT (1995). Empirically validated rrcatmenrs as a basis for clinicalpractice: problems and prospecrs. In: Scientific Standard! ofPrychoiogicalPractice: fssun and Recomm",dationr (I6~/96), Hayes, SC. Follene,YM, Dawes, RM. Grady. KE cds. Reno. NY: Context Press
Unwanted and Wanted Exposure to Online Pornography in a National Sample of Youth Internet Users Janis Wolak, JD.Kimberly Mitchell, PhD, David Finkelhor, PhD
Objective: The goal was to assess thc extent of unwanted and wanted exposure to online pornography among youth Internet users andassociated risk factors. Metbod!: A telephone survey of a nationally representative sample of 1500 youth Interner users aged 10 to 17yeats was conducred between March and June 2005. Reru/tr: Forty-two percent ofyouth Internet users had been exposed to onlinepornography in the past year. Of those, 66% reported only unwanted exposure. Multinomial logistic regression analysis was used tocompare youth with unwalllcd exposure only or any wanted exposure with those with no exposure. Unwanted exposure was relatedto only 1 Internet acrivily, namely, using file-sharing programs to download images. Filtering and blocking software reduced therisk of unwanted exposure, as did attending an Internet safety presentation by law enforcement personnel. Unwanted exposurerates were highet for reens, youth who reponed being harassed or sexually solicited online or interpersonally victimized ominc, andyouth who scored in the borderline or clinically significant tange on the Child Behavior Checklist subscale for depression. Wantedexposure rates were higher for teens, boys, and youth who used file-sharing programs to download images, talked online tounknown persons about sex, used the Internet at friends' homes, or scored in the borderline or clinically significan t range on theChild Behavior Checklist .,ubsca!e for rule-breaking. Depression also could be a risk factor for some youth. Youth who usedfilrering and blocking software had lower odds of wanted exposure. Conclurion!: More research concerning the potential impact ofInternet pornography on youth is warranted, given the high rate of exposure. the fact that much exposure is unwanted, and the factthat youth with cenain vulnerabilities, such as depression, interpetsonal victimization, and delinquent tendencies. have moreexposure. Pediauics 2007; 119:247-257.
652 ]. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 46:5. MAY 2007
Copyright © 2007 American Acadr:lmy of Child and Adolescent Psychiatry. Unauthorized reproduction of this article is prohibited.