UNDERSTANDING THE BASICS OF PRIMARY HYPEROXALURIA
48
UNDERSTANDING THE BASICS OF PRIMARY HYPEROXALURIA Dr.Nageswara Reddy.Pamidi, M.D, D.M(Nephro) Consultant Nephrologist, PREETI Kidney Hospital, Hyderabad Mayo Clinic Hyperoxaluria Center
Transcript of UNDERSTANDING THE BASICS OF PRIMARY HYPEROXALURIA
UNDERSTANDING THE BASICS OF PRIMARY HYPEROXALURIA
Dr.Nageswara Reddy.Pamidi, M.D, D.M(Nephro)
Consultant Nephrologist, PREETI Kidney Hospital, Hyderabad
Mayo Clinic Hyperoxaluria Center
1. Inherited Causes of pediatric stone disease 1.Adenine phosphoribosyltransferase(APRT) deficiency 2.Cystinuria 3.Dent disease 4.Familial hypomagnesemia with hypercalciuria and nephrocalcinosis (FHHNC), 5.Primary hyperoxaluria (PH)
CP1167399-5
- O
C
O
C
O O -
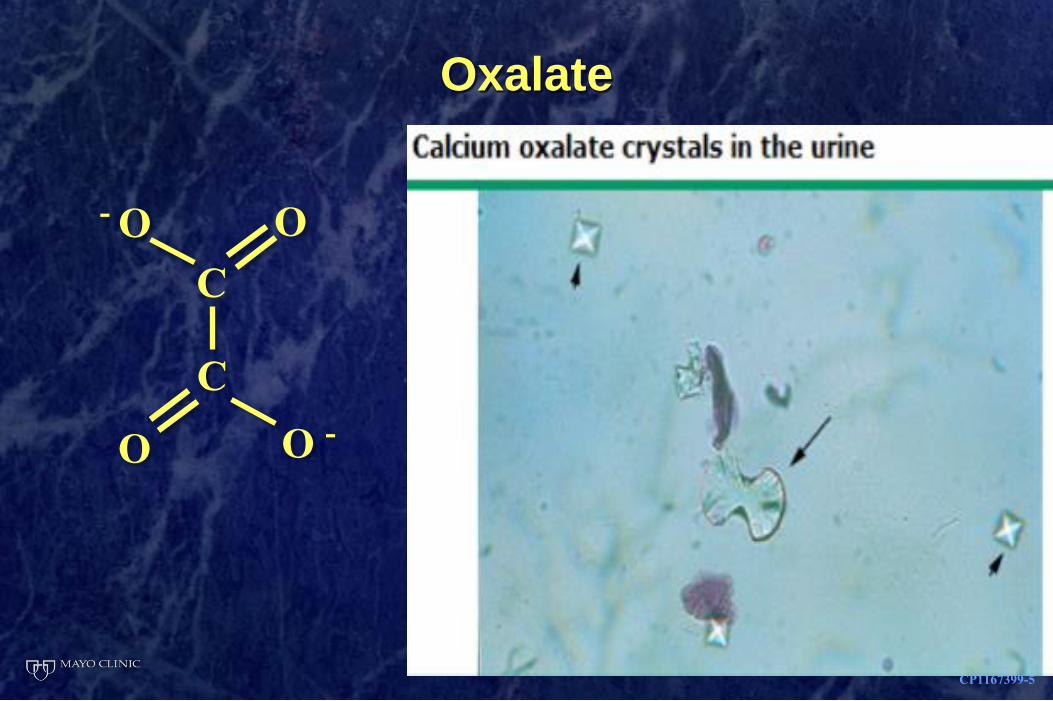
Oxalate
What is oxalate?
• A naturally occurring substance found in plants and animals
• Two sources of oxalate in humans:
• Made in liver during metabolism
• Dietary intake
• Not needed for any human body process
• Majority excreted by healthy kidneys into the urine
CP1167399-1
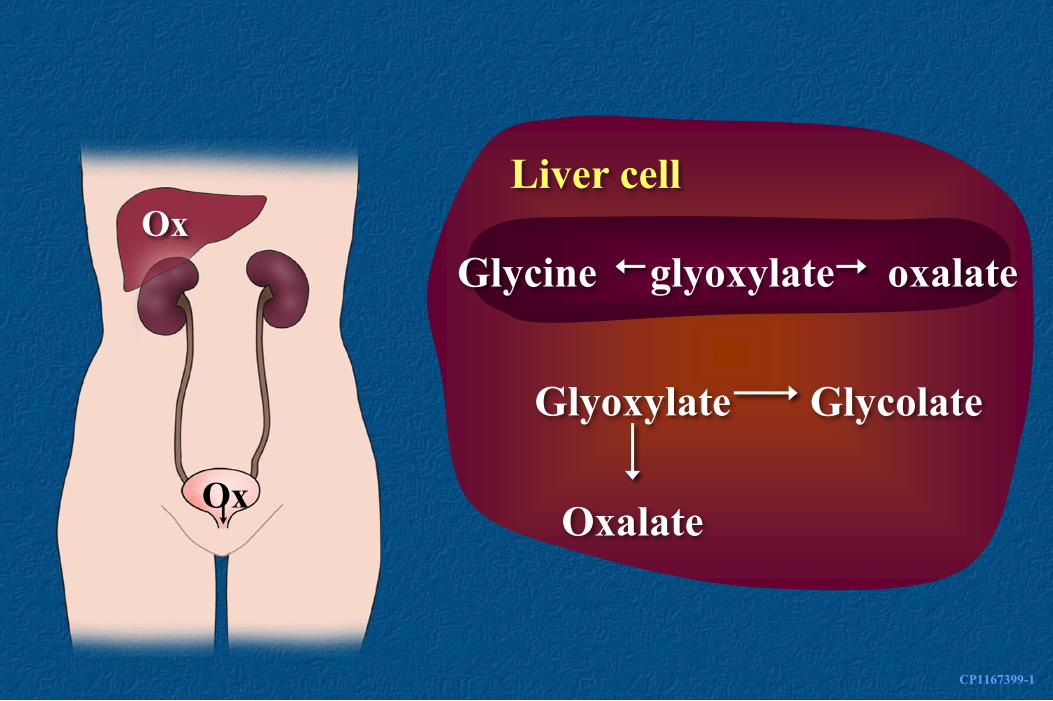
Ox
Ox
Glycine glyoxylate oxalate
Liver cell
Glyoxylate
Oxalate
Glycolate
What is primary hyperoxaluria?
Hyper - oxal - uria
(too much) (oxalate) (in the urine)
Primary (comes from within)
Hyper - oxal - uria (too much) (oxalate) (in the urine)
Primary hyperoxaluria
• A condition in which the liver makes too much oxalate
• Genetic mutations result in defective enzymes
• Three types of primary hyperoxaluria based on which enzyme is defective
Primary hyperoxaluria
• Increased oxalate excreted in the urine
• Oxalate combines with urine calcium forming a salt
• Calcium oxalate damages the kidneys
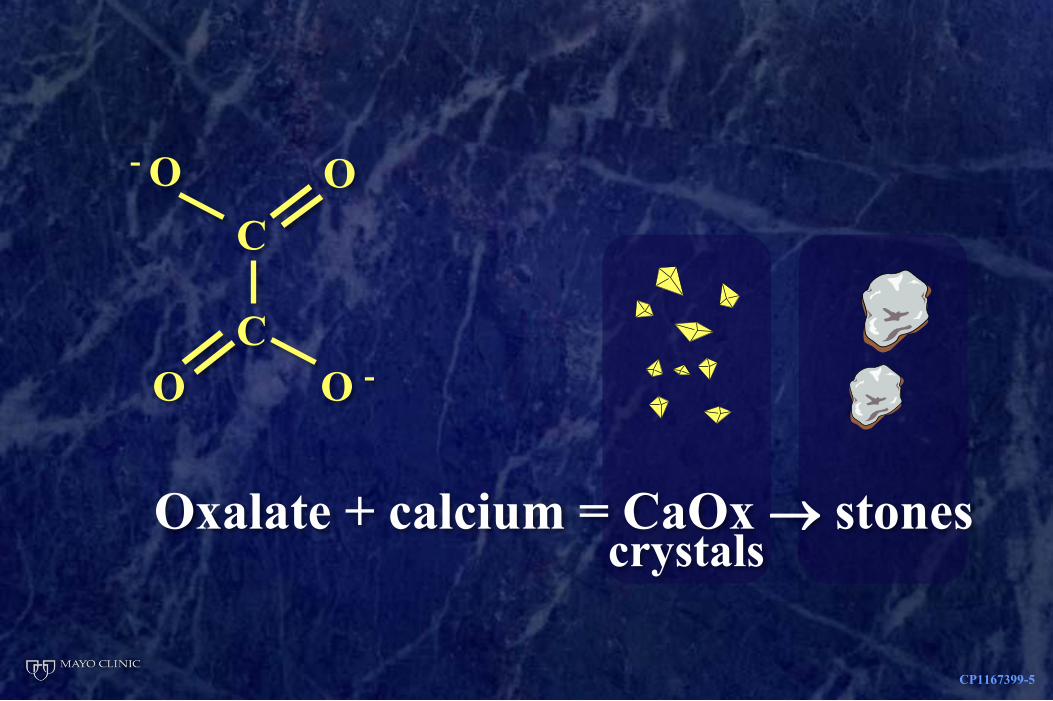
Oxalate + calcium = CaOx stones
CP1167399-5
- O
C
O
C
O O -
crystals
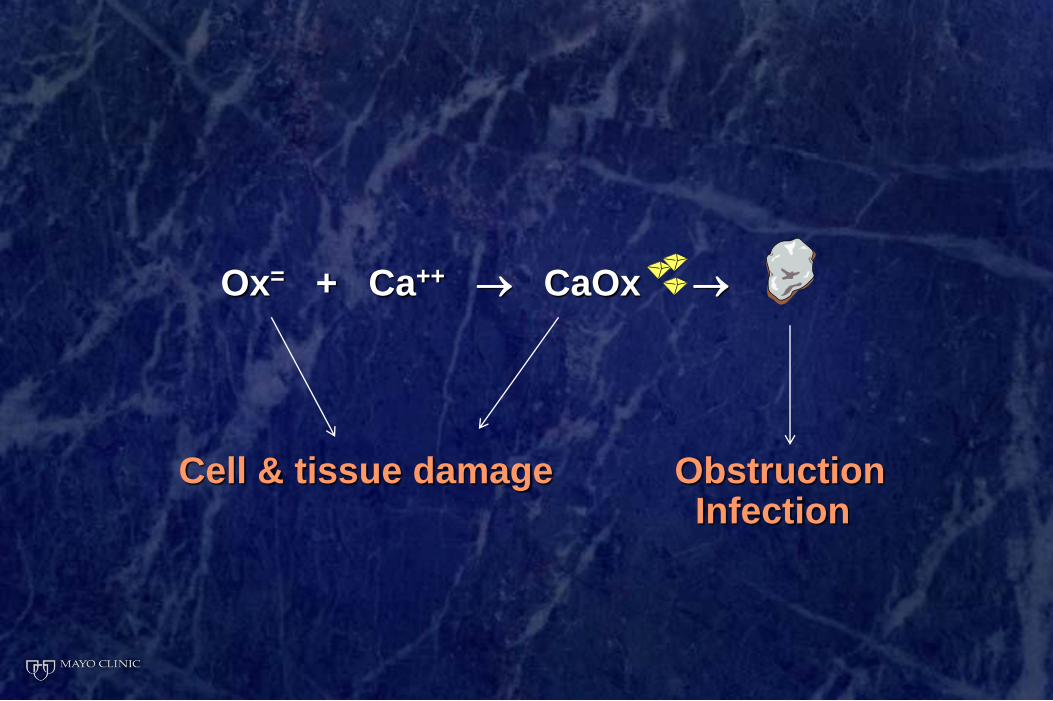
Ox= + Ca++ CaOx
Cell & tissue damage Obstruction Infection
CP1167399-4
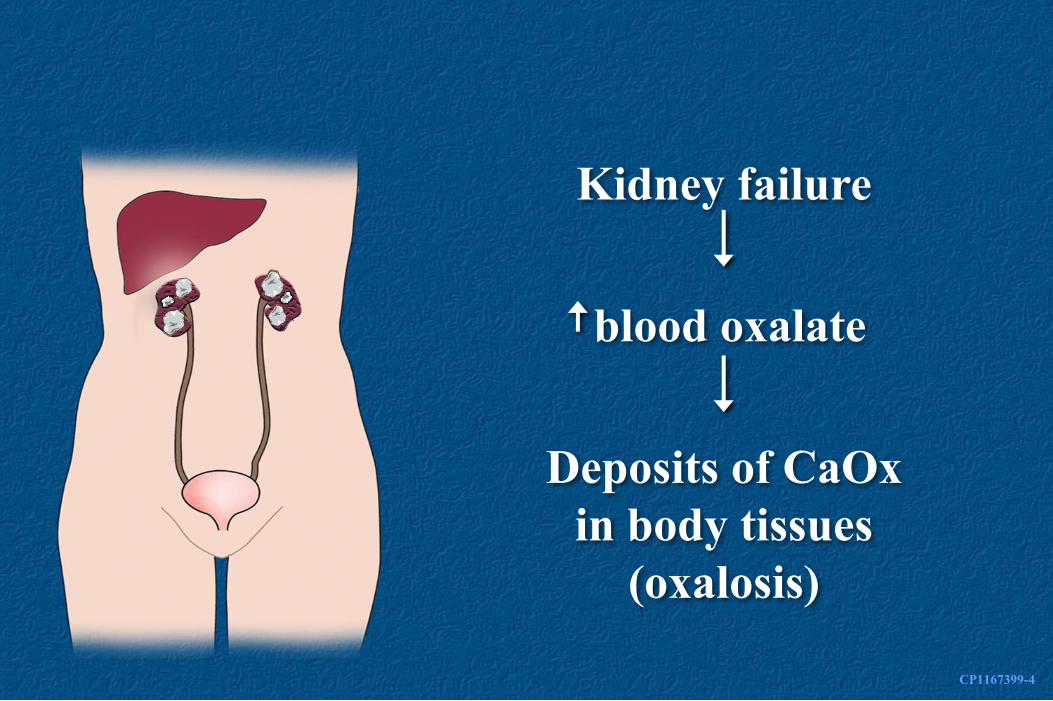
Kidney failure
Deposits of CaOx
in body tissues
(oxalosis)
blood oxalate
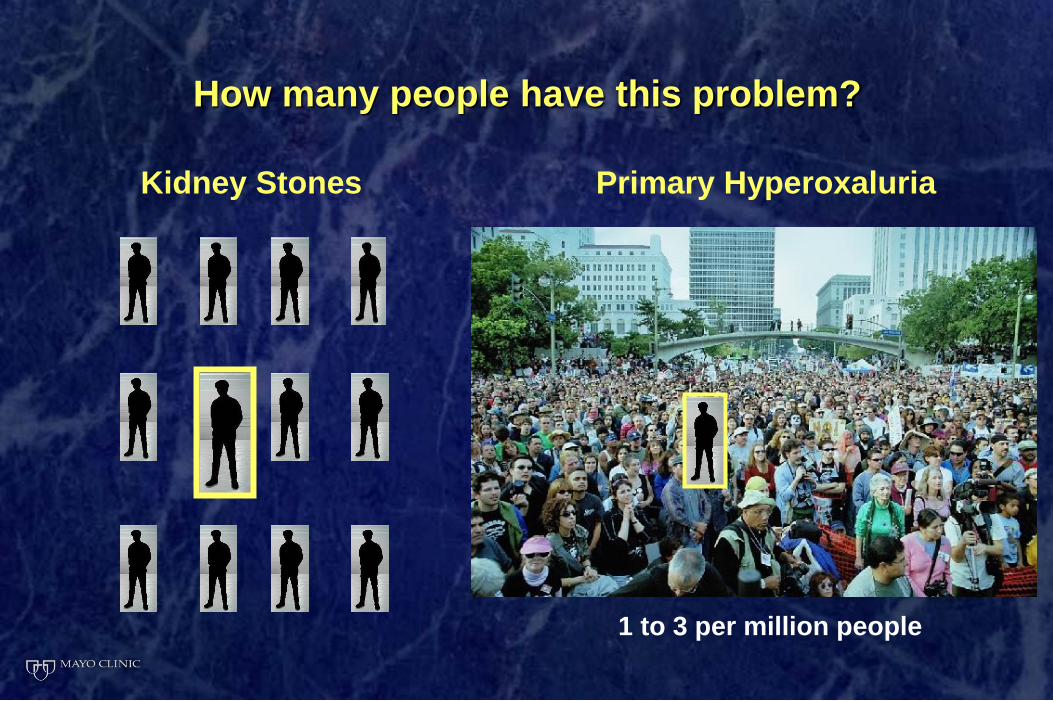
Kidney Stones Primary Hyperoxaluria
1 to 3 per million people
How many people have this problem?

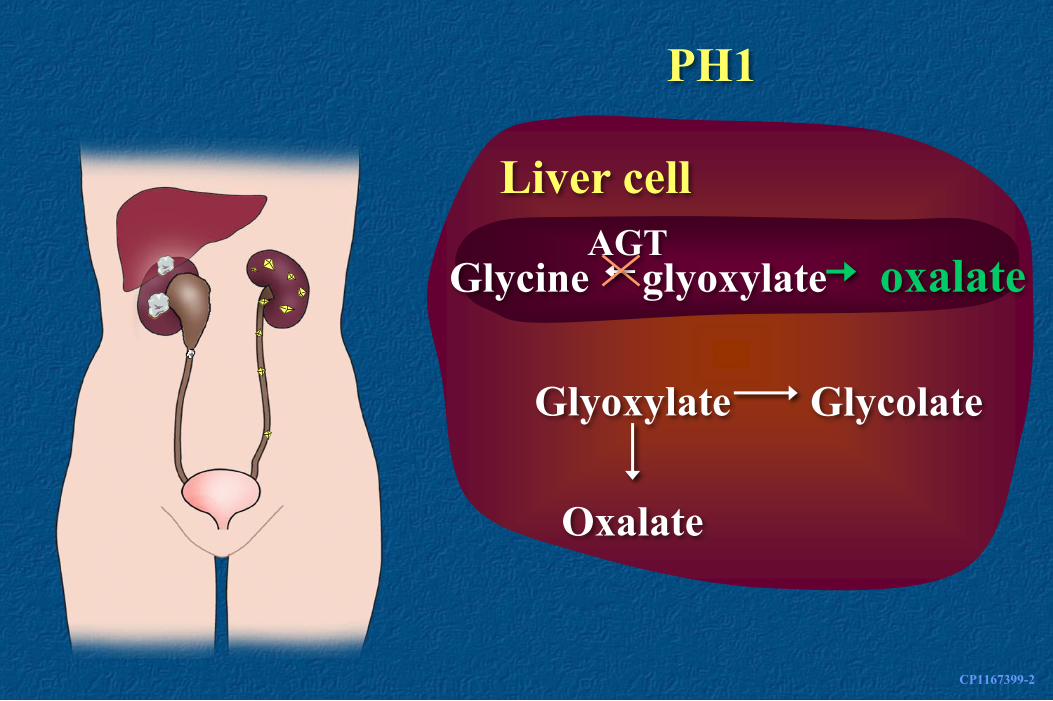
Types of primary hyperoxaluria
PH1 AGT enzyme
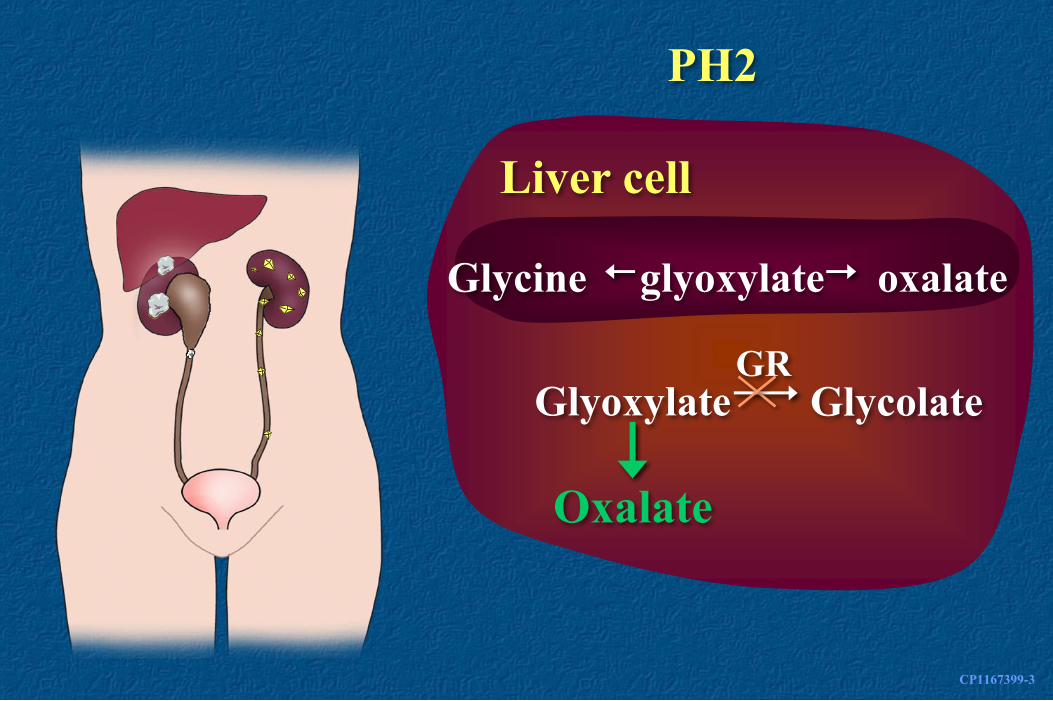
PH2 GR/HPR enzyme
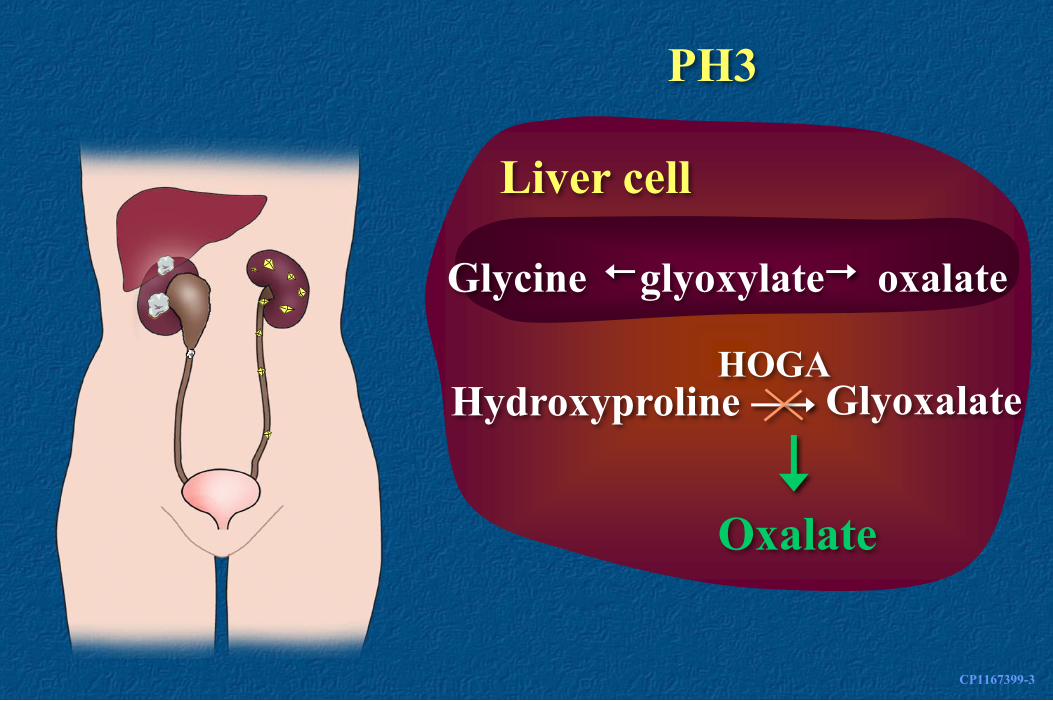
PH3 HOGA1 enzyme
Unclassified ?? cause
CP1167399-2
Glycine glyoxylate oxalate
Liver cell
Glyoxylate
Oxalate
Glycolate
PH1
AGT
CP1167399-3
Glycine glyoxylate oxalate
Liver cell
Glyoxylate
Oxalate
Glycolate
PH2
GR
CP1167399-3
Glycine glyoxylate oxalate
Liver cell
Hydroxyproline
Oxalate
Glyoxalate
PH3
HOGA
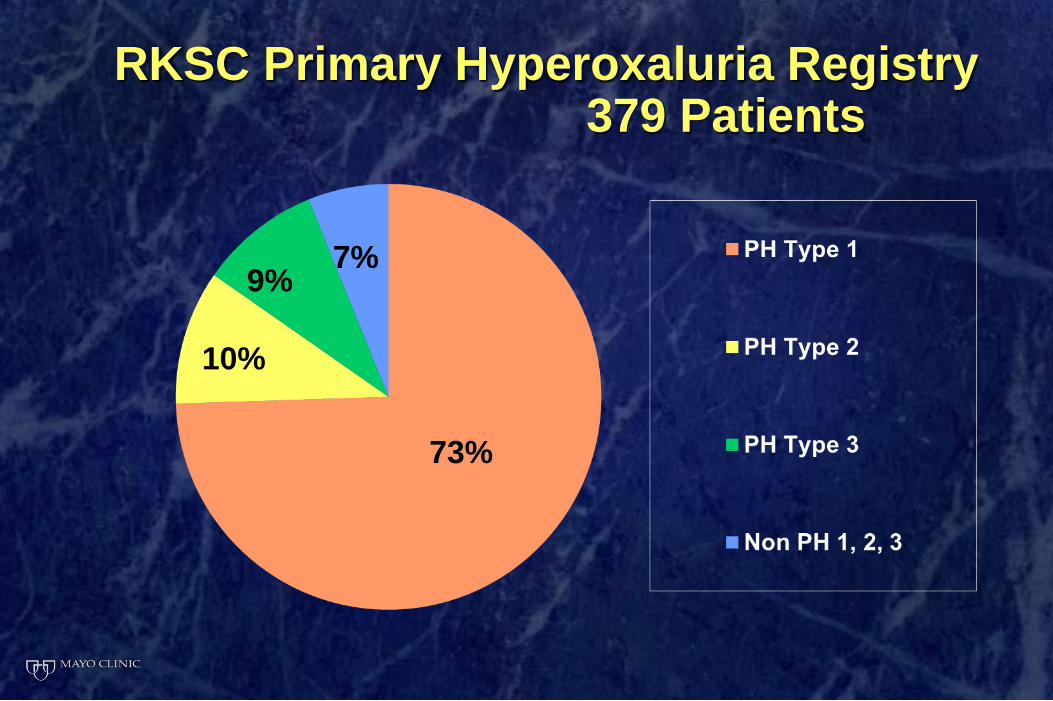
RKSC Primary Hyperoxaluria Registry 379 Patients
73%
10%
9% 7%
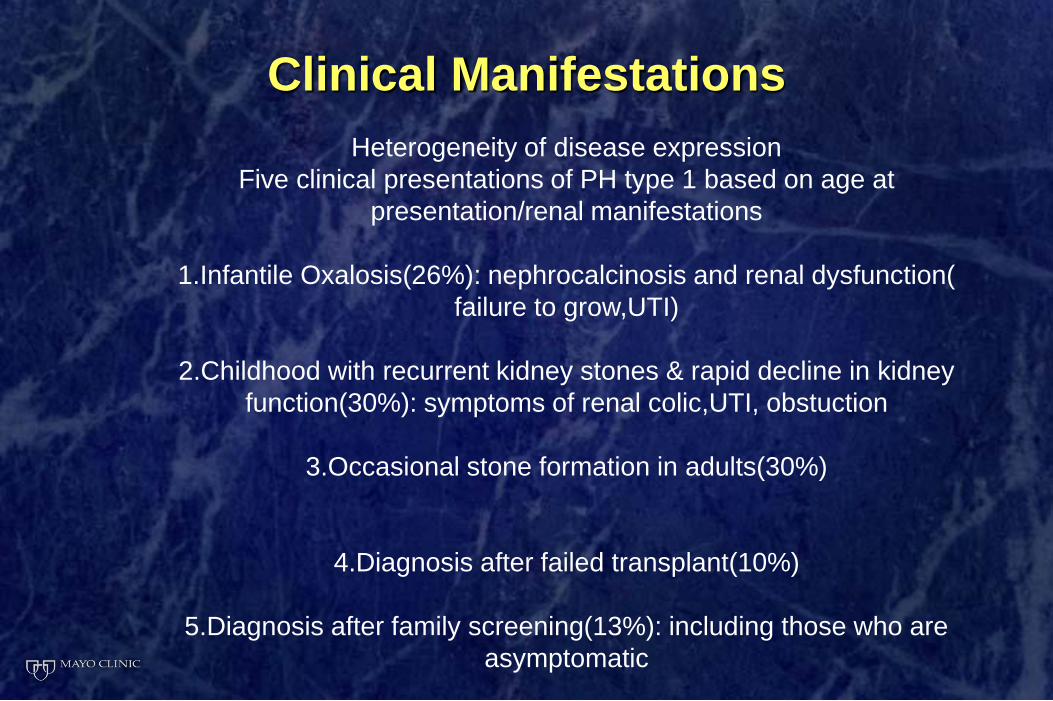
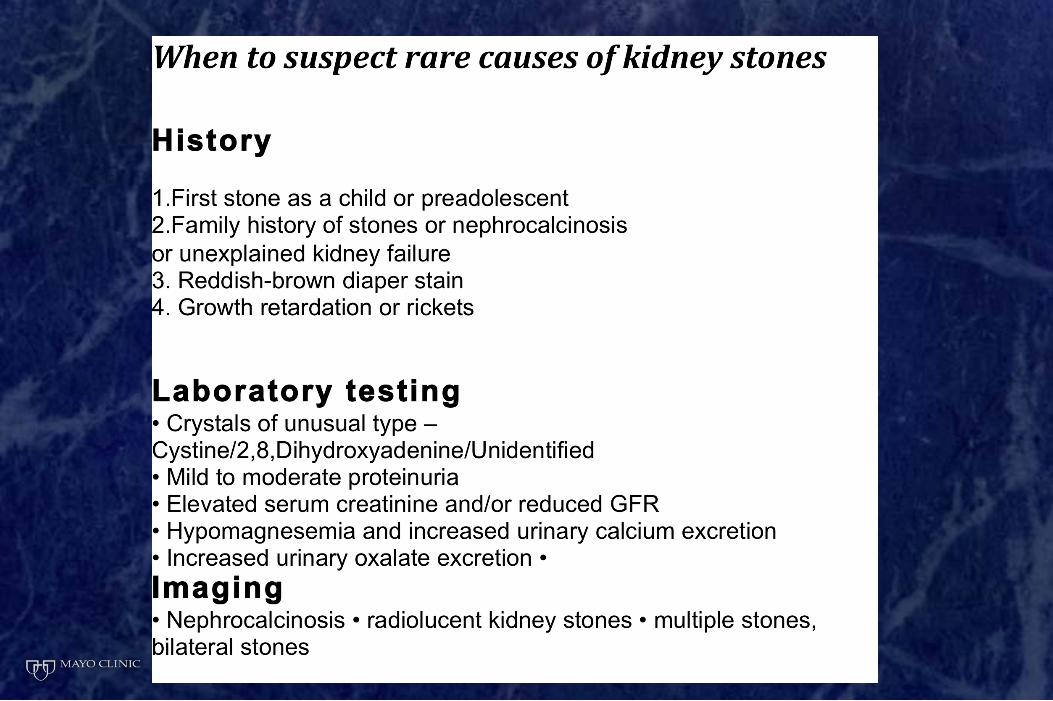
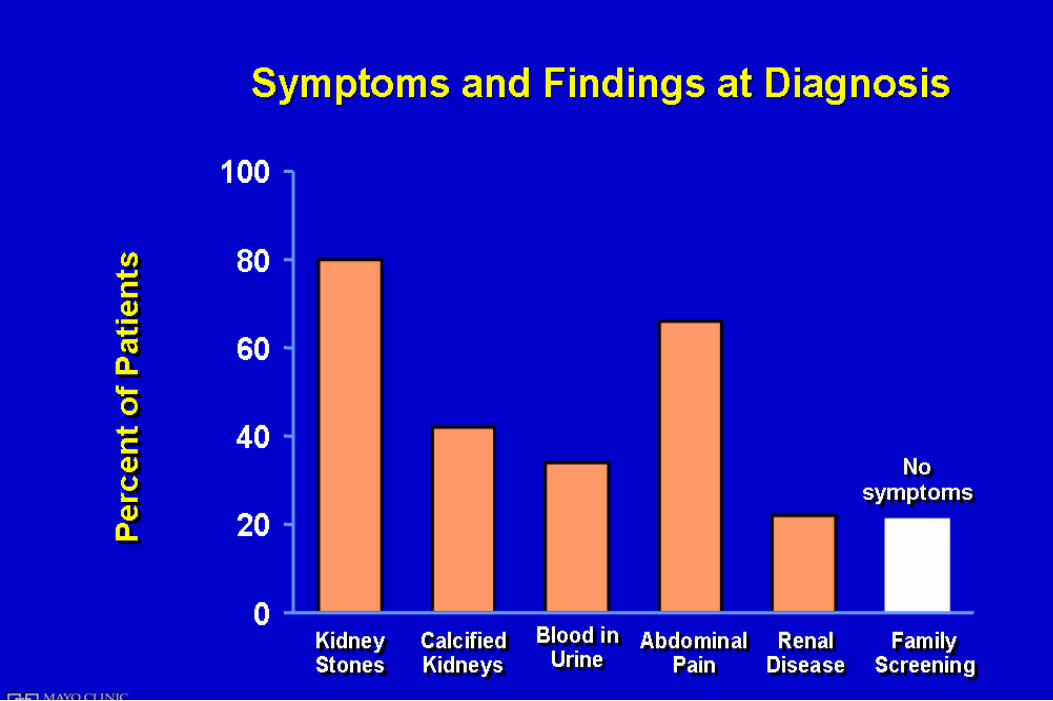
Clinical Manifestations
Heterogeneity of disease expression
Five clinical presentations of PH type 1 based on age at
presentation/renal manifestations
1.Infantile Oxalosis(26%): nephrocalcinosis and renal dysfunction(
failure to grow,UTI)
2.Childhood with recurrent kidney stones & rapid decline in kidney
function(30%): symptoms of renal colic,UTI, obstuction
3.Occasional stone formation in adults(30%)
4.Diagnosis after failed transplant(10%)
5.Diagnosis after family screening(13%): including those who are
asymptomatic
0
1
2
3
4
5
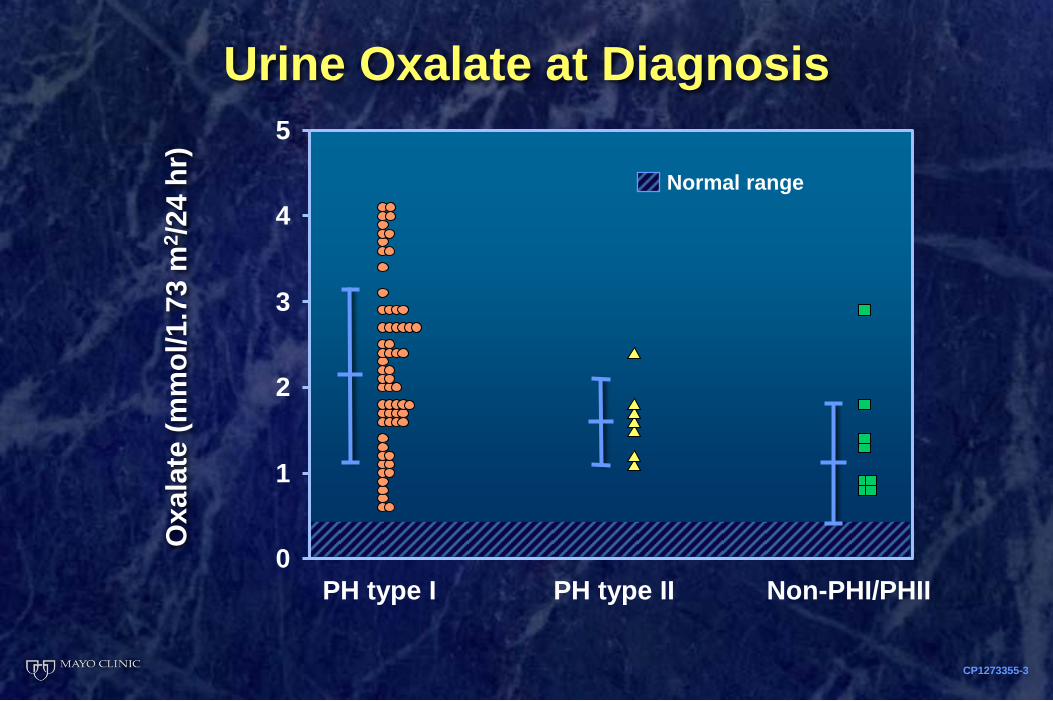
Normal range
CP1273355-3
Oxala
te (
mm
ol/1
.73
m2/2
4 h
r)
PH type I PH type II Non-PHI/PHII
Urine Oxalate at Diagnosis
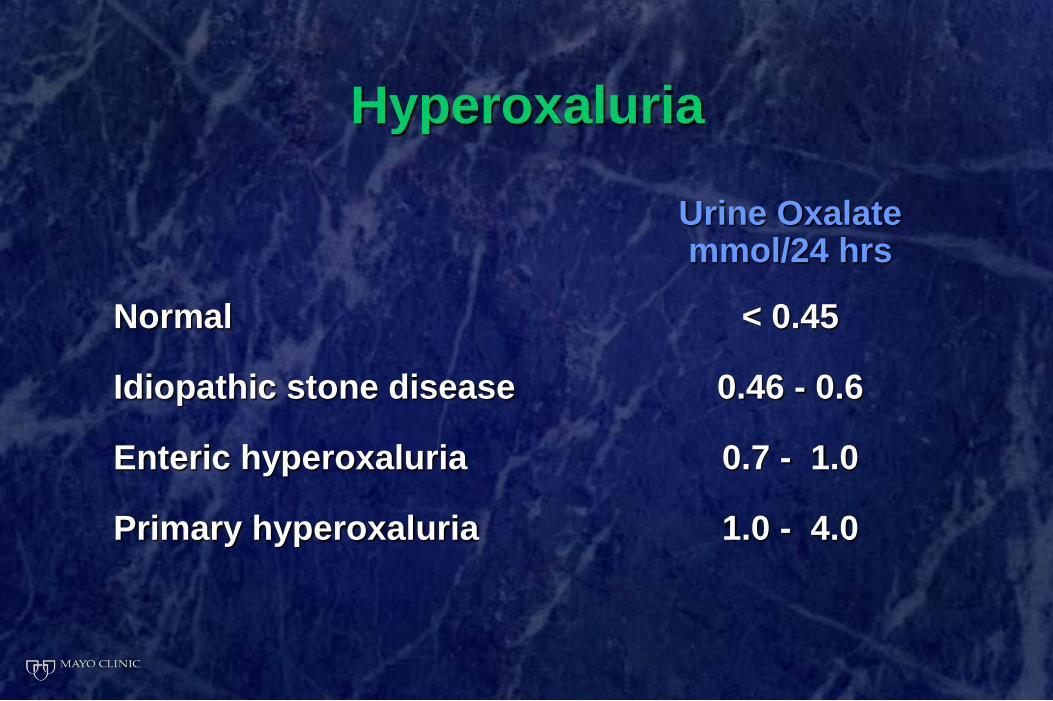
Hyperoxaluria
Urine Oxalate mmol/24 hrs
Normal < 0.45
Idiopathic stone disease 0.46 - 0.6
Enteric hyperoxaluria 0.7 - 1.0
Primary hyperoxaluria 1.0 - 4.0

Plasma Oxalate Measurement
Plasma oxalate levels elevated (>6.3 μM) with
normal renal function
Significantly higher (>80 to 100 μM) in ESRD due
to Oxalosis
Without PH1 (40 to 60 μM)
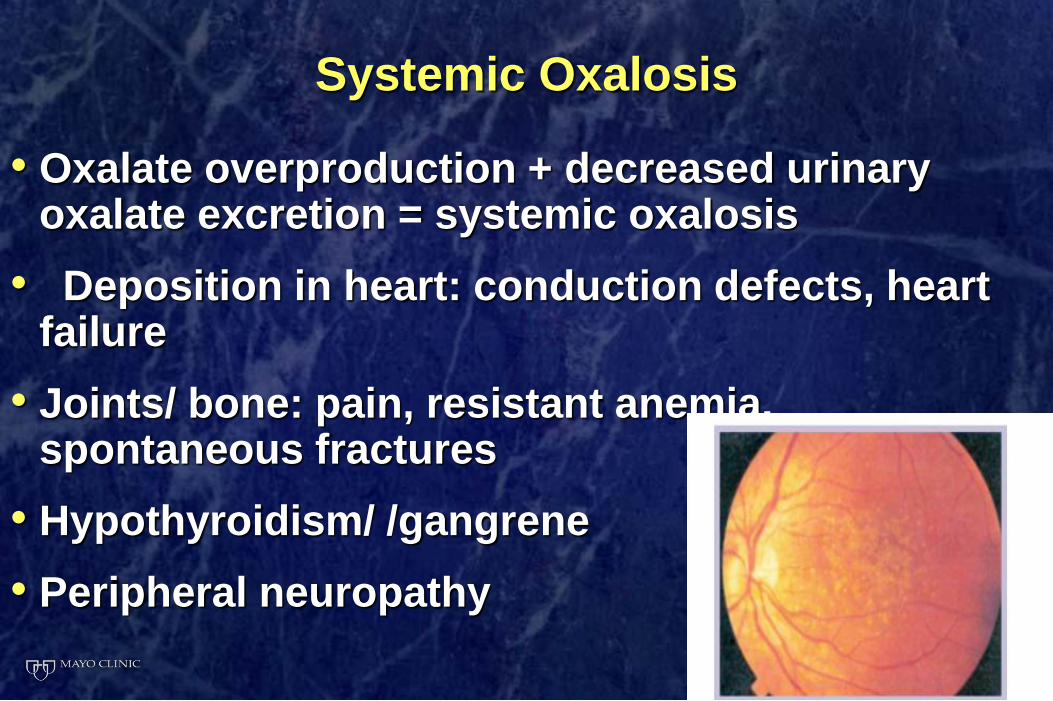
Systemic Oxalosis
• Oxalate overproduction + decreased urinary oxalate excretion = systemic oxalosis
• Deposition in heart: conduction defects, heart failure
• Joints/ bone: pain, resistant anemia, spontaneous fractures
• Hypothyroidism/ /gangrene
• Peripheral neuropathy
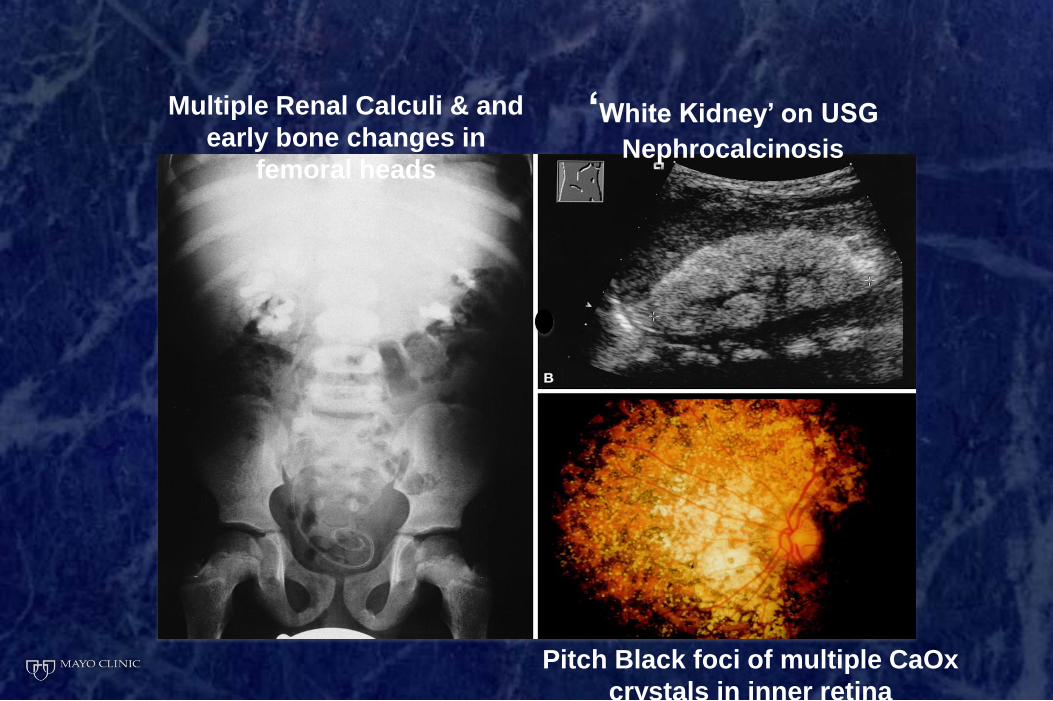
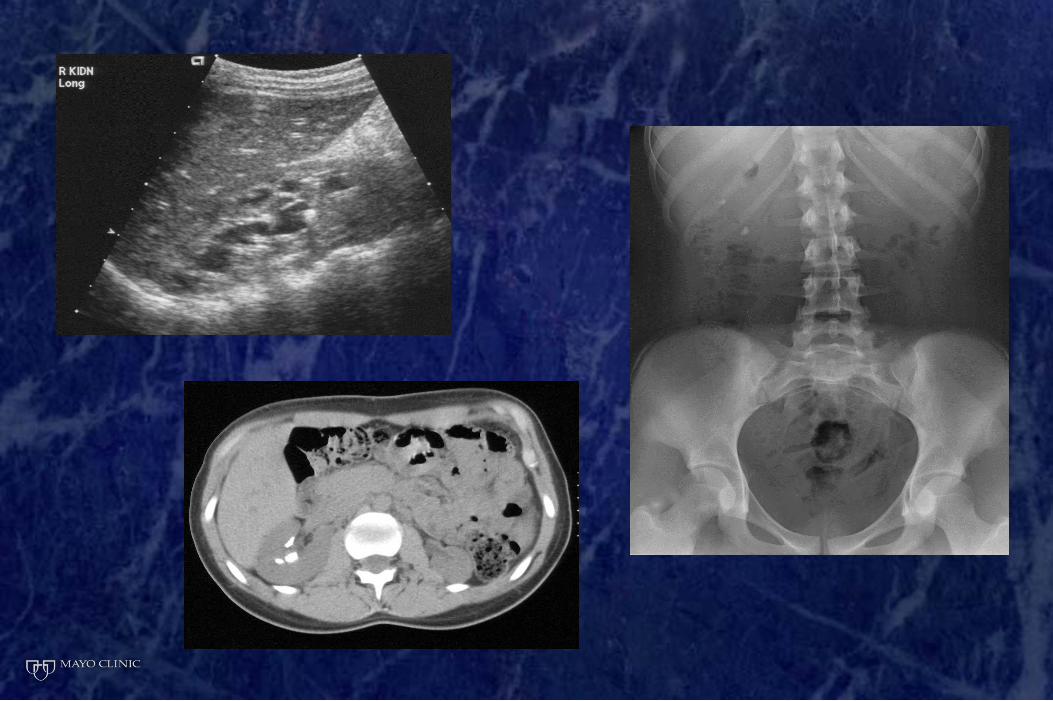
‘White Kidney’ on USG
Nephrocalcinosis
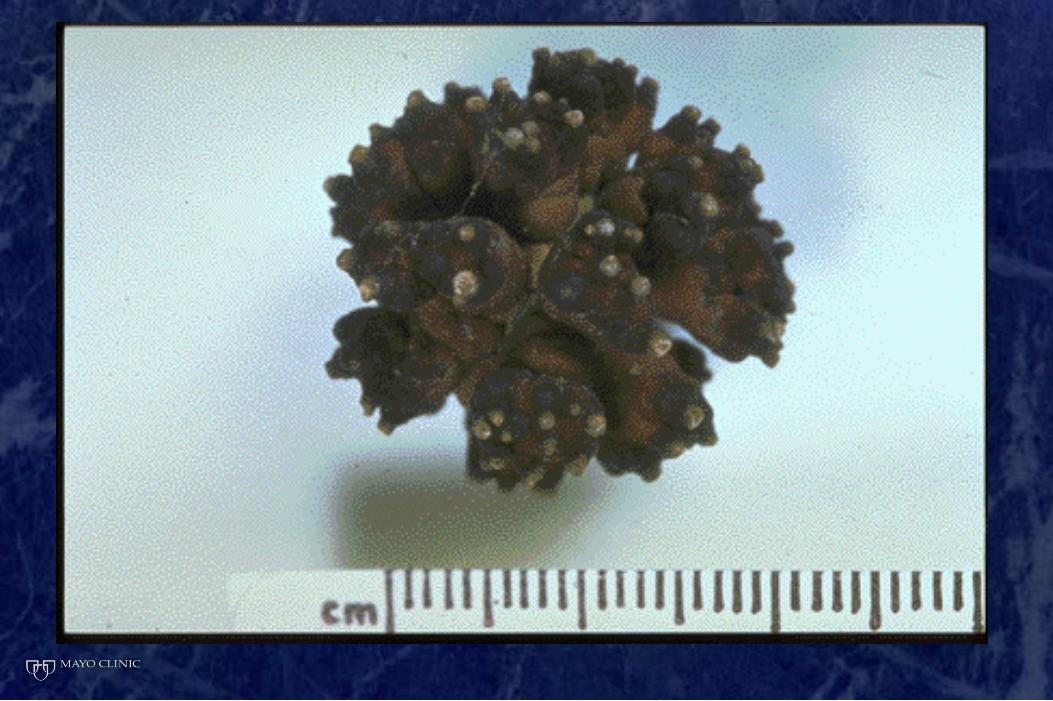
Multiple Renal Calculi & and
early bone changes in
femoral heads
Pitch Black foci of multiple CaOx
crystals in inner retina
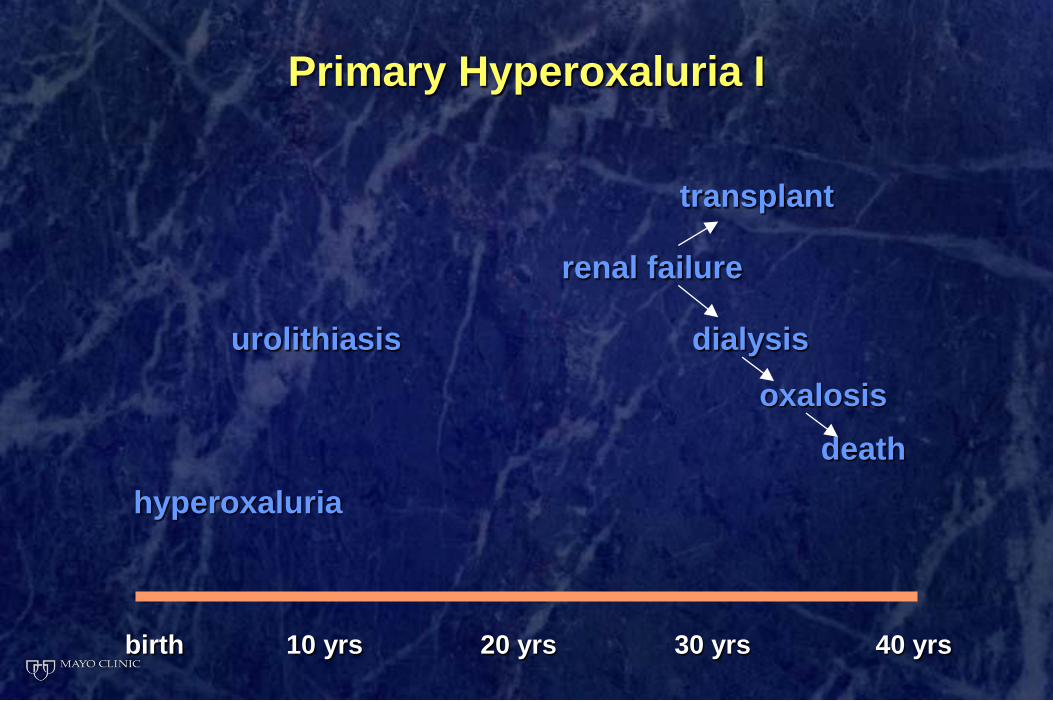
Primary Hyperoxaluria I
transplant
renal failure
urolithiasis dialysis
oxalosis
death
hyperoxaluria
birth 10 yrs 20 yrs 30 yrs 40 yrs
0
20
40
60
80
100
0 10 20 30 40 50 60 70 80
CP1273215-12
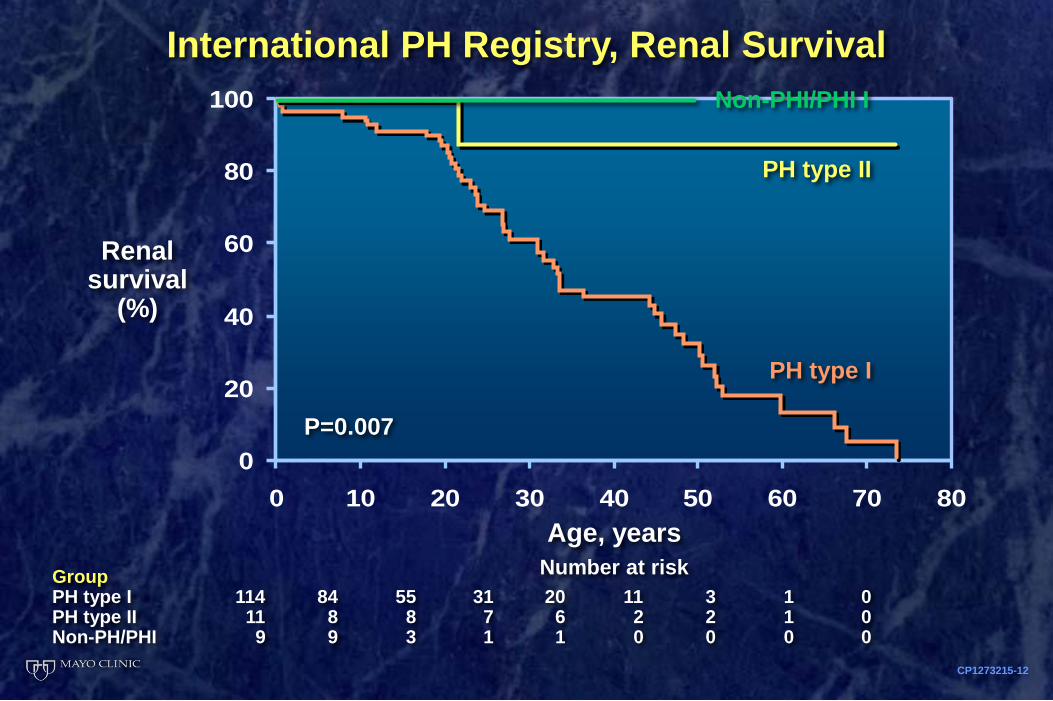
International PH Registry, Renal Survival
Age, years
Number at risk
Renal survival
(%)
P=0.007
PH type II
PH type I
Group PH type I 114 84 55 31 20 11 3 1 0 PH type II 11 8 8 7 6 2 2 1 0 Non-PH/PHI 9 9 3 1 1 0 0 0 0
Non-PHI/PHI I
Clinical metabolic screening (24 hr urinary oxalate by oxidase method,
increased urinary glycolate)
Confirmation by molecular genetic testing: mutation in AGXT gene
Targeted mutational analysis-50-70%
Whole gene sequencing-100%
Diagnosis
GENETICS
4 mutations
Gly170Arg(30-40%)
33_34insC(10-13%)
Phe152Ile(1-5%)
Ile244Thr(3-9%)
Account for 50% of the known 90 mutations of PH typeI disease
Oppurtunity to focus on these to save costs
Caveat: no Indian studies
What can be done to prevent oxalate damage to kidneys?
• Decrease oxalate in the diet?
• Decrease oxalate concentration in urine
• Decrease calcium oxalate crystal formation
• Increase oxalate elimination by the intestines
• Reduce oxalate production by the liver
0
50
100
150
200
Usual Primary
hyperoxaluria
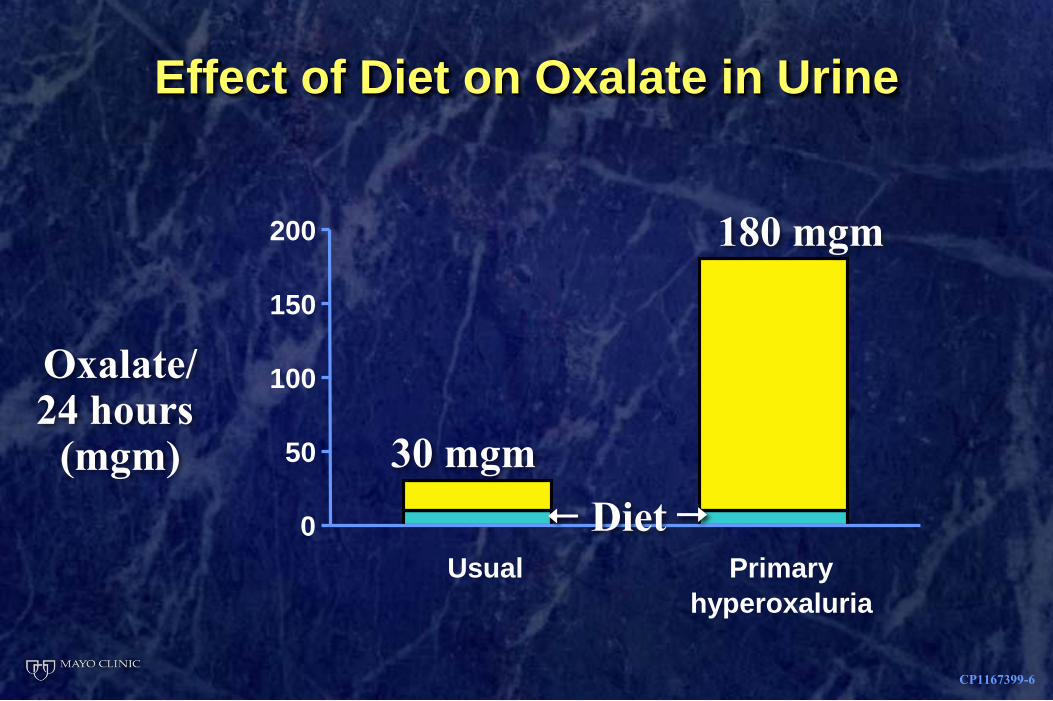
Effect of Diet on Oxalate in Urine
Oxalate/ 24 hours
(mgm)
CP1167399-6
30 mgm
180 mgm
Diet
What can be done to prevent oxalate damage to kidneys?
• Decrease oxalate in the diet?
Little effect
• Decrease oxalate concentration in urine
Drink lots of water
• Reduce calcium oxalate crystal formation
Citrate or phosphate medication
CP1131733-28
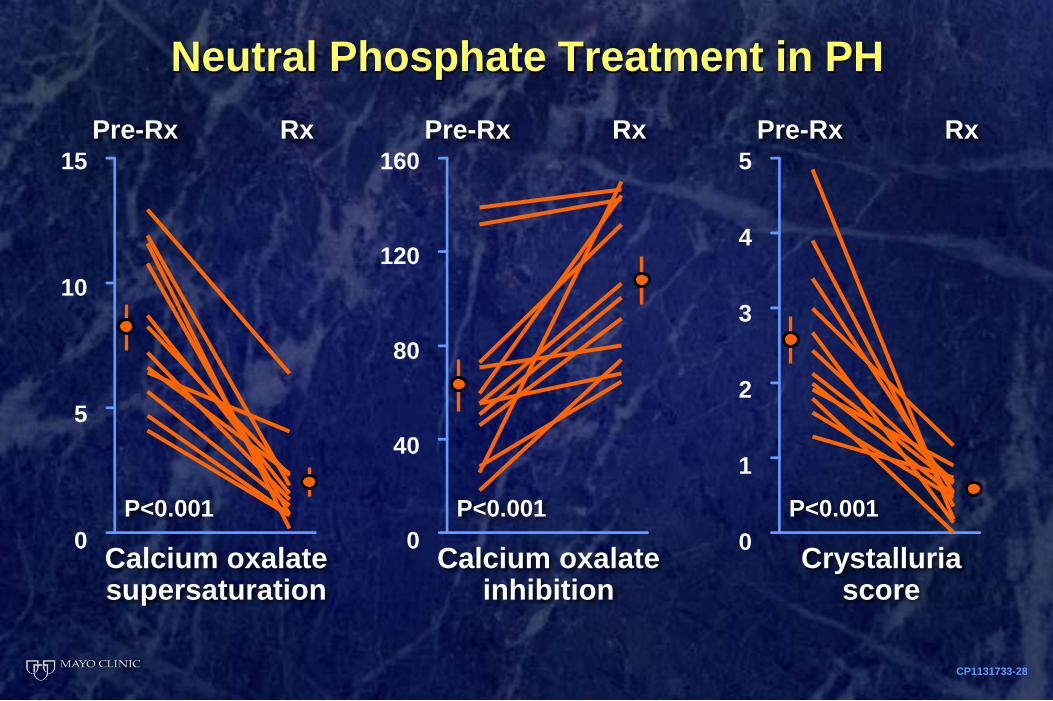
Calcium oxalate supersaturation
Pre-Rx 15
10
5
0
Rx
P<0.001
Calcium oxalate inhibition
Pre-Rx 160
120
80
40
0
Rx
P<0.001
Crystalluria score
Pre-Rx 5
4
3
2
1
0
Rx
P<0.001
Neutral Phosphate Treatment in PH
What can be done to prevent oxalate damage to kidneys?
• Increase oxalate elimination by the intestines
Oxalobacter formigenes
Oxalate degrading enzymes
• Reduce oxalate production by the liver
What can be done to prevent oxalate damage to kidneys?
• Increase oxalate elimination by the intestines
Oxalobacter formigenes
Oxalate degrading enzymes
• Reduce oxalate production by the liver
Pyridoxine (vitamin B6) p.Gly170Arg, c.33_34insC
Liver transplant
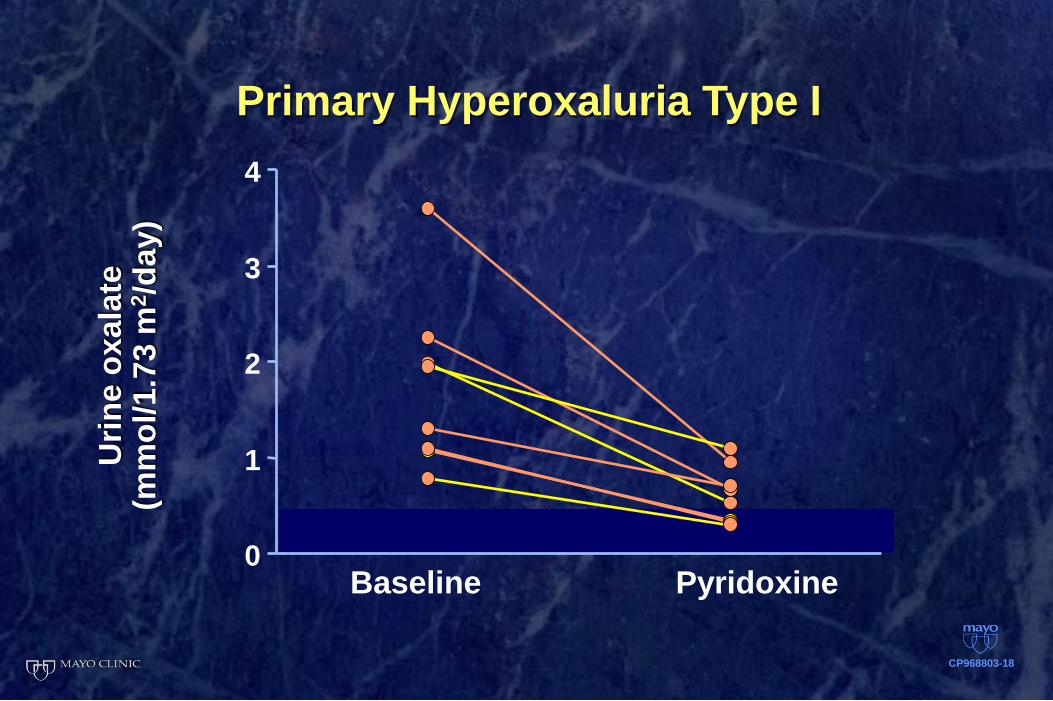
0
1
2
3
4
Primary Hyperoxaluria Type I U
rin
e o
xala
te
(mm
ol/
1.7
3 m
2/d
ay)
CP968803-18
Baseline Pyridoxine
Primary Hyperoxaluria Current Treatment Strategies
By 60 yrs of age, more than 80% of patients with type I PH will have renal failure
Dialysis is not an acceptable option
• Simultaneous/ sequential hepatic & Kidney transplantation
• Restore enzyme activity by liver transplantation
Knowledge of the spectrum of disease expression,
early diagnosis, and initiation of treatment before
renal failure are essential to realize a benefit for
patients.
History of PH at Mayo
• 1967 First PH patient diagnosed at Mayo
• 1974 Research studies with PH patients started in Rochester
• 2003 OHF funded and established the Mayo Clinic Hyperoxaluria Center in Rochester
• 2004 International PH Workshop and first PH Patient meeting in Rochester
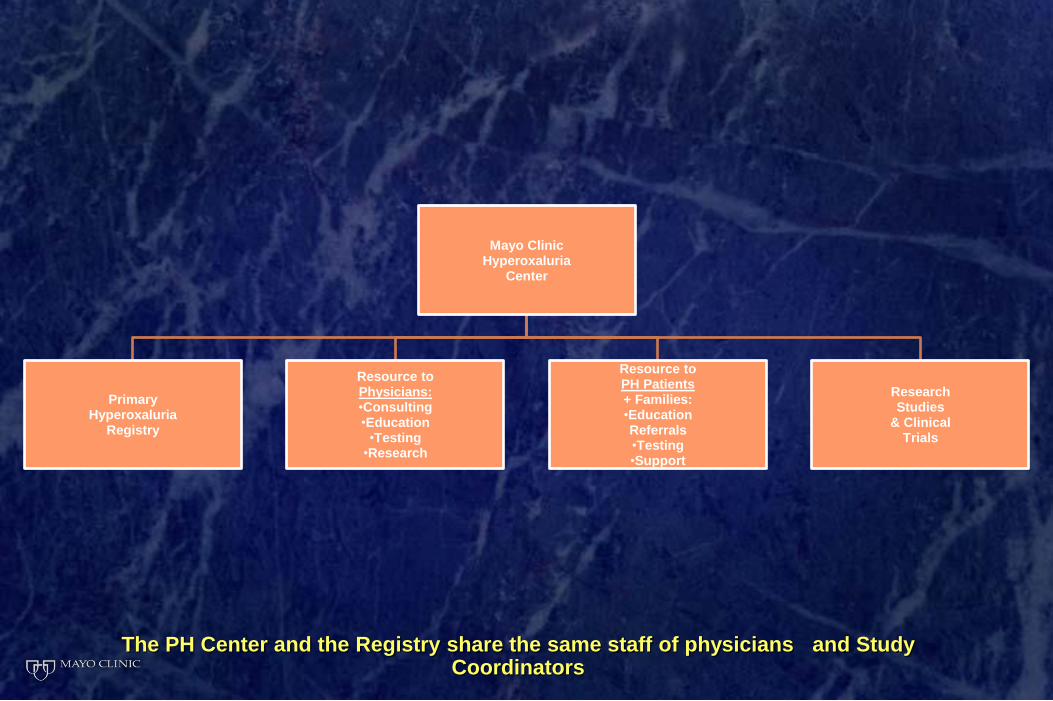
The PH Center and the Registry share the same staff of physicians and Study Coordinators
Mayo Clinic Hyperoxaluria
Center
Primary Hyperoxaluria
Registry
Resource to Physicians: •Consulting •Education •Testing •Research
Resource to PH Patients + Families: •Education Referrals •Testing •Support
Research Studies
& Clinical Trials
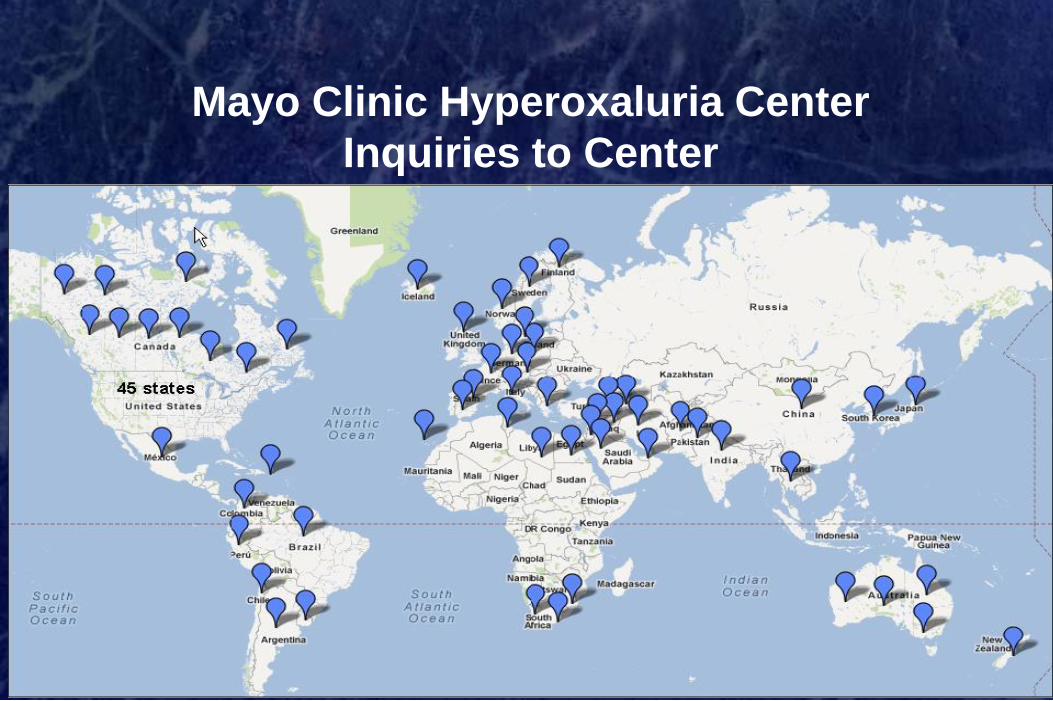
Mayo Clinic Hyperoxaluria Center
Inquiries to Center
Post transplant recurrence study presenting at
Mayo Clinic, Rochester, Minnesota, USA