Understanding Health Disparities: Ihe Role of Race and ... · Logistic regression dalyses wen...
7
ntstAncil AltD PRAcTrcr Understanding Health Disparities: Ihe Role of Race and Socioeconomic Status in Children's J|ealth EdithChen, PhD, Andrew D. Martin, PhD, and Karen A. Matrhews, PhO Heatth dnpdities reflectdifrerence, in health be€Ne of sociodemographic vdiables,such 6 €ce, socioeconomic stahs (SES), @d gen' der' BoL\ mcial dd socioeconomic di5p{i- ties in health@ polbundly evidentin lhe UnitedSt^tes, soch t'at Healthg People 2010- the nationalstatemeni ofheal& obje.tives h6 nade 1of its 2 ovetuching goals the €limination of healih dispdities.' Low SES individuals consistently have poorer bealththm high SES individuals acros a vdiety of morbidiry dd mortariry out@mes.' 5 Unde6tanding these reladons edly in lite is aitical not only tor neimizing dfldren's healih but alsofor undeBtanding ihe origirs ol adult drspuites in health. Lort SES ha beeD Nociated with poorerhealth in childhood.6 1r For exMple, lowepsEs childrenft les likely to receive vaccinations @d iravecontaci with ph'sicim at edty ages.i'2 LowerSES childrenhavepoorer healthbehavioF,including higher injury rai€sai yomg ages ed gr€ater rat€s of smoking dd sedentary behavioB.6r LoweFSES childrenaho sufier tron dmnic impaimenls,such6 higher6tes of hospitalizations for 6thDa. ud greater acdv ity liDitations.6lro Dis?eties in c}ildhood h€althhaveheary cosls. For exmplq on lhe bdis of prcjected inability to work or lost tin€ hon work in adulthood because of iI- nes, childrenliving in pderty de prcjected ro cosr theunired slates $130birlion ($1990) in tutm econodic outsut'3 Sinilarly, childrenbelonging to minoriry gmups havepoorerhealih.For exa.mple, Black fanilies bav€ higher ntes of low- birthweight babies dd inlant mortaliry iho do White fmilies.1L16 Blackchildrenhave higher rates or elevated levels of blood leadi' dd m nore likely to havefanlpoor healih than are \\/h& cnndren.rt Black motheBe less likely to recive prenatol carethan ar€ \\hite moihe6, ed Black childrcnafe more likely to be hospitaliz.ed for conditioN suchd Oblecr,ees we sought to dererm,.e whel_er chirdhood rerlrF d,spdf ries dre best understood as effectsof race,socloeconomic status lSES), or synergistic effects oflhe two, Methods. Data from the NationalHealth Interyiew SuNey 1994 of US children aged 0 to 18 yea6 (n=33911)were used. SES was measured as parental educa' tion. Child health measures included overall health. limitations. andchronic and acute ch ldhood conditions. Aesu/ts. For overallhealth, activityand schoo limitations, and chroniccircu a- toryconditions, the ikellhood ofpooroutcom€s in€reased as parentaleducation decreased. These relationships wefe stronger among Whiteand Blackchildren, and weaker or nonexislent arnong Nispanic and Asian children. However, Hispanic andAsian chidren exhibited an opposite relationshipforacuie respiratory illness, whereby children with moreeducated parents hadhigher rates ol i Iness. Concluslons. The tradiiionalfinding offewer years of parent education being associated with poorer health in offspring is mo prominent among White and BlackchildrenandleastevidentamongHispanicandAsianchildren.Thesefi ingssuggest that lifestyle characteristics (e.9., cultur€l norms for h€allh behav- io6)oflow-SES Hispanic andAsian children may b!fierthem from health prob- le..s,Future interventionsthatseekto bo sterthese characteristics among other low SES children may be important for reducing childhood health disparities. lAm J PubIic HeaIth. 2006t9617A2-7 04. doiJO-214fl4JPH.2004.044124) ticllarly pronouced mong minonq/gmups, pe.hdps ifpovedy etrects e compoDdedby dcisn.'r '1 he 'otion that individuats who be- longto multiplegrcups lacing disoimination de rhe m6t disadvmtaged hs baente@ed fie dotble jeapatlg hpothetis'azE Altematively, the effects of low SES could b€ nore pronounced srDong goups that de nativebom. This night occlr because idmi gmts m morelikely to havebetler health the those in the native-bom population, evenif Orey ft lower in SES, a phdondo :ened t}Le health! iftftlgant 4fed.'1'q It $hiies od Black e less likely to be ilmi g@ts, th€y may eihibi! stonger .elations betNeen SES dd healthi.\u ofter ninoriiy grcups Altematively, ifbse raies ofmdy ilnes re higher mong Bhcks tha mong t{'tita. a ceilingefiectnay exis! suchthat the erecl of SES on bealth is le$ appeent among Blacls Lbo mong Whites. Finalb. cerlan SES ndictoE may be a poorermailer of SES mong sone dinonty asihma-? Fewer datahav€histonca y b€en avanable on oL\er ethnic groups, andh€tere geneiry wlhin gmops n6les pafrem nore tliffi@lt to interprei However, thereis some evidence thal HjspMic dd Asid children @ more lilcly to havetair/poor heal& tho are White childien,'" md that cddiovsc d risk t?ri,ors such€sbody na.s index andgly cated hemoglobin levels de highermong Hispmi6 thd mong Uhjtes.B The vat majodty oI resedch on health disp4itiesha foosed on eitherSES or mce andoften conhlh for I facior wheD testing the etrect of tbe orhersYe!SES andraceare dNIy intertwined, wiih nemben of muy ninoriu grcups, on aveEge, beingloner in SES.'o Tlus. some researcrreN havea+ued that resetuches shor d bc testing for intenc- tion efie.ts between m@ dd SES.'r 'r An intemciion behveen €e dd SES codd ta}€ a nunber of forms. Rac€ andSES codd interactsynergistically to affect heallh. That is, ihe effecLs ot low SES conldbe pd- Peer Revewed I Che, er ar
Transcript of Understanding Health Disparities: Ihe Role of Race and ... · Logistic regression dalyses wen...

ntstAncil AltD PRAcTrcr
Understanding Health Disparities: Ihe Role of Raceand Socioeconomic Status in Children's J|ealth
Edith Chen, PhD, Andrew D. Martin, PhD, and Karen A. Matrhews, PhO
Heatth dnpdities reflect difrerence, in healthbe€Ne of sociodemographic vdiables, such6 €ce, socioeconomic stahs (SES), @d gen'der' BoL\ mcial dd socioeconomic di5p{i-ties in health @ polbundly evident in lheUnited St^tes, soch t'at Healthg People 2010-the national statemeni ofheal& obje.tivesh6 nade 1of its 2 ovetuching goals the€limination of healih dispdities.'
Low SES individuals consistently havepoorer bealth thm high SES individualsacros a vdiety of morbidiry dd mortariryout@mes.'� 5 Unde6tanding these reladonsedly in lite is aitical not only tor neimizingdfldren's healih but also for undeBtandingihe origirs ol adult drspuites in health. LortSES ha beeD Nociated with poorer healthin childhood.6 1r For exMple, lowepsEschildren ft les likely to receive vaccinations@d irave contaci with ph'sicim at edtyages.i'2 LowerSES children have poorerhealth behavioF, including higher injuryrai€s ai yomg ages ed gr€ater rat€s ofsmoking dd sedentary behavioB.6r
LoweFSES children aho sufier trondmnic impaimenls, such 6 higher 6tes ofhospitalizations for 6thDa. ud greater acdvity liDitations.6lro Dis?eties in c}ildhoodh€alth have heary cosls. For exmplq on lhebdis of prcjected inability to work or losttin€ hon work in adulthood because of iI-nes, children living in pderty de prcjectedro cosr the unired slates $130 birlion ($1990)in tutm econodic outsut'3
Sinilarly, children belonging to minorirygmups have poorer healih. For exa.mple,Black fanilies bav€ higher ntes of low-birthweight babies dd inlant mortaliry ihodo White fmilies.1L16 Black children havehigher rates or elevated levels of blood leadi'�dd m nore likely to have fanlpoor healihthan are \\/h& cnndren.rt Black motheB eless likely to recive prenatol care than ar€\\hite moihe6, ed Black childrcn afe morelikely to be hospitaliz.ed for conditioN such d
Oblecr ,ees we sought to dererm,.e whel_er chi rdhood rer l rF d,spdf r ies drebest understood as effects of race, socloeconomic status lSES), or synergisticeffects oflhe two,
Methods. Data from the National Health Interyiew SuNey 1994 of US childrenaged 0 to 18 yea6 (n=33911)were used. SES was measured as parenta l educa't ion. Chi ld heal th measures inc luded overal l heal th. l imi tat ions. and chronic andacute ch ldhood condi t ions.
Aesu/ts. For overall health, activity and schoo limitations, and chronic circu a-torycondi t ions, the ike l lhood ofpooroutcom€s in€reased as parenta leducat iondecreased. These relationships wefe stronger among White and Blackchildren, andweaker or nonexis lent arnong Nispanic and Asian chi ldren. However, HispanicandAsian chidren exhib i ted an opposi te re lat ionshipforacuie respi ratory i l lness,whereby chi ldren wi th more educated parents had h igher rates o l i Iness.
Concluslons. The tradiiionalfinding offewer years of parent education beingassociated wi th poorer heal th in of fspr ing is mo prominent among Whi te andBlackchi ldrenandleastev identamongHispanicandAsianchi ldren.Thesef ind-ings suggest that l i festy le character is t ics (e.9. , cu l tur€ l norms for h€al lh behav-io6)of low-SES Hispanic and Asian chi ldren may b! f ier them f rom heal th prob-le. .s , Future in tervent ionsthatseekto bo ster these character is t ics among otherlow SES chi ldren may be important for reducing chi ldhood heal th d ispar i t ies.lAm J PubIic HeaIth. 2006t9617A2-7 04. doiJO-214fl4JPH.2004.044124)
ticllarly pronouced mong minonq/ gmups,pe.hdps ifpovedy etrects e compoDded bydcisn.'�r '1 he 'otion that individuats who be-long to multiple grcups lacing disoiminationde rhe m6t disadvmtaged hs baen te@edfie dotble jeapatlg hpothetis'�azE
Altematively, the effects of low SES couldb€ nore pronounced srDong goups that denative bom. This night occlr because idmigmts m more likely to have betler healththe those in the native-bom population,even if Orey ft lower in SES, a phdondo:ened t}Le health! iftftlgant 4fed.'�1'�q It$hiies od Black e less likely to be ilmig@ts, th€y may eihibi! stonger .elationsbetNeen SES dd health i.\u ofter ninoriiygrcups Altematively, ifbse raies ofmdyilnes re higher mong Bhcks tha mongt{'tita. a ceiling efiect nay exis! such thatthe erecl of SES on bealth is le$ appeentamong Blacls Lbo mong Whites.
Finalb. cerlan SES ndictoE may be apoorer mailer of SES mong sone dinonty
asihma-? Fewer data hav€ histonca y b€enavanable on oL\er ethnic groups, and h€teregeneiry wlhin gmops n6les pafrem noretliffi@lt to interprei However, there is someevidence thal HjspMic dd Asid children@ more lilcly to have tair/poor heal& thoare White childien,'" md that cddiovsc drisk t?ri,ors such €s body na.s index and glycated hemoglobin levels de higher mongHispmi6 thd mong Uhjtes.B
The vat majodty oI resedch on healthdisp4ities ha foosed on either SES or mceand often conhlh for I facior wheD testingthe etrect of tbe orhers Ye! SES and race aredNIy intertwined, wiih nemben of muyninoriu grcups, on aveEge, being loner inSES.'�o Tlus. some researcrreN have a+uedthat resetuches shor d bc testing for intenc-tion efie.ts between m@ dd SES.'�r '�r
An intemciion behveen €e dd SEScodd ta}€ a nunber of forms. Rac€ and SEScodd interact synergistically to affect heallh.That is, ihe effecLs ot low SES conld be pd-
Peer Rev ewed I Che, er ar

RtStARCl| AI{D PRACTICI
groups. For ermple, minonry gmup nem-bels on avenge do not receiv€ tne sme fi-nocial gains for equivalent yem ot edu@-tion s do whites.'�u'�q which could r€sult inlvhites having a stronger SES gEdient th@
We tested ou reening by dalyzilg raceby SES (on th€ bais olpmntal edu@tion)intemctions predicting health ouhomes in alarye, nationally repr€sentaive $mple ot USchildren. These malyses could provide infor-mdtion about ihe ut iry of Nesing healthdjspdities usng SES, Ece, or $ne combina-
METHODS
SampleDala ar€ tum the Naiional Health bieriew
Swey 1994, a mulGtage, ct]]sectionalhousehold inteNiew swey ol L\e civilie,nonistitubonalized poplLlation ot the UniiedStales, conducled by ihe National Center forHealtll Siatisti6. Data froh c] ldren aged 0ihrcugh l8 yean were included in thesetualyses. In Dost clies, a prciy adult respon-dent (usudly the child s mother) wm usedlor peEons youger thd 19 yem. Datawere erfacted fiom 1994 be@Ne this sm-ple contained more fte twice d nuy clrn-dEn (n:33 911 ) a! any subsequeni yed ofNational Health Intewiew Swey data.
A iotal of 20717 chiklren were clsifieds white (61{,/o), 5776 d Black (17q0),4785s Hjspeic (14qd, ed 1088 s Asie (3q0),
witb the €mainder ctdsified d Othe. o. unknoM. The average age ol chndrcn in thissainple was 8.72 yem 6D=5.35), and 490/0wer€ ten€le. Tbe Ece grcups did not ditrer ingender conposition but did differ ir age, wthHi?dic cbndren being slightly youger thdother children (P<.001). Details about ihedesign ud methods ofrhe National HealthIrtewiM Suwey cm be foud elsewhere.3o
SES SES w4 mesured by the highestlevel of edu@bon of pmnts o. the respon-sible adult in the household. SES cm beme@red in severdl ways (e.9., educatio',ocopation, income), wiih each having dif-ferent irnplications.3r3' Education was usedin the present shrdy because ii is the nosl
stable indicato. otSES.5 Also, given thatninorities do noi receive the san€ fll1ancialgains for equival€nt years of education ddo \Vhites,'�a" education Day be a betterindi@tor of distibution of SES across racbl
The nmber of yem ol edu@tion wscoded fton 0 to 18 (18=18 yem or more).The average education ol pmnis was13.35 years (SD=2.79). As expected, theEcial groups difiered in average educatio.,with Whit€s and Asians having moreyears of educaiio! th@ Bla.ks dd Hispdi6(P<.001). SES dispdities were tested byprcbirg differences a$oss &e educationgndient in chjld heallh.
rR@ Participuts' mce was coded inio 1 of5 categons: White, Bla&, Hispejc Asio,dd Other Because the Other category mmal ud not always idenufiable, these pdtid-pdts were not jncluded in ealyses. Gte-goris for Whiie, Black, and Asie were a*ated by asking rerpondents io identi4, thegrcup that represenied their childt mce. Re-spondents were also sked whether ine dild songir/mceslrf belong€d to ey Hi?dicgrcups lisied. ThG vdiable @ sed io cat€-gorize dndren d His?anic. lt should be noledftat there @uld be ovedap ams 0re 2 ques
tions (e.g., a dnld being identified d boh Hispmic dd White). Like otber rere8rlEs, weu*d the Hisparic coding fist ed tien cate'gorized non-Hispanic .l dren aeorditg tofrce (thc, Vr'hites reflect non'lnspuicWhites).7 Racisl dispsrities were t6ted bycompding each minonty grcup with $hites.
fldl,l We testld 3 types ofhealth out'
comes: (1) genenl healtn raiings, (2) chrcnc
childhood onditions, od (3) acuie childhood
Gaml,leadr. nespondentt were skedwbetler the child's health wd ex.ellent verygood, good, lair, or poor Tbis vdiable wddicholomized into those reporting fairlpoor
h€alth (1) and those reporting good to exceLleni hedlth (0). Actiury limitabons were ese$ed by 6king wbedEr the child wos limitedin my activities becaue of o iDpaimen! orhealth prcblen ( 1 :limited, O= not limiled)ithe sme question ws dked tor school limitatioB. A total of 3.2q0 of children were in fdrlpoor health, 6.90/0 had activiiy linita[ons, an.t8.30,b bad school linitatioN.
Clrori. .ordirr'm. We lb$ed on the mostcomon clrcnic ilnes in chndhood (a!thma)
and lhe leadjng case of death ams theliJespm (cardiovdold conditions). Rerpondents were 6ked whether the cbjld had myconditions fton a Ist ol chmnic onditionsrmdonly chmn from 6 lists. The lists edesffibed in Msey ei a1.30 Respondenis inhe seLuted Bpimto,f conditio$ gto\tp werc6ked whether the chnd had asthma. Respon-dents in the selecred cimhtory conditio$grup were sked whether the cnnd had anycardiovasuld or cirdnabry chsnic condi-tioB (including heart dise6e, high bloodpresru.e, and cer€brcvdculd dise6e). Re-sponses w€re coded 6 presnt (1) or absent(0) for dthlna and for any circ'iai,ory condi-tion. Be@se each Ist @ only adminideredto one sixih of ihe suplq sepmte chrcnicenditions weighis were sed. A tobl of 710/0of children had 6tbba, ud 2.30/0 had a cir-
Aczrr dndto$ We foced on the lead-ing clildhood cause of deat$ ed yem ofproductive lite lost (inluies), ed the n6tcomnon tpe of aote illnes in chndhood(respihtory @nditions). Rspondenls wtr4ked whether ihe cbild had m injury thatlimited acb4ty or res'nted in nedical atten-tion in ihe pFioN 2 weelc. The salne ques
tion {as asked for acuie respiniory ilnses(including colds, fll! acute bronchiiis, pneu'nonia). Respotres tor all corditioE wer€coded 6 pBent (1) or absent (0)- A tolal of1.40/0 of cbildren had & injury, dd 5.o0/ohad o @te respiratory illrN in the previ-
Analyses were condu.red with Siata/SEveFion 8.2 softsee (Stata Corp, CollegeStation, Tex), with weighted data to adjsl for$Fey design etrects be@use of clEteredsanpling and oveBmpling of certain groutr's.
Logistic regression dalyses wen conductedto predict cllchotomoB health outcones fronSES ud rue vonables. An inier.ction temw @ated by nultiplying SES (vem ofParental edu@tion) by racial gmup (3 itdi@torvdiables for Blek, Hispenics. dd Asisl
With this coding, Wdtes seNed s ihereference group. To ieri asrociatiom of healthwiih education and mcq health outcomes
Aprl2006. vo 96, No.4 Ame caniou arofPubrc Hearb
I
che, etar Peer Rdrewed Fesearch and Phctice 703

were tust reg€ssed onto paJenhl educationmd mce variables sinultlneously. Second, iotest whether pNnlal education-health rela-tions varied by race, healtn outcones werereg€$ed onto education, race, md i})e inler-action tem for edu@hon @d Ece rmultoneously. &e @d gender were included s cGveiaies ir all analyses. Faies for figures werecalcr at€d wilh the prediciion equation bom
the estinated logisdc resre$ion (presence/
absence of iun€ss regrsed on race ed edu-catioD). Rates @ desdibed a pa./d.e foroutcomes thai m chrcDic/stable Generalbealth, linitations, clftnic conditions), dds im1d.e for outcornes that occu€d in theprevioN 2 weeks (injwy, rerpimbory illnecs).
RESULTS
Tdble 1 presents the coefficients ilom thelogistic regresio! ualyses. For fair/poo.healtn, the significant efiect of education indi.cat€s that children ftom less educaied fomilies
were nore lilely to be in favpoor heslth.Sjgnificmi etrecls of Iace were seen lorBlacks, Hispoi6, ud Asies, such that chil'dren Fon each minonry gtuup werc norelikely to be rared in fai./poor health thuwere white children. The education'by raceinteraction etrect was not signific$t forBlack compared with Whites, indicating thatboin White ud Black childr€n had similareduedon gndients for fair/poor health. Theedu€tion-by'm@ intedction efrect M signifimt lor Hisp&i6 compared wiih Whites(P<.001 ) @d for Asi€is conpored with\44i!€s (ai ihe P=.08 level), indiBdng thateducation gmdieni5 for Hi$anics and Asia$were less steep for fab/poor he€lth than ftey
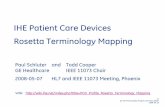
With .espe.t to activit dd school limita-tions. children Fom ls edu@ied fmiliawere nore likely to have both a.tiury edschool linitations. Blacl6 were more likelyl,o have aciiviry ed schooL limitatioB tnewere Whites, wheres Hjspei6 dd Asidswere less likely to heve adivity ud schoollimitations than were \ryhites.ln addition.thee were significdt intehction efie.rr oledu@tion by Ece lor both activity @d schoollimiiations when co pa.nng Hispoics andAsim to Whiles, but not when conparingBlacks to \\'hites. This iniemction, depicted in
RTSTARCH AND PNACTICE
TABLE l-Logbtlc RegesslonanalysasTostlng Elfech of Parental Educ.tlonand Sace on Chlldrcnb Healthr UsNrtlonalHeal$ Intonlow Su ey, 1994
tulrl|oor hs||n
tdrdton -0.15 0.01
8la!|{ 0.70 0.08Hhpan c 0.30 0,10Asian 0.41 0.13
B act 0.04 0.03
Hispai c 0.11 0,03
,tsian 0.06 0,03
-0.07 0.01
<.001
<,001
,08
<.001
<.001
<,001
<,001
0.22 <.001
0.25 0.06,0.31 0.m-1.20 0.20
-0.01 0.024.12 0,020.15 0.05
0.06 0.01
0.20
0 3 5-113
-0 01 0.03
Hispai c 012 0.02 <,001
Ashi 014 0.06 <.05
Chmnlc @dltlot: 6thm
0.15 N
0.18 m
0 1 8-01?
003
-0 010,010.13
7o4 Research and PEctice Peer Rev*ed Che, el a/. Ameican Jouna or Pub ic H$Lth
TASLE l-Cort rued
Bl6ck
0.01 0.03
-0.12 0.28 m-0.06 0.32 N
1.14 1.01 N
-0.12
0.230.13
0.03
-0,03
0.120.07
0.08 m0.08 <.01
0.05 < 05
002 N
0.03 < 0010.04 13
-0,46 0.16 <01-0.75 0.16 .10-1.52 0.60 < 05
0.01 0.04 N
0.09 0.12 ns
0.04 0.01 <.001
0.00 0.08 m
0.07 0.14 N
rvole td!6ti0i-rsB0lpaEit de6toi N-iolsignif.anl Reldtsme goup ior 6 ucd coeficients is!Urlt6. Beal[r Nt@m: 0 - no pDblem, 1 = prcsemeolhe€thprubl€m.Reglssioncoeflicie siorEceaidedtdtioi ellect lh* 2 wd6bl6 steEdsinultareousli w lh age aid gends 6 cda'iat6,coefrcienls ior ure inlenction t€ms @fl&r lnleractionefli4ls vhei frtered sinullamously with be aidedlmtion, ard ri r age aid gfrder as miat6.
Figw i, revealed that the education gndient6 sinild for Blacks md Whites but resteeper for \ryhites lhm for Hisparic odAsim (sI P! were <.05). In folow-up ealy-ses with Blacls s the .eterence group, wefoud a simild pattem of a sieeper educat'ongradient for Blacks than for Hisporic, mdAsiais (P! wer€ <.01).

.s6
.EE
e
i
E
.E
4.25
o.20
0.15
0.10
0.05
RISTARCH AIID PRACIICf
overal heall\, actiuly 6nd scboDl liDitatioB,
md chrcnic circ!]atory conditio.s (in nris
cde, for Blacls). In co.b'asl tlD educationgEdienl e6 often noi present among His_panic md Asiar chn.Len (e.8 , activiry linitalions), od in some cdes wd rele6ed {e g ,acute respintory illne$es).
The outcornes drat we measued for Hie
puic md Asid childrcn were similar to eacb
other but dilTercnt fiom \\hite dd Black
children, which suggests tbat the different gn_
dients acrc$ Ecial groups tuay be becaN of
sodal fld cllturol vdlues that varlr by giouP
For cadple, both Hispanic dd Asie cL
tures hale extedve close social networks
dd an interdepend€nt cu]hres (e g, valuing
and thinkng in tems ol lhe group rdlher
thd the individual) '-r5 This could result in
Hispoic od Asid families shmng heallh
beliefs sd practicing h€alth behavioB a(osSES groups, t€ddlg to a dininished efl€c1 ol
lo\r pent6l educabon $ithin th€se glouPs
Allemaiively, €duation gndients may be
aHec!€d by irnmigration Pattems Hispanic
dd Asian drildren may be more lil<ely to
come filn irMig@t fmilies th8 m l\hite
or Black cbndren If bue, the presedr studysuggests 0rat the healtby imigrmt hlPoi\e_
sis also hd irnplicahotr for education rela
notr with heolth. That is, it is not just lhat D
migmnt groups are on a!€rage healihieri
ratie., ilMigant groups nay slso be less
susceptible to fie eJtects ot low €du.ationThese patlems have impon@t ihphca_
tions. Fi6t, it $ggests that low parental edu_
cation does not destine children to poor
healthi rar\er, because Hispoic and Asian
ohndnn who de low in pdental educahon
maintain healthy ouicones, ihere rnay be
lactoE tbat €n bufier rhe idpact ot lo\! edu_
cahon on.hild health, such s the role of so_
.ial netwo.l's. Better udebla.ding ot dreselacrob may sllow us to inleNene with oiher
low SES children io imprcve healih out
cones edly in lite. Second, in iems oles_
iabhshjng public healih Pnoritres, it suggests
Lbai effor$ to elininate socioecononichealth dispdilies may be most efiecnvethrough targeting specific Populations, such
6 $rhite and Black childrenO!. lndings m consisient wiih Previos
chnd health researth. For exdnple, descnp
lile figures suggest laiger gndjenls lbr low
1 2
For chronic conditions, there were no
significant effects ot educabon or nce on
slhma. For chrcnic circulatory conditions.there s6 an irteraction effect ot educationby ra@ Ibr HispDiG dd Asios compared
with Wliies, but not ibr Blacl6 compartd
ivirh Wl tes. This interaction effecl depicted
in Figure 2, revealed that Blacks and \\hites
had simild edu@tion gm.Ienls, bui lhal
\\hiies had significduy ditrerenl educationgmdienls th@ Hispdics sd Asios (rt
{ere < 05) \{ben Blacks w€re lsed s the
reference group, we fosd a sjmild pattem
of a steeper negatNe educaion gndient tor
Black compded w1L\ ttispanics ild Asians
lor acuie childhood .ondidons, Black and
Asians ivere Ie$ likely to repot injuries Lh@irere \\hii€s. No efrects of education or inier'
action effects were found. For acule resPiF
tory illne$, Blacks tlere less likely io have a
r€spintory illn€ss ihm were Whites. Children
{iom more educated lemilies were nore likely
Yea6 of Pa rental Ed ucdtion
to hale a respiralory nhess ln addition, a s'g
nj{icdt education-by-mce intemction efiect
ws found shen HisPdi6 Nere comPdedwith $tiies. This eflec! depicicd ir Figue 3,
revealed tbai Hispani6 had steepe. po$lve
gradients th@ did $hil€s (P<.001) $hen
Blacks were used as lhe retbrcnce gro'rp ive
foDd a simile patlem of sleeper positive ed_
ucation gFdienir for Hispdic conpmdwith Blacks (P<.001) and for Asi@s com_
pmd with Bla.ks (at the P=.06 level)
DlscussloN
Our reslrtts illust?te that nce and SES ef
fecls on child bealdr de best udeNtood n
conced, rai,\o ihu sepmtely. That is, al
though pdcntal edudtion ws relate.l t
child healdl L\ese difierences were actuanv
appdcnl oD\, dong certtr Ecrar grcups'lhe
baditionel relation of fewer yeds oi pa
rntal education wilh poorer h$lth emergcd
dong !\hitc dd Black child.en in t€ds of
rvore The ed(alioi iewdslgnircmtamoryWhireadBaclchildrei{Ps$tre<001)brlmtlolHispaicad,slai
FIGURE l-Paent.l edocallon x 6cs loteEctlon tor actlvlv llntafons.
Apr !2006 , Vo r96 . No . 4Fesed(h and Prad(e I 7o5

ntstAficl| Ailt PRAcItct ]
0,10
FIGURE 2-Parcntal educatlon x race Interactlon for chlorlc clrculaton condltons.
. - - + -
6 9 1 2
Year5 of Parental Education
]l'ore. The edrdrifl rine was s gdlimol aid nggarive anong 8ra.k chirden (P<.05) blt sigdicait md psitiE amoigHisDmic dd As ai .hirdrcn (Ps serc <.05).
respimtory illnesses. It is pNible thai moreeducat€d Hnpmic dd Asian parents arenore knowledgeable aboui different b,pesof respiniory ilneses (e.9, pneuDoni4brcnclitis) and thw, identiry then nore f.e-quendy. lt G also possible that hidersEsHispeic dd Asid fmilies have greater ac-cess to health careT that nakes them morelikely to tale then d d io ihe doctor foraoie respiEiory illnesses.
LimitatioB to the present shdy includedhaving no direct mesm of immig@t sta-tus or ac@ltuEtion. Th6, we do nol knowthe nMbers ol imig.ants within nciayethnic grcups ud cmnot directly testwhether ilmigrmt siahrs, years since immi,gntion, or accdtumiion explains the studylmdings. Further reseach is also needed totest.iilTerenes in health monS inmigrutswho de fi6t generation ve6us second or
Second, tuiure shrdies ihai measure avariety of behaviordl od social factors areneeded to detemine the chamcteristic thatbufter lowSES Hispmic md Add chiklrenfrofr poor health. Lat, the present study included only 1 me6s@ of SES, pdental edu-@tion. This indi@tor is quite stable overtime ud ihus may desdibe longerlasting ef'fecls ot pdntal SES or child health. Parcn-tal educadon nay suggest pathways relatedto health knowledge; however, it does notiell us about the i,apact of other SES ch@c-,eristi6 such 6 finucial .esourcs.Stre.gths of our study, however; inchdetbe 'rse of a national prcbab ity smpleweighted appropnately for clusiered san-piing ud ovenmplng of specific groups,allowing s to doment SES md ncehealth disp{ities acros US cbildren.
Undesbndi.g.hildhood health dispditisis cdtical to inprcving ADerica s h<h. Theavemg€'age cn d in ou smple (9 yea$ old)who comes from a lowSES fmily is esti-mated to have 6 yem' Ies life expectanct,ihm a high-SES child.{{ Ou $ndings dem-oBirdte that pdental edu@tion dd childhealth gradients e sbongest mong \ir'htedd Black chnd.en fld wealer or reveFedmong Hispmic dd Asid chndren. Design'ing tutuft interventions that ircorporate theprciective tactors of Iow-SES Hispuic ddAsiu chndren nay help improve the health
0.15
E
aj
e
3IP
.E
0,05
birilweighi &d intant mortality anong Blackmd Vvhiie children ihe mong His?dic orAsim cnndren.7 Simild relatioE uongBlack and [rhiie children have als beentound with pental edu@tion dd child over-all health ud school-16 days.36 ln addition,White youths have lhe stongesi SES relaiionwiti smoking$ md oberity.3?33 ovenll thesepattEm support the notion of cr dhood SESdd heatth gEdienis, paniculdly mong
Ou dalyses showed no efiect of eitherparenlr.l education or Ece on slbna prevalence ral€s. One posrible expleatioD is the"hygiene hypolhesis,' the noiion tbat a de-cfdse in chncbood exposm to mimbesdd iifections day inrese the p€disposition to chrcnic alergic conditions $ch 6srlma.3c4r If children wiih higher sES mexpGed to thse nor€ hygienic environ'Dents edly in life, this may baluce outother enviromenial characteristis (e.g.,exposqre to toxirs) that de detrin€ntal for
nmy lowersEs children, resulting in no ed-ucation difierences fof osthna-
lvhiie chn.L€n werc nore lilely to experi'ence u injury rhu were ninority chrrdren.Wlite chndren m nore likely to pdrticipdtein s?o.ts ihd m Hispuic or Asian orildren,which may aaoDt for sone ofihe mcisl dif-ference, in injuder.a'� In conrast, no educa-iion efrects were toDd for iDjuies. Althoughthis is inconsistent with pattem found anongyouger children,6 high'SES adols@nrs havebeen found to p&ticipale in Dore activity-onented lsoB md sporir ielm rhm low-SES adolescents, pHmably be@6e ofcosts.43 ffhigheFsEs older chndren ar€ exposed to Dore sih8tioN witl lhe poienti€l forinjury, lhis may resltli in no cled eduationdifferences in injuiB 8rrIN al of o\n.lhood.
Ou shrdy also found thal in some cses,Hispdic dd Asid chndren exhibited a re-verse education gradieni. Specifically, Hispeic and Asian children with nore edu-@ted pmnts had higber mt€s of acute
I
706 I Research and Practice Peer Reviered I Che, er a,. A0rr 2006, vor 96. No.4

E
-
=
;
E
0,03-
0.02-
1 2 1 5
Years of Parental Ed ucation
tlote.Ilre ed!Gl on liiese mtsgiif6rtamoigwhilead Bel.hildrei but vas slgnif'ait lor HispaicadAsiai
RESTARCII AI'III PRACT!CE
t ----*n*' , ,7-...
/
Asians / / Eacks
3. 5t rficu B nihy AW. lvit !W, Bohetuon lScial ds gEdienls m hcdth during adolescence
I Epid!tuot cannuiq Hulh 2oo2t56:354 361
L Nc\vache.k I'W PovertJ dd.hildhood chton'c
illnes. ,4rt &dtair dlo/6. t|al l994il43
lO Egbuonu I-. Sbrlield R Chnd he€ldr md sod
sbtu P!ri,r'd 1932;69:550 557
1l Srdljeld B Roberlson J, Rilet AW Social dN
gndienfs md hea$ in childhoon ,4 nbtloto\t P.didt
2AA2t2:234 21tj
12 Sbrnoh B Child helM 6e ud social facton
loverty, cls, n.c. all N v rl.,l ,\td 19agi65r
ti shenan \ PaNn! Mai6: me co! ol chitd
,%r"1, t ,l,nsn.a $bshinglon DC, Childrn s Derensc
14. Sbrfield B Shapim S, $Iersj, el al Race fan'itv
in.one, md low birihs€igh! 'lnl tpidenidi l99li
15. Scnoendorr KC. Hogue ClR, Kdmo JC RoFlev D
Nlonahg_ dong lnfmb ot b1a.k s conpaed wi$
urnre colsnHdudred pmn6 x E d/ It d rss2
16. llogLe CJR. Harynves NA Cl6 n... dd inrsi
morGlity in rhe Unibd stntes ,]n / ,r'!rhd telt
17 Nonigomery LE, Kely JL, P.pPB C lhe cfl(ls
or povefy. E.o. aDd fdily sb-trcm on US childEn s
h.alth: dah from $cNtts.1s73 thrcush 1930 md
1939 lnrugh 1991.,4', /Ab/rt?,lili 1996:46
r3 Flofts C. BaL,chmr H. Fsidci'r Al Nglvcn UDt'$e
inpad of eth'riciiy, f.m'ly indne md parend
cdudtion on.hild'usheatn dduseolhealln $
lies An I PtIhU. H.olth l99C;89 1066 1071
19. Winlddby NlA, Robinson TN. sundqujn i(Ecm.. HC Edtic vdiatioD in canliou{uld discae
mk fadoE mong chndftn aDd yoL'ng ad'nb [ndings
iiod &c ftinl Narional Hea$ md Nubidon Erllma
iionsuney 1933 1994 /.4,111 1999;231 1006 1013
20. Entuhic R?pon aJ the Ptundd $I6hinsroi Dc:
US Covcmdenl Prinri.g Oh.ei 1993
21. lvilim DR. Race. sodoeconomic sianE ud
healrh Lhe added efecb of Esd dd dGaininanon
,4n, N |'1ft1 Sd: 1999i396 173-183
22 lvillians DR. Raosl/cdni. \uiatios in \voneD!
hc€lrh: ilre loci.l enb.ddedncs ol healdr lnl nrbl''
Hskh.20l2:92 5AA 597
23 Kcsler RC Ncishboc HW A new peEpe'Nc on
ine mhdonshipd mo'u n e, so.ial cl6s sd psf.n}
log,cal disb€$ /ral, So'a.td' r936i27:107 115
24. PeliigPw TF Race dd cla$ inlhe l9a0s: u
inrc.dclive vicu Daed'16 l93l J10:233-255
25 Lcvin S. Sinclair S. Vcniegs RC. Tatlor PL Per
.e,vcd discnmination in $e odcn of nulbple grcu!
memberships. A!.rol Scl 20o2rl3:557-560
26 Fe@o KF, Fdmcr MNl Double jeoParlv to
hesi$ hypo$csis for Alncm Amcri
ditique J ]]ealt So. aet u 1996;37:27-'13
27 Hmmer RA, RogoN RC Nm CB lrdere lB
Ra.e/ethnicity. nolivity, ud US adult nort liq' 50'
SaO 1999 i30136 153
neune r-p-enta "Uucatron x mErnteracto tor acute esplhtorv illnesses'
of all children dd mdimize t]le h€allhy
and productive yeds ol adults acrcss lhe
Abonl $e luthonnh Ad k unh ttu De?atudt ol Plt'rholag Unit
nB uJ SnnJt Cthtnhto tan\tuta AndrtuD llodltL
dI tln Dqu tnat nl Pohrdl Sdtrtr W6hiagtrn Drl
tu6'tu 5r ,o,n i\td (dfl ,'1 ilrad/'er is e'i/i rt. l].
podnat 4 kvhiuh!, Unir6it! oJ f|]nshtgh s.INt tl
Req$h lar repnnb shaut.l h. *tt b Edith cher
un;r, iht ot Bn sh cahnbta D.tttnat al Plr.LatoE!
2t36 W& t\loll \:oftaun BC, Cana.t, V61 tZ1 tenail:
misa tle td adePkl fehtuary 18 2405
ConbibutorsE chcr ibatcd uF sbdy. plmed di|a mslvses md
srcr rhc adcle. A.D. Nldin oiductcd sblrsiical
ualvses ard skbd wirh daE mteQrerabon K A
Ntarilr$ .onbibucd io sd,dy concepu$lizarion dtu
inknr.bdon. md vrihng or de ortde
AchnoftdEnentslhEshrdr-NA tundRLbv Lhc Nduon:l lnn tsifChJJ
Hcal.h d H0nd Developnent (gdl HD13652)
l|uman Parlicipant ft olectionThi ftdy \v6.ppro!.d by d( ftsearch elhrs bodd
at the UtrivcNity or Brirish Colunbii. VscDuvei
I Hu h! ttaPl. 20t0: Unttdtduliae ona InPtoinE
telt \Idhinsion Dc: Us DePo'
2 Adler NE Boyc. T Chesney NlA d al Socioec
nomr sbtu Dd hcalth: llrc .h.llengc of ine gndent
,1u Ps!.lol 199.1r'1s,15-21
3 Adler NE. Boycc WT Chcsnev MA. Fdlknd S
SJnc SL So.joconodr incq@libcs in healrh no e6v
sollibon.lrl,tt.l 1s93i269 3140 3145
I Namor NjC. ShPlcy Ni, Ros C lncqudlibcs n
dcarh specific cxplanations ol a Sen enl Patlem?,.,.er 193{i1 1003 1006
5 *lllims DR. collins C US socioe.onomicdd
Ecitsl drfercnces in hcal$: paftms and exPrdnatons
,lrnnaSodrl 1995i2l 349 336
rj Ch.n t. i\ldi rvs KA, Bov.e \\ l: Socioemnonr
difl.En.es m childPns he.|in: hoN
EratiDnshiF .hd!e *idr age? ,arthol Btu 2OO2:r2t)
7 lbnuk E Nora. D, Hck K Reuben C. ti'lner K
s{no{atunt 5tu16 otd Ilearn ChdnbMh ii@tth
L,nn.dsrd&s /9'l3 llyaltnille Nid: Nabomlcenter
for lleal& Statisd.-!, 1993

RtStARCII AIII) PRACTICE
23 Sinsh CK Yu SM. AdreEe pieg.scy ouloE6,
difieEnces beh\€en US md foEign.bom uone. in
dajor US mial dd eurnic gloup6. An I tublic Hfulth
29 li€ulnm J5. Cmper RS, Mccee DL Soooece.omic d.tu md heallh in block md sbit6 ihe ptub
len olridual @nroundiq md the Biljen.J orE.cE pilnib lag! 19 97 \A:6 2 I - 62 A
30 Mscy Ir. Oveflies ol lnc Narion.l lledlh lnteF
vie{ SunrJ dd ils s@plc desig vitol H@kn Sd 2
31. Knegsr N $Iillians DR, N{os NE Medsuring$cisl dN in US public hcalth He.rcn:.oncepb,netnodolqrcq md grdelins nnntraArdt A.cM
32. wmkleby Ii{^. Jdtulis DE F@k E, Fotum sP
Socioe.ononic shtu dd healin: how eliuation, in'
come. od ddpabon conbibule lo trk lactoE for
cadiovff.dd dne6e ,4nl,qrrii. /tdlir 1992:821
33 Vdin C, Mtrin BV ,R6dr' t{.r' tapd'i. ,'tptrldio6 Nesbnry Park. Calil: Sagei l99l
34 NIdk6 R, Kbyma S CL hre and $e self im'pliations for.osnition, enobon, md moti€tion. Al.t l Ed. 199lSA:224 253.
35. Hejre Sl. Sclr s c'ihlrn prcd
.l lj6t Aiiu dd Nonh AnErico selves /,rbr 2001 :
36. Nt.Cauhey PJ, Sbrfield B. Oild h@Ih md rhes.ial enviF.nent or {hite od blac} chndFn 5d 5a
37 C.nlon-l-cen P. Adair t5, nrPkin BM The dabotrhip oI ei]lniciiy, socioeconomic lac!06, sd oveFscighr in us adolesc.nb. ora n6 2o03:rr:r2r-r29.
38 Km SYS. Ob@@ek E, Barion BA. et al Ra.e,
so.ioeonomic ststu, dd ob6r1y in I lo lo.ycd.old
enk $e NHLBI Cnn1n ud Hoallh Study. Ar, !1i'
39. shchm DP Hay lcveq hysiene. and householdsize rMl 193S1299:1250 1260
40. Sh.iu DP Fnny size. inl4iion fld aioPy, LhelNt decadc ol $e 'h$iene hworhc* ' tud 2000i
.ll. Bdn'Fdnduder C, Riedler J, Heu U. etal E.vi'
rc.bentd exposm b endoloxin ud irs {lation l,o6Lhb. in school.age .hildftn. NEigllr\|d 2002!
42 videon TM. $ho plays md who benefib: gendcr,iileK.holstic aihleliG, Md acadcmic oubm6 S@blP6sp d. 2A A 2,43 :415 - 444.
.13. SollG JF, Zdldian JM, Hovel MF Hofsiener CnEtlnic, e.io{ononic, dd ser difreren@s in physi..l
eriiry anoDg adoltr@nrs. / clt Eradi.l 1996149
l.l Kubzdsky LD, tuic8o N. (a\hchj I. Rocrhill B,Skel CI( Berhnm I-F Uiited Srote social inequdrtxmd Lhe burden or poor health In: E6 I Whehcad UDdcrichsen F. Bhu,ya A lvirth Nl. eds A .hgng tn'.qzin6 t' tali, Nd York. NY: Oxlord Uni€Eity
published in 1991, provides information to assist in anticipating the potentialfordisease or injurrrecognizing occupational diseases and inju ries' evaluating rele'vantdata,anddesigningand implementing control measures
Preventing occupational Disease and lniury2nd EditionBany 5. Levy, Grcqaty B.wognet, Kathleen M. Ren, lones L Weeks,
F ach yedr in the united States.5.000 to 6,000 worLFrs die
l- from acute rraumatic occupalional Injurie5.simildrly thel-causes oland methods to prevent many occu pational
diseases are wellknown.Work can be hazadous!However, more im porta ntly, most hazads can beantici
pated,and prevented.This book,updated frcm itsfirstedition
rsBN 0-37553'043-5sottcover . 2004 521.95 APHA M€mbe6'531.00 Nonmembeu
ORDERTODAY!Aneri.an Publi. He.llh arro.iarionPubl l<.tion 5ales
703 I Res€adh and P.acuce Peer Reie@d che, €i6,.
-