Ultrasound-Guided Foam Sclerotherapy for Treating Incompetent Great Saphenous Veins—Results of...
7
GENERAL ARTICLE Ultrasound-Guided Foam Sclerotherapy for Treating Incompetent Great Saphenous Veins—Results of 5 Years of Analysis and Morphologic Evolvement Study CHIEN-HSUN CHEN, MD,* † CHENG-SHENG CHIU, MD,* † AND CHIH-HSUN YANG, MD* † BACKGROUND Varicose veins of the lower leg is a common disease and is associated with long-term morbidity. It has been treated using high ligation with stripping and endovenous laser surgery of the great saphenous vein (GSV). OBJECTIVES To investigate the clinical outcomes of GSV insufficiency after ultrasound-guided foam sclerotherapy (UGFS) using 3% sodium tetradecyl sulfate (STS). METHODS Between 2005 and 2009, patients with symptomatic varicose veins secondary to GSV insuffi- ciency were enrolled; 3% STS foam was injected into the GSV under ultrasound visualization. Ultrasound examinations and clinical follow-up were performed at 3- to 6-month intervals. Follow-up visits continued through April 2011. RESULTS Two hundred 88 limbs of 233 patients were enrolled. The mean follow-up interval was 37.8 months. Occlusion was achieved for 89.6% of the incompetent veins in two sessions of UGFS. The mean number of therapy sessions per leg was 1.53. The internal diameters of the treated veins reduced to 66.9% 3 months and 32.7% at 12 months. CONCLUSIONS UGFS is effective in sealing incompetent GSV segments. It is a minimally invasive proce- dure and can be redone several times in cases of recurrence. UGFS is simpler and less painful than strip- ping surgery and endovenous laser treatment. The authors have indicated no significant interest with commercial supporters. F or almost 100 years, varicose veins have been treated using sclerosing solutions. An ideal sclerosing solution should irreversibly destroy the endothelial cell layer and subsequently cause vein fibrosis without damage to the adjacent normal vessels and tissue. Various components of liquids such as absolute alcohol, hypertonic saline, polyio- dinated iodine, and glycerin have been used as scle- rosants for injection. 1 For most cases, the use of these sclerosants fails to yield good results for occlusion of incompetent, dilated great saphenous veins (GSV) because, after injection, the sclerosant is diluted with the blood, and the concentration of the sclerosant becomes too low to induce irrevers- ible vascular endothelial injury on the entire vein segment. Detergent sclerosing solution (polidocanol [POL] and sodium tetradecyl sulfate [STS]) can be converted into foam by vigorous mixing with air. The foam microbubbles come in homogeneous contact with the vein endothelium at an undiluted concentration, so the foam sclerosant causes more damage to the vessels than a liquid sclerosant does. Foam sclerotherapy is mostly performed on blue reticular veins, perforator veins, and branches of the saphenous vein. 2–4 With respect to foam sclero- therapy for incompetent GSV main trunks, the number of patients studied has been small and the follow-up short. 5–7 The aim of this study was to *Department of Dermatology, Chang Gung Memorial Hospital, Taipei, Taiwan; † Chang Gung University College of Medicine, Tao-Yuan, Taiwan © 2012 by the American Society for Dermatologic Surgery, Inc. Published by Wiley Periodicals, Inc. ISSN: 1076-0512 Dermatol Surg 2012;1–7 DOI: 10.1111/j.1524-4725.2012.02408.x 1
-
Upload
chien-hsun-chen -
Category
Documents
-
view
212 -
download
0
Transcript of Ultrasound-Guided Foam Sclerotherapy for Treating Incompetent Great Saphenous Veins—Results of...

GENERAL ARTICLE
Ultrasound-Guided Foam Sclerotherapy for TreatingIncompetent Great Saphenous Veins—Results of 5 Years ofAnalysis and Morphologic Evolvement Study
CHIEN-HSUN CHEN, MD,*† CHENG-SHENG CHIU, MD,*† AND CHIH-HSUN YANG, MD*†
BACKGROUND Varicose veins of the lower leg is a common disease and is associated with long-termmorbidity. It has been treated using high ligation with stripping and endovenous laser surgery of the greatsaphenous vein (GSV).
OBJECTIVES To investigate the clinical outcomes of GSV insufficiency after ultrasound-guided foamsclerotherapy (UGFS) using 3% sodium tetradecyl sulfate (STS).
METHODS Between 2005 and 2009, patients with symptomatic varicose veins secondary to GSV insuffi-ciency were enrolled; 3% STS foam was injected into the GSV under ultrasound visualization. Ultrasoundexaminations and clinical follow-up were performed at 3- to 6-month intervals. Follow-up visits continuedthrough April 2011.
RESULTS Two hundred 88 limbs of 233 patients were enrolled. The mean follow-up interval was37.8 months. Occlusion was achieved for 89.6% of the incompetent veins in two sessions of UGFS. Themean number of therapy sessions per leg was 1.53. The internal diameters of the treated veins reduced to66.9% 3 months and 32.7% at 12 months.
CONCLUSIONS UGFS is effective in sealing incompetent GSV segments. It is a minimally invasive proce-dure and can be redone several times in cases of recurrence. UGFS is simpler and less painful than strip-ping surgery and endovenous laser treatment.
The authors have indicated no significant interest with commercial supporters.
For almost 100 years, varicose veins have been
treated using sclerosing solutions. An ideal
sclerosing solution should irreversibly destroy the
endothelial cell layer and subsequently cause vein
fibrosis without damage to the adjacent normal
vessels and tissue. Various components of liquids
such as absolute alcohol, hypertonic saline, polyio-
dinated iodine, and glycerin have been used as scle-
rosants for injection.1 For most cases, the use of
these sclerosants fails to yield good results for
occlusion of incompetent, dilated great saphenous
veins (GSV) because, after injection, the sclerosant
is diluted with the blood, and the concentration of
the sclerosant becomes too low to induce irrevers-
ible vascular endothelial injury on the entire vein
segment. Detergent sclerosing solution (polidocanol
[POL] and sodium tetradecyl sulfate [STS]) can be
converted into foam by vigorous mixing with air.
The foam microbubbles come in homogeneous
contact with the vein endothelium at an undiluted
concentration, so the foam sclerosant causes more
damage to the vessels than a liquid sclerosant does.
Foam sclerotherapy is mostly performed on blue
reticular veins, perforator veins, and branches of
the saphenous vein.2–4 With respect to foam sclero-
therapy for incompetent GSV main trunks, the
number of patients studied has been small and the
follow-up short.5–7 The aim of this study was to
*Department of Dermatology, Chang Gung Memorial Hospital, Taipei, Taiwan; †Chang Gung University College ofMedicine, Tao-Yuan, Taiwan
© 2012 by the American Society for Dermatologic Surgery, Inc. � Published by Wiley Periodicals, Inc. �ISSN: 1076-0512 � Dermatol Surg 2012;1–7 � DOI: 10.1111/j.1524-4725.2012.02408.x
1

evaluate the efficacy and safety of ultrasound-
guided foam sclerotherapy (UGFS) for treating
incompetent trunks of the GSV.
Materials and Methods
Over a 5-year period, from August 2005 through
October 2009, patients with symptomatic varicose
veins secondary to GSV insufficiency (CEAP classi-
fication C3–6, EpAsPr) were enrolled. GSV insuffi-
ciency, defined as duration of reflux longer than
0.5 s starting from the saphenofemoral junction
(SFJ), was detected using duplex ultrasound.
Patients who had previously undergone sclerotherapy
or vascular surgery of the lower extremities were
excluded. Follow-up visits continued through April
2011.
Sclerosing foam was generated using the Tessari
technique.8 One part 3% STS (Fibrovein, STD
Pharmaceutical, Hereford, UK) and four parts air
were mixed to produce the sclerosing foam. We
used two latex-free disposable plastic 10-mL
syringes; one syringe contained 2 mL of 3% STS
in the liquid form, and the other contained 8 mL
of air. The outlets of the syringes were connected
using a three-way stopcock. The contents of both
syringes were pumped backward and forward,
causing a turbulent flow that generated foam.
Optimal foam was produced after 20 passages.
For performing injections, patients were placed in
the supine position with the treated leg slightly
elevated and rotated outward. A 25-g, 1.5″ needle
was inserted at midthigh level. The needle was
advanced under ultrasound visualization. When
the needle tip was confirmed to be located within
the GSV, the sclerosing foam was injected.
Spreading of the hyperechoic foam column to the
SFJ and vasospasm could be observed was consid-
ered to be the treatment endpoint. As the foam
spread to the SFJ, an assistant immediately com-
pressed the SFJ to prevent the foam from flowing
into the deep venous system. Patients were
instructed to lie in supine position and compress
the SFJ using a 5-pound sand bag for 10 min
after receiving the injection to prevent dislocation
of the foam column into the common iliac vein.
A single injection in the thigh was usually suffi-
cient. To avoid unwanted foam passage into the
perforator causing femoral vein damage, ultra-
sound examination was carefully performed to
detect any perforator vein connected to the femo-
ral vein at midthigh. If one was found, the
midthigh perforator vein was compressed with a
bandage followed by two injections at the proxi-
mal and the distal thigh of the GSV. As for severe
bulging and tortuous extrafascial varicose veins
below the knee, an additional three injections of
1.5% STS were performed using a 27-gauge nee-
dle. After sclerotherapy, all treated legs were
placed in class II, 30- to 40-mmHg graduated
compression hosiery for at least 1 week. All
patients were instructed to walk at a moderate
pace immediately after therapy.
At the first visit, 1 week later, patients were asked
about side effects, including visual disturbances,
headaches, chest tightness, and leg swelling.
Duplex ultrasound was performed to look for deep
vein thrombosis (DVT). Patients were followed up
at 1 weeks, 2 weeks, 1 months, 3 months,
6 months, and thereafter every 6 months. Repeated
duplex ultrasound examination was performed at
each follow-up visit using the same protocol to
determine the changes and patency of the treated
GSV with the patient standing. The internal diame-
ter of the vein was measured at two sites: 5 cm
below the SFJ and at midthigh level. The treatment
was considered successful if absence of reflux or
reflux flow of <0.5 s for the entire treated segment
was observed during the follow-up ultrasound
examination. Patients received a second ultra-
sound-guided 3% STS foam injection if vein recan-
alization or persistent reflux of longer than 0.5 s
was observed.
Results
The therapy was performed for 288 limbs in 233
patients (165 women, 68 men); 156 left and 132
FOAM SCLEROTHERAPY FOR TREATING INCOMPETENT GSV
DERMATOLOGIC SURGERY2

right legs, including both legs in 55 patients, were
treated. The mean age of the patients was 60.1
(range 27–88). Mean follow-up time was
37.8 months from the first therapy session. The
average volume of 3% STS foam administered in
the first injection was 9.7 mL (range 6–16 mL).
Duplex ultrasound examination showed that 173
of the 288 (60.1%) legs were free of reflux after
one session of therapy. Of the remaining cases, 85
(29.5%) were free of reflux after the second session
of therapy and 24 (8.3%) after the third. The mean
time interval between the first and second session
was 3.2 months. Of the six (2.6%) limbs in which
the GSV was not occluded after three injections,
four had an initial vein diameter greater than
10.0 mm and two greater than 8.0 mm. The mean
number of treatment sessions required to treat a
leg for GSV insufficiency was 1.53. Follow-up ran-
ged from 18 to 68 months. The mean number of
treatment sessions needed was 1.47 (n = 19) for
patients with a follow-up period of longer than
5 years, 1.57 (n = 51) for 4 to 5 years, 1.61
(n = 70) for 3 to 4 years, 1.34 (n = 94) for 2 to
3 years, and 1.70 (n = 54) for 1.5 to 2 years
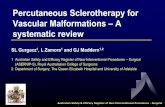
(Figure 1 and 2).
In 52 patients with 65 treated limbs, vein diameter
was precisely measured using duplex ultrasound
scanning at 1 weeks, 2 weeks, 1 months,
6 months, and 12 months. The mean pretreatment
vein diameter 5 cm below the SFJ was 7.57 mm.
The internal diameters of the treated veins were
unchanged at the first and second week after ther-
apy. Involution was gradual; the internal diameter
of the vein at midthigh level at 1, 3, 6, and
12 months was 79.3%, 66.9%, 44.8%, and 32.7%
68~60 monthsN=19
60~48 months N=51
48~36 months N=70
36~24 months N=94
24~18 months N=54
sessions 1.47 1.57 1.61 1.34 1.7
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
Sess
ions
of f
oam
scl
erot
hera
py
Figure 1. Treatment sessions needed for 3% sodium te-tradecyl sulfate ultrasound-guided foam sclerotherapyaccording to the follow-up time.
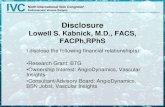
(A) (B) (C)
Figure 2. Clinical results seen with 3% sodium tetradecyl sulfate foam sclerotherapy (A) before treatment and (B) 3 weeksafter treatment. Superficial thrombophlebitis was observed in the calf on previous severe dilated varices. Removal ofcoagulum helps to reduce the tenderness and pigmentation. (C) There is marked improvement of a varicosity of thegreater saphenous vein 9 months after treatment.
CHEN ET AL
2012 3

smaller, respectively. The internal diameter of the
vein 5 cm below the SFJ at 1, 3, 6, and 12 months
was 88.7%, 50.2%, 37.5%, and 30.7% smaller,
respectively (Figure 3). The treated GSV were as
narrow as fibrotic cords (internal diameter,
<2.2 mm) approximately 12 months after therapy
(Figure 4).
Some patients developed thrombophlebitis over the
treated veins, mostly in large extrafascial varices
close to the skin in the calf. Early and repeated
evacuation of the trapped coagulum using a 18-G
needle under local anesthesia helped to relieve the
redness, tenderness, and subsequent overlying skin
hyperpigmentation. No cases of anaphylaxis, deep
vein thrombosis, intra-arterial injection, skin necro-
sis, visual disturbance, or other significant adverse
events were found.
Discussion
An ideal sclerosant would induce target vessel fibro-
sis without recanalization. Vascular fibrosis and
obliteration occur after irreversible destruction of
the endothelial and subendothelial cellular layers of
the treated vein segment, but obliteration of large
veins using a sclerosant is difficult. Foam sclerother-
apy has an advantage over liquid sclerotherapy that
involves the dilution of the sclerosant with blood in
that the injected foam sclerosant pushes the blood
backward, leading to little dilution of the drug.9,10
Furthermore, the spreading of the foam within the
0 1wk 2wk 1m 3m 6m 12m5 cm below SFJ 7.57 7.43 6.98 6.72 3.8 2.84 2.33mid-thigh 6.65 6.73 6.08 5.28 4.45 2.98 2.18012345678Vein diameter (mm)
Figure 3. Internal diameter of the vein measured 5 cmbelow the saphenofemoral junction and at midthigh level1 week, 2 weeks, 1 month, 3 months, 6 months, and12 months after foam sclerotherapy.
Figure 4. Duplex ultrasound scanning of the great saphenous vein 5 cm below the saphenofemoral junction (A) beforetreatment (B) 3 weeks after foam sclerotherapy. Perivascular hazy shadow was observed. The internal diameters of thetreated veins were unchanged. (C) Three months after treatment. The size of treated vein was decreased. (D) The treatedgreat saphenous veins were fibrosed 6 months after treatment.
FOAM SCLEROTHERAPY FOR TREATING INCOMPETENT GSV
DERMATOLOGIC SURGERY4

vessels and vasospasm after the injection can be
detected in real time by performing duplex ultra-
sound scanning because of the hyperechoic signal
of the foam. Hence, a foam sclerosant can be safely
introduced inside the GSV under direct visualiza-
tion. To limit endothelial injury to a controlled
area, patients were instructed to remain in a supine
position and compress their SFJ in the groin area
for 10 min after injection. The abnormally dilated
GSV segments were perfused with the sclerosant,
and the foam was prevented from entering the deep
venous system. Foam prepared according to the
Tessari technique has a half-life of approximately
90 s.11 Therefore, the procedure should be com-
pleted within 1 min, or the foam will separate into
two phases: liquid and air.
Various injection techniques and sclerosants have
been selected to treat varicose veins. Islamoglu
used high ligation plus 3% POL foam injection
from a catheter into the entire saphenous vein.12
Hamahata and colleagues used 1 to 2 mL of 3%
POL foam at midthigh and a second injection
3 cm above the knee.7 Myers and colleagues
injected 3 to 40 mL (median 5 mL) of 3% POL or
3% STS foam using a 1.5″ 25-G needle from a dis-
tal part of the limb.13 Bradbury and colleagues
used 18- to 22-G cannulae under local anesthesia
with each injection of small volume foam aliquots
(2 mL) down the trunk vein to minimize the deep
passage of foam sclerosant.14 We used a 25-G,
1.5″ needle to inject 3% STS foam at the midthigh
and let it flow proximally to the SFJ and distally to
the varicosity around knee. Five to 8 mL of foam
sclerosant can fill up the incompetent, dilated
saphenous trunk according to the vein diameter.15
Usually, a single injection in the thigh was suffi-
cient, although preoperative duplex ultrasound
examination was important because the perforator
vein may connect to the femoral vein at midthigh
(Hunterian perforator). In such cases, adequate
pressure should be applied over perforators, fol-
lowed by administration of two injections—one
each at the proximal and distal thigh of the GSV—
and the flow of the foam is carefully monitored
using ultrasound. This technique prevents
unwanted flow of the sclerosant down the perfora-
tors causing femoral vein occlusion, which has
been reported in balloon catheter–directed foam
sclerotherapy.16,17 Additional multiple small-dose
injections (1–2 mL) using a 27-G needle are per-
formed in the bulging and tortuous varicose vein
below the knee to minimize the spread of foam
into the deep venous system, because there are
many perforators on the calf. These strategies help
to deliver an adequate amount of foam sclerosant
to achieve therapeutic effect with a small number
of adverse events.15,18 The whole injection proce-
dure can be completed in 3 min. We observed no
deep vein thrombosis, visual disturbances, or
neurologic or other significant adverse events.
The use of compression hosiery for 1 week and
patient ambulation maintains the deep vein flow
and prevents thrombus propagation from the SFJ.
In this study, no deep vein thromboses were
observed, although despite good compression,
superficial thrombophlebitis due to blood trapping
is commonly encountered, especially in large extra-
fascial varices in the calf. Early repeated evacua-
tion of the trapped coagulum using an 18-G needle
under local anesthesia performed every week after
treatment helps relieve redness and tenderness. Hy-
perpigmentation of the overlying skin usually sub-
sides in 6 to 12 months, but in a few cases,
hyperpigmentation persists over a year.19,20
Few reports have examined the outcomes of UGFS
for GSV insufficiency. Pang and colleagues reported
an 82% wound healing rate 1 month after their
first foam sclerotherapy. Barrett and colleagues
reported a success rate of 97% (GSV complete scle-
rosis or <3 mm and minimal flow) at 22.5 months
with a mean of 2.19 treatment sessions. Darvall
and colleagues also reported that a single session of
foam sclerotherapy completely eradicated GSV
reflux in 97% of patients at 12 months. In our
long-term follow-up study, duplex-guided foam
sclerotherapy was also effective in treating GSV
insufficiency, with 89.6% of GSV free of recanali-
CHEN ET AL
2012 5

zation with two sessions of therapy during a mean
37.8 months of follow-up. Clinical studies on endo-
venous laser therapy showed that 90% to 95% of
the saphenous trunks are occluded 2 years after
therapy.21,22 Foam sclerotherapy is a simpler, fas-
ter, and more cost-effective than endovenous laser
treatment, and it can be repeated several times in
cases of recurrence. UGFS has replaced 80% of our
endovenous laser procedures.
GSV treated using foam sclerotherapy will eventu-
ally shrink, although the time to achieve fibrosis
for treated GSV after foam sclerotherapy
(12 months) was much longer than the time to
achieve fibrosis after endovenous laser surgery
(5.8 months),23 probably because of the thermal
effect of the laser–tissue interaction, which can
induce panluminal destruction and early tissue con-
traction, whereas chemical ablation using a sclero-
sant is mostly limited to the endothelial layer of
the vessel.24 The vein wall thickening and perivas-
cular tissue blurring observed after endovenous
laser surgery are more prominent than in foam
sclerotherapy using duplex ultrasound examina-
tion. In this study, the four of the six patients in
whom occlusion of the GSV was not achieved
within three sessions had an initial vein diameter
larger than 10 mm. Thus, endovenous laser and
stripping or ligation surgery is the treatment alter-
native for severe dilated incompetent GSV.15,21,25
In conclusion, our results for UGFS were promis-
ing, with achievement of effective occlusion of
GSV segments in 95% of patients and no compli-
cations at up to 37.8 months. Large-scale long-
term studies should be conducted to determine the
optimal protocol for foam sclerotherapy and to
investigate the role of different sclerosants such as
POL for treating chronic venous insufficiency.
References
1. Goldman MP, Bergan JJ, Guex J-J. Sclerotherapy–Treatment of
varicose and telangiectatic leg veins (4th ed). New York:
Mosby; 2007; pp. 163–88.
2. John Bergan, Cheng VL. Foam sclerotherapy. London: Royal
Society of Medicine Press; 2008; pp. 31–42.
3. Murad Alam SS. Procedures in cosmetic dermatology series:
treatment of leg veins: text with DVD (2nd ed). Philadelphia:
Saunders; 2006; pp. 71–106.
4. Hsu TS, Weiss RA. Foam sclerotherapy: a new era. Arch
Dermatol 2003;139:1494–6.
5. Darvall KA, Bate GR, Adam DJ, Silverman SH, et al. Duplex
ultrasound outcomes following ultrasound-guided foam
sclerotherapy of symptomatic primary great saphenous varicose
veins. Eur J Vasc Endovasc Surg 2010;40:534–9.
6. Barrett JM, Allen B, Ockelford A, Goldman MP. Microfoam
ultrasound-guided sclerotherapy of varicose veins in 100 legs.
Dermatol Surg 2004;30:6–12.
7. Hamahata A, Yamaki T, Sakurai H. Outcomes of ultrasound-
guided foam sclerotherapy for varicose veins of the lower
extremities: a single center experience. Dermatol Surg
2011;37:804–9.
8. Tessari L, Cavezzi A, Frullini A. Preliminary experience with a
new sclerosing foam in the treatment of varicose veins.
Dermatol Surg 2001;27:58–60.
9. Frullini A, Cavezzi A. Sclerosing foam in the treatment of
varicose veins and telangiectases: history and analysis of safety
and complications. Dermatol Surg 2002;28:11–5.
10. Cavezzi A, Tessari L. Foam sclerotherapy techniques: different
gases and methods of preparation, catheter versus direct
injection. Phlebology 2009;24:247–51.
11. Rao J, Goldman MP. Stability of foam in sclerotherapy:
differences between sodium tetradecyl sulfate and polidocanol
and the type of connector used in the double-syringe system
technique. Dermatol Surg 2005;31:19–22.
12. Islamoglu F. An alternative treatment for varicose veins:
ligation plus foam sclerotherapy. Dermatol Surg 2011;37:470–9.
13. Myers KA, Jolley D, Clough A, Kirwan J. Outcome of
ultrasound-guided sclerotherapy for varicose veins: medium-
term results assessed by ultrasound surveillance. Eur J Vasc
Endovasc Surg 2007;33:116–21.
14. Bradbury AW, Bate G, Pang K, Darvall KA, Adam DJ.
Ultrasound-guided foam sclerotherapy is a safe and clinically
effective treatment for superficial venous reflux. J Vasc Surg
2010;52:939–45.
15. Barrett JM, Allen B, Ockelford A, Goldman MP. Microfoam
ultrasound-guided sclerotherapy treatment for varicose veins in
a subgroup with diameters at the junction of 10 mm or greater
compared with a subgroup of less than 10 mm. Dermatol Surg
2004;30:1386–90.
16. Parsi K. Catheter-directed sclerotherapy. Phlebology 2009;24:98
–107.
17. Proebstle TM, Lehr HA, Kargl A, Espinola-Klein C, et al.
Endovenous treatment of the greater saphenous vein with a
940-nm diode laser: thrombotic occlusion after endoluminal
thermal damage by laser-generated steam bubbles. J Vasc
Surg 2002;35:
729–36.
FOAM SCLEROTHERAPY FOR TREATING INCOMPETENT GSV
DERMATOLOGIC SURGERY6

18. Yamaki T, Nozaki M, Sakurai H, Soejima K, Kono T. Multiple
small-dose injections can reduce the passage of sclerosant foam
into deep veins during foam sclerotherapy for varicose veins.
Eur J Vasc Endovasc Surg 2009;37:343–8.
19. Darvall KA, Bate GR, Adam DJ, Silverman SH. Ultrasound-
guided foam sclerotherapy for the treatment of chronic venous
ulceration: a preliminary study. Eur J Vasc Endovasc Surg
2009;38:764–9.
20. Darvall KA, Bate GR, Sam RC, Adam DJ, et al. Patients’
expectations before and satisfaction after ultrasound guided
foam sclerotherapy for varicose veins. Eur J Vasc Endovasc
Surg 2009;38:642–7.
21. Goldman MP. Intravascular lasers in the treatment of varicose
veins. J Cosmet Dermatol 2004;3:162–6.
22. Weiss RA, Munavalli G. Endovenous ablation of truncal veins.
Semin Cutan Med Surg 2005;24:193–9.
23. Yang CH, Chou HS, Lo YF. Incompetent great saphenous
veins treated with endovenous 1,320-nm laser: results for 71
legs and morphologic evolvement study. Dermatol Surg
2006;32:1453–7.
24. Fan CM, Rox-Anderson R. Endovenous laser ablation:
mechanism of action. Phlebology 2008;23:206–13.
25. Lo YF, Yang CH. Stripping and ligation of the saphenous vein.
Semin Cutan Med Surg 2005;24:200–8.
Address correspondence and reprint requests to:Chih-Hsun Yang, MD, Department of Dermatology,Chang Gung Memorial Hospital, 199, Tung-HwaNorth Road. Taipei, Taiwan, ore-mail: [email protected]
CHEN ET AL
2012 7