Ultrasound elastography of breast and prostate lesions
41
Ultrasound Elastography of Breast and Prostate Lesions . Daniel T. Ginat, MD, MS • Stamatia V. Destounis, MD • Richard G.Barr, MD, PhD • Benjamin Castaneda, PhD• John G. Strang,MD Deborah J. Rubens, MD
-
Upload
rajesh-venunath -
Category
Health & Medicine
-
view
194 -
download
13
Transcript of Ultrasound elastography of breast and prostate lesions
Ultrasound Elastography
of Breast and Prostate
Lesions.
Daniel T. Ginat, MD, MS • Stamatia V. Destounis, MD • Richard
G.Barr, MD, PhD • Benjamin Castaneda, PhD• John G.
Strang,MD Deborah J. Rubens, MD
Abstract• Elastography is a technique that maps relative tissue stiffness.
• Ultrasonographic (US) elastography (sonoelastography) is a novel modality that is the subject of active research for clinical applications,primarily breast and prostate lesions.
• Breast and prostate tumors generally have biomechanical properties different from those of normal tissues: Tumors are usually stiffer. This phenomenon is responsible for tissue contrast on elastograms.
• In this journal, the sonoelastographic appearances of several common breast lesions, including fibroadenomas, simple and complex cysts, ductal carcinomas, malignant lymph nodes, and hematomas, are reviewed. In addition, the US elastographic appearances of the normal prostate gland, prostate carcinomas, and benign prostate hyperplasia are also illustrated.
• Potential pitfalls in the interpretation of elastograms, including false-positive and false-negative images, are also illustrated.

Introduction
• Ultrasonographic (US) elastography (sonoelastography) is a noninvasive imaging technique that can be used to depict relative tissue stiffness or displacement (strain) in response to an imparted force.
• Stiff tissues deform less and exhibit less strain than compliant tissues in response to the same applied force. Thus, the basis of elastography is analogous to manual palpation.
• The application of US elastography for imaging tissues is relatively novel, first described in 1987 by Krouskop et al.
• Since its inception, sonoelastography has been used to evaluate numerous types of tissues, including breast, prostate,liver, blood vessels, thyroid, and musculoskeletal structures.
Types Of Elastography
• Compression Sonoelastography
• Vibration Sonoelastography.
Elastography• Sonoelastography is based on the comparison of signals
acquired before and after tissue displacement.
• Compression elastography involves calculating a strain profile in a direction perpendicular to the tissue surface in response to an externally applied force.
• Specialized software is used to calculate the relative difference in tissue movement from one frame to another and then to estimate the tissue deformation. The deformation measurements are mapped onto an elastogram, on which stiffer areas are depicted as dark and more-elastic areas are lighter, according to convention.
Elastography
• Vibration elastography, on the other hand, generates tissue displacement through the use of an independent external vibration source. Relative displacement is measured by using a variant of Doppler imaging that depicts differential motion of tissue types.
• This technique provides good correlation for tissues that have a large difference in stiffness.
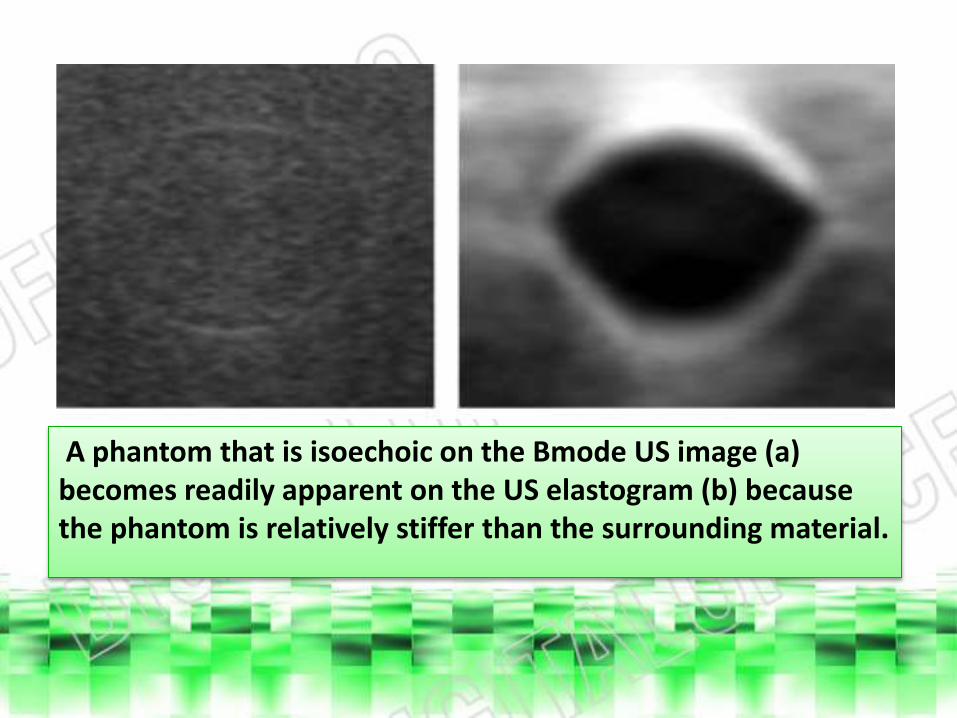
A phantom that is isoechoic on the Bmode US image (a) becomes readily apparent on the US elastogram (b) because the phantom is relatively stiffer than the surrounding material.
Breast US Elastography
• Compression elastography may have a role for further evaluating abnormal findings on conventional breast US images and differentiating benign from malignant breast lesions.
• The two most important elastographic characteristics in evaluating breast lesions are size and stiffness criteria.
• The size criterion denotes the difference in the measurement of the longest diameter on the corresponding B-mode image and the elastogram.
• Structures that are less compressible than surrounding tissues measure larger on the elastogram than they do on the corresponding B-mode image, resulting in a size discordance. Therefore, cancers will be larger on the elastogram than on the conventional US image.
Breast US Elastography
• Alternatively, this characteristic can be expressed as a ratio, such that a ratio of elastogram–to–B-mode lesion diameters that is greater than or equal to one is suggestive of malignancy . This phenomenon is attributed to the desmoplastic reaction incited by many malignant breast neoplasms.
Normal Breast Tissue
• Biomechanical testing has shown normal fibro-glandular breast tissue to be markedly stiffer than normal fatty breast tissue by as much as two orders of magnitude. Therefore, at elastography, fatty tissue will appear bright with respect to the adjacent glandular tissue, and normal fibrous parenchyma appears darker.
• Normal lymph nodes are reniform in shape and contain a hyperechoic fatty hilum on B-mode US images. At elastography, these features translate into relative softness of the lymph node, with a slightly lower elastogram-to-B-mode size ratio.
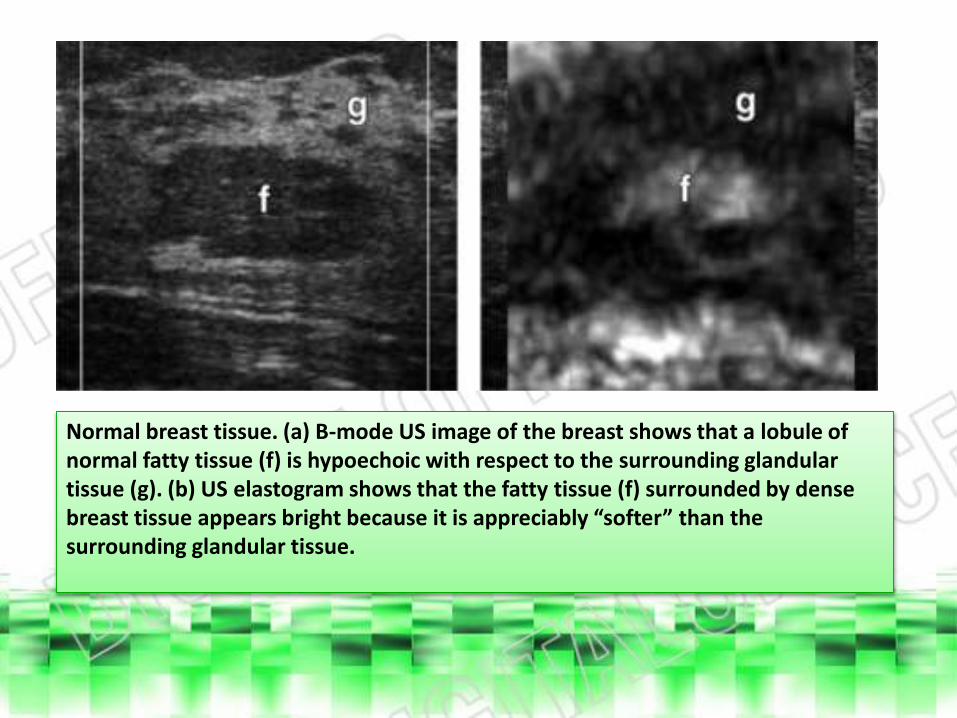
Normal breast tissue. (a) B-mode US image of the breast shows that a lobule of normal fatty tissue (f) is hypoechoic with respect to the surrounding glandular tissue (g). (b) US elastogram shows that the fatty tissue (f) surrounded by dense breast tissue appears bright because it is appreciably “softer” than the surrounding glandular tissue.
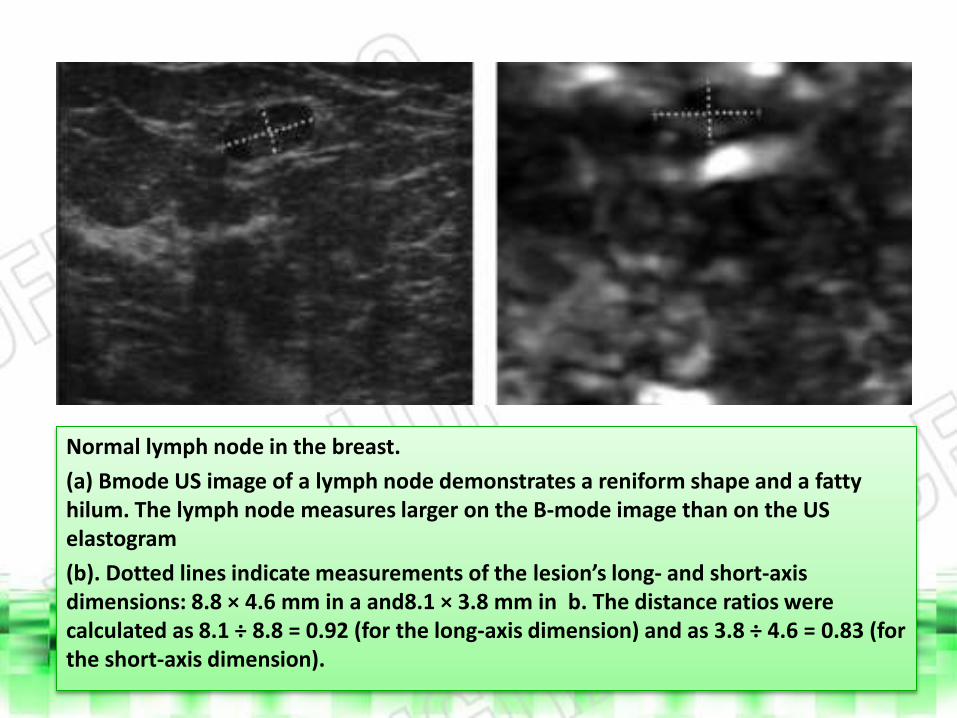
Normal lymph node in the breast.
(a) Bmode US image of a lymph node demonstrates a reniform shape and a fatty hilum. The lymph node measures larger on the B-mode image than on the US elastogram
(b). Dotted lines indicate measurements of the lesion’s long- and short-axis dimensions: 8.8 × 4.6 mm in a and8.1 × 3.8 mm in b. The distance ratios were calculated as 8.1 ÷ 8.8 = 0.92 (for the long-axis dimension) and as 3.8 ÷ 4.6 = 0.83 (for the short-axis dimension).
Simple Cysts, Complex Cysts, and Fibrocystic
Change.• Simple cysts represent the most common type of breast mass. Simple
cysts are benign entities that result from fluid accumulation within the terminal ducts.
• These lesions usually are recognized easily on conventional US images and are characterized as anechoic round or oval well-circumscribed lesions with enhanced through transmission and an imperceptible posterior wall. However, these lesions often demonstrate variable elastographic appearances.
• The typical manifestation of a simple cyst at elastography is a “target” or “bull’s-eye” appearance, in which central bright compressible material is surrounded by a dark concentric rim. This appearance, as well as the additional bright area often observed deep to the cyst, is attributable to artifact .
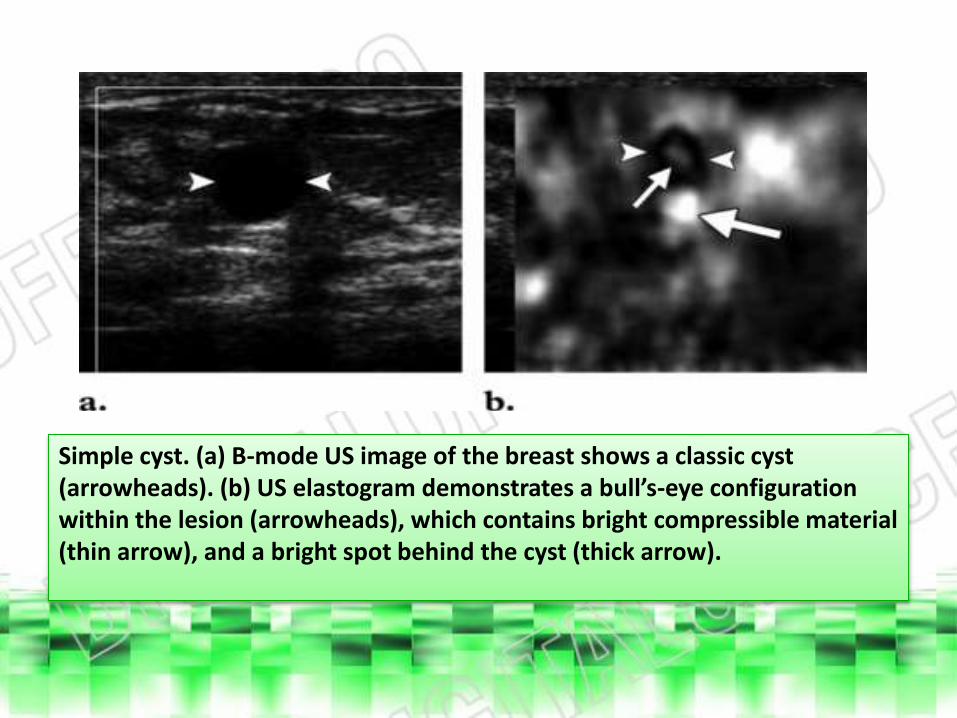
Simple cyst. (a) B-mode US image of the breast shows a classic cyst (arrowheads). (b) US elastogram demonstrates a bull’s-eye configuration within the lesion (arrowheads), which contains bright compressible material (thin arrow), and a bright spot behind the cyst (thick arrow).
• The presence of internal debris or septa characterizes complex cysts. As a result, complex cysts can mimic the appearance of solid lesions at B-mode US. Lesions containing thick walls or septa or an appreciable solid component are usually subjected to biopsy.
• US elastography can help elucidate the cystic nature of lesions with confounding appearances at B-mode US. Thus, elastography is useful for characterizing complex cysts with greater confidence, which can help avoid an unnecessary core biopsy in some instances.
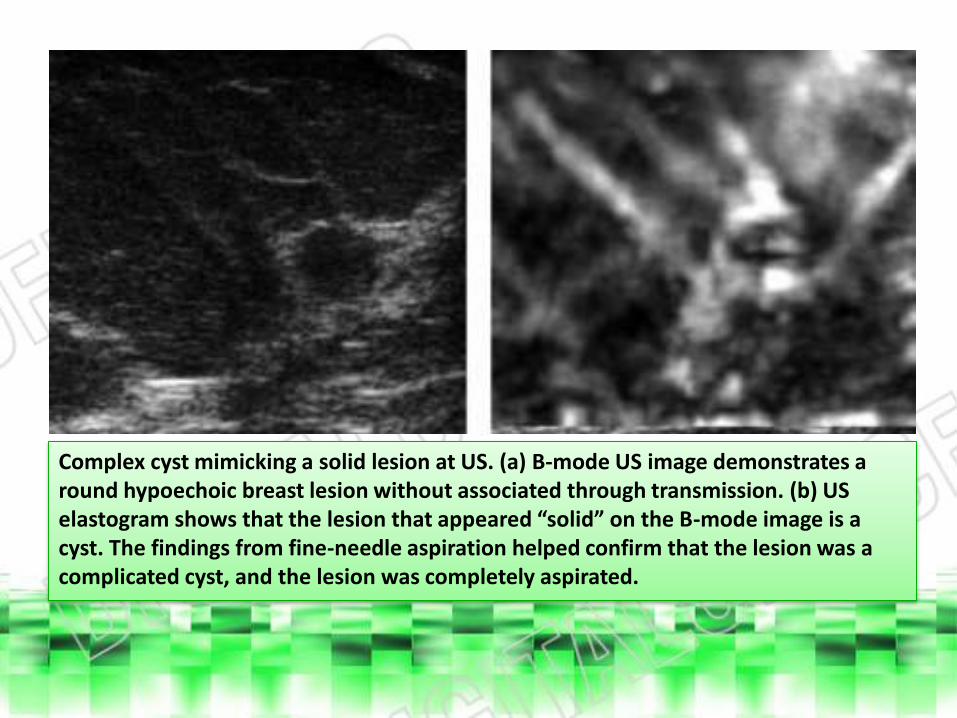
Complex cyst mimicking a solid lesion at US. (a) B-mode US image demonstrates a round hypoechoic breast lesion without associated through transmission. (b) US elastogram shows that the lesion that appeared “solid” on the B-mode image is a cyst. The findings from fine-needle aspiration helped confirm that the lesion was a complicated cyst, and the lesion was completely aspirated.

• Fibrocystic change represents a commonly encountered spectrum of nonsimple cysts. Although this entity is benign and may be considered a normal variant, the differential diagnosis at imaging includes atypical ductal hyperplasia, lobular neoplasia, and ductal carcinoma in situ, thereby requiring biopsy. At sonoelastography, however, the benign cystic nature of fibrocystic change is often apparent .

Fibrocystic change. (a) B-mode US image demonstrates an irregular heterogeneous lesion in a patient who presented with a palpable mass in the right breast. (b) On the US elastogram, the lesion appears soft and smaller than on the B-mode image. The findings from a subsequent biopsy showed fibrocystic change and periductal inflammation. Dotted lines indicate measured lesion diameters: 1 = 7.16 mm; 2 = 5.55 mm; 3 = 5.02 mm; and 4 = 4.29 mm. Distance ratio was calculated as 5.02 ÷ 7.16 = 0.70.
Fibroadenoma
• Fibroadenomas are benign tumors that represent the most common type of solid breast mass.
• At mammography, these lesions classically are seen as lobulated circumscribed masses with coarse calcifications in a “popcorn” configuration. US images typically demonstrate fibroadenomas as well-circumscribed hypoechoic masses that are wider than tall, such that the long axis is parallel to the skin. Occasionally, fibroadenomas can have confounding features at B-mode US, such as dimensions that are taller than wide.
Fibroadenoma
• In such instances, sonoelastography can help elucidate the benign nature of the lesion Indeed, as many as 73% of fibroadenomas could be differentiated from malignant tumors on the basis of elastographic size and brightness criteria However, fibroadenomassometimes have elastographic size or stiffness features that are more typical of malignancy Such false-positive elastographic findings tend to occur in fibroadenomasthat are larger than 2 cm and contain calcifications.
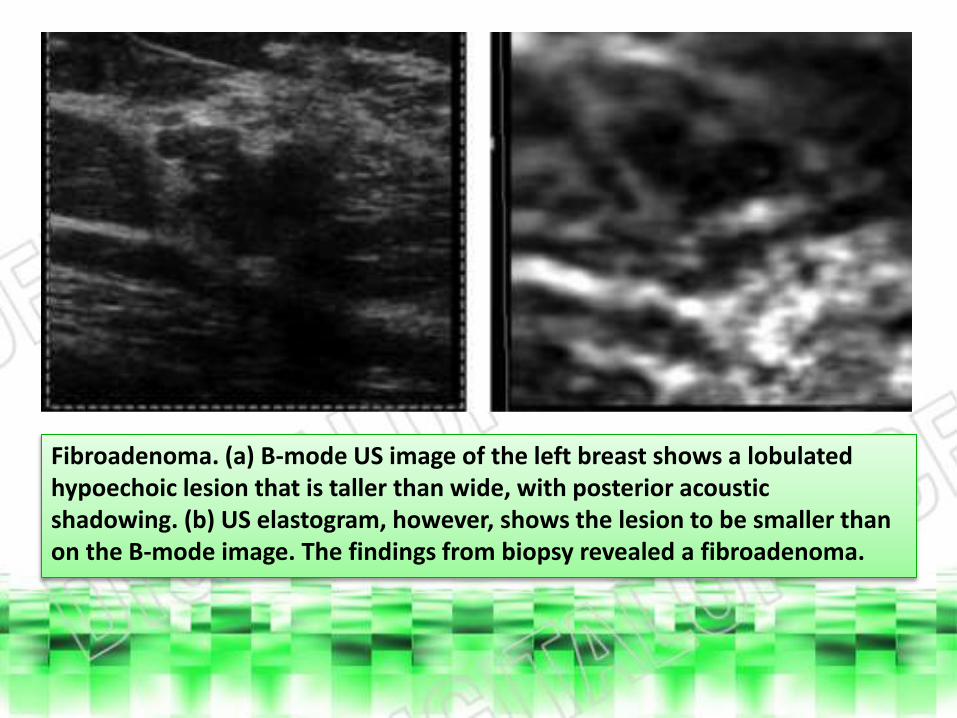
Fibroadenoma. (a) B-mode US image of the left breast shows a lobulated hypoechoic lesion that is taller than wide, with posterior acoustic shadowing. (b) US elastogram, however, shows the lesion to be smaller than on the B-mode image. The findings from biopsy revealed a fibroadenoma.
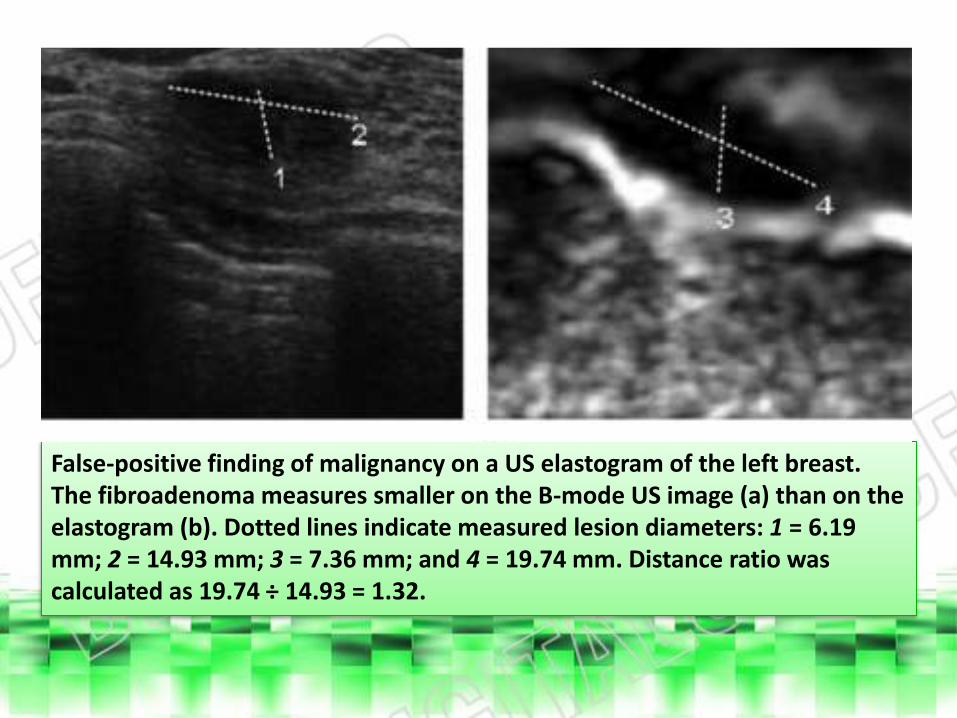
False-positive finding of malignancy on a US elastogram of the left breast. The fibroadenoma measures smaller on the B-mode US image (a) than on the elastogram (b). Dotted lines indicate measured lesion diameters: 1 = 6.19 mm; 2 = 14.93 mm; 3 = 7.36 mm; and 4 = 19.74 mm. Distance ratio was calculated as 19.74 ÷ 14.93 = 1.32.
Invasive Ductal Carcinoma
• Invasive ductal carcinoma is the most common malignant neoplasm of the breast. At mammography, invasive ductal carcinoma typically manifests as a dense spiculated irregular mass associated with microcalcifications, particularly pleomorphic microcalcifications, and indistinct margins that reflect the infiltrative behavior of the tumor.
• Similarly, characteristic US features of invasive ductal carcinoma include a hypoechoic spiculated or microlobular branching mass that is taller than wide, with angular margins and a hyperechoichalo. Skin thickening, lymphadenopathy, edema, and ligament retraction are secondary indicators of malignancy that can also be identified at US examination.

Invasive Ductal Carcinoma
• Invasive ductal carcinoma is generally much stiffer than any of the other breast tissues and benign tumors such as fibroadenomas. As a result, invasive ductal carcinoma typically is appreciably darker than normal tissues or benign lesions and is substantially larger on the elastogram than on B-mode US images.
• Although uncommon, invasive ductal carcinoma can have the appearance of a benign well-circumscribed round mass on B-mode US images.

• Similarly, tumor necrosis can manifest as anechoic areas with acoustic enhancement that can mimic cysts. False-negative elastograms can also occur and are characterized by high strain, erroneous measurements, and other technical errors.
• Lesions that have only one discordant feature between the B-mode US image and the elastogram may be considered indeterminate on the elastogram.
• Overall, US elastography is reported to have a sensitivity greater than 95% and a specificity of about 85% for differentiating between benign and malignant breast lesions.
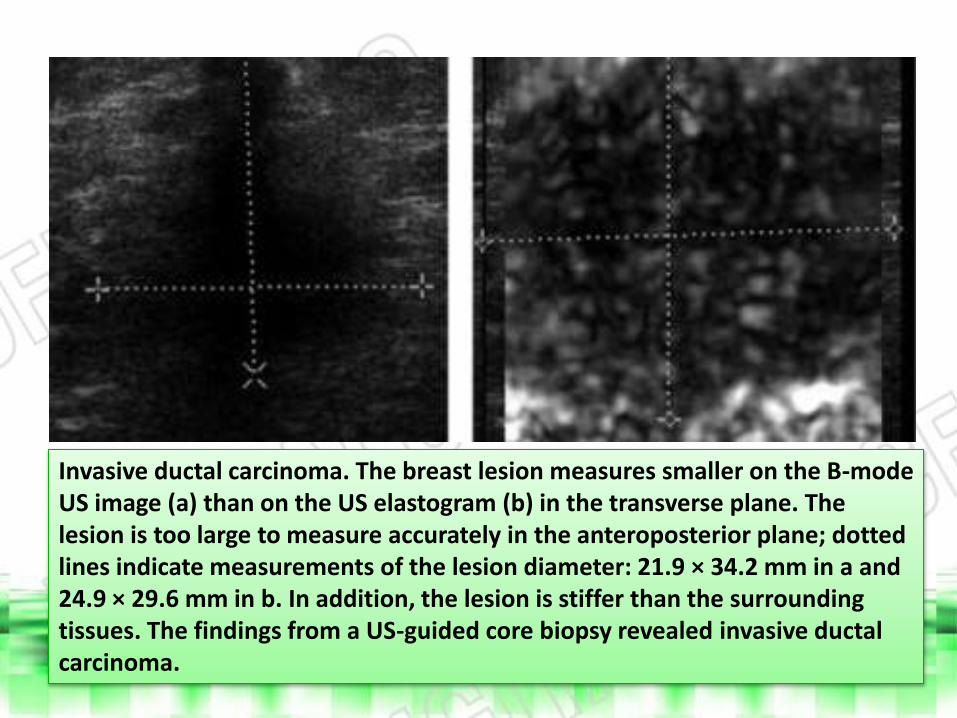
Invasive ductal carcinoma. The breast lesion measures smaller on the B-mode US image (a) than on the US elastogram (b) in the transverse plane. The lesion is too large to measure accurately in the anteroposterior plane; dotted lines indicate measurements of the lesion diameter: 21.9 × 34.2 mm in a and 24.9 × 29.6 mm in b. In addition, the lesion is stiffer than the surrounding tissues. The findings from a US-guided core biopsy revealed invasive ductal carcinoma.

Metastatic Lymph Node Involvement
• At B-mode US, malignant lymph nodes classically exhibit rounded enlargement with effacement of the normal fatty hilum.
• The use of Doppler US can improve the diagnostic accuracy for metastatic involvement by demonstrating increased vascularity.
• Similar to other malignant breast lesions, lymph nodes that contain metastases tend to appear stiffer and disproportionately larger at elastography.
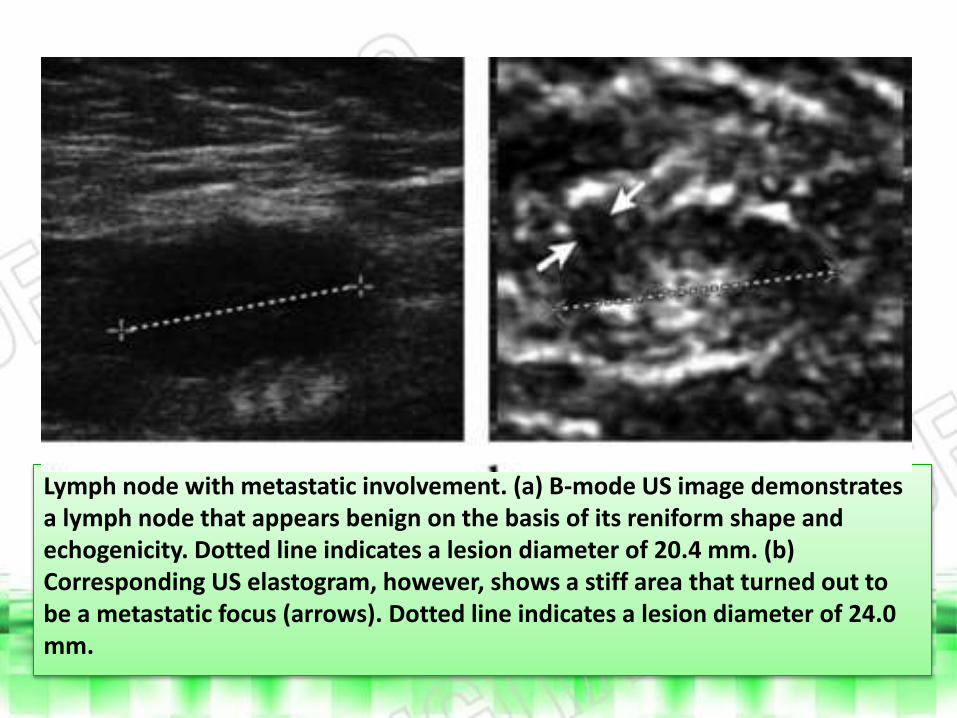
Lymph node with metastatic involvement. (a) B-mode US image demonstrates a lymph node that appears benign on the basis of its reniform shape and echogenicity. Dotted line indicates a lesion diameter of 20.4 mm. (b) Corresponding US elastogram, however, shows a stiff area that turned out to be a metastatic focus (arrows). Dotted line indicates a lesion diameter of 24.0 mm.
Hematoma
• Breast hematomas may be iatrogenic or a result of trauma.
• US appearance of these lesions varies with time, beginning as hyperechoic fluid collections that progress to hypoechoic lesions and then to septate cystic structures that eventually regress.
• At mammography, hematomas may appear as irregular masses of increased density. Although clinical history and results of physical examination are often helpful in confirming the diagnosis, further work-up is sometimes warranted.
• Elastography can help confirm benign nature of hematomas by demonstrating low stiffness and a low elastogram–to–B-mode size ratio.
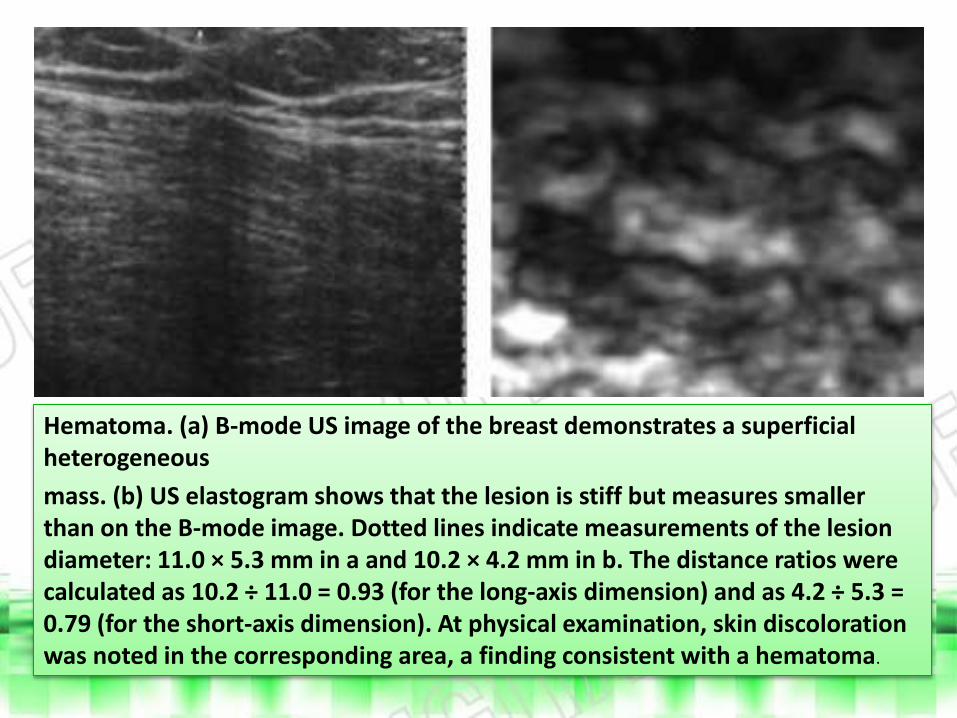
Hematoma. (a) B-mode US image of the breast demonstrates a superficial heterogeneous
mass. (b) US elastogram shows that the lesion is stiff but measures smaller than on the B-mode image. Dotted lines indicate measurements of the lesion diameter: 11.0 × 5.3 mm in a and 10.2 × 4.2 mm in b. The distance ratios were calculated as 10.2 ÷ 11.0 = 0.93 (for the long-axis dimension) and as 4.2 ÷ 5.3 = 0.79 (for the short-axis dimension). At physical examination, skin discoloration was noted in the corresponding area, a finding consistent with a hematoma.
Prostate US Elastography
• Two main types of US elastography have been applied for imaging the prostate: compression and vibration.
Prostate Cancer• Endorectal US continues to be the most commonly used imaging
modality for assessing the prostate; however, it is relatively inaccurate for cancer detection. Endorectal US has a role in guiding prostate biopsies .
• Magnetic resonance imaging and computed tomography are mainly implemented for staging.
• At B-mode US, most prostate cancers are hypoechoic, but many are isoechoic, and a few are hyperechoic. As a result, the overall sensitivity of endorectal US for prostate cancer detection is about 50% (20). The added use of Doppler imaging increases the detection rate by only 5%.
Prostate Cancer
• In contrast, endorectal real-time elastography enables the diagnosis of prostate cancer with a reported accuracy of 76% . However, the major role of elastography is to improve the results of image-directed biopsy and therapy, compared with the use of endorectal US alone.
• Prostate cancers have a higher elastic modulus (stiffness) than that of surrounding normal prostate tissue. Consequently, prostate cancers will appear dark on elastograms.
• Often, intermediate-grade and high-grade malignant lesions that are subtle or even unapparent on B-mode US images are prominent on elastograms as dark areas of low strain.
• Overall, US elastography has a sensitivity in the range of 68%–86%, a specificity of 72%–81%, and an accuracy of 76% for the detection of prostate cancers.
Prostate Cancer
• With regard to brachytherapy, it is feasible to image radioactive brachytherapy seeds with US elastography; however, it is not yet established whether this imaging modality would be of benefit for seed implantation.
• Image processing of the elastograms, including three-dimensional volume rendering, can be performed to provide comprehensive lesion assessment .This type of image reconstruction can be useful for surgical planning, particularly for partial prostatectomy.
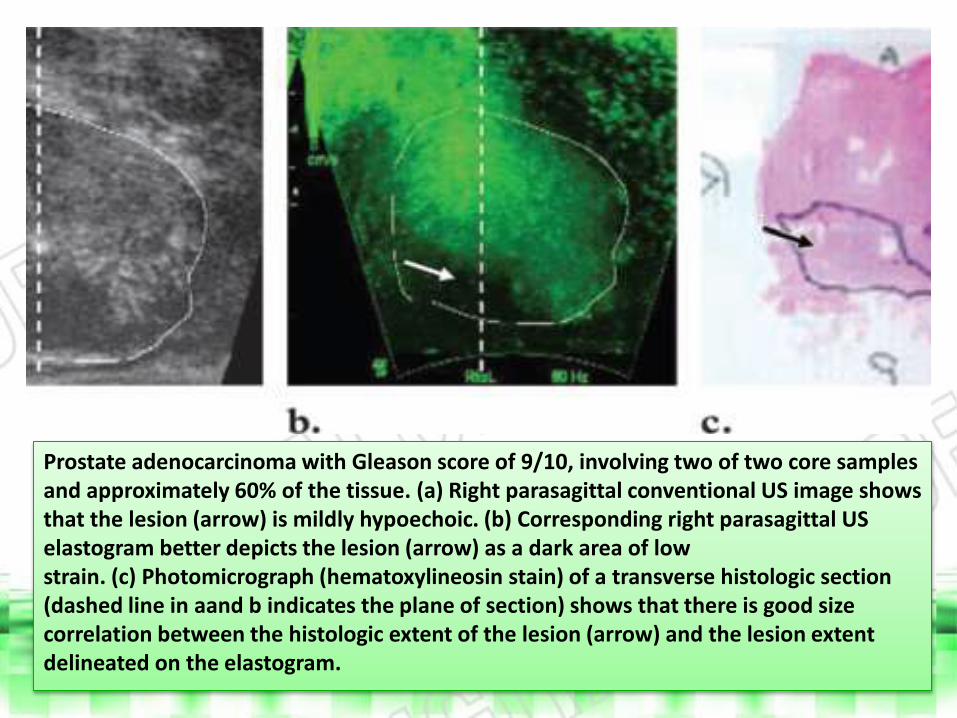
Prostate adenocarcinoma with Gleason score of 9/10, involving two of two core samples and approximately 60% of the tissue. (a) Right parasagittal conventional US image shows that the lesion (arrow) is mildly hypoechoic. (b) Corresponding right parasagittal US elastogram better depicts the lesion (arrow) as a dark area of low strain. (c) Photomicrograph (hematoxylineosin stain) of a transverse histologic section (dashed line in aand b indicates the plane of section) shows that there is good size correlation between the histologic extent of the lesion (arrow) and the lesion extent delineated on the elastogram.
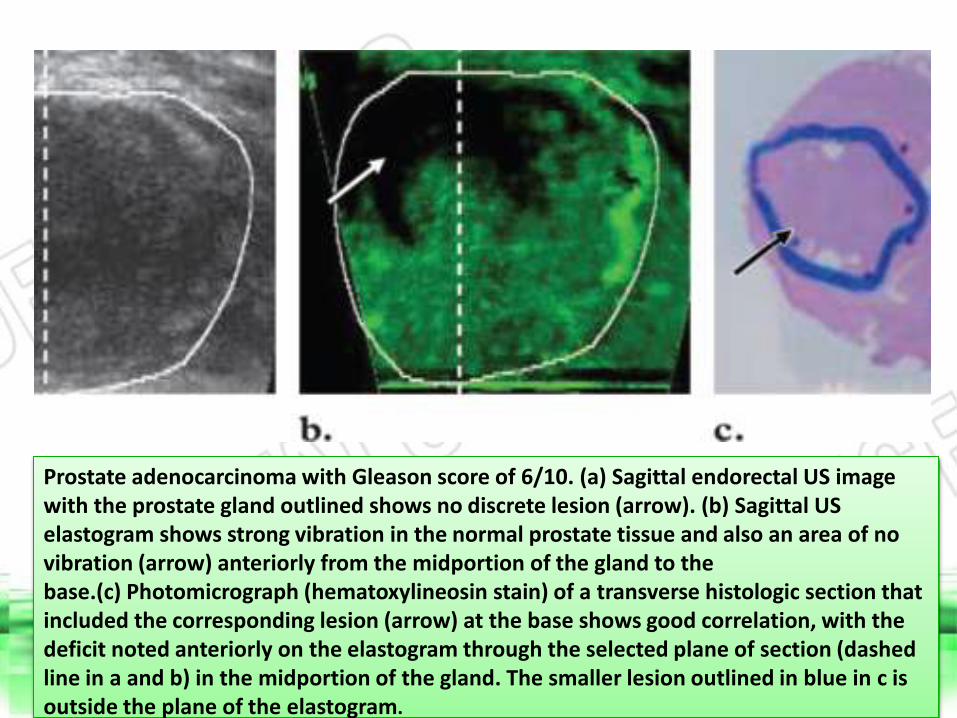
Prostate adenocarcinoma with Gleason score of 6/10. (a) Sagittal endorectal US image with the prostate gland outlined shows no discrete lesion (arrow). (b) Sagittal US elastogram shows strong vibration in the normal prostate tissue and also an area of no vibration (arrow) anteriorly from the midportion of the gland to the base.(c) Photomicrograph (hematoxylineosin stain) of a transverse histologic section that included the corresponding lesion (arrow) at the base shows good correlation, with the deficit noted anteriorly on the elastogram through the selected plane of section (dashed line in a and b) in the midportion of the gland. The smaller lesion outlined in blue in c is outside the plane of the elastogram.
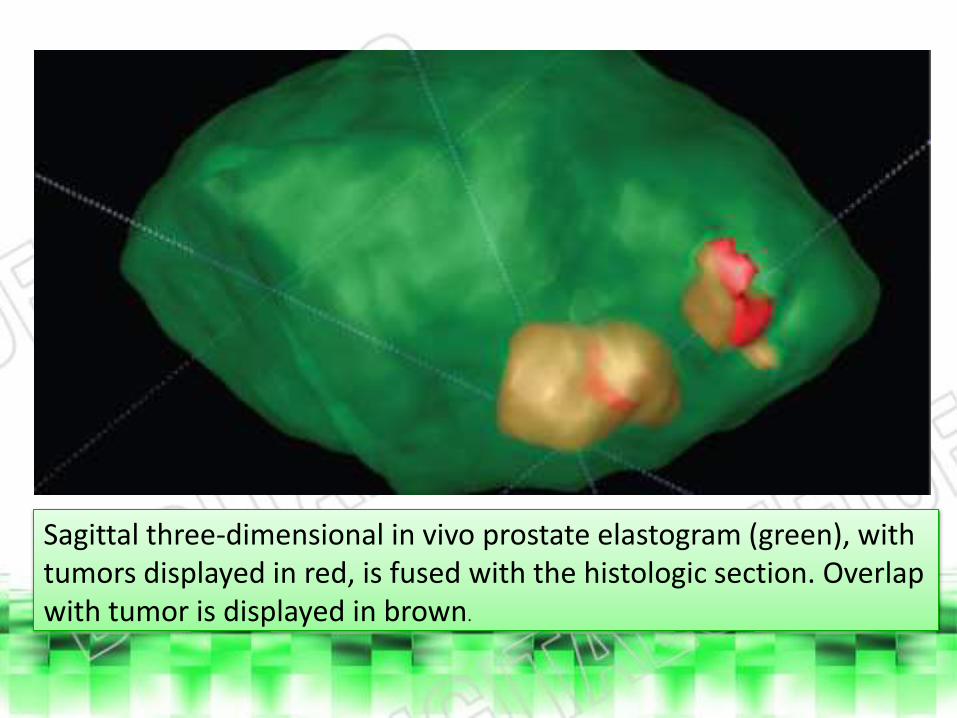
Sagittal three-dimensional in vivo prostate elastogram (green), with tumors displayed in red, is fused with the histologic section. Overlap with tumor is displayed in brown.
Benign Prostatic Hyperplasia
• The appearance of benign prostatic hyperplasia at endorectal US is variable but usually consists of a heterogeneous hypoechoic area or areas in the transitional zone.
• In general, foci of benign prostatic hyperplasia have elastic moduli (stiffness) that are an order of magnitude greater than those of normal prostate tissues but are less than those of prostate carcinomas.
• As a result, on elastograms, benign prostatic hyperplasia will appear darker than normal prostate tissue.
• However, the difference between benign prostatic hyperplasia and prostate carcinoma can be difficult to discern because benign prostatic hyperplasia also appears darker than the background tissues. Consequently, benign prostatic hyperplasia can represent a false-positive finding for cancer.
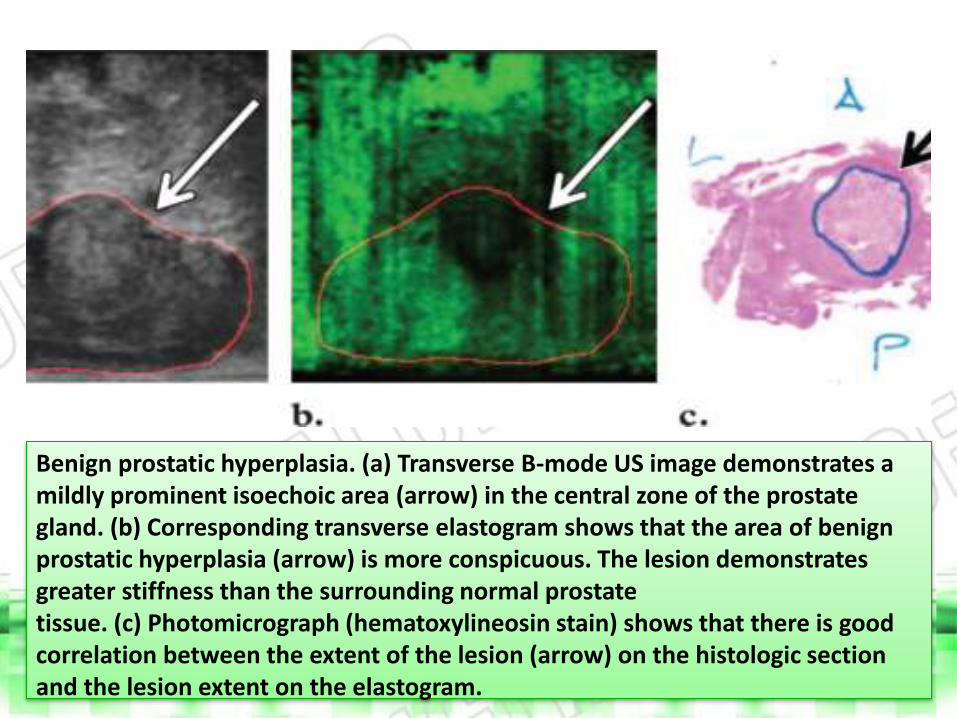
Benign prostatic hyperplasia. (a) Transverse B-mode US image demonstrates a mildly prominent isoechoic area (arrow) in the central zone of the prostate gland. (b) Corresponding transverse elastogram shows that the area of benign prostatic hyperplasia (arrow) is more conspicuous. The lesion demonstrates greater stiffness than the surrounding normal prostate tissue. (c) Photomicrograph (hematoxylineosin stain) shows that there is good correlation between the extent of the lesion (arrow) on the histologic section and the lesion extent on the elastogram.
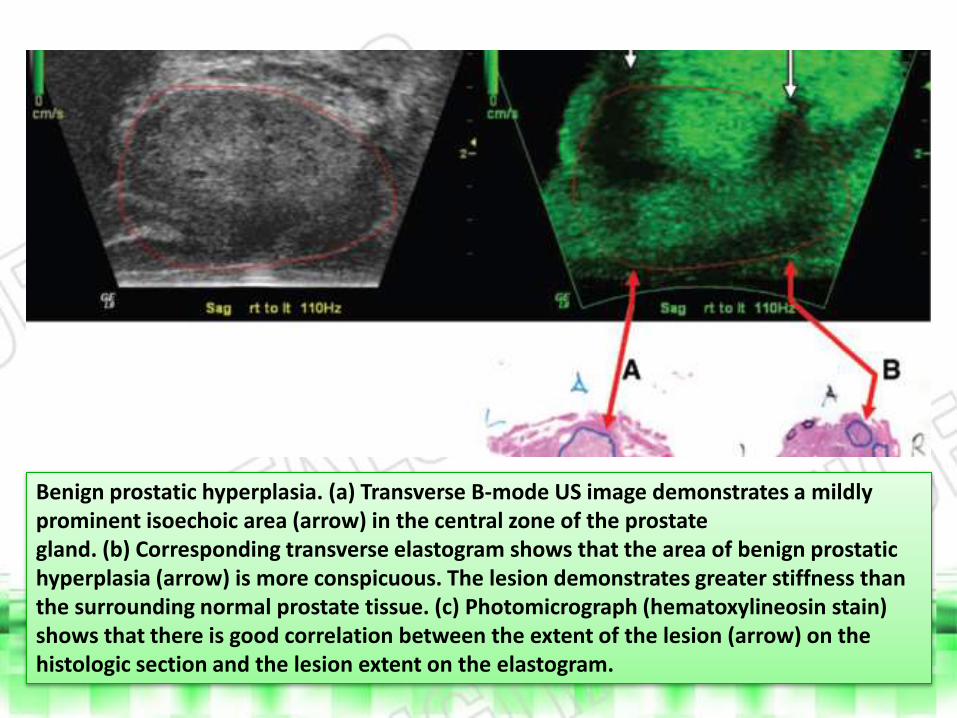
Benign prostatic hyperplasia. (a) Transverse B-mode US image demonstrates a mildly prominent isoechoic area (arrow) in the central zone of the prostate gland. (b) Corresponding transverse elastogram shows that the area of benign prostatic hyperplasia (arrow) is more conspicuous. The lesion demonstrates greater stiffness than the surrounding normal prostate tissue. (c) Photomicrograph (hematoxylineosin stain) shows that there is good correlation between the extent of the lesion (arrow) on the histologic section and the lesion extent on the elastogram.
Conclusions
• Although not yet established for routine clinical use, US elastography is a promising adjunctive modality for evaluating breast and prostate lesions, on the basis of the results of the initial laboratory and clinical investigations. Nevertheless, validation of this modality through prospective trials is warranted.
• Ultimately, sonoelastography is expected to improve the accuracy of diagnosis for breast and prostate lesions in conjunction with conventional modalities.
• As a result, US elastography may be used to reduce biopsy rates for breast lesions and to more appropriately guide biopsy of prostate lesions.
• The potential use of US elastography for therapeutic applications is also foreseen. For example, real-time elastography could be applied to monitor therapy with lesion ablation, such as radiofrequency ablation and treatment with high-intensity focused ultrasound.